
Abstract
Background:
Cervical cancer remains the fourth most common malignant cancer in females and the fourth most common cause of mortality in women worldwide. Approximately 70% of new cases are diagnosed as locoregionally advanced cervical cancer (LACC), posing a significant threat to women’s health. Concurrent chemoradiotherapy (CCRT) is the established standard treatment for LACC. However, more than 30% of patients still experience local recurrence and distant metastasis. Improving treatment outcomes for LACC is a critical global objective.
Objective:
To investigate the safety and efficacy of adding Endostar to CCRT in patients with LACC.
Design:
This is a multicenter, open-label, randomized, controlled, phase II trial.
Methods:
A total of 120 patients were randomly allocated (1:1) to receive either CCRT alone (definitive radiotherapy plus cisplatin 40 mg/m2 every week for 4–5 cycles) or CCRT plus Endostar, Endostar at a dose of 7.5 mg/m2/day, from 5 days before CCRT for 10 consecutive days every 15 days for four cycles).
Results:
The CCRT + E arm demonstrated a significantly higher complete response rate (CRR) compared to the CCRT arm (68.3% vs 35.0%, p = 0.001), while the overall response rate (ORR) was similarly in both arms (98.3% vs 100%, p = 1.000). The CCRT + E arm showed significantly improved distant metastasis-free survival (DMFS) (1-year: 91.6% vs 94.8%, 2-year: 82.3% vs 91.6%, 5-year: 67.0% vs 88.0% p = 0.029). No significant differences were found in overall survival (OS), progression-free survival (PFS), or locoregional recurrence-free survival (LRFS) (p > 0.05). Multivariable analysis identified maximum tumor diameter >4 cm and failure to achieve CR as predictive factors of poor PFS, and maximum tumor diameter >4 cm and stage IIIA–IVA disease as poor prognostic factors for OS. According to the subgroup analysis, Endostar significantly improved the DMFS in cohorts of patients with squamous cell carcinoma (p = 0.005), a maximum tumor diameter > 4 cm (p = 0.011), and stage IB2 or IIA2–IIB disease (p = 0.005). The rates of acute and late adverse reactions were similar in both arms (p > 0.05), with no cardiac toxicity, hypertension, or grade 5 toxicity reported.
Conclusion:
The addition of Endostar to CCRT significantly enhanced tumor response (CRR) and reduced distant metastasis (DMFS) in LACC patients without increasing treatment toxicity, offering a promising therapeutic enhancement. Clinically, patients with squamous cell carcinoma, maximum tumor diameter > 4 cm, and International Federation of Gynecology and Obstetrics stage IB2 or IIA2–IIB disease derived particularly robust DMFS benefits from the combination regimen, suggesting they should be prioritized for this approach. Although the 5-year DMFS results are encouraging, validation in a larger phase III study and longer follow-up are warranted before considering this regimen as a new standard treatment modality for LACC.
Trial registration:
This trial was registered at ClinicalTrials.gov (NCT 03086681, registered 22 March 2017, https://clinicaltrials.gov/study/NCT03086681.
Background
Cervical cancer remains the fourth most common malignant cancer in females and the fourth most common cause of mortality in women worldwide, with locoregionally advanced cervical cancer (LACC) accounting for approximately 70% of new diagnoses and posing a significant threat to women’s health.1,2 Concurrent chemoradiotherapy (CCRT) is the established standard treatment for LACC, offering significant survival benefits over radiotherapy alone (CCRT results in a 30% to 50% decrease in the risk of cancer-related mortality and a 10%–12% improvement in survival). However, more than 30% of patients still experience local recurrence and distant metastasis.3 –7 Improving treatment outcomes for LACC is a critical global objective.
In 1971, Folkman confirmed that angiogenesis is the key mechanism underlying tumor growth. 8 Targeting tumor angiogenesis is a validated approach in advanced cervical cancer. Bevacizumab, an antibody against vascular endothlial growth factor (VEGF), combined with doublet chemotherapy improves survival in metastatic or recurrent cervical cancer but is associated with significant toxicities (e.g., bleeding, gastrointestinal perforation) that limit its broader application.9 –11
Endostar, a recombinant human endostatin, offers a potentially more favorable profile. It demonstrates enhanced stability, multi-target anti-angiogenic activity, and the ability to normalize tumor vasculature, potentially improving oxygen delivery and treatment efficacy. 12 While promising results with Endostar combined with chemotherapy exist for recurrent/metastatic disease, 13 and preliminary data suggest improved short-term response rates when combined with CCRT in LACC. 14 A randomized controlled study of 52 patients with International Federation of Gynecology and Obstetrics (FIGO) IIB–IVA cervical cancer demonstrated that the Endostar + CCRT arm had a significantly higher complete response rate (CCR) and objective response rate (ORR) than the CCRT arm (CCR: 73.1% vs 34.6%; ORR: 96.2% vs 76.9%, p < 0.05). The 1-year survival rates were 100% in the CCRT + E arm and 84.6% in the CCRT arm, with the difference being statistically significant (p < 0.05). 15 However, the long-term efficacy and safety of adding Endostar to definitive therapy for LACC has not been reported. This study was therefore conducted to investigate the clinical efficacy and toxicity of integrating Endostar into standard CCRT for patients with LACC, specifically evaluating long-term outcomes.
