
Abstract
Background:
Mesothelioma is a rare and highly aggressive tumor that causes severe damage. However, there is a lack of systematic reports on the incidence and clinical characteristics of mesothelioma in the Chinese population.
Objectives:
This study aims to characterize the epidemiological features of mesothelioma in the Chinese population and to evaluate the effectiveness of current treatment strategies, to inform clinical decision-making and improve patient care.
Designs:
The epidemiological characteristics of patients were collected by regional study centers according to the predefined inclusion and exclusion criteria. Asbestos exposure status was clearly identified for each patient, and treatment strategies were analyzed across mesothelioma cases with different primary tumor sites.
Methods:
Data on mesothelioma patients and their treatment information were collected from 11 hospitals across China between January 2006 and December 2024. Epidemiological data and baseline characteristics were summarized using descriptive methods. The Kaplan–Meier method was used to analyze progression-free survival (PFS) and overall survival (OS). Key response indicators included the objective response rate (ORR) and disease control rate (DCR).
Results:
A total of 927 patients from 11 provinces in China were included in the analysis. The major types of mesothelioma observed were pleural mesothelioma (n = 537), peritoneal mesothelioma (n = 240), pericardial mesothelioma (n = 5), and mesothelioma of the tunica vaginalis testis (n = 5). Among these patients, 163 had confirmed asbestos exposure. For pleural mesothelioma, 45.6% (n = 245) of patients were from Yunnan Province. For peritoneal mesothelioma, 62.5% (n = 150) of patients were from Zhejiang Province. The median PFS rates for pleural and peritoneal mesothelioma patients were 6.6 and 5.7 months, respectively. The median OS was 16.6 months for pleural mesothelioma and 12.1 months for peritoneal mesothelioma. The ORR for pleural mesothelioma was 15%, with a DCR of 85.9%, while the ORR for peritoneal mesothelioma was 14.4%, with a DCR of 84.7%.
Conclusion:
The incidence of mesothelioma in China exhibits distinct regional characteristics. Pleural mesothelioma is predominantly associated with crocidolite asbestos exposure in Yunnan Province, while peritoneal mesothelioma is linked to hand-spun chrysotile asbestos exposure in Zhejiang Province, with notable sex differences observed. No significant differences in treatment outcomes were identified between pleural and peritoneal mesothelioma patients undergoing first-line therapy. These findings highlight the importance of region-specific strategies for the diagnosis and treatment of mesothelioma in China.
Introduction
Mesothelioma is a rare and highly aggressive tumor with a poor prognosis.1,2 According to the latest Chinese expert consensus, the primary sites of mesothelioma include the pleura, peritoneum, pericardium, and tunica vaginalis, with pleural mesothelioma being the most common. 3 In 2019, the estimated number of mesothelioma patients in China exceeded 380 million. 3 The World Health Organization reported that newly diagnosed mesothelioma cases accounted for 0.2% of all malignant tumors worldwide in 2020. 4 Globally, the crude incidence rate of mesothelioma is approximately 30 cases per million people. 5 With a deeper understanding of mesothelioma’s etiology, researchers have identified asbestos use and exposure as the major cause of the disease. 6 According to the Weinman international conference on mesothelioma, six types of asbestos—including chrysotile and crocidolite—have been used as commercial minerals and are confirmed to be associated with malignant mesothelioma. 7 In China, chrysotile asbestos exposure in the southeastern region has been linked to the incidence of peritoneal mesothelioma. 8 Research from Nordic countries has preliminarily shown that preventing asbestos exposure can improve survival outcomes for mesothelioma patients. 9 However, there remains a lack of large-scale studies to reflect the real-world incidence and epidemiology of mesothelioma in the Chinese population.
Regarding first-line treatment for mesothelioma, the combination of pemetrexed and cisplatin or carboplatin has been the standard therapy regimen. 10 More recently, the addition of bevacizumab to chemotherapy has demonstrated greater benefits for pleural mesothelioma patients, with an overall survival (OS) of 18.8 months. 11 The advent of immunotherapy has further advanced treatment options—the CheckMate-743 trial revealed the promising efficacy of nivolumab plus ipilimumab in untreated pleural mesothelioma patients, marking the first study to confirm the benefits of dual immunotherapy in this population. 12 Additionally, several studies have explored the potential advantages of combining immunotherapy with chemotherapy or bevacizumab for mesothelioma patients.13,14 While research on pleural mesothelioma has been extensive, other types of mesothelioma—such as peritoneal, pericardial, and tunica vaginalis mesothelioma—have received less attention in terms of treatment strategies.
To enhance understanding of the different types of mesothelioma, the current study aims to analyze the epidemiological characteristics and asbestos exposure-related risks among patients in China. Concrete statistical data were collected to provide fundamental references for mesothelioma prevention. Moreover, this study incorporated systematic therapy analyses to assess the efficacy of various treatment regimens, offering a comprehensive overview of real-world therapeutic practices. The findings could serve as a valuable resource for developing future treatment strategies and alternative options for mesothelioma patients.
