
Abstract
Introduction
We aimed to synthesise the experiences of people living with hand osteoarthritis (HOA) and the perceptions of clinicians and carers relating to the quality of life and treatment services.
Methods
We undertook a systematic search on MEDLINE, Embase, and CINAHL electronic databases for qualitative studies in HOA. We used the Critical Appraisal Skills Programme (CASP) checklist to assess methodological quality and thematically-synthesise the findings. We used GRADE-CERQual (Grading of Recommendations Assessment, Development, and Evaluation- Confidence in the Evidence from Reviews of Qualitative Research) to assess the quality of the evidence.
Results
We identified 13 studies involving people with HOA (288 women and 39 men, average age 61.4 years) and clinicians. Five themes were identified from studies involving people with HOA: i) My hands are painful whenever I use them; ii) It stops me doing everyday activities; iii) It stops me doing things I value; iv) It’s psychologically challenging and v) I find ways of doing things. The quality of evidence was moderate except for pain with low quality of evidence. Most studies were conducted in Europe and the United Kingdom with participants recruited predominantly from hospital settings. We were not able to synthesise the three studies that involved clinicians as each explored different topics of HOA. There were no studies that involved carers.
Conclusions
Our findings highlighted the impact of HOA in various areas of life and the need for personalised psychological support in practice.
Introduction
Osteoarthritis (OA) is a leading cause of musculoskeletal disability and socio-economic burden worldwide.1–3 This condition is caused by progressive cartilage and bone destruction, with narrowing of joint space. 3 Hand OA (HOA) typically involves the proximal inter-phalangeal (PIP), distal inter-phalangeal (DIP) and the first carpometacarpal joint (CMCJ).2,4 Depending on the joints affected, there are subgroups including nodal OA, erosive HOA (when the subchondral bone is eroded) and CMCJ OA. 2 HOA is defined by clinical or radiological criteria. The American College of Rheumatology4,5 definition includes hand pain or ache, stiffness and three of the other four clinical criteria: i) hard tissue enlargements in two or more DIP and PIP joints of the index and middle fingers, and CMCJ of both hands, ii) hard tissue enlargements in two or more DIP joints, iii) less than three swollen metacarpophalangeal joints, and iv) deformity in at least one of the DIP joints of the index and middle fingers, third PIP joints and CMCJ of both hands. 4 Radiologically, the Kellgren-Lawrence grading for the presence of osteophytes, joint space narrowing, and number of joints affected is used. 4
For patients, HOA is characterised by pain, joint stiffness and deformity, and reduced range of motion, grip strength, ability to perform activities of daily living, and quality of life.5,6
The severity of the condition is often increased by risk factors such as increasing age, women at menopause, genetic heritability, white population, obesity and smoking.4,6,8,9
Hand osteoarthritis (HOA) is highly prevalent between 40 and 60 years, especially in women.5–8 In a 2022 study involving 3588 adults with or at risk of symptomatic knee OA, 10 women were at greater risk (Prevalence Ratio, PR 2.16 [95% CI 1.76–2.64]). They had a modestly increased risk of radiographic hand OA (PR 1.18 [95% CI 1.10–1.27]) compared to men. There was no increased risk of incident radiographic hand OA (Risk Ratio 1.05 [95% CI 0.73–1.51]).
Treatment for HOA includes oral non-steroidal anti-inflammatory drugs, patient education, exercise, self-management, and splints.11–15 Surgery is considered for severe joint instability and deformity.16,17
Many qualitative studies have explored the experiences of people living with HOA.18–27 For an even better understanding of HOA, it is important to know the perspectives of clinicians, family members or carers of people with HOA. Carers are from the patients' immediate social environment (spouse or a family member) who could provide insight into patients’ experiences of living with HOA and how they cope and self-manage. We aimed to review the qualitative literature on the experiences of people living with HOA and the perceptions of clinicians and carers relating to the quality of life (physical, social and psychological well-being) and treatment services available.
Methods
We conducted a systematic review of qualitative research and reported in accordance with the ENTREQ guidelines. 28 The review protocol was prospectively registered on the PROSPERO database (CRD42019153378). 29 A patient representative was involved in the design and planning of the review.
A comprehensive search strategy was developed in collaboration with a health sciences librarian (NT) and was designed to capture all relevant articles about qualitative research on hand osteoarthritis (Supplementary file 1). In an initial search, the search strategy was applied to Medline (OvidSP), Embase (OvidSP) and CINAHL (EBSCO) from inception to 16th September 2022. An updated search was conducted on 21st February 2023. The search comprised title/abstract keywords and subject headings for osteoarthritis, hand and qualitative. References were exported to EndNote 20 (Clarivate, Philadelphia PA) for de-duplication.
Qualitative or mixed-method studies containing qualitative interviews relating to patient experiences and perceptions about treatment services, reported either by people with any type of HOA or clinicians or main carers were considered for inclusion. Systematic reviews, surveys, and studies not published as full article (conference abstracts, theses and dissertations), or those published in languages other than English were excluded.
Duplicates were removed and relevant studies identified from the search were imported into EndNote 20 referencing software for screening. Studies were independently screened by the title and abstract by two reviewers (BD & AB). This was followed by a full-text evaluation of the selected studies. References of relevant studies and review articles were also screened for studies that may potentially have met the inclusion criteria. Any disagreements were resolved through discussion with a third reviewer (CS) to include the relevant papers.