Materials and methods
Inclusion and exclusion criteria
This multicenter, open-label, randomized, controlled, phase II trial was conducted at seven hospitals in Guangxi, China. This multicenter study involved the following seven institutions: The First Affiliated Hospital of Guangxi Medical University (Nanning, China), The Second Affiliated Hospital of Guangxi Medical University (Nanning, China), The Liuzhou People’s Hospital (Liuzhou, China), The Liuzhou Worker’s Hospital (Liuzhou, China), The Guilin Medical University Affiliated Hospital (Guilin, China), The Red Cross Hospital of Yulin City (Yulin, China), and The People’s Hospital of Beihai (Beihai, China). This trial was designed by the First Affiliated Hospital of Guangxi Medical University in Nanning, China. Patients with LACC were randomly assigned in a 1:1 ratio to either the CCRT arm, which received standard treatment with concurrent chemoradiotherapy, or the CCRT + E arm, which received Endostar in addition to CCRT (Figure 1). Random assignments were based on computer-generated random numbers. Simple randomization, such as stratification or blocking, was adopted without any restriction. Patients with odd random numbers were assigned to the CCRT + E arm, and those with even random numbers were assigned to the CCRT arm. The inclusion criteria were as follows: LACC patients with stage IB2, IIA2–IVA (FIGO version 2009); confirmed by pathological biopsy to be squamous cell carcinoma or adenocarcinoma; aged 18–65 years; Karnofsky performance status of 70 or more; estimated survival at least 6 months; adequate bone marrow function (white blood cell count ⩾ 4.0 × 109/L, platelets ⩾ 100×109/L); liver and renal functions values ⩽ 1.25 × upper normal limits and normal prothrombin time. Patients were excluded if they had other primary malignancies, contraindications to radiotherapy, chemotherapy, or targeted therapy, including severe infection, serious cardiovascular disease, or serious neurological or mental deficiency. The research program strictly followed the Helsinki Declaration. The reporting of this study conforms to the CONSORT reporting guidelines (Supplementary File S1). 15

Study design.
Radiotherapy
In this study, all patients received external beam radiation therapy (EBRT), which was delivered using intensity-modulated conformal radiotherapy, and high-dose rate intracavitary brachytherapy (BT). Regional lymphatics were administered at a dose of 45–50 Gy in 25 fractions (1.8–2.0 Gy per fraction, five times per week). Pelvic metastatic lymph nodes were boosted to a total dose of 56–60 Gy. Image-guided radiotherapy (IGRT) or cone-beam computed tomography (CBCT) was utilized with imaging for positional verification at the time of radiotherapy delivery and weekly. BT, which uses an iridium-192 source, was carried out at the end of EBRT with a dose of 28–30 Gy (6–7 Gy per fraction, twice a week). Brachytherapy planning was performed using 3D techniques based on CT, conducting dose-volume histogram (DVH) evaluation in 93.3% (112/120) of patients and 2D techniques based on point A in 6.7% (8/120) of patients. The median overall treatment time was 45.5 days (range: 36–67 days), with 87.5% of patients completing treatment within 56 days.
Chemotherapy and antiangiogenesis therapy
All patients received chemotherapy with cisplatin at a dose of 40 mg/m2 on day 1 once a week for 4–5 weeks, and those in the CCRT + E arm also received four planned cycles of Endostar (Simcere Pharmaceutical, Nanjing, China) at a dosage of 7.5 mg/m2/day, and was given via intravenous micropump maintenance from 5 days before CCRT for 10 consecutive days every 15 days for four cycles. The selection of 7.5 mg/m2/day of Endostar from 5 days before CCRT was based on the results of trials of Endostar with chemoradiation therapy that had already been performed.14,16
Treatment assessments
The tumor response evaluation was based on physical examination and pelvic magnetic resonance imaging (MRI), or CT with contrast and chest/abdomen CT with contrast at 3 months after the completion of treatment. Tumor response was evaluated according to RECIST 1.1, a standardized criteria developed by international oncology organizations, was categorized as follows: complete remission (CR), partial response (PR), stable disease (SD), and progressive disease (PD). The objective response rate (ORR) was the sum of the CR and PR rates.
