
Abstract
Background:
Gastric cancer (GC) is the fifth most common cancer and the fourth leading cause of cancer-related mortality worldwide. The liver is the primary metastatic site, and the prognosis of gastric cancer with liver metastasis (GCLM) remains poor. While transarterial chemoembolization (TACE) and hepatic arterial infusion chemotherapy (HAIC) are used for liver cancer, their roles in GCLM remain underexplored.
Objectives:
This study aimed to evaluate the efficacy and safety of drug-eluting bead TACE (DEB-TACE) combined with HAIC in patients with unresectable GCLM.
Design:
This was a retrospective, single-center cohort study.
Methods:
We retrospectively analyzed 62 patients with GCLM treated at Peking University Cancer Hospital between July 2018 and June 2023. Patients underwent 135 sessions using either HepaSphere beads plus HAIC-FOLFOX (HEPA-HAIC, n = 33) or DC bead plus HAIC-FOLFOX (DCB-HAIC, n = 29). The primary endpoint was median overall survival (mOS); secondary endpoints included median hepatic progression-free survival (mhPFS), median progression-free survival (mPFS), tumor response, and safety.
Results:
Among the patients (53 male, 9 female), 75.8% had intestinal-type cancer. Over 95% underwent prior treatments. The mOS was 10.7 months in both groups. The HEPA-HAIC cohort achieved longer mhPFS (8.6 vs 7.6 months) and mPFS (5.7 vs 4.4 months), though not statistically significant. Objective response rate and disease control rate were similar (30.3%/75.8% vs 31.0%/75.9%). Propensity score matching confirmed these findings. Univariate Cox regression suggested primary tumor location and carcinoembryonic antigen were prognostic for hPFS and OS, respectively. No treatment-related deaths occurred. Common adverse events (AEs) were transaminase elevation and pain. Nausea, vomiting, and severe pain were significantly less frequent with HEPA-HAIC (5.6% vs 31.7%, p = 0.001; 4.2% vs 31.7%, p < 0.001; 8.3% vs 22.2%, p = 0.01).
Conclusion:
DEB-TACE plus HAIC was feasible and demonstrated intrahepatic disease control with acceptable tolerability in unresectable GCLM; HEPA-HAIC showed a favorable safety profile.
Plain language summary
Background:
Stomach cancer is a serious illness. When it spreads to the liver, treatment options are limited and outcomes are often poor Treatments that deliver therapy directly to the liver through its blood supply are commonly used for primary liver cancer, but their value for liver tumors from stomach cancer is not well understood. In this study, we examined whether combining two liver-directed treatments, one blocks liver tumor blood flow while releasing chemotherapy drugs, and the other delivers chemotherapy directly into the liver artery, can improve outcomes for patients whose liver tumors cannot be surgically removed.
Methods:
We reviewed the records of 62 patients with stomach cancer that had spread to the liver who were treated at Peking University Cancer Hospital between July 2018 and June 2023. All patients received a combination of liver artery treatments: drug-releasing beads used to treat liver tumors, together with direct chemotherapy infusion into the liver artery. Two types of drug-releasing beads (HepaSphere and DC Bead) were compared. We evaluated how long patients lived, how well the tumors were controlled, and what side effects occurred.
Results:
Most patients had already tried other cancer treatments before this therapy. On average, patients lived about 11 months after starting treatment, and this was similar in both groups. Tumor control and response were also similar. No deaths were related to treatment. The most common side effects were temporary liver enzyme increases and pain. Nausea, vomiting, and severe pain occurred less often in patients treated with HepaSphere.
Conclusion:
Combining drug-releasing liver artery treatment with direct chemotherapy infusion may be a safe and helpful option for patients with stomach cancer that has spread to the liver and cannot be surgically removed. HepaSphere showed better tolerability, suggesting it may be a safer choice for some patients.