BD & AB independently assessed the methodological quality of the included studies using the Critical Appraisal Skills Programme (CASP) qualitative studies checklist. 30 Any discrepancies were resolved through discussion with another reviewer (CS) to reach a consensus.
Contextual information about the included studies (author, title, date, country of origin, research question, data collection, analytic method, sample and setting) was extracted by BD & AB. The data were cross-checked for accuracy and tabulated. The results sections of all included studies were imported into NVivo qualitative data analysis software version 12 31 for analysis.
BD & CS independently analysed the data following the three steps of thematic synthesis adapted from Sandelowski and Barroso 32 : (i) familiarisation with data involved reading and re-reading the study findings; (ii) line-by-line coding of the data within the results section including themes, sub-themes and quotes from the included studies; (iii) grouping of similar codes (from a minimum of two studies), abstracted inductively to final themes that were labelled to reflect the content of the data. A fourth reviewer (FT) reviewed the coding of each study to comment on any missed nuance and to reach a consensus about the final themes.
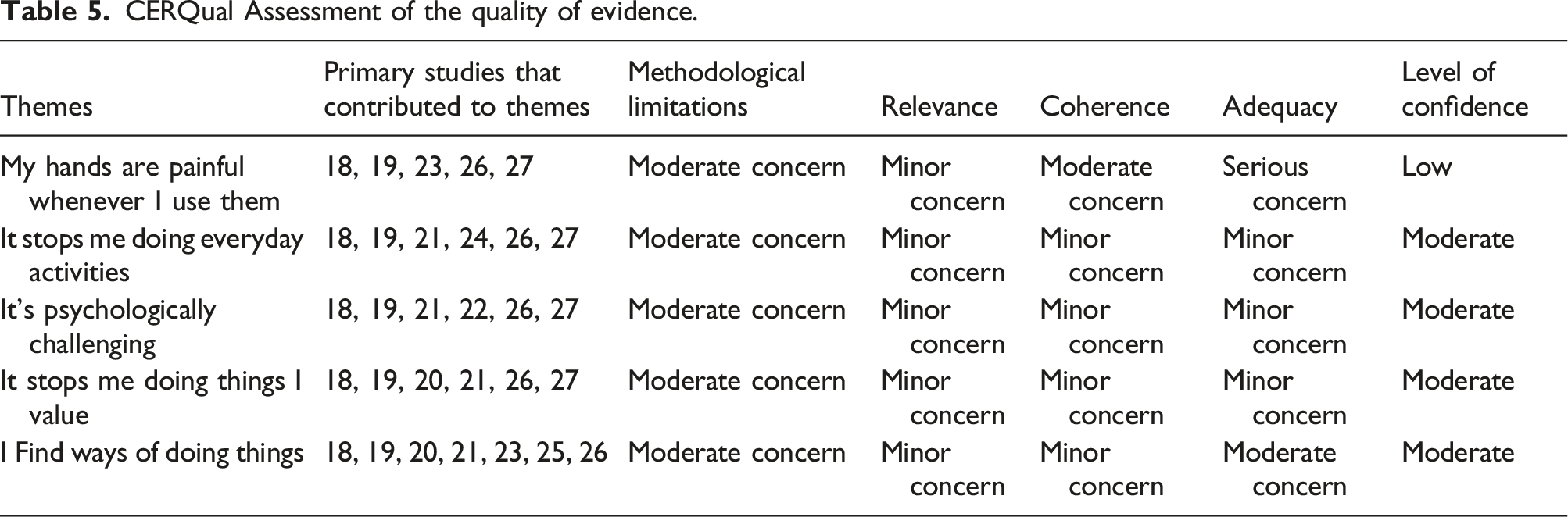
The confidence in each of the themes was assessed using the four components i) methodological limitations, ii) relevance, iii) coherence, and iv) adequacy of data of the GRADE-CERQual (Grading of Recommendations Assessment, Development, and Evaluation- Confidence in the Evidence from Reviews of Qualitative research) approach. 33 Methodological limitations refer to any concerns around the design and conduct of the primary studies that contribute to the review. Relevance refers to the applicability of the studies. Coherence refers to the extent of fit between the data from the primary studies and findings. Adequacy refers to the volume and richness of data supporting each finding. For each component, various levels of concern (none or very minor, minor, moderate and serious) that might influence the review findings were applied. Finally, an overall judgement of the quality of evidence in relation to the four components was made. The confidence ratings range from ‘Very low (when findings are less likely a reasonable representation of the topic of interest), ‘Low’, ‘Moderate’ and ‘High (when findings are highly likely a reasonable representation of the topic of interest).
