
Abstract
Objective
To evaluate the effect of undernutrition when young on the risk of poor renal function in adulthood in women with diabetes mellitus.
Methods
We studied diabetic women born between 1921 and 1958 who were exposed to the 1959-to-1962 Chinese famine when they were 0 to 37 years old. Exposure age was classified as young adulthood (18 to 37 years), adolescence (10 to 17 years), or childhood (0 to 9 years). The Adolescence group, which was provided with the largest amount of food during the famine, was used as the control group, and variance and binary logistic regression analyses were performed.
Results
The prevalences of low estimated glomerular filtration rate (eGFR) in the Childhood, Adolescence, and Young adulthood groups were 5.26%, 22.39%, and 79.24%, respectively. The risk of low eGFR for the Young adulthood group (odds ratio [OR] 1.65, 95% confidence interval [CI] 1.10, 2.48), but not for the Childhood group (OR 1.10, 95% CI 0.68, 1.78), was higher than that for the Adolescence group after adjustment for potential confounders.
Conclusions
Undernutrition during young adulthood significantly increases the risk of renal dysfunction in adult women with diabetes. Therefore, the nutrition of less affluent young women should be improved.
Introduction
Diabetic nephropathy has become the commonest reason to commence haemodialysis in Latin America. 1 In China, the prevalence of diabetes has increased significantly, from 0.67% in 1980 2 to 11.6% in 2013. 3 Because of the large number of patients with diabetes, diabetic nephropathy has replaced chronic nephritis as the commonest reason to commence haemodialysis in Beijing 4 and Shanghai, 5 which are the most economically developed cities in China. Indeed, the prevalence had reached 579 per million people by the end of 2013. 2 Therefore, it is important to identify risk factors for poor renal function in patients with diabetes.
Previous studies have shown that living through a famine when young, such as the Dutch famine of 1944 to 1945 and the Chinese famine of 1959 to 1962, significantly increases the subsequent prevalences of diabetes6–8 and proteinuria 9 in adulthood. Nutritional and economic development programs have helped children and adolescents in less affluent areas improve their nutrition, but women in their young adulthood are typically not targeted. For historical, traditional, cultural and economic reasons, women in less affluent areas often have lower social status. Moreover, young adult women in such areas often have to do a lot of housework and caring for others. Because of this, such women may have difficulty getting enough food and experience undernutrition, 10 which can have long-lasting effects on health.
China experienced a severe famine between 1959 and 1962. 11 During this period, food was supplied strictly according to age.12,13 The largest amount of food (16 kg/month) was provided for adolescent girls, who were usually in school, because the amount supplied was gradually increased according to age in female children. However, young adult women aged 18 to 37 were allocated less food (12.5 kg/month), 14 despite having to work. This disparity allows us to determine the effect of undernutrition in young adulthood on renal function in adult women with diabetes.
In the present study, health examination data for 2435 women with diabetes in Jiangchuan Community, Shanghai, China, who were between 0 and 37 years old at the time of the 1959 to 1962 famine, were collected between October 2011 to September 2014 and used to evaluate the effect of undernutrition during young adulthood on the risk of poor renal function in adult women with diabetes.
Methods
Data collection and ethics
Using physical examination data collected between October 2011 and September 2014 in Jiangchuan Community, Shanghai, China, we retrospectively studied women with diabetes who were 0 to 37 years old at the time of the famine in China, between 1959 and 1962, and classified them according to their age at the time of exposure. Questionnaires were used by professional medical staff to obtain the name, sex, date of birth, and history of diabetes from the patients; and physical examination data (blood pressure, body mass index [BMI] and waist-hip ratio [WHR]) and laboratory data (serum lipid profile, fasting blood glucose [FBG], glycosylated haemoglobin A1c [HbA1c] and urine albumin/creatinine ratio [UACR]) were recorded (Figure 1). The study was performed according to the principles of the Declaration of Helsinki of 1975, revised in 2013, and approved by the Ethics Committee of the Fifth People’s Hospital of Shanghai, Fudan University (approval number 2010-024). All the participants provided their written informed consent. All the patient details were de-identified for the study.