Keywords
Introduction
Gastric cancer (GC) is a significant global health concern, ranking as the fifth most commonly diagnosed malignancy and the fourth leading cause of cancer-related deaths worldwide. 1 The highest tumor burden occurs in Asia, particularly in China, where GC is the third leading cause of cancer-related mortality, following lung cancer and hepatocellular cancer.2,3 Over 80% of GC patients are diagnosed at an advanced stage due to nonspecific early symptoms. The liver is a common site for distant metastases, with liver involvement observed in up to 50% of advanced cases 4 and liver metastasis is a critical prognostic factor in GC.5–7 However, most patients with gastric cancer liver metastases (GCLM) present with multiple hepatic lesions and often involve concurrent extrahepatic spread, such as to lymph nodes, bone, or other organs,8,9 making the majority ineligible for curative surgical resection. 10
Systemic chemotherapy is the standard treatment for patients with unresectable or surgery-intolerant GCLM, achieving a median overall survival (mOS) of approximately 13 months.11,12 However, this outcome is unsatisfactory. Systemic chemotherapy often fails to achieve effective intrahepatic drug concentrations and demonstrates limited efficacy in controlling liver lesions, particularly in patients with liver-dominant or liver-only disease. Although recent advances in targeted therapy, immunotherapy, and multidisciplinary treatment approaches have improved outcomes in advanced GC,13,14 the management of unresectable GCLM remains a significant clinical challenge.
Locoregional therapies such as transarterial chemoembolization (TACE) and hepatic arterial infusion chemotherapy (HAIC) are gaining attention for their potential to enhance intrahepatic tumor control. These intra-arterial therapies exploit the liver’s unique dual blood supply, where normal liver tissue is primarily perfused by the portal vein, while metastases rely predominantly on the hepatic artery. This anatomical distinction enables selective delivery of chemotherapeutic agents to tumor tissue, thereby increasing local drug exposure and minimizing systemic toxicity.15,16 TACE utilizes this arterial blood supply to deliver chemotherapeutic agents along with embolic materials, inducing tumor ischemia and necrosis while reducing systemic exposure. 16 Drug-eluting bead TACE (DEB-TACE), an advancement over conventional TACE, employs microspheres (e.g., HepaSphere or DC Bead) that load and gradually release chemotherapeutic drugs in a controlled and sustained manner, resulting in improved local drug concentration and reduced toxicity.17,18 In GCLM, DEB-TACE has demonstrated improved response rates and reduced toxicity. 19 HAIC involves continuous or intermittent chemotherapy infusion directly into the hepatic artery via a catheter or port system, preserving hepatic perfusion and minimizing ischemic injury. It has also shown encouraging results in patients with GCLM.20,21 While both DEB-TACE and HAIC are well-established for hepatocellular carcinoma (HCC) and colorectal cancer liver metastases (CRLM),22–24 their roles in GCLM are not yet well defined. This study aims to evaluate the efficacy and safety of DEB-TACE combined with HAIC in patients with unresectable GCLM. Additionally, the impact of different drug-eluting beads on treatment response and toxicity profiles is accessed.
Methods
Study design and patient selection
A retrospective study was conducted at Peking University Cancer Hospital from July 2018 to June 2023, involving 67 patients treated with DEB-TACE combined with HAIC for GC with predominant hepatic metastases, which primarily determined patient outcomes over extrahepatic disease. Inclusion criteria were: age 18–75 years, GCLM confirmed by MRI, CT, or liver biopsy, at least one measurable liver tumor, Eastern Cooperative Oncology Group performance status <2, and Child-Pugh liver function classification A or B. Exclusion criteria included history of other malignancies or concurrent cancers or pregnancy. Patients with potential brain metastasis, peritoneal metastasis, ovarian metastasis, or other conditions unlikely to benefit from D‑TACE and HAIC. The reporting of this study conforms to the European Society for Medical Oncology (ESMO) guidance for reporting oncology real-world evidence (GROW). 25 The completed ESMO GROW reporting checklist is provided as a Supplemental File (Table S1).
Treatment protocol
Preoperative contrast-enhanced abdominal CT or MRI was performed to evaluate the size, location, and vascular supply of the tumor. The Hepasphere mixture was prepared by injecting 2 mL of normal saline containing 40–60 mg of epirubicin and 8 mL of nonionic isotonic contrast medium (Visipaque; 270 mg/mL iodixanol) into a vacuum-sealed vial containing HepaSphere microspheres (Merit Medical, Salt lake city, UT, USA; 30–60 μm). For the DC Bead mixture, the microspheres were drawn into a 20 mL syringe and allowed to settle upright for 5 min. The supernatant was discarded, and the DC Bead were mixed with 10 mL of normal saline containing 40–60 mg epirubicin, followed by 10 mL of nonionic isotonic contrast medium was added. The mixture was shaken and left to stand for approximately 30 min to ensure complete epirubicin absorption by the microspheres.