The primary endpoints were the CRR and treatment-related toxicity. The secondary endpoints included ORR, OS, PFS, distant metastasis-free survival (DMFS), and locoregional recurrence-free survival (LRFS). OS was defined as the time from randomization to the date of death or the last follow-up visit. PFS, DMFS, and LRFS were calculated from the date of randomization to the date of the first event, which was defined as progressive disease or death due to any cause for PFS, distant metastasis for DMFS, and regional recurrence for LRFS, respectively. Acute adverse events were defined as any treatment-related toxicities that occurred during the treatment and the following 3 months. Late treatment-related morbidities were assessed more than 3 months after completion of treatment. Acute and late drug-related events were assessed according to the Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 (NCI, Bethesda, MD, USA). Acute and late radiation-induced morbidities were assessed according to the Radiation Therapy Oncology Group (RTOG) Toxicity Criteria. The patients were followed up every 3 months during the first 2 years, every 6 months from 3 to 5 years, and then annually. Cervical/vaginal cytology test was performed annually. For patients with suspicious recurrent/metastatic disease, additional imaging such as positron emission tomography, bone scintigraphy, or a biopsy, whenever possible, was obtained to confirm.
Sample size calculation
According to previous studies, for LACC patients, the CRR in those undergoing chemoradiation was 34.6%, whereas the CRR in those undergoing chemoradiation plus Endostar was 73.8%. 15 In this study, the CRR was expected to increase from 35% with CCRT to 65% with CCRT + Endostar. Sample size calculation was performed using PASS 15 software, which indicated that 108 patients (54 in each arm) were required to achieve a 90% confidence level at a type I error of 0.05 (two-sided). An estimated dropout rate of 10% was considered for each arm. The intended number of patients randomly assigned to each arm was 60.
Statistical analyses
All the data were analyzed using IBM SPSS 25.0 software (SPSS, Chicago, IL, USA), PASS 15 software (NCSS, LLC; Kaysville, UT,USA) and R V.4.3.2 (The R Foundation for Statistical Computing, Vienna, Austria). OS, PFS, DMFS, LRFS, and subgroup analysis were analyzed using the Kaplan–Meier approach and compared by the log-rank test. Statistical comparisons of continuous variables were performed by t-test, and classification variables were conducted by χ2 test or Fisher’s exact test. The prognosis analysis was performed using the Cox proportional hazard regression model. All variables considered clinically relevant and prognostically significant based on the literature (Treatment arm, Age, Maximum tumor diameter, Pelvic lymph node status, FIGO stage, Histology, Grade, and Remission status) were included univariate analysis. Multivariate analyses were performed on variables with p values < 0.05 in the univariate analysis. Subgroup analyses were performed using the Kaplan–Meier method and Cox proportional hazards regression. To control the family-wise error rate arising from multiple comparisons, the Bonferroni P/2 correction was applied to adjust significance levels. All reported p-values for subgroup comparisons are adjusted values. Toxicity incidence was analyzed using non-parametric statistical tests.
Results
Patients
Between March 2017 and September 2020, a total of 126 patients with cervical cancer stages IB2, and IIA2–IVA (FIGO 2009) were enrolled, and six patients were lost to follow-up (four patients in the CCRT arm, and two patients in the CCRT + E arm). Finally, 120 cases were included in the analysis. There were 60 patients in each arm. The median age was 53 years (range: 30–65 years). One hundred and nine patients (90.8%) had squamous cell carcinoma, and 11 (9.2%) had adenocarcinoma. Most patients were diagnosed with stage IIB disease (65.0%), followed by IIA2 (13.4%), IIIB (10.8%), IB2 (4.2%), IIIA (3.3%), and IVA disease (3.3%). In 86 patients, the maximum tumor diameter was greater than 4 cm. Moreover, 46 patients had pelvic lymph node metastasis. The clinical characteristics were well balanced between the two arms (all p > 0.05). Table 1 provides further details.
Baseline demographic and disease characteristics in the intention-to-treat population.