Laboratory measurements and definitions
Venous blood was collected in the early morning, after fasting for 8 hours, for the measurement of FBG, HbA1c, creatinine and lipids; and urine samples were collected to measure UACR. FBG was measured using the glucose oxidase method (Roche Diagnostics, Basel, Switzerland). Lipids, creatinine and urine albumin were measured using an automatic analyser (Hitachi 7170s, Tokyo, Japan). HbA1c was measured using high-performance liquid chromatography (ha-8180 HbA1c analyser, Arkray, Kyoto, Japan).
The American Diabetes Association criteria were used to define diabetes. Therefore, participants had to meet one or more of the following criteria: (1) fasting blood glucose ≥7.0 mmol/L, (2) a random blood glucose ≥11.1 mmol/L or (3) a clear history of diabetes. Estimated glomerular rate filtration (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula and was used to evaluate renal function: eGFR (mL × minute−1 ×1.73 m−2) = 144 × (Scr/κ)a × (0.993)age, where Scr = serum creatinine concentration. If Scr was >0.7 mg/dL (62 μmol/L), then “a” was given a value of −1.209, and if Scr ≤0.7 mg/dL (62 μmol/L), then “a” was given a value of −0.329, and κ = 0.7. 15 An eGFR <90 mL × minute−1 × 1.73 m−2 was defined as low. BMI was calculated as body weight in kilograms divided by the square of height in metres. WHR was calculated as waist circumference/hip circumference.
Grouping of the participants
According to Bogin’s definition of the postnatal human life cycle 16 and date of birth, the participants were allocated to three groups: (1) a Childhood exposure group, born between 1 January 1949 and 31 December 1958, consisting of participants who experienced famine as a child (0 to 9 years), during which period rapid development of physical strength, behaviour and cognition occurs; (2) an Adolescence exposure group, born between 1 January 1941 and 31 December 1948, consisting of participants who experienced famine when 10 to 17 years old, when accelerated growth and sexual development occurs; and (3) a Young adulthood exposure group, born between 1 January 1921 and 31 December 1940, consisting of participants who experienced famine when 18 to 37 years old, when a steady state is reached.
Food was supplied on a strict basis during the famine (Table 1). 12 During this period, the supply of food to children (0 to 9 years old) was gradually increased with age. Adolescents (10 to 17 years old), who were usually in school, were supplied with 12.5 to 16 kg/month of food, but only 12.5 kg/month of food was supplied to young adults (18 to 37 years), despite that age group having to work. Moreover, we believe young mothers usually shared their allocation of food with their children, which would have resulted in more severe undernutrition in young women than in adolescents. Therefore, the Adolescence group would have been on the highest plane of nutrition during the famine, so this was used as the control group for the study of the effect of undernutrition during young adulthood on kidney function in adult women with diabetes.
The quantity of food supplied per month during the famine in Shanghai to girls/women according to their age.

Statistical analysis
Continuous data are expressed as mean ± standard deviation and categorical data are expressed as the number of cases and percentages. One-way analysis of variance (ANOVA) was used to compare the characteristics of the participants between groups. The effect of famine on the risk of low eGFR in adulthood was assessed using binary logistic regression analysis. The initial analysis was unadjusted for potential confounding factors; model 1 was adjusted for the duration of diabetes and age; model 2 was adjusted for model 1 factors plus systolic blood pressure (SBP), diastolic blood pressure (DBP), BMI and WHR; and model 3 was adjusted for model 2 factors, plus FBG, HbA1c, total cholesterol (TC), low-density lipoprotein-cholesterol (LDL-C), high-density lipoprotein-cholesterol (HDL-C), triglycerides (TG) and UACR. Statistical analyses were performed using SPSS 22.0 (IBM Corp., Armonk, NY, USA) and P < 0.05 was accepted as indicating statistical significance.
Results
Clinical characteristics
Between October 2011 and September 2014, 2435 women with diabetes, aged 53 to 93 years, who were living in the Jiangchuan Community, Shanghai, were enrolled and allocated to the three groups: a Childhood exposure group (n = 723; 60.08 ± 3.12 years old), an Adolescence exposure group (n = 710; 67.86 ± 2.49 years old) and a Young adulthood exposure group (n = 1002; 78.03 ± 3.86 years old) (P < 0.001; Table 2).
Clinical data for women with diabetes who were previously exposed to famine at each life stage.