Under local anesthesia, the femoral artery was punctured using the Seldinger technique. Under fluoroscopic guidance, angiography of the celiac and hepatic arteries was performed to assess the number, size, location of the tumors, as well as their feeding arteries and any vascular variations. In some cases, superior mesenteric artery angiography was also performed. The tumor-feeding artery was super-selectively catheterized using a coaxial microcatheter. The prepared drug-microsphere mixture was then injected into the tumor-feeding artery. Additional embolic agents such as gelatin sponge particles or embolization microspheres were used as needed to achieve complete embolization. Upon completion of DEB-TACE, repeat angiography was performed to confirm achievement of the embolization endpoint, defined as angiographic near stasis of tumor-feeding arteries with marked slowing of antegrade flow and substantial reduction of tumor blush, while preserving segmental or lobar hepatic arterial patency. Complete arterial stasis was intentionally avoided to minimize ischemic liver injury and to allow subsequent HAIC. Protective embolization with microcoils was performed to prevent reflux of high-concentration chemotherapeutic agents into gastrointestinal arteries, which could otherwise result in ulcers or bleeding. An arterial catheter was retained for HAIC. The tip of a 2.4–2.7 French microcatheter was positioned in the proper hepatic artery, with placement confirmed using digital subtraction angiography (Innova 4100IQ; General Electric Company, Boston, MA, USA). The catheter was securely fixed to the skin to prevent displacement. An arterial infusion pump was connected to the microcatheter to administer HAIC on the ward. The HAIC regimen consisted of a 4-h infusion of oxaliplatin (OXA) at 60–85 mg/m2, followed by a 2-h intravenous infusion of leucovorin (CF) at 200 mg/m2, and then a 20-h continuous infusion of 5-fluorouracil at 1.2 g. Treatment cycles were repeated every 4–6 weeks until intrahepatic disease progression, intolerable toxicity, or voluntary treatment withdrawal by the patients. Tyrosine kinase inhibitors (TKIs) or trastuzumab were initiated 3 days after each DEB-TACE plus HAIC session if no contraindications were present. To minimize peri-procedural risk, these agents were routinely withheld for 3 days prior to subsequent interventional treatments. All targeted therapies were administered orally at standard recommended doses. For immunotherapy, PD-1/PD-L1 inhibitors were administered intravenously starting 3 days post-intervention if no contraindications existed and continued every 2–3 weeks following standard protocols.
Follow-up
All information was obtained from patients’ medical records or through telephone interviews. The follow-up period continued until death or until December 31, 2024. During follow-up, five patients were lost to follow-up shortly after treatment and before any evaluable post-treatment assessment could be obtained. As a result, these 5 patients were excluded from all subsequent analyses, and the final study population consisted of 62 patients.
Efficacy and safety evaluation
Tumor response was evaluated every 6–8 weeks after DEB-HAIC therapy using contrast-enhanced CT or MRI. Two experienced radiologists, each with over 10 years of experience, independently performed the assessments. Hepatic progression-free survival (hPFS) was defined as the time from the first DEB-HAIC treatment to liver-specific disease progression or death. Progression-free survival (PFS) was defined as the time from the first DEB-HAIC to progression at any site or death. Overall survival (OS) was the interval from treatment initiation to death or last follow-up. Objective response rate (ORR) and disease control rate (DCR) were assessed according to both of the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST1.1) and the modified Response Evaluation Criteria in Solid Tumors (mRECIST) which is based on the change in the viable (contrast-enhancing) portion of lesions on dynamic contrast-enhanced CT/MRI in order to better capture treatment-induced devascularization/necrosis following embolization-based intra-arterial therapies.
AEs were recorded during hospitalization and for 30 days following each treatment cycle. All AEs, except pain, were graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events (NCI-CTCAE), version 5.0. Pain severity was evaluated separately using the Numeric Rating Scale.