Methods
Patient eligibility
Patients with pathologically confirmed mesothelioma, reviewed by pathologists from 11 different provinces in China—Zhejiang, Yunnan, Fujian, Anhui, Shanxi, Henan, Jiangxi, Hubei, Guangxi Zhuang Autonomous Region, Qinghai, and Jiangsu—between January 2006 and December 2024, were included. All data were retrospectively collected from hospitals located in the aforementioned regions. The research centers participating in this study include the following: Chuxiong Yi Autonomous Prefecture People’s Hospital, Zhejiang Cancer Hospital, Zhejiang Provincial People’s Hospital, Affiliated Jinling Hospital of Medical School of Nanjing University, Anhui Chest Hospital, Huzhou Central Hospital, The Second Affiliated Hospital of Guilin Medical University, Affiliated Jinhua Hospital of Zhejiang University School of Medicine, The First Affiliated Hospital of Wenzhou Medical University, Lishui Municipal Central Hospital, The First Affiliated Hospital of Xiamen University, The Second Affiliated Hospital of Nanchang University, The Cancer Hospital of Qinghai Province, The First Affiliated Hospital of Xinxiang Medical University, The 900th Hospital of the Joint Logistics Team, Union Hospital of Tongji Medical College of Huazhong University of Science and Technology, Hangzhou First People’s Hospital, Quhua Hospital, Quzhou People’s Hospital, Fujian Cancer Hospital, and Bethune Hospital of Shanxi Province.
Primary medical records completed by the treating physicians were collected according to uniform criteria across all research centers. Mesothelioma was classified into four major subtypes: pleural mesothelioma, peritoneal mesothelioma, pericardial mesothelioma, and mesothelioma of the tunica vaginalis testis. Patients at all stages were eligible for analysis. Baseline characteristics, including sex, age, performance status, pathological type, sites of metastases, smoking history, surgical history, and radiotherapy history, were recorded. For patients with confirmed asbestos exposure, details such as the site of exposure and duration were also documented. Asbestos exposure can occur in workplaces, schools, homes, or military settings, with occupational exposure being the most common. Family members of asbestos workers may also be at risk of secondary exposure. Other sources include household products, talcum powder, or damaged asbestos in old homes and buildings. There is no safe level of asbestos exposure, and both the intensity and duration of exposure influence the risk of asbestos-related diseases. Therefore, exposure duration was incorporated into our analysis to establish a comprehensive assessment method for asbestos exposure. All relevant asbestos exposure data were sourced from the electronic medical records maintained by each participating study center.
Exclusion criteria included patients with severe underlying diseases, other malignancies, or abnormal liver and kidney function. Individuals with severe infectious diseases—such as hepatitis, acquired immune deficiency syndrome, or tuberculosis—were also excluded. Patients with biphasic mesothelioma involving both the pleura and peritoneum were not included in this study. The research adhered to the Declaration of Helsinki, and individual consent was waived across all research centers. The study was approved by the leading institutional review board of Chuxiong Yi Autonomous Prefecture People’s Hospital (approval number: IRB-2025-017). The reporting of this study conforms to the statement of ESMO Guidance for Reporting Oncology real-world evidence. 15
Treatment methods
Patients who received systemic treatment were included in survival analyses, and their therapy regimens were recorded. The most common first-line treatments were a combination of pemetrexed and cisplatin, or a triple regimen of pemetrexed, cisplatin, and bevacizumab. For patients intolerant to cisplatin, carboplatin was allowed as a substitute. Less common regimens, such as paclitaxel with cisplatin or carboplatin, were also analyzed. Immunotherapy was primarily represented by nivolumab plus ipilimumab. Single-agent immunotherapy combined with chemotherapy or anti-angiogenic therapy was permitted. All treatment regimens and dosages followed clinical guidelines and recommendations from relevant clinical trials. Each therapy cycle was scheduled every 3 weeks, with adjustments made based on patient condition. To clarify the overall treatment strategy, the regimens were classified into three main subgroups: C (chemotherapy alone), C + A (chemotherapy combined with anti-angiogenic therapy), and Contain I (chemotherapy combined with immunotherapy or dual immunotherapy).
Survivals and follow-up
Progression-free survival (PFS) and OS were the primary survival outcomes. PFS was defined as the time from initiation of systemic therapy to disease progression, while OS was calculated from the start of systemic therapy to death from any cause or the last follow-up. The final follow-up date was December 31, 2024.
Responses
All patients receiving systemic therapy underwent response evaluations. Baseline tumor size was assessed using computed tomography (CT). CT scans were conducted every two therapy cycles to monitor efficacy and adjust treatment strategies. In cases of disease progression, CT results were recorded. Magnetic resonance imaging or bone scans were incorporated when necessary. Ultrasonography was used to evaluate lymph node involvement. Tumor response was assessed according to the Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST 1.1). Response indicators included objective response rate (ORR)—the sum of complete response (CR) and partial response (PR)—and disease control rate (DCR), which comprised CR, PR, and stable disease (SD). Progressive disease (PD) indicates ineffective treatment.
