
Abstract
Background:
Hepatocellular carcinoma (HCC) patients with multiple tumors have a poor prognosis and need more attention.
Objectives:
To develop an easily available radiological indicator that can differentiate the prognosis of Barcelona Clinic Liver Cancer stage A (BCLC-A) patients with multiple tumors.
Design:
This was a retrospective, multicenter study. Magnetic resonance imaging (MRI) data were collected from patients who underwent thermal ablation (TA), laparoscopic hepatectomy (LH), or LH combined with TA at five tertiary hospitals.
Methods:
Tumor distribution (TD) was classified into three types: same-segment, different-segments, and different-lobes, and three junior doctors (<5 years of experience) were invited to classify the tumors. We compared disease-free survival (DFS) and overall survival (OS) among the different TD types and performed pathological consistency and classification analyses. Six pathological indicators (tumor differentiation, alpha-fetoprotein (AFP), arginase-1 (Arg-1), hepatocyte paraffin 1, cytokeratin-19 (CK-19), and vascular endothelial growth factor (VEGF)) were included.
Results:
A total of 373 patients were included with a 36.0-month median follow-up. The Fleiss kappa score among the three doctors was 0.803. Patients with the same-segment type had better DFS and OS than those with different-segment (p < 0.001) and different-lobe (p < 0.001) types; therefore, the same segment was defined as a concentrated distribution. Different segments and lobes had comparable DFS (p = 0.072) and OS (p = 0.830) and were defined as having dispersed distributions. Patients in concentrated group had higher pathological consistency in tumor-differentiation (96.2% vs 86.7%, p = 0.003), AFP (95.3% vs 84.4%, p = 0.005), Arg-1 (96.7% vs 83.3%, p = 0.001) and CK-19 (96.0% vs 82.4%, p = 0.004), and better tumor-differentiation (23.3% vs 41.7%, p < 0.001) and lower expression rate in AFP (36.8% vs 49.5%, p = 0.035), CK-19 (9.3% vs 24.3%, p = 0.008), and VEGF (17.0% vs 39.3%, p = 0.004) than dispersed group.
Conclusion:
We established a method based on MRI to accurately differentiate the TD type of multiple tumors for patients in the BCLC-A stage. Patients with concentrated distribution tumors had a better prognosis than patients with dispersed distribution.
Introduction
Hepatocellular carcinoma (HCC) is the sixth most commonly diagnosed cancer and the third most common cause of cancer-related deaths worldwide.1,2 Barcelona Clinic Liver Cancer (BCLC) prognosis and treatment strategies are important staging systems that can guide doctors in selecting treatment methods for patients with different physical conditions. 3 According to the BCLC guidelines, local curative treatment (surgery or ablation) is recommended for patients with BCLC-A stage. BCLC-A stage includes two categories: patients with solitary HCC or patients with 2–3 HCCs and each ⩽3 cm. 3 Previous studies have shown that multiple tumors are risk factors for patient prognosis2,4; however, only a few studies have been conducted in patients with multiple tumors.5,6 Therefore, it is important to identify an effective indicator for determining the prognosis of these patients.
Compared with pathological or radiomic features, tumor distribution (TD) is an easily available feature for patients with multiple tumors. TD could be assessed through preoperative imaging examinations without an additional financial burden on patients and it depends on doctors with additional knowledge. 7
The TD is an important factor in treatment decisions. 8 For concentrated distributed tumors, laparoscopic hepatectomy (LH) can simultaneously remove multiple tumors at one time without causing excessive damage to the liver parenchyma. However, for dispersed distributed tumors, multiple resections at different locations would inevitably increase damage to the parenchyma. For these patients, thermal ablation (TA) or LH combined with TA (LH + TA) may be safer options. 9 Therefore, the effects of different treatment methods on patients with different TD types also need to be analyzed.
This study aimed to analyze the influence of the TD type on the prognosis of BCLC stage A patients with multiple tumors, examine the possible reasons for this, and compare the effects of different treatment methods on patients with different TD types.
Materials and methods
Patients
This study included patients from five tertiary hospitals between January 2010 and March 2021. It was a secondary analysis of a prospective multi-center study enrolled in the National China Register on Ultrasound of Liver Lesions. This study was conducted in accordance with the Declaration of Helsinki. This study was approved by the Institutional Review Board of the People’s Liberation Army Hospital (Beijing, China; approval number: S2021-056-07), and the requirement for informed consent was waived. The inclusion criteria were: (1) pathologically diagnosed HCC; (2) treatment by TA, LH, or LH + TA; (3) tumor number of 2–3, and tumor size ⩽3 cm; and (4) no treatment history. The exclusion criteria were: (1) palliative treatment, (2) combination with other malignant tumors, and (3) metastasis or vascular invasion on imaging.