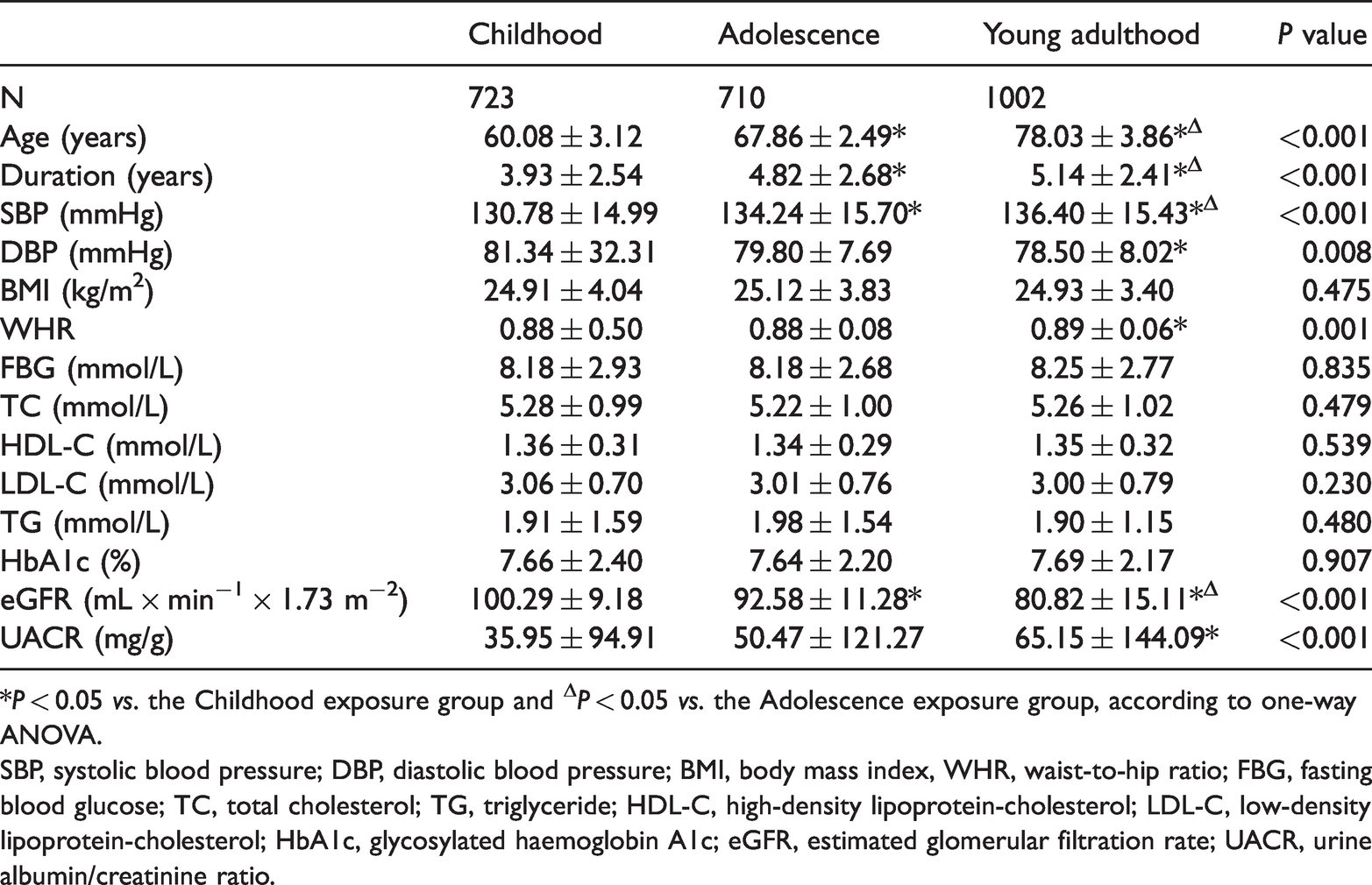
*P < 0.05 vs. the Childhood exposure group and ΔP < 0.05 vs. the Adolescence exposure group, according to one-way ANOVA.
SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index, WHR, waist-to-hip ratio; FBG, fasting blood glucose; TC, total cholesterol; TG, triglyceride; HDL-C, high-density lipoprotein-cholesterol; LDL-C, low-density lipoprotein-cholesterol; HbA1c, glycosylated haemoglobin A1c; eGFR, estimated glomerular filtration rate; UACR, urine albumin/creatinine ratio.