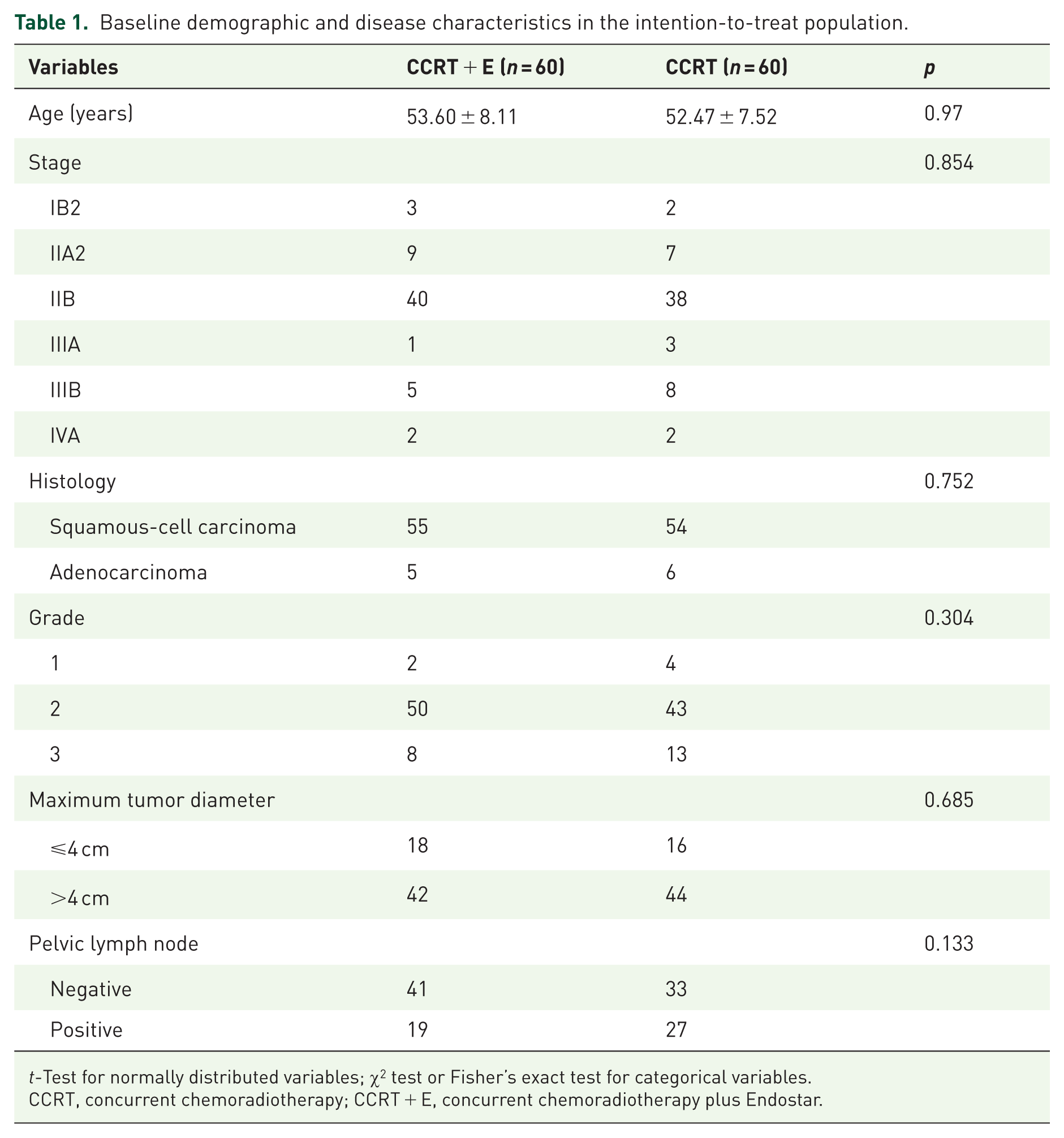
t-Test for normally distributed variables; χ2 test or Fisher’s exact test for categorical variables.
CCRT, concurrent chemoradiotherapy; CCRT + E, concurrent chemoradiotherapy plus Endostar.
Early treatment response
All patients completed the planned treatment regimen. Among the 120 patients eligible for evaluation, CR and PR were observed in 62 patients (51.7%) and 57 patients (47.5%), respectively. In the CCRT arm, 21 patients achieved CR (35.0%) and 39 (65.0%) achieved PR, resulting in a CRR of 35.0% and an ORR of 100%. In the CCRT + E arm, 41 patients achieved CR (68.3%), 18 achieved PR (30.0%), and 1 achieved SD, resulting in a CRR of 68.3% and an ORR of 98.3%. The CCRT + E arm had a higher CRR than the CCRT arm did (68.3% vs 35.0%, p = 0.001), while there was no significant difference in the ORR between the two arms (98.3% vs 100%, p = 1.000).
Survival analysis
Follow-up was performed until December 31, 2023, and the median follow-up time was 53.0 months (range of 8–81 months). The median follow-up duration was 48.0 months (range of 9–81 months) in the CCRT + E arm and 54.5 months (range: 8–81 months) in the CCRT arm. Among all the patients, 42 (35.0%) experienced treatment failure. Specifically, in the CCRT arm, 24 patients experienced treatment failure: 5 had locoregional failure alone, 10 had distant metastases alone, and 9 had both locoregional failure and distant metastases. In the CCRT + E arm, 18 patients experienced treatment failure: 10 had locoregional failure alone, 5 had distant metastases alone, and 3 had both locoregional failure and distant metastases. The DMFS rate was significantly higher in the CCRT + E arm than in the CCRT arm. The 1-, 2-, and 5-year DMFS rates were 91.6% versus 94.8%, 82.3% versus 91.6%, and 67.0% versus 88.0% in the CCRT and CCRT + E arms, respectively (p = 0.029). No significant differences were found in OS, PFS, or LRFS. The 1-, 2-, and 5-year OS rates were 95.0% versus 98.3%, 90.0% versus 88.3%, and 67.3% versus 76.2% (p = 0.332), PFS rates were 88.3% versus 88.3%, 76.7% versus 83.3%, and 62.6% versus 71.7% (p = 0.338), and the LRFS rates were 90.0% versus 93.1%, 83.3% versus 87.7%, and 77.7% versus 79.1% (p = 0.881) in the CCRT and CCRT + E arms, respectively (Figure 2(a)–(d)).