Study design
This study conforms to the STARD statement 10 (Supplemental Material). TD was first grouped into three types: tumors in the same segment, tumors in different segments (different segments but in the same lobe), and tumors in different lobes. Three junior doctors (with <5 years of imaging experience) were invited to examine cases by TD type based on preoperative multisequence magnetic resonance imaging (MRI; T1, T2, arterial phase, portal phase, and delay phase). Three doctors knew that there were multiple tumors on MRI but were not informed of the exact tumor number. We then assessed the consistency among the three doctors. If the results were inconsistent, a senior doctor (with >15 years of imaging experience) was invited to determine the final result.
Disease-free survival (DFS) and overall survival (OS) were compared among the three TD types, and post hoc comparisons between pairs of groups were performed.
We then compared the pathological consistency and classification of different TD types. Pathologically consistent results were defined as multiple tumors in one patient with the same pathological result, and pathologically inconsistent results were defined as multiple tumors with different pathological results. For pathologically inconsistent patients, the pathological classification was recorded as the worst type among multiple tumors. The pathological indicators included tumor differentiation, alpha-fetoprotein (AFP), arginase-1 (Arg-1), hepatocyte paraffin 1 (Hep Par1), cytokeratin-19 (CK-19), and vascular endothelial growth factor (VEGF).
We compared the prognoses of different TD types in different subgroups, including sex, age, tumor size, and tumor number. We also compared the effects of different treatment methods on the different types of TD. Propensity score matching (PSM) and inverse probability of treatment weighting (IPTW) were used to balance the baselines. 11
Treatment process
The LH, TA, and LH + TA processes were performed as described previously12,13 (detailed process in the Supplemental Materials). In patients, the TA process is percutaneous. In the LH + TA group, the TA process was laparoscopic.
Follow-up
The follow-up protocol included regular outpatient physical, serum, and imaging examinations. US and CT/MRI were performed in the first and third months after treatment, followed by scans every 6 months. In cases with abnormal findings, further tests were conducted to confirm tumor recurrence.
Statistical analysis
Continuous data were expressed as the means ± SDs and were evaluated by independent sample t test or variance analysis. Categorical variables were analyzed using the χ2 test or Fisher’s exact test. The consistency of three doctors was assessed by Fleiss’ kappa (0.40–0.60 as moderate, 0.60–0.80 as substantial, and 0.80–1.00 as perfect). Kaplan–Meier curves and log-rank tests were used to compare DFS and OS. PSM and IPTW were used to balance the baseline values. R (version 4.0.1) was used for the data analyses.
Results
A total of 373 eligible patients with 828 tumors from 5 hospitals were enrolled between January 2010 and March 2021, with a 36.0-month median follow-up (23.3–53.2 months; Figure 1).
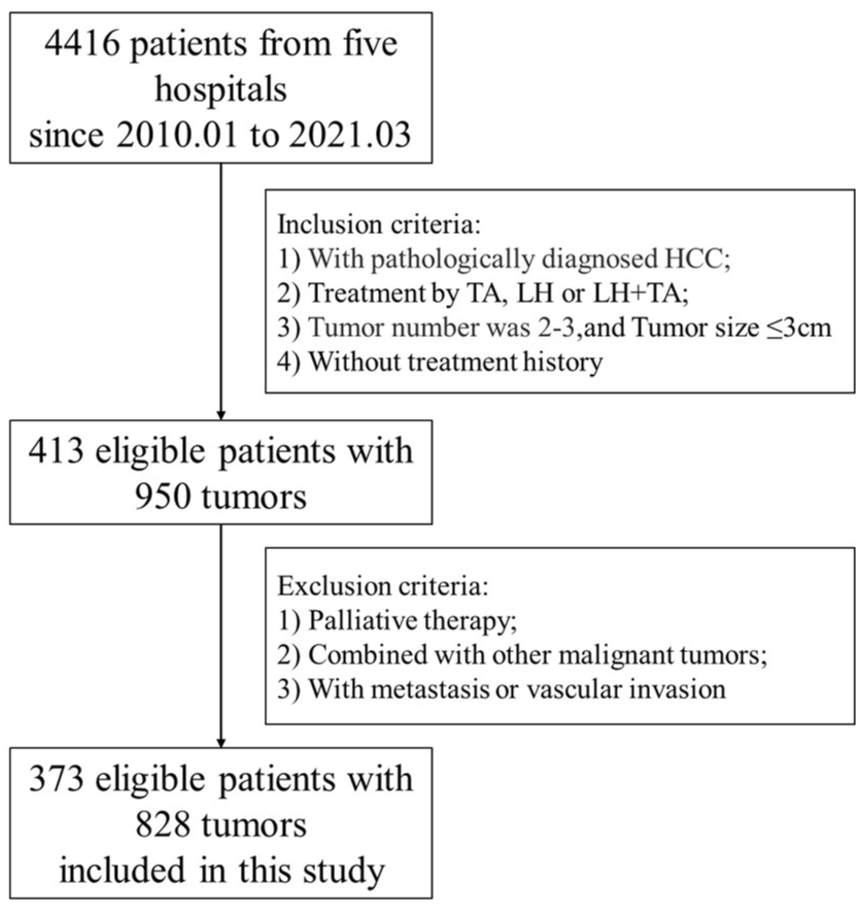
Flowchart of study.