Statistical analysis
Propensity score matching (PSM) was employed to mitigate baseline covariate imbalance between HepaSphere beads plus HAIC-FOLFOX (HEPA-HAIC) and DC bead plus HAIC-FOLFOX (DCB-HAIC) groups for the subsequent treatment efficacy analysis. Propensity scores were estimated using a multivariable logistic regression model. Baseline variables with a p value ⩽0.5 in the pre-matching comparison were included as covariates in the propensity score model to avoid omission of potential confounding factors. Patients were matched at 1:1 ratio using the nearest-neighbor matching method with a caliper width of 0.05 and without replacement. The survival data were estimated using Kaplan–Meier method, and prognostic factors were analyzed with Cox regression model. Quantitative data were expressed as mean ± standard deviation, while qualitative data were reported as frequencies and percentages (n, (%)). A p value of <0.05 indicated statistically significant difference. All statistical analyses were performed using IBM®SPSS® software (v.27.0; IBM Corporation, Armonk, NY, USA).
Results
Patients’ baseline characteristics
Of 67 initially enrolled patients with histologically confirmed GCLM who received DEB-TACE combined with HAIC at Peking University Cancer Hospital & Institute, 5 were lost to follow-up before any post-treatment evaluation and were excluded from the analysis. The remaining 62 patients constituted the evaluable cohort for efficacy and survival analyses. There was no statistically significant difference in the distribution of enrollment time between HEPA-HAIC and DCB-HAIC. The baseline characteristics are summarized in Table 1. Among these patients, 53 (82.8%) were male, and 37 (59.7%) were aged ⩽65 years. Most primary tumors (80.6%, n = 50) were located in the proximal or middle stomach, and 75.8% (n = 47) were classified as intestinal type according to the Lauren classification. Poorly differentiated tumors were observed in 45 patients. Molecular profiling showed that 24 patients were positive for PD-L1, HER2, or microsatellite instability. Synchronous liver metastases were identified in 49 patients (79.0%) while metachronous liver metastases were shown in 13 patients (21%). Only 25 (40.3%) had undergone primary tumor resection and 42 (67.7%) presented with elevated carcinoembryonic antigen (CEA) levels. Hepatitis was reported in 23 patients (37.1%). Liver metastases were predominantly multiple, with 98.4% of patients harboring more than one lesion; 72.6% had metastatic lesions ⩾3 cm in diameter. Although extrahepatic metastases were detected in 48 patients, liver metastases remained the dominant disease burden and primary therapeutic target. In terms of treatment history, only 4.8% of patients were treatment-naïve, whereas 46.8% had received two or more prior lines of systemic therapy. Regarding systemic co-therapy, a total of 28 patients received targeted therapy, immunotherapy, or both during the treatment. Among TKIs used (Table 2), Apatinib was the most frequent (27.4%, n = 17), with a higher utilization rate in DCB-HAIC group (41.4%) compared to HEPA-HAIC group (15.2%). Other targeted agents included lenvatinib, fruquintinib, and trastuzumab. Immunotherapy consisted primarily of PD-1 inhibitors, including nivolumab (8.1%), camrelizumab (4.8%), sintilimab (1.6%), and tislelizumab (1.6%), as well as the PD-L1 inhibitor envafolimab (3.2%). PSM was conducted to reduce potential baseline covariate imbalance between HEPA-HAIC and DCB-HAIC groups in the comparative treatment efficacy analyses. After 1:1 nearest-neighbor matching without replacement, baseline characteristics were well balanced between these two groups, with no statistically significant differences observed across the matched variables (Table 3).
Baseline characteristics of patients before PSM.

CEA, carcinoembryonic antigen; DCB-HAIC, DC bead plus HAIC-FOLFOX; ECOG, Eastern Cooperative Oncology Group; HEPA-HAIC, HepaSphere beads plus HAIC-FOLFOX; MSS, Microsatellite Stable; PSM, propensity score matching.
Targeted therapy and immunotherapy used in the study.

DCB-HAIC, DC bead plus HAIC-FOLFOX; HEPA-HAIC, HepaSphere beads plus HAIC-FOLFOX; TKI, tyrosine kinase inhibitors.
Baseline characteristics of patients after PSM.

CEA, carcinoembryonic antigen; DCB-HAIC, DC bead plus HAIC-FOLFOX; MSS, Microsatellite Stable; ECOG, Eastern Cooperative Oncology Group; HEPA-HAIC, HepaSphere beads plus HAIC-FOLFOX; PSM, propensity score matching.
