
Abstract
Background:
Depression and anxiety are common among patients with breast cancer, but prospective studies of depression and anxiety after radiotherapy (RT) among these patients remain scarce.
Objective:
To evaluate the prevalence of and changes in depression and anxiety among patients with breast cancer from the first day of RT (T0) to 6 months post-RT, and to identify risk factors associated with depression and anxiety and higher levels of them over time.
Design:
This observational study used a prospective, longitudinal design.
Methods:
This study was conducted in China between August 2022 and August 2023. Depression and anxiety were measured, respectively, by Patient Health Questionnaire and the Generalized Anxiety Disorder Scale, from T0 to 6 months post-RT. Univariate and multivariate logistic regressions were performed to explore risk factors for baseline depression and anxiety. Generalized Estimating Equations were performed to evaluate changes in depression and anxiety and risk factors for higher levels of them over time.
Results:
A total of 504 patients completed baseline questionnaires (response rate: 90.9%). The prevalence of depression and anxiety decreased significantly over time, from 37.3% and 26.0% at T0, to 28.4% and 20.3% at 6 months post-RT, respectively. Having a family history of cancer and receiving anti-HER2-targeted therapy were independently associated with depression at T0, and premenopausal status, poor family income, and self-reported menopausal symptoms were independently associated with both depression and anxiety at T0. Receiving anti-HER2-targeted therapy, having a lower personal income, and living in rural areas were associated with higher depression levels over time, whereas poor family income and self-reported menopausal symptoms were associated with higher anxiety levels over time.
Conclusion:
Depression and anxiety levels were high among patients with breast cancer receiving RT and decreased over time from pre-RT to 6 months post-RT. Routine screening is necessary, especially for high-risk patients.
Plain language summary
Introduction
According to Global Cancer Statistics 2022, breast cancer remains the most frequent cancer (both cases and deaths) in women. 1 Mental health problems, particularly anxiety and depression, among patients with breast cancer are becoming more prominent with improved prognosis due to advances in screening and treatment.2,3 The estimated prevalence of depression and anxiety among patients with breast cancer was 30%–40% worldwide in the past 20 years,4,5 and these prevalence rates were as high or higher (27%–50%) in China during this time. 6 While symptoms of depression and anxiety in patients with breast cancer tend to improve after treatment, they may persist beyond 5 years after diagnosis.7–10 However, most previous studies mainly focused on the follow-up of patients with breast cancer after they received surgery or chemotherapy.
Radiotherapy (RT) is an integral treatment modality for breast cancer, but most patients have limited knowledge or hold preconceived notions about RT, thereby leading to a substantial increase in anxiety and depression.11,12 Previous studies reported that patients generally had lower prevalence rates of depression and anxiety after RT than they did before RT.13,14 However, most studies have been conducted in Western countries, with limited research conducted in the Asian context, particularly China. Moreover, previous research focusing on continuous follow-ups of depression and anxiety after RT among patients with breast cancer is limited.
Several sociodemographic variables are associated with anxiety and depression among patients with breast cancer, including age,15–18 marital status,13,15,19,20 religion,15,19 education level,16,19,21 place of residence, 19 and financial status.15,17,18,20,22 However, previous results about these variables have been inconsistent. Furthermore, little longitudinal research has been conducted on the risk factors associated with high levels of depression and anxiety among patients with breast cancer who received RT. Early identification of patients in this population who have a high risk for depression and anxiety is essential for timely and targeted interventions.
Therefore, we conducted this prospective observational study of breast cancer patients receiving RT. We aimed to evaluate the prevalence of and longitudinal changes in depression and anxiety symptoms from pre-RT to 6 months post-RT, and to identify the clinical and sociodemographic variables associated with baseline depression and anxiety and higher levels of depression and anxiety over time.
Materials and methods
Study design and participants
This prospective observational study was conducted at our institution between August 2022 and August 2023. Patients were recruited if they met the following criteria: (1) women over 18 years of age; (2) diagnosed with breast cancer and received RT; (3) had an education level of primary school or higher; and (4) had no speech or hearing impairments. Patients who had a history of previous mental disorders or RT, could not complete the questionnaires independently, or refused to participate, were excluded from the study. The reporting of this study conforms to the STROBE statement for reporting observational studies (see Supplemental File 1).