Statistical analyses
Baseline characteristics and epidemiological data were analyzed using descriptive statistics. Kaplan–Meier analysis was used to generate survival curves, and comparisons between groups were performed using the log-rank test. A p-value <0.05 was considered statistically significant. Statistical analyses and visualizations were conducted using the Statistical Package for Social Sciences software (version 25; IBM, Armonk, NY, USA) and GraphPad Prism software (version 9; GraphPad Software, San Diego, CA, USA).
Results
Patient characteristics
The baseline characteristics of patients with mesothelioma are summarized in Table 1. A total of 927 patients were included in the analysis, with 52.6% (n = 488) being male and 47.4% (n = 439) female. The majority of mesothelioma patients (70.4%, n = 653) were aged 65 years or younger. Regarding performance status, 641 patients had an ECOG performance status of 0–1, while the performance status for 146 patients was uncertain.
Summary of baseline profiles for all patients with mesothelioma.

Mesothelioma cases originated from four primary sites: pleural mesothelioma (n = 537), peritoneal mesothelioma (n = 240), pericardial mesothelioma (n = 5), and mesothelioma of the tunica vaginalis testis (n = 5). The origin was uncertain for approximately 140 patients. Pathologically, the cases included epithelioid mesothelioma (n = 420), sarcomatoid mesothelioma (n = 37), and biphasic mesothelioma (n = 32). Most patients (69%) were diagnosed at stage IV. Regarding medical history, 249 patients had a history of smoking, 462 had a history of surgery, and 53 had received radiotherapy.
The baseline characteristics of patients with pleural and peritoneal mesothelioma are detailed in Table 2. Significant differences were observed between pleural and peritoneal mesothelioma patients in terms of sex, age, performance status, pathological type, smoking history, receipt of systemic therapy, history of surgery, and radiotherapy. However, no significant differences were found between the two groups in terms of disease stage.
Baseline characteristics of patients with pleural and peritoneal mesothelioma.

Among pleural mesothelioma patients, 60.5% were male and 39.5% female, whereas peritoneal mesothelioma patients comprised 29.6% male and 70.4% female. Regarding age, 163 pleural mesothelioma patients and 56 peritoneal mesothelioma patients were older than 65 years. Performance status of 0–1 was observed in 63.1% of pleural mesothelioma patients and 89.6% of peritoneal mesothelioma patients. Systemic therapy was administered to 345 pleural mesothelioma patients and 178 peritoneal mesothelioma patients.
Epidemiology characteristics