Consistency of TD type derived from preoperative MRI
Three doctors classified the TD types based on preoperative multi-sequence MRI, and Fleiss’ kappa was 0.803 (Supplemental Table 1). After review by a senior doctor, 133 patients with 291 tumors were included in the same-segment type, 130 patients with 290 tumors were included in the different-segment type (tumors in different segments but in the same lobe), and 110 patients with 247 tumors were included in the different-lobe type.
Prognosis among patients with different TD types
The baseline characteristics of the three groups are shown in Table 1. Due to the influence of TD on the choice of treatment method, there was a significant difference in the treatment method among the three types (p < 0.001). Most patients with LH were of the same segment type (90.8%, 5.1%, and 4.1% in same-segment, different-segment, and different-lobe types, respectively), no LH + TA patients were of the same segment type (0%, 48.9%, and 51.1% in same-segment, different-segment, and different-lobe types, respectively), and TA patients were evenly distributed in three types (23.5%, 43.9%, and 32.6% in same-segment, different-segment, and different-lobe types, respectively).
Baseline of the same-segment, the different-segments and the different-lobes groups.

Note: Values are mean ± standard deviation or number (%).
AFP, alpha fetoprotein; ALB, serum albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DB, direct bilirubin; INR, international normalized ratio; LH, laparoscopic hepatectomy; PLT, platelets; TA, thermal ablation; TB, total bilirubin; TP, total protein; γ-GT, γ-glutamyl transpeptidase.
There was a significant difference in DFS among the three TD types (p < 0.001, Figure 2(a)), and post hoc comparisons showed that the same-segment type had significantly better DFS than the different-segments (p < 0.001, Supplemental Figure 1(A)) and different-lobe (p < 0.001, Supplemental Figure 1(B)) types. There were no significant differences between the different-segments and -lobe types (p = 0.072, Supplemental Figure 1(C)).

DFS between patients with different TD. DFS among patients in same-segment, different-segments, and different-lobes types (a), DFS between patients in concentrated and dispersed groups in original (b), PSM (c), IPTW (d), and subgroup (e).
There was a significant difference in OS among the three TD types (p = 0.001, Figure 3(a)), and post hoc comparisons showed that patients with the same segment type had significantly better OS than patients with different segment types (p = 0.001, Supplemental Figure 1(A)) and different lobe types (p = 0.001, Supplemental Figure 1(B)). There were no significant differences between the different segments and lobe types (p = 0.83; Supplemental Figure 2(C)).

OS between patients with different TD. OS among patients in same-segment, different-segments, and different-lobes types (a), DFS between patients in concentrated and dispersed groups in original (b), PSM (c), IPTW (d), and subgroup (e).
According to patient prognosis, we defined patients with multiple tumors distributed in the same segment as the concentrated group (n = 133) and those with multiple tumors distributed in different segments and lobes as the dispersed group (n = 240).