Kaplan–Meier estimates of cumulative survival curves after treatment with concurrent chemoradiotherapy compared with concurrent chemoradiotherapy plus Endostar. (a) Progression-free survival. (b) Overall survival. (c) Distant metastasis-free survival. (d) Locoregional recurrence-free survival for all patients in CCRT and CCRT + E groups.
Prognostic factors
Univariable analysis revealed that a maximum tumor diameter > 4 cm, stage IIIA–IVA, and failure to achieve CR were significant predictors of shorter PFS, OS, and LRFS. Treatment without Endostar, stage IIIA–IVA disease, and failure to achieve CR were significant predictors of shorter DMFS. In the multivariable analysis, only a maximum tumor diameter > 4 cm and failure to achieve CR were identified as predictive factors indicating poor PFS. In addition, maximum tumor diameter > 4 cm and stage IIIA–IVA disease were factors indicating a poor prognosis with regard to OS. Stage IIIA–IVA disease was a significant predictor of shorter DMFS. The maximum tumor diameter was a significant predictor of shorter LRFS (Tables 2 and 3).
Univariate and multivariate analyses associated with PFS and OS.

Cox proportional hazard regression model for univariate and multivariate analyses.
CCRT, concurrent chemoradiotherapy; CCRT + E, concurrent chemoradiotherapy plus Endostar; OS, overall survival; PFS, progression-free survival.
Univariate and multivariate analyses associated with DMFS and LRFS.

Cox proportional hazard regression model for univariate and multivariate analyses.
CCRT, concurrent chemoradiotherapy; CCRT + E, concurrent chemoradiotherapy plus Endostar; DMFS, distant metastasis-free survival; LRFS, locoregional recurrence-free survival.
Subgroup analyses
In further subgroup analyses, we evaluated the effects of histology, maximum tumor diameter, FIGO stage, the presence of pelvic lymph node metastasis, and treatment response on PFS, OS, DMFS, and LRFS in the CCRT and CCRT + E arms. The results demonstrated that Endostar could significantly improved DMFS in patients with squamous cell carcinoma (p = 0.005), a maximum tumor diameter > 4 cm (p = 0.011), and stage IB2 or IIA2–IIB cervical cancer (p = 0.005). The other indicators were not significantly different between the two arms (p > 0.05; Tables 4 and 5).
Subgroup analysis with multiple testing correction of OS and PFS in CCRT versus CCRT + E for locally advanced cervical cancer.

Subgroup analyses were performed using the Kaplan–Meier method and Cox proportional hazards regression. To control the family-wise error rate arising from multiple comparisons, the Bonferroni P/2 correction was applied to adjust significance levels.
CCRT, concurrent chemoradiotherapy; CCRT + E, concurrent chemoradiotherapy plus Endostar; OS, overall survival; PFS, progression-free survival.
Subgroup analysis with multiple testing correction of DMFS and LRFS in CCRT versus CCRT + E for locally advanced cervical cancer.
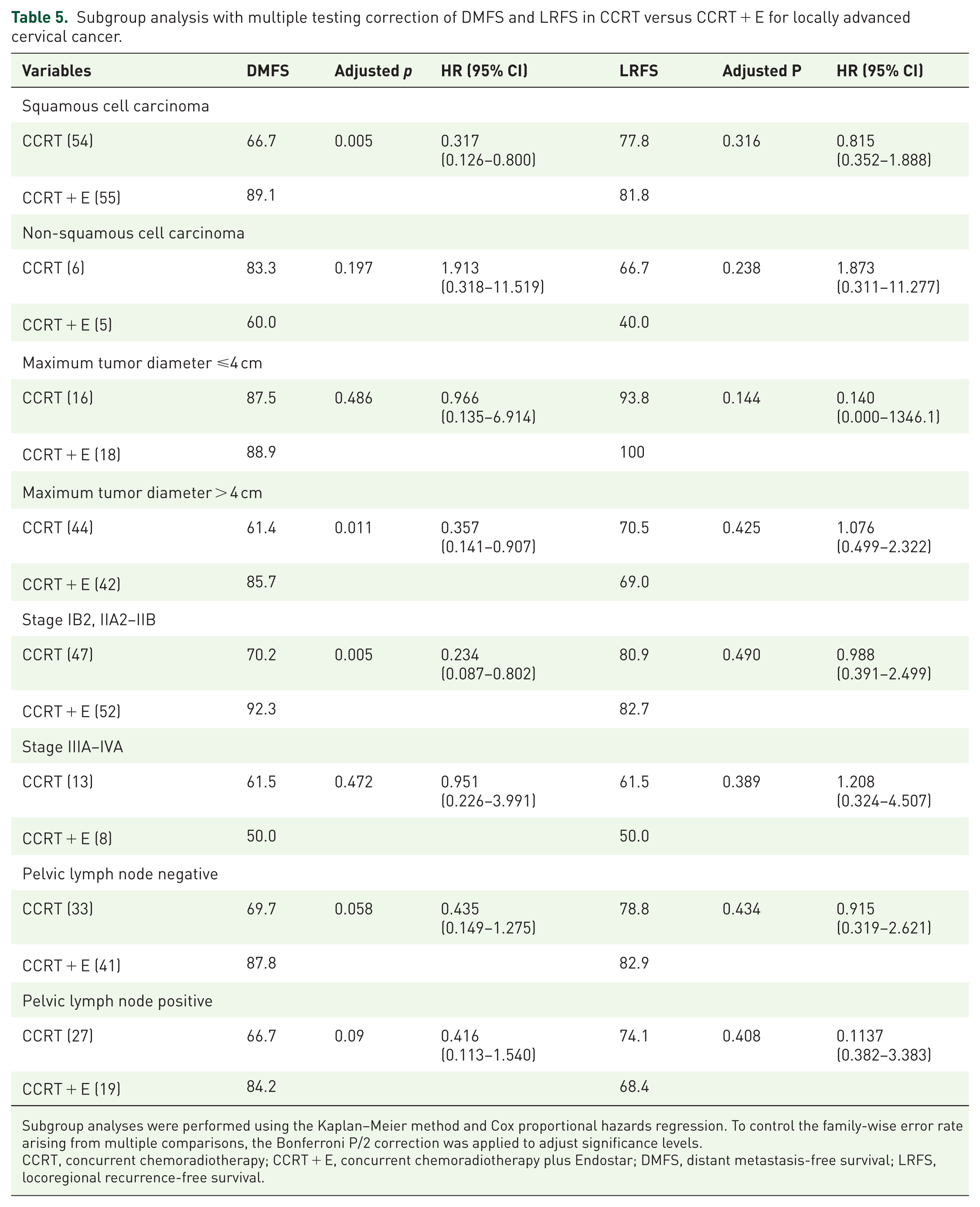