The study analyzed 927 patients from 11 provinces in China, including Zhejiang, Yunnan, Fujian, Anhui, Shanxi, Henan, Jiangxi, Hubei, Guangxi Zhuang Autonomous Region, Qinghai, and Jiangsu, between January 2006 and December 2024. Figure 1 illustrates the geographical distribution of patients. Zhejiang (n = 350) and Yunnan (n = 245) provinces were the primary regions of mesothelioma cases, followed by Fujian (n = 196).
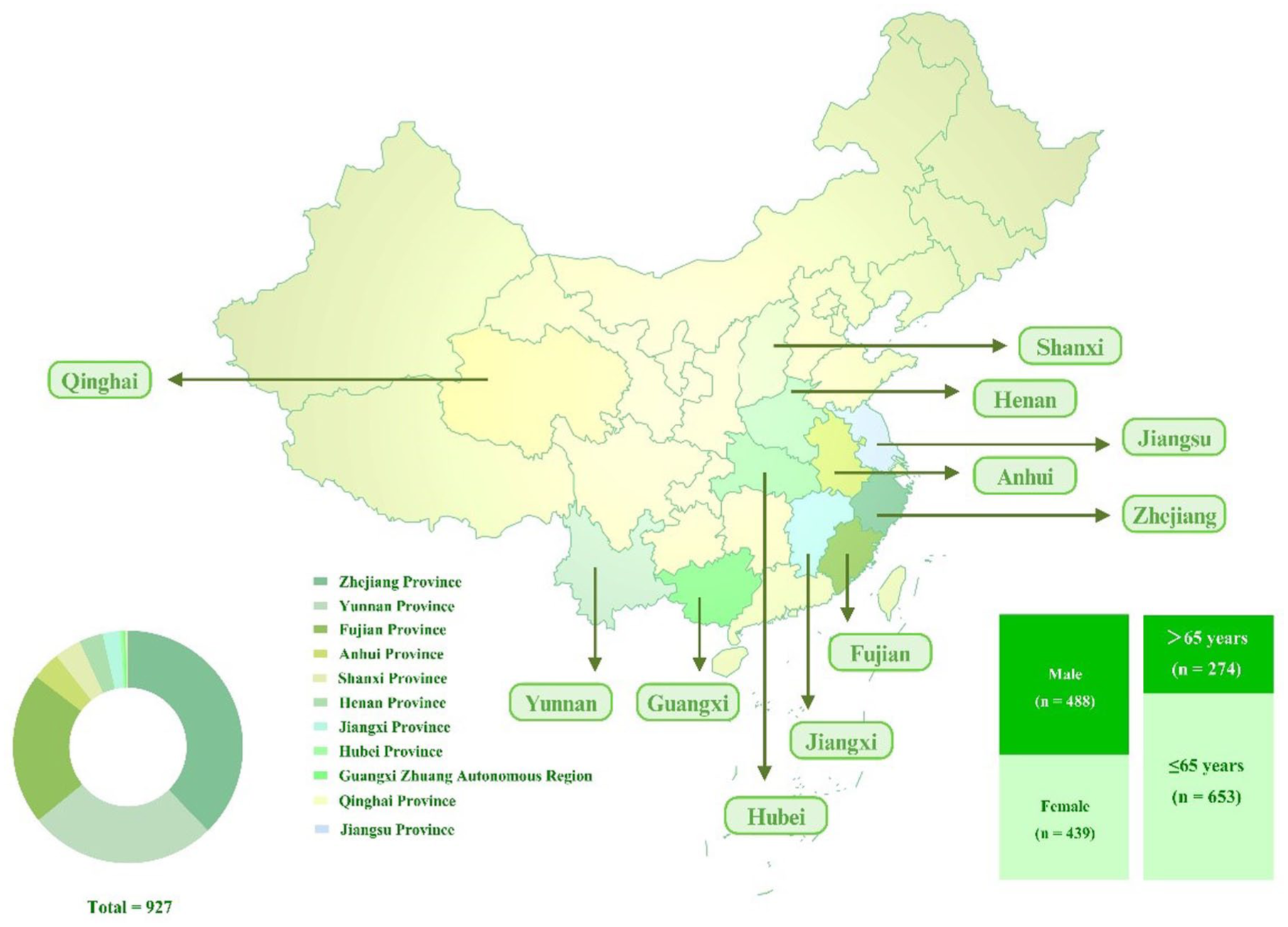
Distribution and characteristics of mesothelioma patients in China.
Pleural mesothelioma was the most common site of origin in this study (57.9%), followed by peritoneal mesothelioma (25.9%; Figure 2(a)). Among the pathological types, epithelioid mesothelioma was the most common (45.3%), with sarcomatoid, biphasic, and other types accounting for 4.0%, 3.5%, and 6.4%, respectively (Figure 2(b)).

Basic characteristics for patients. (a) The different histological origins for mesothelioma patients include pleural mesothelioma, peritoneal mesothelioma, pericardial mesothelioma, mesothelioma of tunica vaginalis testis, and other origins. (b) The different pathological types include epithelial mesothelioma, sarcomatoid mesothelioma, biphasic mesothelioma, and other types. (c) A certain history of asbestos exposure in certain regions and their sustained exposure time. (d) Stages for all mesothelioma patients and concrete sites of metastases.
A total of 163 patients reported confirmed asbestos exposure, mainly from Yunnan (n = 144), Zhejiang (n = 18), and Fujian (n = 1). Among these patients, 107 (65.6%) had an exposure history of more than 10 years, while 56 patients had an exposure history of less than 10 years (Figure 2(c)). Crocidolite asbestos was the primary cause of mesothelioma in Yunnan, while hand-spun chrysotile asbestos was prevalent in Zhejiang. Notably, all mesothelioma cases in Yunnan were pleural mesothelioma. Patients from Yunnan and Zhejiang accounted for 45.6% (n = 245) and 31.7% (n = 170) of pleural mesothelioma cases, respectively. For peritoneal mesothelioma, 62.5% (n = 150) were from Zhejiang.
Among the mesothelioma patients, 69% were diagnosed at stage IV. Metastatic sites were documented in 558 patients, with pericardial metastases in 19 patients, lung metastases in 75, liver metastases in 62, bone metastases in 68, and brain metastases in 12 (Figure 2(d)).
Survival analyses
Survival analysis included patients with pleural and peritoneal mesothelioma. The median PFS for pleural mesothelioma was 6.6 months (95% confidence intervals (CI): 5.6–7.6 months; Figure 3(a)), and the median OS was 16.6 months (95% CI: 14.3–18.9 months; Figure 3(b)). For peritoneal mesothelioma, the median PFS was 5.7 months (95% CI: 4.6–6.9 months; Figure 3(c)), and the median OS was 12.1 months (95% CI: 7.9–16.3 months; Figure 3(d)).