Measures and data collection
All questionnaires were administered through an online platform. Trained physicians first introduced the purpose and protocols of the study, the rules of confidentiality, and precautions about filling in the electronic questionnaires. Each participant then used this online platform to create an account and complete a questionnaire that collected their sociodemographic information at baseline before the initiation of RT. Each participant’s electronic medical records were reviewed by physicians for clinical information collected at the end of the RT.
Depression symptoms were measured by the Patient Health Questionnaire (PHQ-9), which consists of nine items that are all rated from 0 (not at all) to 3 (almost every day). The Total score indicates the severity of depression, categorized as 0–4 (no), 5–9 (mild), 10–14 (moderate), 15–19 (moderately severe), and 20–27 (severe). 23 Anxiety symptoms were measured by the Generalized Anxiety Disorder Scale (GAD-7), which consists of seven items that are all rated from 0 (not at all) to 3 (almost every day). The Total score indicates the severity of anxiety, categorized as 0–4 (no), 5–9 (mild), 10–14 (moderate), and 15–21 (severe). 24 Higher scores on the PHQ-9 and GAD-7 indicate higher levels of depression and anxiety, respectively. The Chinese versions of the PHQ-9 and GAD-7 have been demonstrated to have good reliability and validity.25,26 Total scores >4 on the PHQ-9 or GAD-7 indicate the presence of depression or anxiety symptoms, respectively.23,24 Patients with a PHQ-9 or a GAD-7 ⩾10 were recommended to be referred to the psychiatry department for further evaluation and treatment according to China’s management guidelines for breast cancer follow-up and healthcare. 27
Participants completed the PHQ-9 and GAD-7 five times: before RT—on the first day of the RT course (T0), during RT (T1), at the end of RT (T2), and 1 month (T3) and 6 months post-RT (T4). They completed the questionnaires at these specific points by scanning a QR code using a smartphone or clicking a link sent to them via a short message service.
Statistical analysis
Categorical variables are presented as frequencies (percentages). Though the PHQ-9 and GAD-7 scores were not normally distributed at the follow-up points, they are presented as means to facilitate comparisons between the current study and previous studies. Mean PHQ-9 and GAD-7 scores were analyzed as continuous variables. Univariate and multivariate logistic regressions were performed on PHQ-9 and GAD-7 scores >4 as dependent variables to explore the risk factors for depression and anxiety at T0. Variables with a p < 0.10 in the univariate analyses were entered into the multivariate analysis. The sample size in this study met the requirements that the outcome event should be at least 10 times the number of independent variables in a multivariate model. There was no collinearity among the variables in the multivariate model, as the variance inflation factor for all the variables was less than 10.
Longitudinal analyses were conducted on changes in depression and anxiety levels from T0 to T4, and the risk factors for higher levels of depression and anxiety over time. The analyses were performed with Generalized Estimating Equations (GEEs) using a log link function for mean scores because of the non-normal distribution of the data. The choice of the most suitable working correlation matrix was based on the lowest quasi-likelihood under the independence model criteria. Given that the missing data on the questionnaires were random, they were treated as being missing at random.
A two-tailed p < 0.05 was chosen as the level of statistical significance for most analyses. However, the level of statistical significance for the GEE analysis was set at p < 0.01 to account for multiple testing. Statistical analyses were performed with R 3.6.3 software and SPSS 26.0 (IBM, Armonk, NY, USA). Graphs were created using GraphPad Prism 9.0 (GraphPad Software, San Diego, CA, USA).
Results
Patient characteristics
A total of 552 patients met the eligibility criteria (see Supplemental File 2), 48 of whom declined to participate in the study. Of the 504 participants, all completed the baseline questionnaires, and 458 patients completed all five assessments of depression and anxiety (response rate = 90.9%). Table 1 summarizes the results of the clinical and sociodemographic variables. All patients underwent either breast-conserving surgery or a mastectomy, except for two patients who were initially diagnosed with inoperable stage IV disease.
Univariable and multivariable logistic regression analyses of risk factors for PHQ-9 > 4 and GAD-7 > 4 at baseline pre-radiotherapy (T0).

Poor family income was defined as household income per capita below 1.5 times the local minimum subsistence level.
The urban–rural classification was based on the standards of the National Bureau of Statistics of China, mainly taking into account population density (<1500/km² for rural and ⩾1500/km² for urban) and economic structure (agricultural vs nonagricultural dominance).