Results
After reviewing 37 full-text citations, we identified 10 published reports from seven studies in people with HOA18–27 and three studies in clinicians.34–36 We didn’t find any qualitative studies that explored carers’ perceptions of HOA. Figure 1 shows the study selection process. PRISMA flow diagram.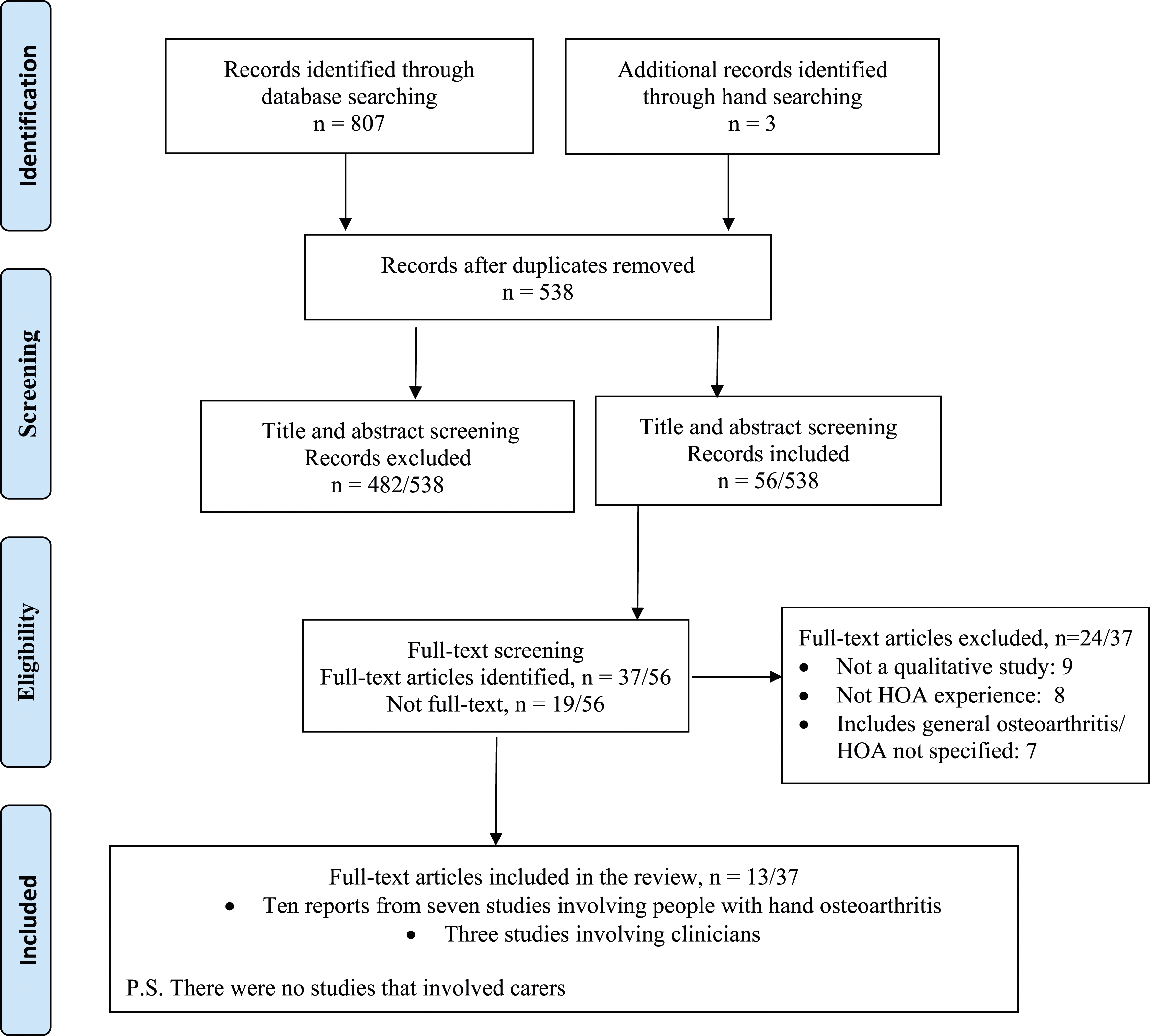
Characteristics of studies involving clinicians.