The duration of diabetes in the Childhood group was 3.93 ± 2.54 years, that in the Adolescence group was 4.82 ± 2.68 years, and that in the Young adulthood group was 5.14 ± 2.41 years (P < 0.001; Table 2). SBP gradually increased with age (P < 0.001), and the Young adulthood group had a significantly lower DBP than the Childhood group (P < 0.05) (Table 2). The WHR of the Young adulthood group (0.89 ± 0.06) was significantly higher than that of the Childhood group (0.88 ± 0.50) (P < 0.05). However, there were no significant differences in BMI, FBG, TC, TG, LDL-C, HDL-C or HbA1c among the three groups (Table 2).
eGFR and UACR in the three groups
The eGFR of the Childhood group (100.29 ± 9.18 mL × minute−1 × 1.73 m−2) was significantly higher than those of the Adolescence group (92.58 ± 11.28 mL ×minute−1 × 1.73 m−2) and the Young adulthood group (80.82 ± 15.11 mL ×minute−1 × 1.73 m−2) (both P < 0.05). In addition, the eGFR of the Adolescence group was significantly higher than that of the Young adulthood group (P < 0.05). Furthermore, the UACR of the Young adulthood group (65.15 ± 144.09 mg/g) was significantly higher than that of the Childhood group (35.95 ± 94.91 mg/g) (P < 0.05) (Table 2). Thirty-eight (5.26%) participants in the Childhood group, 159 (22.39%) in the Adolescence group and 794 (79.24%) in the Young adulthood exposure group had low eGFR (Table 3). Therefore, the prevalence of low eGFR was highest in the Young adulthood group.
Prevalences of low eGFR in the three exposure groups.

Relationship between the age of exposure to famine and subsequent eGFR in women with diabetes
Using the Adolescence group, which received the largest amount of food, as the reference group, the odds ratios (ORs) for the Childhood and Young adulthood groups were 0.19 (95% confidence interval [CI] 0.13, 0.28; P <0.05) and 13.23 (95% CI 10.48, 16.71; P <0.05), respectively (Table 4). After adjustment for the duration of diabetes and age, the ORs for the Childhood and Young adulthood groups were 1.08 (95% CI 0.67, 1.74; P > 0.05) and 1.60 (95% CI 1.07, 2.38; P < 0.05), respectively (Table 4, model 1). After further adjustment for SBP, DBP, BMI and WHR, the ORs for the Childhood and Young adulthood groups were 1.08 (95% CI 0.67, 1.74; P > 0.05) and 1.62 (95% CI 1.08, 2.41; P <0.05), respectively (Table 4, model 2). Finally, after further adjustment for FBG, TC, LDL-c, HDL-c, TG, HbA1c and UACR, the ORs for the Childhood and Young adulthood groups were 1.10 (95% CI 0.68, 1.78; P > 0.05) and 1.65 (95% CI 1.10, 2.48; P < 0.05), respectively (Table 4, model 3). Thus, the risk of low eGFR in women with diabetes who were exposed to famine during young adulthood was significantly higher than that of women who were exposed when adolescents.
Associations between exposure to famine during each life stage and subsequent low estimated glomerular filtration rate.

The Adolescence group was used as the reference. Data are odds ratios (95% confidence intervals), calculated using binary logistic regression models. *P < 0.05. Model 1 was adjusted for the duration of diabetes and age. Model 2 was adjusted the model 1 factors, plus systolic blood pressure, diastolic blood pressure, body mass index and waist-to-hip ratio. Model 3 was adjusted for the model 2 factors, plus fasting blood glucose, glycated haemoglobin, total cholesterol, triglyceride, high-density lipoprotein-cholesterol, low-density lipoprotein-cholesterol and urine albumin/creatinine ratio.