BMI, body mass index; CI, confidence interval; GAD-7, 7-item Generalized Anxiety Disorder; NA, not applicable; OR, odds ratio; PHQ-9, 9-item Patient Health Questionnaire; RMB, renminbi. Bold p-value indicates a statistically significant difference less than 0.05.
Prevalence and longitudinal changes in depression and anxiety
At T0, 37.3% of the participants had depression and 26.0% had anxiety. The percentage of patients with depression was 34.0% at T1, 31.5% at T2, 29.5% at T3, and 28.4% at T4. The percentage of patients with anxiety was 19.8% at T1, 18.3% at T2, 19.4% at T3, and 20.3% at T4. Overall, the percentage of participants with depression and/or anxiety was 40.7% at T0, 36.6% at T1, 33.5% at T2, 32.2% at T3, and 35.2% at T4.
As shown in Figure 1(a), the GEE analysis indicated that the mean PHQ-9 and GAD-7 scores were both significantly higher at T0 than they were at any of the follow-up time-points (all p’s ⩽ 0.001). However, as shown in Figure 1(b) and (c), stratification analyses found no significant changes in mean PHQ-9 scores from T0 to T4 (all p’s > 0.01) among patients with premenopausal status, patients whose families resided in rural areas, or patients who did not report menopausal symptoms.

Longitudinal changes in PHQ-9 and GAD-7 scores from pre-RT to 6 months post-RT in all patients (a), and stratification analyses of the longitudinal changes in PHQ-9 scores, (b) and GAD-7 scores (c). Error bars represent SDs.
As shown in Figure 2, changes in each PHQ-9 or GAD-7 item were not identical. Most items, including PHQ-9 Q1, Q2, and Q3 and GAD-7 Q1, Q3, and Q6, significantly decreased over time (all p’s < 0.001). PHQ-9 Q3 (sleep problems) had the highest scores, followed by Q4 (feeling tired) at each time-point. GAD-7 Q1 (feeling nervous) and Q3 (worrying too much) ranked as the top two problems during the treatment period, whereas Q6 (annoyed or irritable) ranked at the top at 1 and 6 months post-RT.
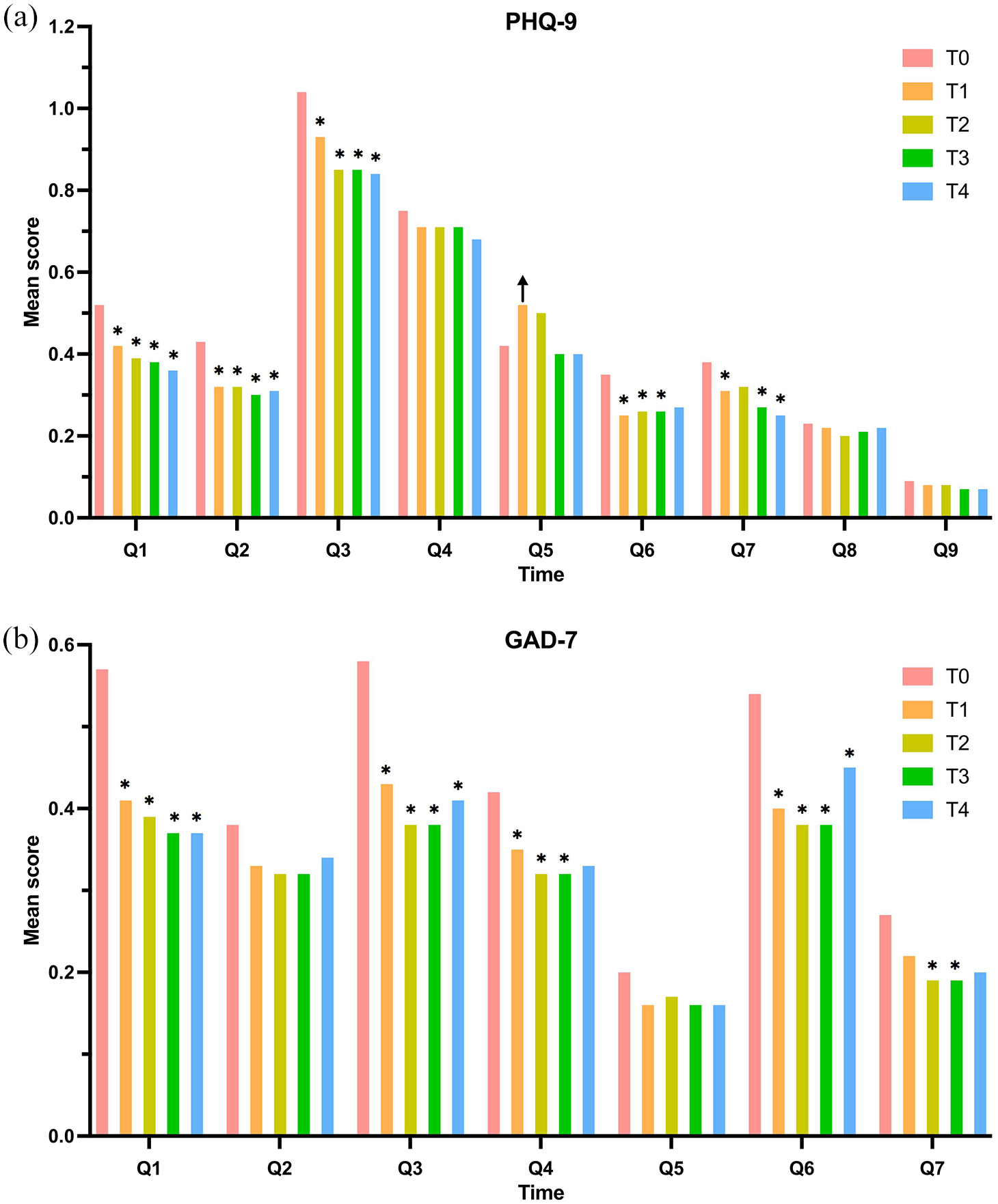
Longitudinal changes of individual item scores on the PHQ-9 (a) and GAD-7 (b) of patients with breast cancer from pre-RT to 6 months post-RT. Error bars represent SDs.
Variables associated with depression and anxiety at pre-RT