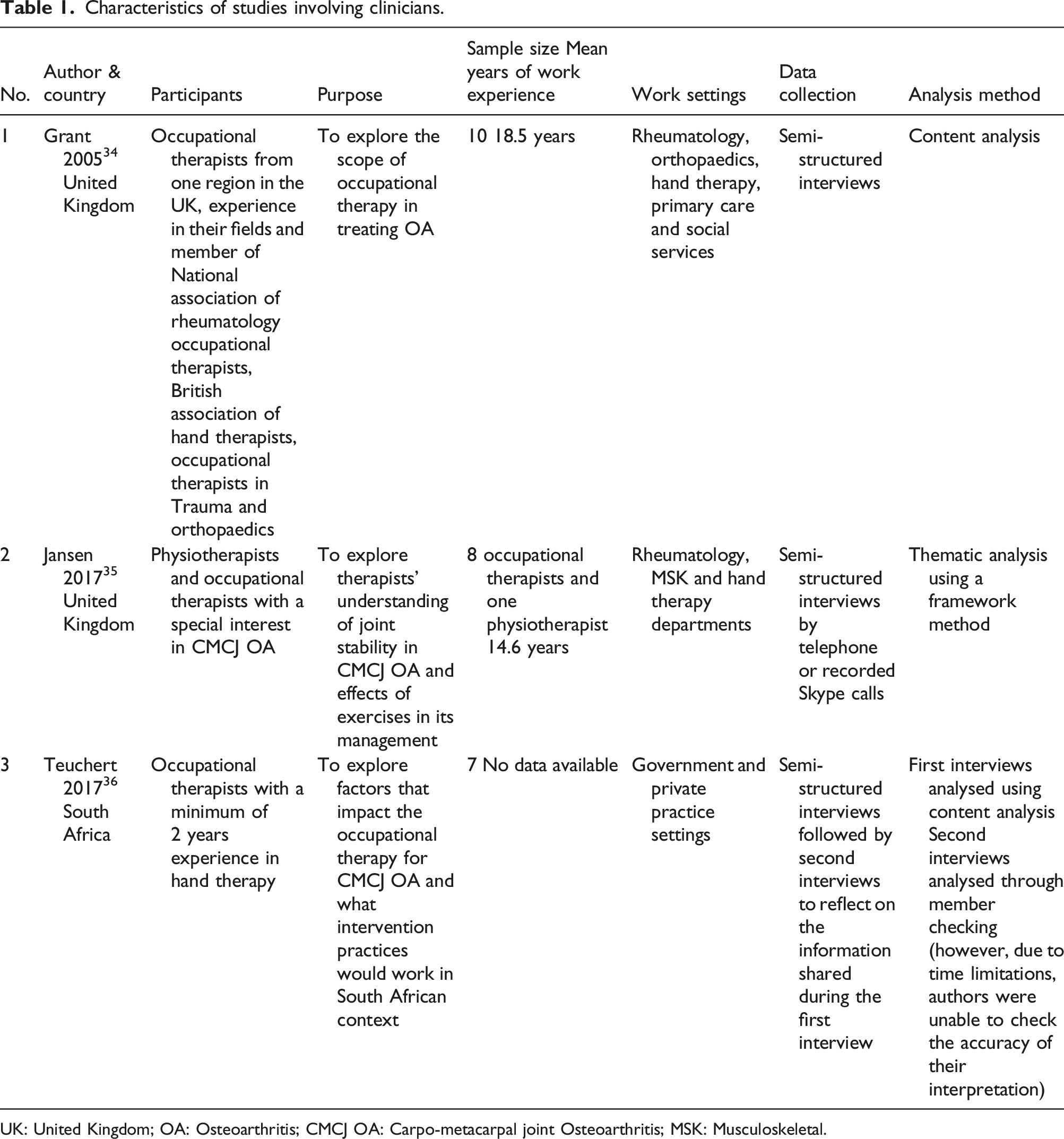
UK: United Kingdom; OA: Osteoarthritis; CMCJ OA: Carpo-metacarpal joint Osteoarthritis; MSK: Musculoskeletal.
Characteristics of included studies involving people with hand osteoarthritis.
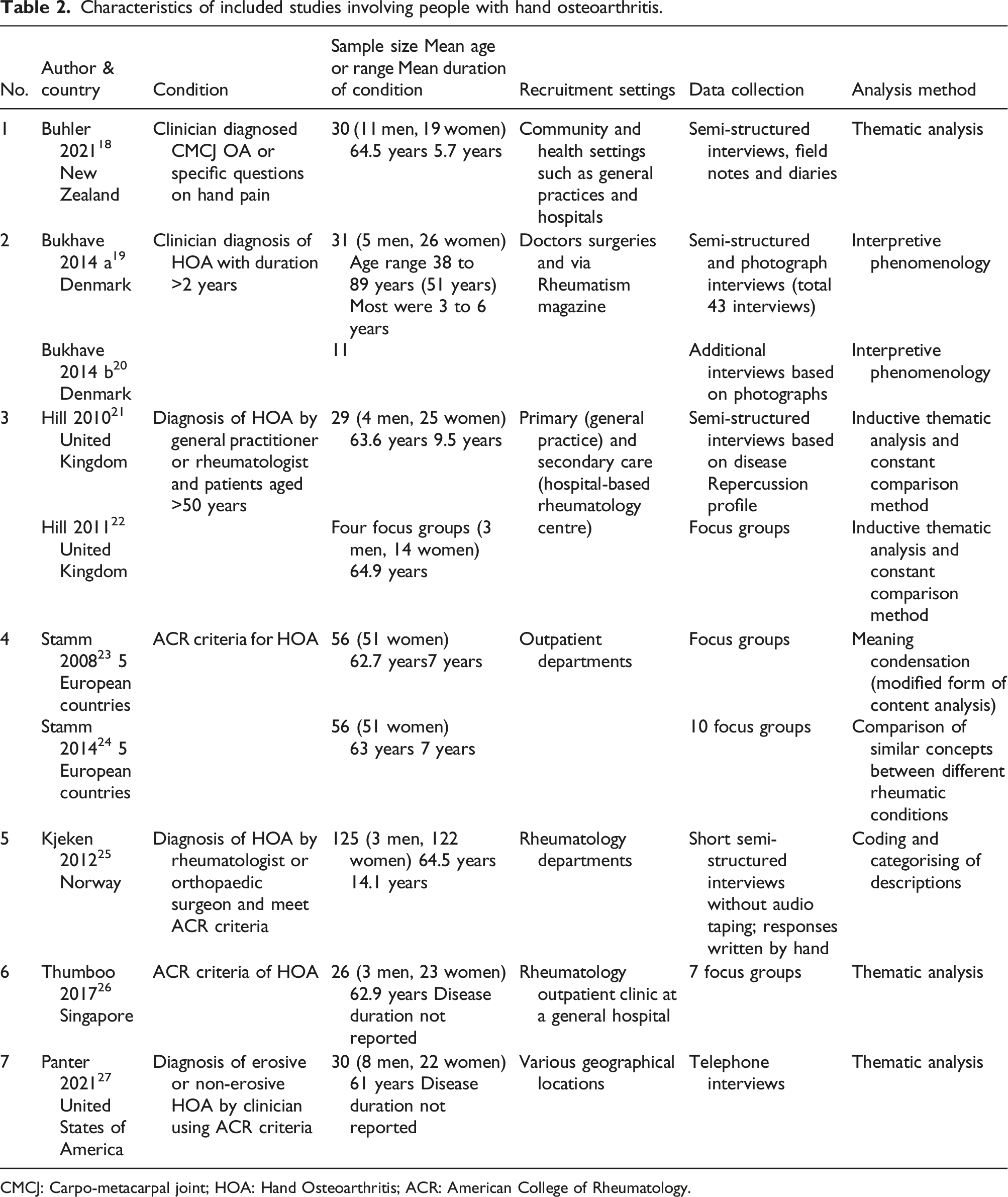
CMCJ: Carpo-metacarpal joint; HOA: Hand Osteoarthritis; ACR: American College of Rheumatology.