Prognosis between concentrated and dispersed groups
There were significant differences in age (55.63 ± 10.03 vs 58.27 ± 10.62 years, p = 0.020), ALT (42.41 ± 27.89 vs 36.08 ± 23.98 U/L, p = 0.022), and PLT (138.36 ± 54.10 vs 119.32 ± 52.45 109/L, p = 0.001) between the concentrated and dispersed groups in the crude cohort (Supplemental Table 2). The log-rank test showed that the concentrated group exhibited significantly better DFS and OS than the dispersed group (hazard ratio (HR) = 2.25, 95% confidence interval (CI): 1.57–3.21, p < 0.001, Figure 2(b) and (e)) and (HR = 2.58, 95% CI: 1.52–4.36, p < 0.001, Figure 3(b) and (e)). After PSM, all baselines in the concentrated group (n = 122) and dispersed group (n = 122) were comparable, and the concentrated group exhibited significantly better DFS and OS (HR = 2.24, 95% CI: 1.51–3.03, p < 0.001, Figure 2(c) and HR = 2.28, 95% CI: 1.28–4.05, p = 0.003, Figure 3(c), respectively) than the dispersed group. After IPTW, all baselines in the concentrated group (n = 356) and dispersed group (n = 383) were comparable, and the concentrated group still exhibited significantly better DFS and OS (HR = 2.33, 95% CI: 1.52–3.13, p < 0.001, Figure 2(d) and HR = 2.20, 95% CI: 1.30–4.11, p = 0.005, Figure 3(d), respectively) than the dispersed group.
Subgroup analysis
We compared the DFS and OS between the concentrated and dispersed groups in several subgroups, including sex, age, tumor size, and tumor number. The DFS in the concentrated group was significantly better than that in the dispersed group for several variables, including sex (male (HR = 2.08, 95% CI: 1.41–3.08, p < 0.001), female (HR = 3.28, 95% CI: 1.35–7.94, p = 0.005)), age (⩾60 years (HR = 1.94, 95% CI: 1.12–3.38, p = 0.017) and <60 years (HR = 2.53, 95% CI: 1.59–4.04, p < 0.001)), tumor size (⩾2 cm (HR = 2.29, 95% CI: 1.52–3.45, p < 0.001) and <2 cm (HR = 2.09, 95% CI: 1.01–4.33, p = 0.043)), and multiple tumors (double tumors (HR = 2.07, 95% CI: 1.39–3.08, p < 0.001) and three tumors (HR = 2.96, 95% CI: 1.31–6.69, p = 0.006); (Figure 2(e) and Supplemental Figure 3). The OS in the concentrated group was significantly better than that in the dispersed group by for sex (male (HR = 2.40, 95% CI: 1.34–4.30, p = 0.002), female (HR = 3.65, 95% CI: 1.05–12.64, p = 0.029)), age (⩾60 years (HR = 2.35, 95% CI: 1.04–5.34, p = 0.035) and <60 years (HR = 2.70, 95% CI: 1.36–5.37, p = 0.003)), tumor size (⩾2 cm (HR = 2.66, 95% CI: 1.42–4.98, p = 0.001)), and multiple tumors (double tumors (HR = 2.23, 95% CI: 1.21–4.10, p = 0.008) and three tumors (HR = 3.98, 95% CI: 1.37–11.55, p = 0.006)), and slightly better than that of dispersed group for tumor size <2 cm (HR = 2.35, 95% CI: 0.89–6.22, p = 0.075; Figure 3(e) and Supplemental Figure 4).
Analysis of pathological consistency and pathological classification
Only if all tumors in one patient had pathological results could the patient be included in the analysis. The number of patients with different pathological indicators is shown in Supplemental Table 3.
In the pathological consistency analysis, the concentrated group had a significantly higher pathologically consistent rate than the dispersed group in tumor differentiation (96.2% vs 86.7%, p = 0.003), AFP (95.3% vs 84.4%, p = 0.005), Arg-1 (96.7% vs 83.3%, p = 0.001), and CK-19 (96.0% vs 82.4%, p = 0.004); the concentrated group exhibited a pathologically consistent rate comparable to that of the dispersed group in Hep Par 1 (91.9% vs 91.0%, p = 0.825) and VEGF (91.5% vs 84.5%, p = 0.255; Figure 4(a)).

Analysis of pathological consistency and pathological classification. (a) Pathological consistency rate between concentrated and dispersed groups. (b) Pathological classification between concentrated and dispersed groups.
In pathological classification analysis, the concentrated group exhibited better tumor differentiation (23.3% vs 41.7%, p < 0.001), lower AFP expression (36.8% vs 49.5%, p = 0.035), lower CK-19 (9.3% vs 24.3%, p = 0.008), and lower VEGF expression (17.0% vs 39.3%, p = 0.008) than the dispersed group; the concentrated group exhibited Arg-1 expression (30.1% vs 33.9%, p = 0.528) and Hep Par1 (80.2% vs 77.6%, p = 0.629) expression comparable to that of the dispersed group (Figure 4(b)).