Subgroup analyses were performed using the Kaplan–Meier method and Cox proportional hazards regression. To control the family-wise error rate arising from multiple comparisons, the Bonferroni P/2 correction was applied to adjust significance levels.
CCRT, concurrent chemoradiotherapy; CCRT + E, concurrent chemoradiotherapy plus Endostar; DMFS, distant metastasis-free survival; LRFS, locoregional recurrence-free survival.
Therapy-related toxicities
Both arms had similar toxicity profiles. The most commonly observed acute toxicities were hematologic and gastrointestinal toxicities. Grade 1–2 bone marrow suppression was recognized in 31 patients (51.7%) and grade 3–4 bone marrow suppression was detected in 24 patients (40.0%) in the CCRT + E arm, compared with 26 patients (43.3%) and 28 patients (46.7%) in the CCRT arm, respectively (p = 0.592). Grade 1–2 gastrointestinal toxicity was identified in 42 patients (70.0%) and grade 3–4 gastrointestinal toxicity occurred in 4 patients (6.7%) in the CCRT + E arm, compared to 40 patients (66.7%) and 5 patients (8.3%) in the CCRT arm, respectively (p = 0.511). No statistically significant differences were observed in the incidence of grade 1–2 hepatic toxicity (8.3% vs 8.3%), renal toxicity (8.3% vs 3.3%), and bleeding (6.7% vs 5.0%) between the two arms, with all p > 0.05. No cardiac toxicity or hypertension was observed. The most commonly observed late toxicities, which manifested mainly as grade 1 or 2, were lower extremity lymphedema (5.0 % vs 6.7%), radiation proctitis (8.3% vs 5.0%), or radiation cystitis (1.7% vs 1.7%), in the two arms, with all p > 0.05. Only one patient experienced grade 3–4 radiation proctitis in the CCRT + E arm. There were no observations of grade 3–4 hepatic toxicity, renal toxicity, bleeding, lower extremity lymphedema, or radiation cystitis. Furthermore, no grade 5 toxicity was reported. The detailed data are shown in Table 6. The addition of Endostar to chemoradiotherapy was safe and well-tolerated.
Spectrum and incidence of treatment-related adverse events in the study cohort.

Toxicity incidence was analyzed using non-parametric statistical tests.
CCRT, concurrent chemoradiotherapy; CCRT + E, concurrent chemoradiotherapy plus Endostar.
Discussion
CCRT, consisting of radiotherapy and cisplatin-based chemotherapy, has been the standard treatment for LACC for nearly 20 years, yet its efficacy remains unsatisfactory. To improve the prognosis of LACC, a variety of strategies combining radiotherapy and chemotherapy have been adopted, including neoadjuvant chemotherapy plus CCRT,17,18 chemotherapy with brachytherapy, 19 and adjuvant chemotherapy after CCRT. 20 Nevertheless, no breakthrough in efficacy has been achieved, and more than 30% of patients with LACC eventually develop locoregional recurrences or distant metastases. 7 With a deeper understanding of the molecular biology and pathology involved in tumor initiation, development, and metastasis, the efficacy and safety of targeted therapy have been proven in multiple tumor types. It has become a novel therapeutic method combined with surgery, radiotherapy, and chemotherapy for patients with advanced disease.