288 women and 39 men (total 327; men to women ratio: one to 7.4) with an average age of 61.4 years participated in the included studies. They were mostly recruited from primary care or rheumatology clinics in hospital settings. Four studies used ACR criteria for diagnosing HOA.23–27 Others were based on the clinicians’ diagnosis or asking specific questions about hand pain.18–22
Data collection was through face-to-face semi-structured interviews and focus groups. Duration of semi-structured interviews in the included studies ranged from 40 to 150 min. Focus groups ranged from 57 to 120 min. One study added diary entries and field notes, 18 another used participant-generated photographs of daily activities to guide the interviews 19 and another conducted interviews via telephone. 27 Interviews were audio recorded and transcribed verbatim in six out of seven studies.18–21,23,24,26,27 Focus group interviews 21 were both audio and video recorded in another report. 22 In one study 25 interviewers took written notes instead of audio recording. In the study that was conducted in five European countries,23,24 the focus group interview questions were formulated in German language that were forward and back-translated to local languages. In the Singapore-based study, focus groups were conducted either in English or Mandarin. 26 Interviews were audio taped, transcribed, and translated into English.
Thematic analysis was undertaken in four studies.18,21,22,26,27 The study that was conducted in five European countries23,24 used an adapted form of content analysis called ‘meaning condensation’ where the interview data were divided into meaning units and common concepts within the meaning units were then combined. Another study from Denmark19,20 used theoretical frameworks from social practice theory and critical psychology and was analysed using interpretative phenomenology.
The CASP quality assessment of studies involving people with hand osteoarthritis.
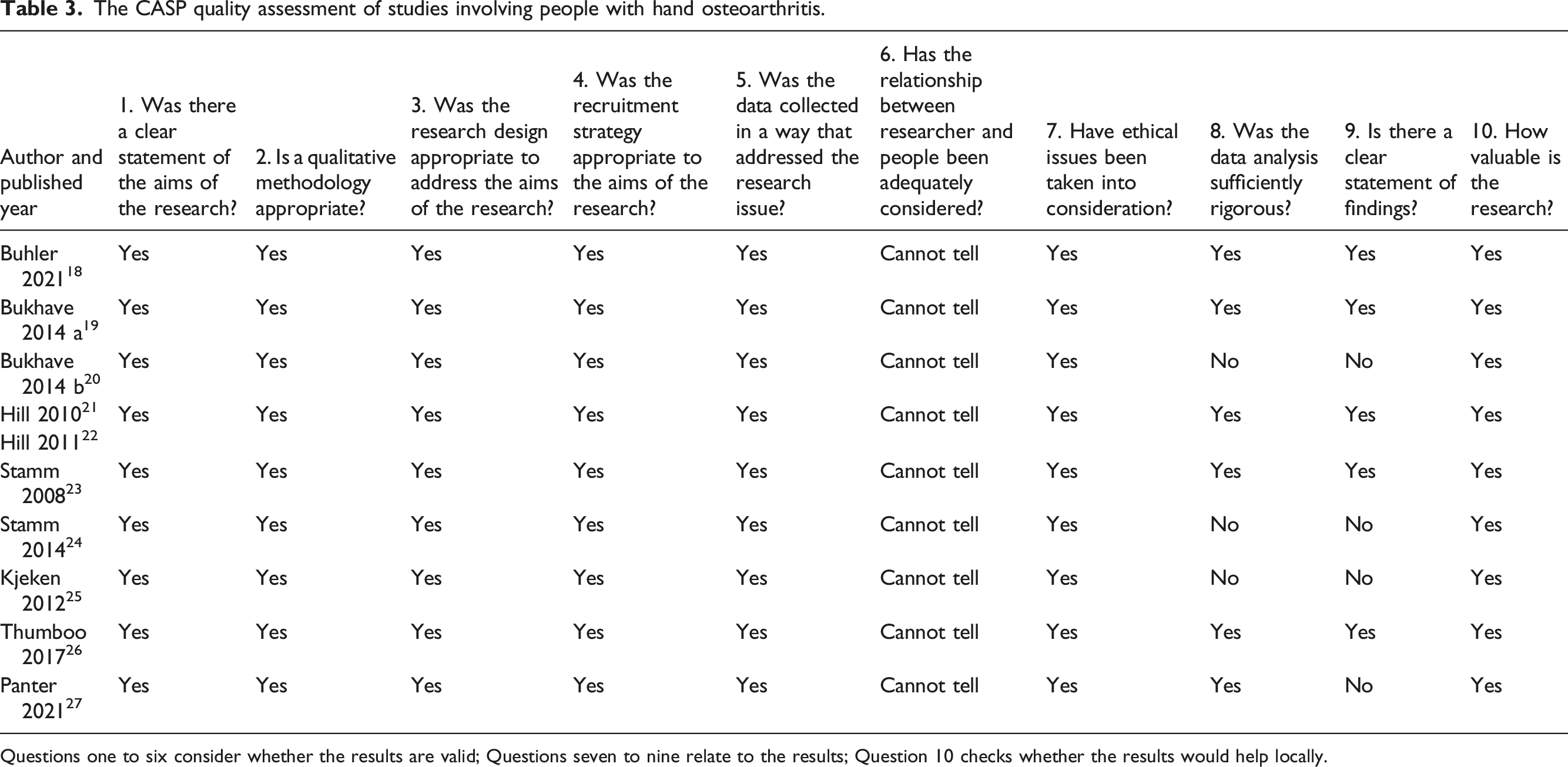
Questions one to six consider whether the results are valid; Questions seven to nine relate to the results; Question 10 checks whether the results would help locally.
Identification of emergent themes from the included studies assessment.
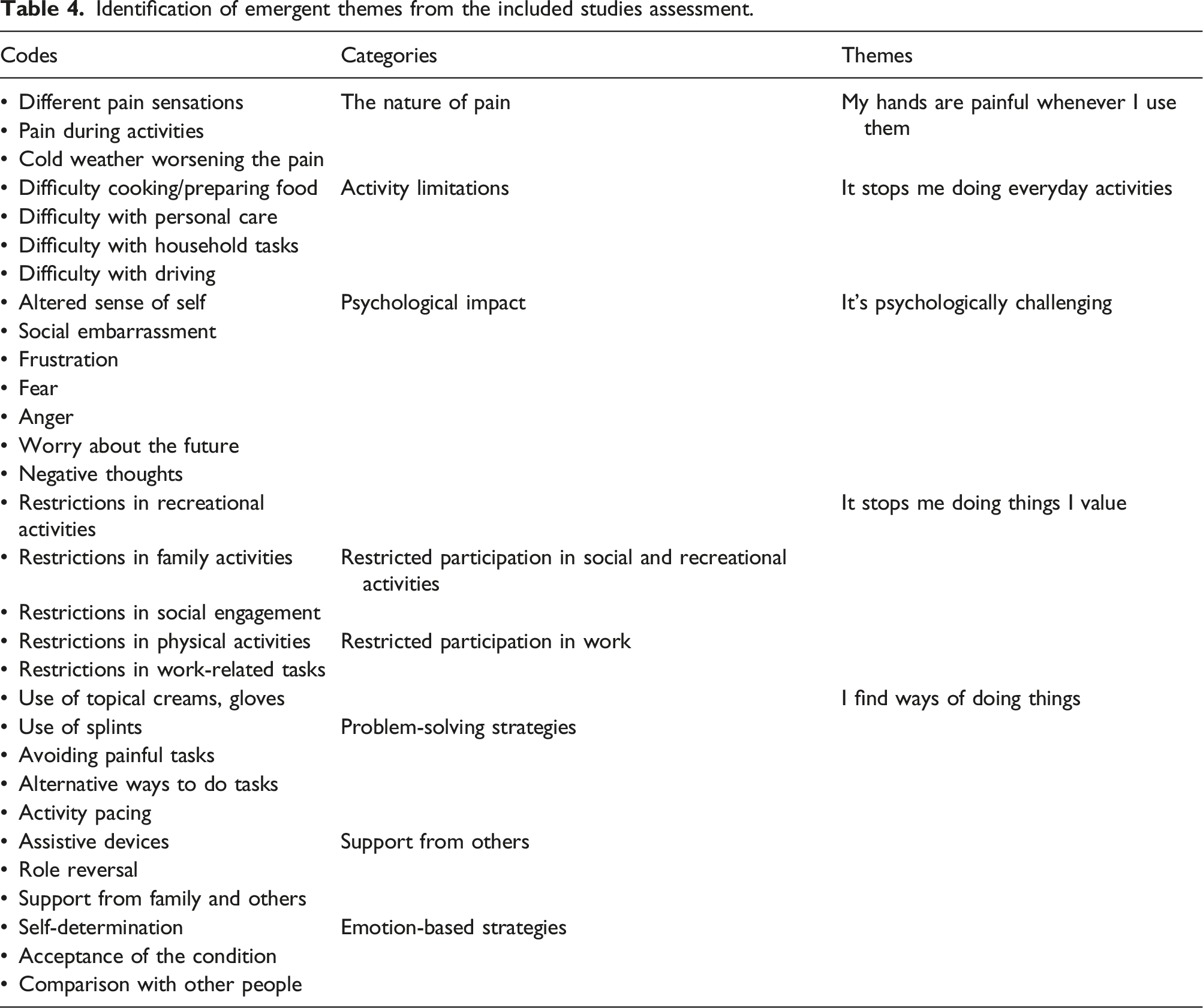
The themes identified were labeled as: i) My hands are painful whenever I use them; ii) It stops me doing everyday activities; iii) It stops me doing things I value; iv) It’s psychologically challenging and v) I find ways to keep doing things. The supportive quotes for each theme are presented in Supplementary file 2 (online only).