Efficacy and prognostic factors
The median follow-up duration for the cohort was 10.8 months (range: 0.7–64.3 months). Treatment responses were evaluated approximately 8 weeks after therapy using both RECIST1.1 and mRECIST. According to RECIST 1.1, no patients achieved complete response (CR); 17 patients (27.4%) achieved partial response (PR), 30 (48.4%) had stable disease (SD), and 15 (24.2%) experienced progressive disease (PD), yielding ORR of 27.4% and DCR of 75.8%. ORR and DCR were comparable between HEPA-HAIC and DCB-HAIC groups (ORR: 27.3% vs 27.6%, p = 0.978; DCR: 75.8% vs 75.9%, p = 0.992). Using mRECIST, 2 patients (3.2%) achieved CR, 17 (27.4%) achieved PR, 28 (45.2%) had SD, and 15 (24.2%) had PD, corresponding to ORR of 30.6% and DCR of 75.8%. Similarly, no significant differences were observed between HEPA-HAIC and DCB-HAIC groups (ORR: 30.3% vs 31.0%, p = 0.950; DCR: 75.8% vs 75.9%, p = 0.992). Importantly, response rates and between-group comparisons were highly consistent across RECIST 1.1 and mRECIST analyses, indicating that the choice of response criteria did not materially affect the comparative efficacy results (Table 4).
Response evaluation before PSM.
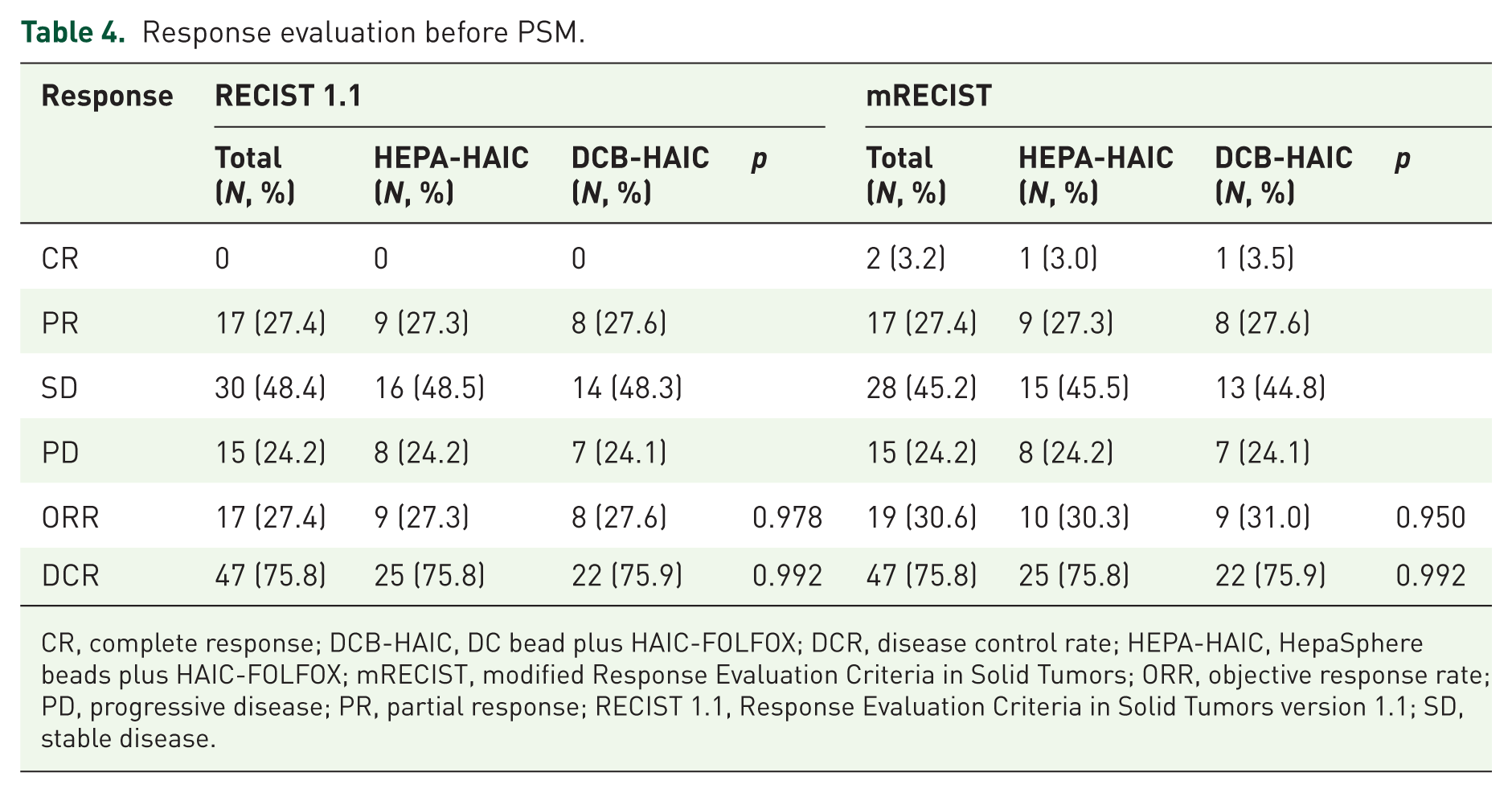
CR, complete response; DCB-HAIC, DC bead plus HAIC-FOLFOX; DCR, disease control rate; HEPA-HAIC, HepaSphere beads plus HAIC-FOLFOX; mRECIST, modified Response Evaluation Criteria in Solid Tumors; ORR, objective response rate; PD, progressive disease; PR, partial response; RECIST 1.1, Response Evaluation Criteria in Solid Tumors version 1.1; SD, stable disease.
The median hPFS (mhPFS) following the first treatment was 7.6 months (95% CI: 6.7–8.9 months) while the median PFS (mPFS) was 4.6 months (95% CI: 3.1–6.1 months; Figure 1) and the mOS was 10.7 months (95% CI: 8.2–13.2 months). Subgroup analysis revealed that the HEPA-HAIC group had numerically longer mhPFS and mPFS, though the differences were not statistically significant (mhPFS: 8.6 vs 7.6 months, p = 0.457; mPFS: 5.7 vs 4.4 months, p = 0.341). The mOS was identical between the two groups at 10.7 months.

Kaplan–Meier curves for hPFS (a), PFS (b) and OS (c) in patients.