The efficacy of treatment methods in different TD groups
The concentrated group included 44 TA patients, 89 LH patients, and zero LH + TA patients; we compared the prognosis between TA patients and LH patients. There was no significant difference in DFS (HR = 0.930, 95% CI: 0.481–1.799, p = 0.831, Figure 5(a)) or OS (HR = 0.642, 95% CI: 0.247–1.669, p = 0.362, Figure 5(b)) between TA patients and LH patients. The dispersed group included 143 TA patients, 9 LH patients, and 88 LH + TA patients; we compared the prognosis between TA patients and LH + TA patients. There was no significant difference in DFS (HR = 0.914, 95% CI: 0.774–1.079, p = 0.291, Figure 5(c)) or OS (HR = 0.781, 95% CI: 0.606–1.006, p = 0.053, Figure 5(d)) between TA patients and LH + TA patients.

Prognosis of different treatment methods in concentrated and dispersed groups. (a) DFS between TA and LH patients in concentrated group. (b) OS between TA and LH patients in concentrated group. (c) DFS between TA and LH + TA patients in dispersed group. (d) OS between TA and LH + TA patients in dispersed group.
Discussion
Multiple tumors are common and associated with a poor prognosis. 8 It is important to analyze the factors influencing the prognosis of these patients and understand the reasons for these influences.
Multiple tumors have many unique characteristics that a single tumor cannot possess, and the most typical characteristic is the positional relationship between multiple tumors. The distance between tumors is an intuitive method for classifying TD; however, this approach does not align with the inherent anatomical structure of the liver. Additionally, although it may be straightforward for dual tumors, it becomes complex for all three tumors. The Couinaud system was established based on the distribution of the main blood vessels and bile ducts. Therefore, we determined the tumor location based on the Couinaud system, classified multiple tumors according to TD type, and analyzed the influence of TD type on patient prognosis. In this study, we first grouped TD into three types: same-segment, different-segments (different segments but in the same lobe), and different-lobe tumors, and invited three junior doctors to perform TD-type classification based on multisequence MRI.
Benefiting from the widespread application of the Couinaud system and the development of MRI technology, classifying tumors according to the TD type is not a difficult task, even for junior doctors. The Fleiss’ kappa value of the three junior doctors was 0.803, indicating that multi-sequence MRI was a good method for classifying the TD type. Multi-sequence MRI, especially the arterial phase sequence, can clearly show the main blood vessels, which is helpful for determining tumor location and conducting TD-type classification.
We compared the prognosis of the three TD types and found that the DFS and OS of same-segment-type patients were significantly better than those of different-segment-type and different-lobe-type patients, but there was no significant difference in DFS and OS between the different-segment-type and different-lobe-type patients. Based on tumor location and patient prognosis, we defined same-segment type as concentrated distribution and different-segment type and different-lobe type as dispersed distribution. In the original cohort, PSM cohort, IPTW cohort, and various subgroup analyses, the prognosis of the patients in the concentrated group was significantly better than that of the patients in the dispersed group.
For this difference, we speculated that the possible reason was that the TD type could reflect the patient’s potential tumor burden.14,15 The formation of multiple tumors can be summarized in three ways: local invasion, 16 vascular metastasis, 17 and multiple-origin tumors. For patients in the concentrated group, the formation of multiple tumors was more likely to be a local invasion; therefore, the area of tumor dissemination on the liver parenchyma would be smaller, and the potential tumor burden would be lower. However, for patients in the dispersed group, the formation was more likely to be vascular metastasis; therefore, the area of tumor dissemination was greater, and the potential tumor burden was higher. Even worse, for patients in the dispersed group, the formation could also be multiple-origin tumors,18,19 which means that the liver parenchyma of these patients would have a higher cancer tendency and their prognosis would be more unfavorable.