My hands are painful whenever I use them
This theme describes the pain experienced by people with HOA in the included studies.
There were five studies18,19,23,26,27 that captured peoples’ experiences with various symptoms such as pain, stiffness, swelling,26,27 reduced dexterity 18 and grip strength.18,27 However, these studies did not fully and richly cover these symptoms (including pain) with verbatim quotes. Pain was the most frequently reported problem.18,19,23,26,27 The types of pain sensations varied, with common descriptors such as ‘dull-ache’, ‘sore’, ‘knife-like’ or ‘burning’ or ‘killing pain’.18,23 Pain occurred throughout the activity18,23 and was unpredictable and fluctuating.18,19,26 Cold weather increased the intensity.18,23,26
It stops me doing everyday activities
This theme describes the difficulties that people with HOA had in activities relating to self-care and domestic and work life. HOA redefined what people were able to do, and people found a wide range of day-to-day activities (from self-care to work) either difficult or unable to perform.
The impact of HOA on activities of daily life was identified in six studies,18,19,21,24,26,27 prominently, personal care activities such as washing and bathing,18,21 dressing18,19,26 doing housework,18,21,26,27 using cutlery19,21,26 and driving.18,19,23 Difficulty cutting meat or vegetables19,21,27 or opening lids18,26 were also reported.
Activity limitations at work led to indirect consequences such as poor work productivity, early retirement, quitting the job and eventually, financial burden. Difficulty with job-related tasks due to functional difficulties, reduced work productivity and the need to change careers, retire earlier or even leave jobs were commonly reported.18,19,21,26,27 These indirectly led to financial stress on the individual and meant a change in their financial independence status.21,26
It stops me doing things I value
This theme describes the restrictions in taking part in hobbies, leisure and recreational activities as reported in five studies.18–21,26,27 People with HOA had restrictions participating in their own personal, family and social activities due to pain and disability. They gave up activities that were valued and meaningful to them such as fishing, bicycling, and going out with friends.
Hobbies such as gardening were restricted.18,19 People had difficulties participating in family activities such as caring for grandchildren or other family members18,19,26 and cooking for family. 26 Studies reported problems participating in social events such as dinners, skiing, going out and maintaining friendships.18,19,26,27 Activities such as biking were also restricted.18,19
It’s psychologically challenging
This theme refers to the psychological impact of HOA highlighted in five studies.18,19,21,22,26,27 HOA has a significant impact on psychological well-being. Pain and disability led to a variety of psychological responses such as anger, frustration, lack of confidence, worry, and suicidal thoughts. An altered sense of one’s self due to pain and inability to do things that they could do before was reported in three studies.18,21,26 Fear of becoming dependent on others due to functional difficulties led to frustration.18,19,21,26 Anger due to pain and disability18,26 and worry about the future18,21,26 were reported.
Two studies18,26 described negative thinking, including thoughts of self-harm due to pain and disability from HOA. People were embarrassed in public due to an inability to use a knife and fork or carry a shopping bag.21,26 Similarly, they were prone to dropping things that led to loss of confidence.18,19,26,27 Some felt shame and stigma (negative feelings and beliefs) about their finger deformities,21,24,26 although there were those who were not concerned about their hand appearance OA. 18
Three studies18,21,22,26 reported frustration as the major emotional response to the inability to carry out a task, pain, or the need to depend on others. Some people with HOA18,22,26 were frustrated due to a lack of support and understanding from their doctors/general practitioners (GPs). HOA was not always perceived as a serious problem and was often framed as part of ageing that has no cure.
Four studies18,19,21,26 reported that people chose not to ask for help for fear of losing their independence, or becoming dependent on others in simple tasks of daily living.
People with HOA were concerned about their future due to the disease's progressive nature and their reduced ability to carry out day-to-day activities.18,21,26
I find ways of doing things
This theme refers to the experiences of using coping strategies18–21,23,25,26 to manage pain and to achieve functional independence. People with HOA use a wide range of self-help strategies to manage pain and disability in their everyday lives. Strategies were mainly problem-solving (avoiding painful activities, finding alternate ways, using assistive devices) and less often, emotion-based (acceptance, faith, determination).