After PSM, HEPA-HAIC group demonstrated mhPFS of 8.4 months and mPFS of 4.6 months, compared with 7.2 and 4.9 months in DCB-HAIC group. The corresponding mOS values were 9.4 and 10.0 months, respectively (Figure 2). None of these comparisons showed statistically significant differences.

Kaplan–Meier analysis of hPFS (a), PFS (b), and OS (c) between post-PSM groups.
In terms of prognostic factors, univariate Cox regression analysis showed that the primary tumor site, particularly tumors located in the middle stomach, was significantly associated with hPFS (p < 0.05; Table 5). As only one variable reached statistical significance in univariate analysis, a multivariable model for hPFS was not constructed. For OS, univariate analysis identified CEA level as a significant predictor (p = 0.047). Variables of clinical relevance were subsequently entered into a multivariable Cox proportional hazards model; however, no independent prognostic factors for OS were identified in the multivariable analysis (Table 6).
Univariate analyses of the prognostic factors for hPFS and PFS before PSM.

CEA, carcinoembryonic antigen; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; hPFS, hepatic progression-free survival; HR, hazard ratio; PFS, progression-free survival; PSM, propensity score matching.
Univariate and multivariate analyses of the prognostic factors for OS before PSM.

CEA, carcinoembryonic antigen; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; OS, overall survival; PSM, propensity score matching.
Safety assessment
A total of 135 treatment sessions were administered to all patients. Treatment-related toxicities were systematically evaluated and summarized in Table 7. The most prevalent AEs were abdominal pain (47.4%), elevated serum liver enzymes (42.9%) and hyperbilirubinemia (32.6%). Severe toxicities, classified as NCI-CTCAE grade 3–4, included elevated serum liver enzymes (9.6%) and hypertension (2.2%). Severe abdominal pain with a score ⩾7 was the most frequent AE, reported in 20 patients (32.3%). Nausea, vomiting, and abdominal pain occurred significantly more frequently in patients treated with DCB-HAIC. In addition, no serious vascular complications were observed despite repeated arterial punctures. Importantly, no treatment-related deaths occurred, and all toxicities were successfully managed with appropriate interventions.