Recently, the combination of angiogenesis inhibitors with chemoradiotherapy has become a new hot topic in the field of LACC treatment. As an anti-VEGF antibody, bevacizumab is capable of reducing tumor volume, postponing tumor growth, and suppressing tumor metastasis. The RTOG 0417 trial investigated chemoradiotherapy with bevacizumab among 49 patients with IB–IIIB stage cervical cancer and showed promising efficacy results. The 2- and 3-year OS rates were 89.8% and 81.3%. The OS was improved in this study compared to the results from RTOG 9001 (2- and 3-year OS rates of 80.2% and 76.8%, respectively). 21 However, the high incidence of side effects with bevacizumab has limited its widespread clinical application.9,11 Unlike the single-target VEGF-A inhibitor bevacizumab, Endostar is a novel antiangiogenic anti-VEGF target medication that was independently developed in China and can act on multiple targets such as VEGF, VEGF receptor-2 (VEGFR-2), and platelet-derived growth factor receptor (PDGFR), to improve the effectiveness of cancer therapy. 22 A retrospective clinical investigation revealed that LACC patients treated with chemoradiotherapy combined with Endostar had a greater CRR (48.8% vs 26.8%, p < 0.04), and no differences were observed in the ORR (82.9% vs 70.7%) and DCR (92.7% vs 80.5%) (p > 0.05). 23 An earlier study conducted by Shu et al. reported that, compared with CCRT alone, CCRT + Endostar significantly improved the CRR compared to the CCRT arm (83.33% vs 65.12%, p < 0.05). 24 Similarly, in this study, we found that the combination of Endostar with chemoradiotherapy significantly increased the CRR (68.3% vs 35.0%; p = 0.001) compared to the CCRT arm. This improvement was primarily driven by the conversion of PR to CR, evidenced by the reduction in PR proportion from 65.0% in the CCRT arm to 30.0% in the CCRT + E arm. The ORR remained comparably high in both arms (98.3% vs 100%; p = 1.000) with no significant difference observed. These findings are consistent with the results of the abovementioned studies and indicate that the addition of Endostar could have a favorable effect on patients with LACC.
Inspired by the marked short-term efficacy of Endostar and chemoradiotherapy in LACC, there have been ongoing efforts to improve survival rates. Overall, most studies have shown that Endostar does not improve 2-year survival rates. A retrospective study by Feng et al. grouped the patients with stage IIB–IVA cervical carcinoma based on whether they received Endostar or not. The results revealed that receiving Endostar did not significantly affect PFS (p = 0.323) or OS (p = 0.154) between the two groups. 23 Lu et al. reported that the 2-year PFS in patients with stage IB2–IVA cervical cancer in the CCRT + Endostar group was 80.6%, whereas it was 63.5% in the CCRT group (p = 0.091), and the corresponding 2-year OS rates were 85.6% and 70.0% (p = 0.212), respectively. Compared with CCRT alone, CCRT + Endostar significantly improved DMFS (1- and 2-year DMFS rates were 92.7% vs 81.1% and 86.0% vs 65.1%, respectively; p = 0.031). 25 The results of our study were similar to those of previous studies. However, most prior studies had short follow-up times, reporting only 2-year survival rates. Our study had a longer follow-up period of 53 months (range 8–81 months), and the results demonstrated that the 1-, 2-, and 5-year DMFS rates were 91.6% versus 94.8%, 82.3% versus 91.6%, and 67.0% versus 88.0% (p = 0.029) for the CCRT and CCRT + E arms, respectively. Compared with the CCRT arm, the CCRT + E arm had significantly improved DMFS. The lower distant metastasis rate observed in the CCRT + E arm might be attributable to the addition of Endostar to concurrent chemoradiotherapy, which increased the CR rate. This finding is in line with the findings of Beskow, who identified achieving CR as a strong prognostic factor for long-term survival. 26 Accordingly, a longer follow-up is needed to establish whether the increased rate of CR will translate into better long-term survival. While our study focused on cervical cancer, the demonstrated broad anticancer efficacy of endostatin-based therapies combined with chemoradiotherapy in other malignancies substantiates our observed outcomes. A 2021 meta-analysis by Yuan et al. in non-small cell lung cancer showed endostatin significant improved ORR (RR 1.263, 95% CI: 1.137–1.403, p < 0.001), disease control rate (DCR 1.274, 95% CI: 1.124–1.444, p < 0.001), and 1-year survival (1.113, 95% CI: 1.006–1.231, p = 0.038)), with manageable toxicity. 27 Similarly, Kang et al. 28 reported enhanced CRR (90.0% vs 80.7%, p = 0.022) and 3-year PFS (84.8% vs 75.1%, p = 0.011) with Endostar-chemoradiotherapy in locoregionally advanced nasopharyngeal carcinoma. Recent landmark trials further inform LACC management. KEYNOTE-A18 (2024) demonstrated pembrolizumab significantly improved 3-year OS when added to chemoradiotherapy (82.6% vs 74.8%; HR 0.67, 95% CI 0.50–0.90; p = 0.0040). 29 The EMBRACE II study (2025) achieved 89% 5-year LRFS, 75% OS, and 78% DMFS using precision radiotherapy (IG-IMRT + MR-IGABT) with concurrent cisplatin. 30 These outcomes are similar to ours. Unlike immune checkpoint inhibitors, Endostar’s efficacy in chemoradiotherapy combinations likely involves angiogenesis inhibition, improved oxygen availability, and induction of endothelial cell apoptosis.22,31,32 Our prior work demonstrated that Endostar significantly reduces vascular malformations and normalizes tumor blood flow during combination therapy. 33 Collectively, the demonstrated efficacy enhancement potential of combination approaches in locally advanced cervical cancer supports prioritizing strategic integration of antiangiogenics, immunotherapies, and precision radiotherapy in future clinical trial designs to maximize therapeutic benefit.