People wanted to be self-reliant and independent and avoided tasks that caused more pain.18,19,21 They used alternative ways to do a task18,19,21,23,26; used assistive devices19,20,23; or accepted assistance from others.19,21,25 Activity pacing or slowing down were reported in two studies.19,23 Some used emotion-focused strategies such as determination and faith,18,26 and acceptance and positive thinking to persevere despite pain. 23
People purchased assistive devices to maintain independence in cooking, eating, self-care, dressing and participation in social and leisure activities.19,22 However, some felt their knowledge and information needs on the availability and use of devices was unmet.19,21
People with HOA reported receiving support from family members 26 or others18,19 to assist them in daily activities. Some18,21 compared themselves positively to other people with worse arthritis symptoms. However, it is not clear if their perceptions helped inform decisions in adapting to HOA.
Level of confidence in the review findings
CERQual Assessment of the quality of evidence.
The review is reported as per ENTREQ guidelines (Supplementary file 3).
Discussion
This review aimed to synthesise the experiences of people living with HOA and the perceptions of carers and clinicians concerning the quality of life and treatment services. Following a systematic search, we identified seven (with 10 published reports) qualitative studies on people with HOA18–27 that were thematically synthesised. Three studies included clinicians who treat hand arthritis conditions.34–36 There were no qualitative studies that involved carers of people with HOA.
Studies in people with HOA indicated that HOA affects the person as a whole. Several issues that reduced their quality of life were pain, inability to do everyday tasks and participate in activities of personal value, and psychological challenges. People with HOA used various strategies to control their symptoms and to be functional inside and outside of the home. They also had feelings of shame, self-stigma and social embarrassment due to aesthetic issues from the joint deformities. Our review found that common impairments of HOA such as reduced grip strength, stiffness, fatigue and loss of dexterity and joint mobility were not explored from the patients’ perspective.
A few studies18,19,23,26,27 reported pain as the most troublesome symptom of HOA, requiring different coping strategies and living with it. However, we were not able to synthesise them due to a lack of in-depth exploration and patient quotes (for example nature of pain; how pain affects sleep, mental health, etc.). Chronic musculoskeletal pain (that includes arthritis pain) is no longer perceived as a single physical problem but rather a complex overlap of emotional, cultural, cognitive and neurological aspects interplaying with the joint pathology.37,38 Therefore, a broader understanding of the patients’ experience of HOA pain is required to provide holistic management in the context of patients’ expectations, beliefs, preferences and lifestyles. The variety of self-made coping strategies highlights how people were self-reliant and autonomous from their lived experiences with pain. These strategies are similar to people coping with OA in other joints.39,40
Studies in hip or knee OA41,42 have shown a significant association between psychological well-being and disability. The psychological impact of HOA from the patients’ perspective closely resonates with previous studies 43 and the experiences of people living with OA in other joints.39,40 Recent guidelines from the American College of Rheumatology 13 strongly recommend the use of structured self-efficacy and self-management programmes in building skills such as positive thinking, problem-solving and goal setting in HOA. Our findings highlight the need for a better understanding of the psychological impact of HOA and to consider a holistic treatment approach to help with the psychological symptoms.
Our review has some limitations. Firstly, we included studies published in the English language only. Secondly, we were able to identify only a small number of relevant studies (with three studies having six reports) with limited data for synthesis. Thirdly, the studies on people with HOA were from Europe and the UK, except one, 26 and were mainly recruited from hospital settings. Therefore, the overall findings might not reflect the experiences of living with HOA and health services in other ethnic groups, cultures and countries. Fourthly, the average age of participants in the included studies was 61.4 years and the symptom duration was above 5 years in four of the seven studies. The perspectives may differ in those who are newly diagnosed. Finally, studies used interviews with written notes, photographs, semi-structured interviews or focus groups for data collection. Hence there is a possibility that the nuances and essence of meanings are lost during synthesis. These limitations may impact the internal validity and transferability of the review findings.
Our review recommends that clinicians should appreciate the wide range of problems people have due to HOA in terms of individual and social life, and psychological well-being. The psychological impact of HOA must be acknowledged to facilitate personalised and ongoing formal support for those at risk. More qualitative work is required in the following areas: understanding pain experience, sleep problems, and other impairments such as reduced grip strength and dexterity; experiences of male participants with HOA; and perceptions of clinicians and carers or family members.
Conclusions
Our qualitative synthesis strengthens the evidence bases for the profound impact of HOA in terms of pain, being unable to do everyday tasks and things of value, and the psychological consequences from patients’ perspective. We recommend a personalised treatment approach to address the psychological challenges and provision of accessible and ongoing support for those in need.
Supplemental Material
Supplemental Material - Experiences of people with hand osteoarthritis and perceptions of clinicians and carers on quality of life and treatment services: A qualitative synthesis
Supplemental Material for Experiences of people with hand osteoarthritis and perceptions of clinicians and carers on quality of life and treatment services: A qualitative synthesis by Cynthia Srikesavan, Benjamin Dean, Francine Toye, Alex Bolt and Neal Thurley in Hand Therapy
Footnotes
Author contributions
CS and BD: conceptualisation, methodology, writing, Reviewing and editing of the manuscript versions; FT: review and consultation of themes and editing of the manuscript versions; AB: methodology, writing, reviewing and editing of the manuscript versions.
NT: developed the search strategy and syntax, advised on the databases to use, ran and re-ran the searches, identified papers for inclusion, and reviewed the pre-submission manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Benjamin Dean discloses receipt of financial support for research, authorship, and publication from British Medical Association Doris Hiller grant.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.