Comparison of AEs between two groups before PSM.

AEs, adverse events; DCB-HAIC, DC bead plus HAIC-FOLFOX; HEPA-HAIC, HepaSphere beads plus HAIC-FOLFOX; PSM, propensity score matching.
Discussion
GCLM remains a clinically challenging scenario due to poor prognosis and limited therapeutic options. Conventional systemic chemotherapy demonstrates limited efficacy in controlling liver metastases, particularly in patients who have received ⩾2 prior lines of therapy.26,27 The development of more targeted and effective therapies has prompted interest in locoregional approaches such as TACE and HAIC.19,28–30 However, most studies on TACE or HAIC are case reports or involve small patient cohorts, despite showing promising results. In GCLM, the prevalent multifocal liver involvement and the biological differences from primary hepatic malignancies constrain the application of TACE alone. Combining TACE with HAIC may enhance tumor control while reducing complications associated with extensive embolization, providing a rationale for the present study.
Sun et al. 31 demonstrated mOS from liver metastasis diagnosis of 12 months in patients receiving comprehensive treatment, whereas mOS of the entire GCLM cohort was only 4 months. In our population, mOS from GC diagnosis was 25.6 months, mOS from liver metastasis diagnosis was 20.4 months, and mOS from the first DEB-TACE plus HAIC treatment was 10.7 months, suggesting that DEB-TACE combined with HAIC represents a promising regimen. Vogl et al. 32 reported ORR of 3.6% and DCR of 55.4% in GCLM patients receiving multiple TACE procedures, with mOS from the first TACE of 13 months. In contrast, our study observed ORR of 27.4%–30.6% and DCR of 75.8%. The discrepancy in response rates, despite similar survival outcomes, likely reflects the heavily pretreated status of our cohort, in which prior therapies may have limited OS despite favorable tumor responses. mRECIST is the preferred method for assessing treatment response in HCC undergoing locoregional therapies. Unlike original RECIST, mRECIST incorporates the assessment of the viable tumor tissue rather than just the size, thus providing a more accurate and sensitive evaluation of tumor response following interventional treatments. However, response was additionally assessed using RECIST 1.1 because RECIST 1.1 is the standard response criterion for metastatic disease. Notably, response rates and between-group comparisons were consistent across RECIST 1.1 and mRECIST analyses, supporting the robustness of the observed treatment effects regardless of response assessment criteria.
Current guidelines, including NCCN Clinical Practice Guidelines in Oncology and Japanese Gastric Cancer Treatment Guidelines, recommend fluoropyrimidine- or taxane-based systemic chemotherapy, supplemented with targeted therapy and best supportive care, as standard treatment for advanced GC.33,34 Nevertheless, the management of GCLM remains controversial due to the limited efficacy of these approaches. Oxaliplatin combined with fluoropyrimidines is a commonly used regimen in GC, 35 and FOLFOX-based HAIC has demonstrated favorable outcomes in colorectal liver metastases. Accordingly, we adopted the HAIC (FOLFOX) regimen in this study. Targeted and immunotherapeutic agents were also administered according to PD-L1 expressions and other biomarkers; 25.8% of patients received targeted therapy, 11.7% received immunotherapy, and 8.1% received a combination of targeted therapy and immunotherapy. Such multimodal strategies may improve the control of extrahepatic disease.
Prognostic analysis identified tumor location and CEA levels as independent predictors of survival. Patients with tumors located in the middle stomach exhibited more favorable outcomes, whereas elevated CEA levels were associated with poorer prognosis, consistent with prior reports.36–38 These findings may help guide patient selection and risk stratification in clinical practice.
The safety profile of DEB-TACE combined with HAIC was generally favorable. No treatment-related deaths were observed, and the most common grade 3–4 adverse events (AEs) were transaminase elevation (9.6%) and pain (14.8%), consistent with the expected toxicities of liver-directed locoregional therapy. These events were manageable and did not compromise overall treatment tolerability. Importantly, the combination of DEB-TACE and HAIC did not increase toxicity compared with either modality alone. Prior studies have reported myelosuppression, diarrhea, and transaminase elevation with HAIC, and fever or transaminase elevation with TACE in GCLM.19,39 The FOLFOX-based HAIC regimen includes oxaliplatin, which can cause cumulative dose-dependent hypersensitivity reactions; although no hypersensitivity events occurred in our cohort, continued vigilance is warranted. 40 Notably, gastrointestinal toxicities, including nausea, vomiting, and severe pain, were less frequent in HEPA-HAIC group compared with DCB-HAIC group, potentially reflecting differences in drug-release characteristics between HepaSphere and DC Bead. These findings suggest that DEB-TACE combined with HAIC is tolerable and that device selection may further optimize safety.