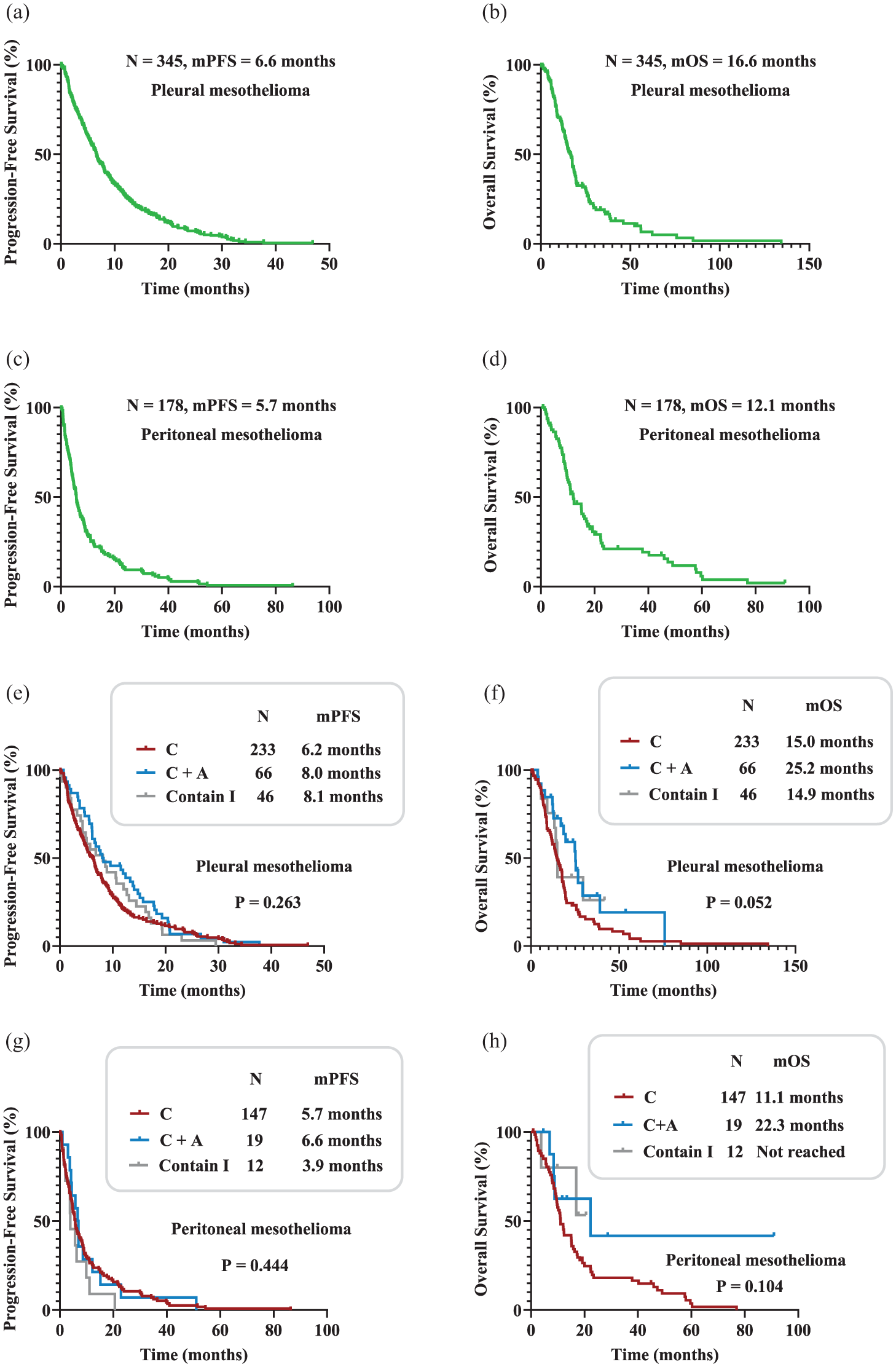
Kaplan–Meier estimates of PFS and OS. (a) PFS in all patients with pleural mesothelioma (n = 345, mPFS = 6.6 months). (b) OS in all patients with pleural mesothelioma (n = 345, mOS = 16.6 months). (c) PFS in all patients with peritoneal mesothelioma (n = 178, mPFS = 5.7 months). (d) OS in all patients with peritoneal mesothelioma (n = 178, mOS = 12.1 months). (e) PFS differences in all pleural mesothelioma patients with different therapy regimens (6.2 vs 8.0 vs 8.1 months, p = 0.263). (f) OS differences in all pleural mesothelioma patients with different therapy regimens (15.0 vs 25.2 vs 14.9 months, p = 0.052). (g) PFS differences in all peritoneal mesothelioma patients with different therapy regimens (5.7 vs 6.6 vs 3.9 months, p = 0.444). (h) OS differences in all peritoneal mesothelioma patients with different therapy regimens (11.1 vs 22.3 vs not reached, p = 0.104).
Therapy regimen analysis showed no significant differences in PFS among pleural mesothelioma patients receiving chemotherapy, chemotherapy combined with anti-vascular therapy, and Contain I regimens of chemotherapy combined with immunotherapy or double immunotherapy (6.2 vs 8.0 vs 8.1 months, p = 0.263; 95% CI: 5.1–7.4, 2.8–13.2, 3.9–12.4 months; Figure 3(e)). OS differences were also not statistically significant (15.0 vs 25.2 vs 14.9 months, p = 0.052; 95% CI: 11.9–18.1, 17.6–32.8, 13.4–16.4 months; Figure 3(f)).