Previous studies reported that the most common acute toxicities associated with Endostar combined with chemoradiotherapy were myelosuppression and gastrointestinal toxicity, which were mainly grade 1–2. A meta-analysis of 13 studies suggested that the combined use of Endostar significantly increased the occurrence of gastrointestinal adverse reactions and hypertension; however, it did not affect treatment efficacy. 34 Another study revealed that CCRT + E increased the incidence of adverse cardiac reactions, digestive system reactions, and allergies. 25 Unlike the aforementioned studies, a recent study reported that the combined use of Endostar did not increase the treatment-related toxicities. 23 In this study, we found that the frequently observed acute adverse reactions were hematological, gastrointestinal toxicity, renal toxicity, and liver function damage. Patients in both arms had similar acute and late toxicity profiles. The safety profile of Endostar combined with chemoradiotherapy was consistent with the known profiles of the individual therapeutic components. The results suggested that Endostar did not worsen the known toxicities associated with chemoradiotherapy. In general, Endostar is safe, and the side effects are mild.
To provide potential insights into the selection of the patients who may benefit the most from treatment with Endostar combined with chemoradiotherapy, a subset analysis was conducted. Prior studies have shown that patients with positive VEGFR2 expression who were treated with CCRT + E tended to have a better ORR and PFS than those treated with CCRT alone. However, this difference was not statistically significant in the entire study population. 25 Another retrospective study by Feng et al. demonstrated that Endostar could significantly improve PFS in patients with stage IIB cervical cancer (p < 0.05). 23 As presented in Table 5, the results of the subgroup analysis demonstrated that Endostar could significantly improve DMFS in patients with squamous cell carcinoma, maximum tumor diameter > 4 cm, and stage IB2 or IIA2–IIB cervical cancer. These findings indicate that Endostar may not uniformly affect patients with various stages of locally advanced cervical cancer. However, there may be specific populations may benefit from its use. According to our research results, for patients with squamous cell carcinoma, a maximum tumor diameter > 4 cm, and stage IB2 or IIA2–IIB cervical cancer, Endostar combined with chemoradiotherapy is recommended.
Limitations
To our knowledge, this is the first phase II study to report the 5-year survival rate of LACC patients treated with Endostar combined with chemoradiotherapy in LACC. However, this study has several limitations. First, as a phase II clinical trial, it included a small sample size. Second, the follow-up time should be longer. Third, our study adopts simple randomization without stratification may introduce imbalance in baseline characteristics. When used with concurrent chemoradiotherapy, Endostar has the potential to further improve long-term survival rates. Therefore, we believe that it is imperative to initiate a well-designed, randomized phase III trial to properly evaluate the role of Endostar in combination with chemoradiotherapy for the treatment of patients with LACC.
Conclusion
The addition of Endostar to CCRT significantly enhanced tumor response (CRR) and reduced distant metastasis (DMFS) in LACC patients without increasing treatment toxicity, offering a promising therapeutic enhancement. Clinically, patients with squamous cell carcinoma, maximum tumor diameter > 4 cm, and FIGO stage IB2 or IIA2–IIB disease derived particularly robust DMFS benefits from the combination regimen, suggesting they should be prioritized for this approach. Although the 5-year DMFS results are encouraging, validation in a larger phase III study and longer follow-up are warranted before considering this regimen as a new standard treatment modality for LACC.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251379397 – Supplemental material for Efficacy of Endostar plus concurrent chemoradiotherapy in locally advanced cervical cancer: a multicenter, phase II randomized trial
Supplemental material, sj-docx-1-tam-10.1177_17588359251379397 for Efficacy of Endostar plus concurrent chemoradiotherapy in locally advanced cervical cancer: a multicenter, phase II randomized trial by Fang Wu, Xiaobi Tang, Wenqi Liu, Zhanxiong Luo, Haixing Huang, Meilian Liu, Hongqian Wang, Sihui Liao, Shanshan Ma, Li Jiang and Yong Zhang in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.