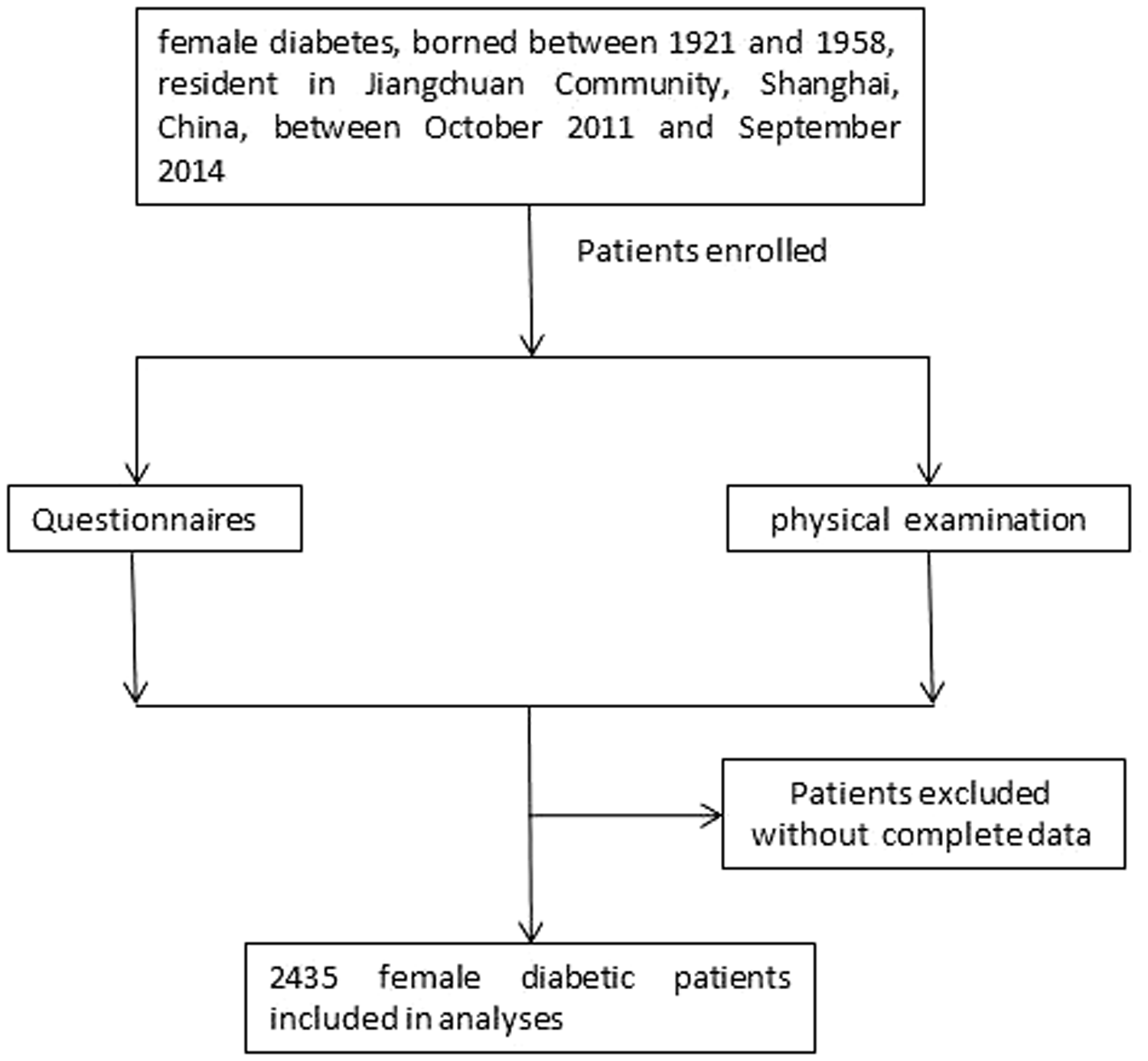
Screening and enrolment of the study participants.
Discussion
It is estimated that the Chinese famine caused 20,000,000 to 30,000,000 excess deaths.17,18 Food distribution during this 1959-to-1962 famine differed to that during the 1944-to-1945 Dutch and 1941-to-1945 Leningrad famines, which were caused by rapid declines in food supply.19,20 The food rationing system was strictly executed between 1959 and 1962 in Shanghai, as follows: 12.5 kg/month of food was supplied for 10-year-olds, 16 kg/month for 11- to 17-year-olds, and 12.5 kg/month for >18-year-olds, with children aged 0 to 9 years receiving an amount of food according to their age (Table 1). 12 However, the food supply for young adult women, who were working, was only 12.5 kg/month, which was a much smaller amount than that provided to adolescents. Furthermore, many young women were mothers during the famine, and would often have shared their food with their children, which would have further worsened the nutritional status of the young mothers. This disparity in food supply permits study of the effect of undernutrition during young adulthood on the renal function of adult women with diabetes.