Similarly, peritoneal mesothelioma patients showed no significant differences in PFS (5.7 vs 6.6 vs 3.9 months, p = 0.444; 95% CI: 4.5–7.0, 5.2–8.0, 1.0–6.8 months; Figure 3(g)) or OS (11.1 vs 22.3 vs not reached, p = 0.104; 95% CI: 9.0–13.1 months; 0–48.3 months, not reached; Figure 3(h)) across the three therapy regimens.
Clinical efficacy
The clinical efficacy of different therapies for pleural and peritoneal mesothelioma is detailed in Table 3. Among pleural mesothelioma patients, 220 underwent efficacy evaluations, with an ORR of 15% and a DCR of 85.9%. For peritoneal mesothelioma, 118 patients were evaluated, yielding an ORR of 14.4% and a DCR of 84.7% (Figure 4(a)–(d)).
Efficacy evaluation of pleural and peritoneal mesothelioma.
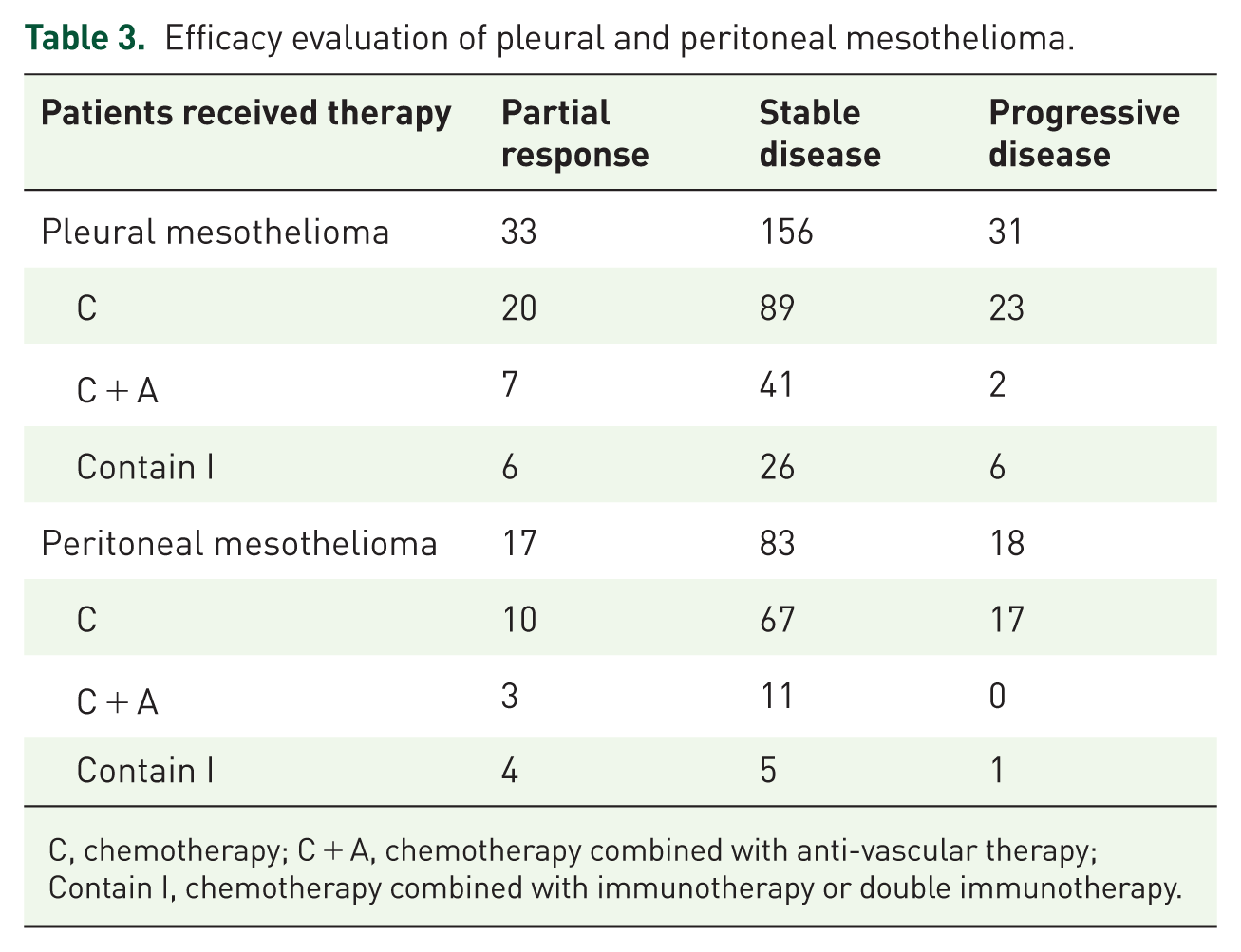
C, chemotherapy; C + A, chemotherapy combined with anti-vascular therapy; Contain I, chemotherapy combined with immunotherapy or double immunotherapy.

Efficacy evaluation for patients. Efficacy evaluation for (a) all patients with pleural mesothelioma; (b) all pleural mesothelioma patients with different therapy regimens; (c) all patients with peritoneal mesothelioma; and (d) all peritoneal mesothelioma patients with different therapy regimens.