Our study demonstrates that DEB-TACE combined with HAIC is a feasible locoregional treatment strategy for patients with unresectable GCLM, particularly those who have failed or are intolerant to systemic therapy. The combination therapy achieved meaningful tumor control with a manageable safety profile, with HEPA-HAIC showing a modest advantage in tolerability. These results highlight the potential role of locoregional interventions to address a critical unmet need in patients with limited systemic options, offering a viable approach to improve disease control, providing symptom palliation and potentially extend survival. However, the application of combined DEB-TACE and HAIC requires careful patient selection in the setting of GCLM. This intensified locoregional treatment is optimally suited for patients who are either free of extrahepatic metastases or those who have a controlled, limited systemic tumor burden, ensuring that the liver-dominant disease remains the key driver of prognosis and therapeutic focus. Therefore, this approach should be considered for patients where the potential benefit of aggressive local control outweighs the risks associated with systemic progression.
Several limitations warrant consideration. First, the retrospective, single-center design may introduce selection bias and residual confounding, and the relatively small and heterogeneous cohort, including variations in time to liver metastasis and the use of targeted therapy and/or immunotherapy, may limit the precision of efficacy and safety estimates. In addition, the follow-up period was relatively short, restricting the assessment of long-term outcomes and late-onset AEs. The absence of a randomized control group precludes direct comparison with alternative therapies and limits the ability to define the relative benefit of DEB-TACE combined with HAIC.
Baseline imbalances between treatment groups were observed prior to matching, particularly in time to liver metastasis and exposure to targeted therapy or/and immunotherapy, both of which may influence prognosis and treatment response. To mitigate these potential sources of confounding, PSM was performed to balance clinically relevant baseline characteristics between groups. After matching, baseline differences were adequately minimized, and comparative analyses demonstrated treatment efficacy outcomes were consistent with those observed in the pre-matching cohort, suggesting that the observed treatment effects were not driven by baseline imbalance. Five patients (7.5%) were lost to follow-up and excluded from the analysis due to the absence of any evaluable outcome data, resulting in a complete-case analysis. Although the proportion was small and no documented disease progression or death occurred before loss to follow-up, a potential impact on the results cannot be entirely excluded. Finally, AEs were recorded during hospitalization and up to 30 days after each treatment cycle. While this captures most acute and early toxicities, delayed or cumulative AEs, such as biliary injury, vascular complications, or cumulative hepatic toxicity, may have been underestimated. Accordingly, longer-term prospective studies are warranted to more comprehensively evaluate delayed and cumulative toxicities associated with DEB-TACE combined with HAIC.
Conclusion
Our results suggest that DEB-TACE combined with HAIC can achieve intrahepatic disease control with manageable toxicity in patients with unresectable GCLM, supporting its potential role as a locoregional option for carefully selected patients. These results lay a foundation for future prospective, multicenter, randomized studies to validate efficacy, optimize patient selection, refine treatment protocols, and explore the mechanistic basis underlying the clinical benefits of locoregional therapy in this challenging patient population.
Supplemental Material
sj-pdf-1-tam-10.1177_17588359261449078 – Supplemental material for Efficacy and safety of drug-eluting bead transarterial chemoembolization combined with hepatic arterial infusion chemotherapy in unresectable gastric cancer with liver metastasis
Supplemental material, sj-pdf-1-tam-10.1177_17588359261449078 for Efficacy and safety of drug-eluting bead transarterial chemoembolization combined with hepatic arterial infusion chemotherapy in unresectable gastric cancer with liver metastasis by Baojiang Liu, Di Wu, Song Gao, Jianhai Guo, Fuxin Kou, Xin Zhang, Aiwei Feng, Xiaodong Wang, Guang Cao, Liang Xu, Hui Chen, Peng Liu, Haifeng Xu, Qinzong Gao, Renjie Yang and Xu Zhu in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.