In the present study, eGFR, calculated using the CKD-EPI formula, was used to assess renal function. Previous studies have demonstrated that the older a patient with diabetes is, the longer that patient's duration of diabetes is, and the higher that patient's blood pressure and UACR are, the greater the risk of a reduction in GFR.21,22 The present results are consistent with the findings of these studies. We measured eGFRs of 100.29±9.18, 92.58±11.28, and 80.82±15.11 mL × minute−1 × 1.73 m−2 in the Childhood, Adolescence, and Young adulthood groups, respectively. Thus, the lowest eGFR was in participants exposed to famine during young adulthood, and this was accompanied by the oldest age, the longest duration of diabetes, the highest SBP, and the highest UACR. Furthermore, the prevalences of low eGFR were 5.26%, 22.39%, and 79.24% in the Childhood, Adolescence, and Young adulthood groups, respectively. Thus, the prevalence for the Young adulthood group was higher than those for the Childhood and Adolescence groups. However, the BMI, TC, TG, LDL-c, HDL-c, FBG and HbA1c did not significantly differ among the groups, which may be because of progress in the health education and management of patients with diabetes.
To control for differences between the groups on the basis of differences in age, binary logistic regression analysis was performed and adjusted for age and other potential confounding variables. Using the Adolescence group, which received the largest food supply, as the reference group, we studied the effect of undernutrition at different ages on the risk of having a low eGFR in adult women with diabetes. After adjustment for the duration of diabetes, age, SBP, DBP, BMI, WHR, TC, TG, LDL-c, HDL-c, FBG, HbA1c and UACR, the ORs were 1.65 for the Young adulthood group and 1.10 for the Childhood group. Thus, the risk of poor renal function in women with diabetes following undernutrition in young adulthood is significantly higher than that following undernutrition during adolescence, and this is an independent risk factor.
Previous studies have shown that undernutrition predisposes toward metabolic disorders.23–25 However, the present study is the first to report that undernutrition during young adulthood is a risk factor for low eGFR in adult women with diabetes. Chen et al. 26 reported that exposure to famine during early life induces visceral adipose dysfunction in adult women. In addition, undernutrition in rats causes lower cholesterol content and disturbances in membrane microdomains in the kidney, which affects Ca2+ homeostasis and the activities of enzymes that generate important lipids, such as diacylglycerol kinase, phosphatidylinositol-4 kinase, phospholipase A2 and sphingosine kinase. 27 Therefore, imbalances in lipid concentrations may contribute to the development of chronic kidney disease. 26 However, the mechanism linking undernutrition and subsequent renal dysfunction may also involve Na+ pumps in the proximal tubule of the nephron. 28 The Na+/K+-ATPase activity in the kidneys of undernourished rats was 30% lower and its expression was 20% lower than those of control rats, whereas the activity of the ouabain-insensitive Na+-ATPase, which is responsible for the fine control of Na+ reabsorption, was three-fold higher. 28 However, the mechanism linking poor renal function in adult women with diabetes and undernutrition during young adulthood requires further study.
In China, the nutritional status of less affluent school-age children and adolescents has been improved by the Nutrition Plan for Elementary and Middle-school Students, 29 but this does not address the undernutrition of less affluent young women. The present findings show the effect of undernutrition in young adulthood on the risk of poor renal function in adult women with diabetes. Therefore, public health policy makers should also focus on the nutritional status of less affluent women aged 18 to 37 to reduce their risk of poor renal function in later life.
Conclusions
The present study is the first to show that undernutrition during young adulthood is an independent risk factor for poor renal function in adult women with diabetes. The mechanism underlying this finding should be investigated in the future. In addition, a focus of public health policy should be the improvement of nutrition in less affluent young women.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the National Natural Science Foundation of China [no. 81770716], the Natural Science Foundation of Shanghai Municipality [no. 13ZR1432600], the National Natural Science Foundation of China [no. 30871175], Minhang District Natural Science Foundation [no. 2016MHZ09] and Shanghai Minhang District Medical Specialty Construction Project [no. 2017MWTZ04].
Author contributions
Qiaojing Qin and Kaili Chang analysed the data and prepared the manuscript. Yong Gu contributed to the conception of the study. Xueguang Liu and Jianying Niu designed and revised the manuscript. Qing Wu and Weifeng Fan participated in the collection of data. Qiaojing Qin wrote the manuscript. All the authors read and approved the final version of the manuscript.