For pleural mesothelioma patients receiving chemotherapy, 20 achieved PR, and 89 had SD. Among those treated with chemotherapy combined with anti-vascular therapy, 7 achieved PR, 41 had SD, and 2 had PD. Patients on Contain I regimens combining chemotherapy with immunotherapy or double immunotherapy showed 6 PR and 26 SD cases.
For peritoneal mesothelioma, 10 chemotherapy patients achieved PR, and 67 had SD. Among those receiving combined anti-vascular therapy, 3 achieved PR, and 11 had SD. Contain I regimen recipients reported 4 PR and 5 SD cases, with only one patient experiencing PD.
Discussion
To the best of our knowledge, the current study is the first to systematically analyze the epidemiology of mesothelioma, its clinical characteristics, and the impact of asbestos exposure in the Chinese population. The results revealed distinct regional characteristics and patterns of mesothelioma distribution, particularly in Zhejiang and Yunnan provinces. The type of asbestos exposure had a significant influence on mesothelioma patients. In Yunnan, crocidolite asbestos was the primary exposure, while in Zhejiang, hand-spun chrysotile asbestos from small workshops was the leading cause of peritoneal mesothelioma. Regarding treatment, different therapeutic regimens did not show a significant survival difference in pleural mesothelioma, with a similar trend observed in peritoneal mesothelioma. Furthermore, this study compared the characteristics of pleural and peritoneal mesothelioma, highlighting notable differences between the two, which could provide useful insights for clinical practice in the future.
Genetic mutations and environmental factors, such as asbestos exposure, contribute to the development of mesothelioma. Previous studies have identified BAP1 mutations as being prevalent in mesothelioma patients,16,17 and other genes such as CDKN2A, CDKN2B, and NF2 have also been linked to the disease.18,19 The focus of mesothelioma research has largely been on environmental factors and the interaction between genetic mutations and environmental exposures. According to estimates, approximately 29,300 people die from mesothelioma annually, 20 with nearly 80% of cases linked to asbestos exposure. 21 While erionite exposure has also been suggested as a risk factor for mesothelioma, it remains a rare cause confined to specific areas. 22 As carcinogenic mineral fibers, six minerals (five amphiboles and one serpentine-chrysotile) were used commercially before being banned. 23 The fiber structure facilitates the aggregation of macromolecules, leading to chronic inflammation. 24 Moreover, the activation of asbestos fibers by macrophages results in the release of cytokines and reactive oxygen species, which cause DNA damage and interfere with DNA repair mechanisms. 25 The increased susceptibility to carcinogenesis in environments exposed to carcinogens further contributes to mesothelioma development. 26
In the present study, significant asbestos exposure was observed in certain regions of China. In Yunnan Province, exposure to crocidolite asbestos primarily affected male patients, with the majority suffering from pleural mesothelioma. Liu et al. 27 ’s report also highlighted the impact of crocidolite exposure on the incidence of pleural mesothelioma in Dayao County, Yunnan. By contrast, in Zhejiang Province, people working in small workshops producing hand-spun chrysotile asbestos were mostly women, and peritoneal mesothelioma was the predominant type in this group. A similar trend was noted in a small-scale study from Yuyao, Zhejiang. 28 According to incomplete statistics from the Dayao County Center for Disease Control and Prevention since 2013, among the county’s population of 280,000, at least 21 deaths from pleural mesothelioma are reported annually, with the number exceeding 35 in some years. Mesothelioma ranks as the fifth leading cause of cancer-related death in Dayao County. In rural Zhejiang Province, the asbestos product industry once thrived, especially along National Highway 329 in the Cixi and Yuyao regions. During the 1980s, asbestos processing workshops were widespread in this area, with some villages described as having “every household spinning asbestos.” The high incidence of peritoneal mesothelioma in Yuyao and Cixi is closely linked to working conditions. There, asbestos processing was largely carried out in small workshops, where people lived and worked in the same space. This significantly increased the risk not only of inhaling asbestos but also of ingesting it. By contrast, asbestos exposure in Yunnan mainly stems from mining activities. Workers typically returned home after work, and daily living took place away from the mines. As a result, while the risk of inhalation was high, the likelihood of accidental ingestion was relatively low.
Overall, regional environmental factors played a key role in determining the types of mesothelioma observed in different areas of China. Amphibole asbestos types, including crocidolite, have been completely banned nationwide in China since July 2002. The only exception is chrysotile, which is still permitted for limited use under strict occupational health regulations and exposure limits. To further explore the impact of asbestos exposure, research has shown that asbestos bans correlate with a decline in mesothelioma incidence. 29 However, even after the ban, elevated mortality rates persist due to the long latency period of asbestos exposure, which can last up to 40 years in some Western countries. 30 Future studies are needed to investigate whether other factors contribute to mesothelioma incidence.