To test this hypothesis, we performed pathological consistency and classification analyses between the two groups. We found that the concentrated group exhibited a significantly higher pathologically consistent rate of tumor differentiation, AFP, Arg-1, and CK-19, and a comparable pathologically consistent rate of Hep Par1 and VEGF to the dispersed group. Tumors of the same origin were more likely to have the same pathological type, whereas those of different origins were more likely to have different pathological types. Therefore, the lower pathological consistency rate in the dispersed group could indicate that, compared to the concentrated group, the dispersed groups may contain more tumors of multiple origins. Hep Par1 is widely expressed in most HCCs, but there are not enough cases to compare the pathologically consistent rates of VEGF expression. Therefore, there was no significant difference in consistency between these two pathological indicators. We also found that the concentrated group exhibited better tumor differentiation, lower AFP expression, lower CK-19, and lower VEGF expression than the dispersed group, and had comparable Arg-1 expression and Hep Par1 expression to the dispersed group. Previous studies showed that tumor differentiation, AFP, CK-19, and VEGF were significantly related to tumor metastasis ability and patient prognosis. 20 Therefore, the higher expression rates of these pathological indicators in the dispersed group could indicate that the tumors in the dispersed group had stronger aggressiveness, allowing them to metastasize to a wider area. Arg-1 and Hep Par1 did not have a strong relationship with prognosis and were diagnostic tumor markers for HCC, so there was no significant difference in the pathological classification between the two groups in Arg-1 and Hep Par1.
Previous studies have investigated the prognosis of patients with multiple tumors.21,22 In these studies, surgical resection was usually the main research objective and preferred treatment method. 23 However, with advancements in medical technology, TA has achieved treatment effects comparable to those of LH in patients with a single HCC <3 cm. 24 Additionally, with the rise in multidisciplinary approaches, LH combined with TA has emerged in many clinical scenarios. Therefore, we compared the prognosis of different treatment methods in different groups.
In the concentrated group, there were no significant differences in DFS or OS between patients with TA and LH. In the dispersed group, there were no significant differences in DFS and OS between patients with TA and those with LH + TA. These results showed that TA could achieve a satisfactory treatment effect in BCLC-A patients with different TD types and multiple tumors. Additionally, because the prognosis of different treatment methods for the same TD type was comparable, it further proved that the TD type, rather than the treatment method, affected patient prognosis. Therefore, even if our study included patients who received different treatment methods, the reliability of the results would not have been affected. The latest BCLC guidelines recommend that patients with multiple tumors undergo TA. The results of our study support this conclusion. In addition, we suggest that, for patients with HCC and multiple tumors in different segments, the follow-up interval should be shortened to detect possible tumor recurrence early.
In summary, our study is significant in guiding treatment decisions for patients with HCC with multiple tumors in the BCLC-A stage and in analyzing tumor metastasis mechanisms. From a clinical perspective, we evaluated three treatment methods (LH, TA, and LH + TA) in patients with different TDs. In concentrated and dispersed distributions, TA demonstrated comparable efficacy to LH and LH + TA, respectively, suggesting that TA might serve as a versatile approach for managing multiple tumors in the BCLC-A stage. This finding might expand the therapeutic options for these patients. From the perspective of the tumor mechanism, we identified significant pathological differences between the concentrated and dispersed distributions. These differences aid in distinguishing locally infiltrative metastasis from hematogenous metastasis, thereby advancing our understanding of the mechanisms underlying tumor metastasis. Furthermore, variations in VEGF and Arg-1 expression between concentrated and dispersed distributions provide valuable reference information for patients undergoing targeted or immunotherapy.
Our study had some limitations. First, this was a retrospective analysis, and the results must be verified using prospective data. Second, some of the imported molecular data were absent. Although we included six pathological indicators in this study, some classical histological characteristics (such as VEGF 131/373 and CK-19 211) and molecular data (such as TP53 and HBV-related) were still lacking. Advanced pathological technologies, such as single-cell sequencing and whole-exome sequencing, should be used in future studies. Third, the pathological results of surgery and biopsy may not be consistent. To prevent this interference, we selected less controversial pathological indicators, such as microvascular invasion and macrotrabecular mass, which are considered to have different detection rates between surgical and biopsy pathology.
Conclusion
MRI can be used to accurately classify the distribution type of multiple tumors in patients with BCLC stage A, and patients with concentrated distribution of tumors have a better prognosis than patients with dispersed distribution.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251403407 – Supplemental material for Tumor distribution type helps distinguish the prognosis of HCC patients with multiple tumors in BCLC-A stage: a multi-center retrospective study
Supplemental material, sj-docx-1-tam-10.1177_17588359251403407 for Tumor distribution type helps distinguish the prognosis of HCC patients with multiple tumors in BCLC-A stage: a multi-center retrospective study by WenZhen Ding, Xueqin Tian, Yongfeng Yang, Haokai Xu, Xin Li, Jie Yu and Ping Liang in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.