Regarding the treatment of advanced mesothelioma, traditional chemotherapy with pemetrexed and cisplatin remains the gold standard. The addition of bevacizumab to this regimen has been shown to improve survival by nearly 3 months. 11 In our current study, chemotherapy combined with an anti-angiogenic regimen appeared to improve OS in patients with pleural mesothelioma. However, the difference did not reach statistical significance. Researchers have suggested that anti-angiogenic agents may offer clinical benefits, particularly in patients with pleural effusion. Nevertheless, the overall response rate remains suboptimal, which needs further investigation in the prospective study. Some clinical trials have explored new immunotherapy options, but single-agent immunotherapy targeting cytotoxic T-lymphocyte-associated protein 4 has not demonstrated significant efficacy in improving survival. 31 By contrast, the CheckMate 743 trial demonstrated improved OS with the combination of ipilimumab and nivolumab in patients with pleural mesothelioma, with an OS of 18.1 months compared to 14.1 months with chemotherapy alone. 32 Other studies, such as those evaluating tremelimumab combined with durvalumab, have shown promising results with an OS of 16.6 months. 33 The DREAM trial, which investigated durvalumab with first-line chemotherapy, reported a PFS of 6 months, 34 while a phase II trial of durvalumab with platinum-pemetrexed showed an OS of 20.4 months. 35 In our study, no significant survival differences were observed between different therapeutic regimens in pleural and peritoneal mesothelioma. However, chemotherapy combined with bevacizumab showed potential treatment benefits, with OS of 25.2 months in pleural mesothelioma and 22.3 months in peritoneal mesothelioma. Nevertheless, further research with larger sample sizes is needed to identify optimal treatment strategies for mesothelioma in clinical practice. Despite the distinct biological characteristics between pleural and peritoneal mesothelioma, treatment regimens did not exhibit a significant difference. The feasibility and dissemination of specialized therapeutic regimens for diverse patient populations remain to be fully explored. There remains a need for further research to optimize treatment strategies for mesothelioma patients based on tumor site of origin, especially for the pericardial mesothelioma and mesothelioma of the tunica vaginalis testis. Due to the rarity of these subtypes, collaborative multicenter registries and case series are encouraged to better characterize clinical behavior, molecular profiles, and treatment outcomes, thereby guiding evidence-based management in the future. Recently, our team published the expert consensus on the diagnosis and treatment of malignant pericardial mesothelioma, which may provide an option for patients. And the series of consensus on mesothelioma of the tunica vaginalis testis was under discussion, which may supplement the diagnostic and therapeutic strategies for rare subtypes of mesothelioma. At the same time, further exploration of therapy targets and biomarkers to guide clinical decision-making is required. Currently, research on biomarkers for mesothelioma remains limited. Previous studies have identified the potential of several biomarkers, including alterations in NF2, BAP1, and CDKN2A genes. Region-specific cohort studies from areas with high asbestos exposure, such as Yunnan and Zhejiang Province, offer valuable opportunities for the identification of early diagnostic markers. Large-scale, multi-omics analyses—including transcriptomics, methylomics, and proteomics—are warranted to uncover molecular targets with distinct characteristics relevant to the Chinese population.
There are several limitations to this study. First, patient data from certain areas of China were not collected, which should be addressed in future research. Second, some basic information, such as smoking history, was unavailable. Additionally, the sample size for certain therapy subgroups was insufficient, especially for the combination regimen, and there was a lack of research on mesothelioma originating from the pericardium and tunica vaginalis, which should be explored further. Besides, a proportion of cases in our cohort were categorized as an unknown subgroup, including the tumor origin and some pathological subtypes, which means that this missing information may introduce bias and limit the interpretability of subgroup analyses. Future studies with more complete pathological data are warranted to validate and expand upon these findings. The present study collected data from selected hospitals across 11 provinces in China. However, this sampling approach is not ideal for accurately assessing the true incidence of this disease in the general population. The limitation is particularly evident given that not all cancer centers within these provinces participated in the study. Therefore, future research should aim to establish population-based cohort studies that systematically collect data on asbestos exposure in healthy individuals and conduct long-term follow-up to determine how many eventually develop mesothelioma. Such an approach would enable a more accurate estimation of the population-level incidence of mesothelioma. And further studies should also investigate additional therapeutic regimens to provide alternative options for mesothelioma patients.
Conclusion
The incidence of mesothelioma exhibits regional characteristics. In Yunnan Province, pleural mesothelioma is primarily caused by crocidolite asbestos exposure, while in Zhejiang Province, hand-spun chrysotile asbestos exposure is the leading cause of peritoneal mesothelioma. These findings highlight the regional variations in the origins of mesothelioma. In Yunnan, the mining industry is associated with a high risk of inhaling crocidolite asbestos, while in Zhejiang, the small workshops where people produce hand-spun chrysotile asbestos lead to increased accidental ingestion. Pleural mesothelioma predominantly affects males, while peritoneal mesothelioma is more common in females. As for treatment, no significant survival difference was observed between different regimens in pleural mesothelioma. Peritoneal mesothelioma showed similar results.