Table 1 shows the risk factors for depression and anxiety at T0. Univariate logistic regression indicated that menopausal status, personal income before illness, family income, family place of residence, and menopausal symptoms were associated with both depression and anxiety at T0. In the multivariate analysis, the following variables were independently associated with depression at T0 (ranked by odds ratio (OR) values): menopausal symptoms (OR = 2.29; 95% confidence interval (CI) = 1.52–3.44; p < 0.001), poor family income (compared to the average family income, OR = 2.01; 95% CI = 1.06–3.83; p = 0.033), anti-HER2-targeted therapy (OR = 1.71; 95% CI = 1.10–2.64; p = 0.016), premenopausal status (OR = 1.63; 95% CI = 1.09–2.45; p = 0.017), and having a family history of cancer (OR = 1.59; 95% CI = 1.07–2.38; p = 0.022). The variable that had the strongest independent association with anxiety at T0 was poor family income (compared to the average family income, OR = 2.23; 95% CI = 1.18–4.22; p = 0.014), followed by self-reported menopausal symptoms (OR = 1.73; 95% CI = 1.11–2.69; p = 0.015) and premenopausal status (OR = 1.71; 95% CI = 1.10–2.65; p = 0.017).
Variables associated with a higher depression and anxiety over time
As shown in Table 2, we performed simple effect analyses on the variables with time interactions. A higher level of depression was significantly associated with poor family income (compared to average and above levels) at T0 (OR = 1.86; 95% CI = 1.51–2.29; p < 0.001), T2 (OR = 1.46; 95% CI = 1.12–1.91; p = 0.005), and T4 (OR = 1.52; 95% CI = 1.17–1.96; p = 0.001). A higher level of depression was also significantly associated with menopausal symptoms at T0 (OR = 1.51; 95% CI = 1.27–1.80; p < 0.001) and T1 (OR = 1.44; 95% CI = 1.19–1.74; p < 0.001).
Factors with time × variable interaction associated with a higher depression level over time based on GEE analysis.

CI, confidence interval; GEE, generalized estimating equation; OR, odds ratio; PHQ-9, 9-item Patient Health Questionnaire.
Bold p-value indicates a statistically significant difference less than 0.01.
Tables 3 and 4 indicate the variables without time interactions that were associated with higher levels of depression and/or anxiety over time, which means that the observed decreases in prevalence rates were similar in the subgroups of these variables. Significantly higher depression levels between pre-RT and 6 months post-RT were consistently associated with anti-HER2-targeted therapy (OR = 1.25; 95% CI = 1.07–1.46; p = 0.006), personal income before illness (⩽8000 compared with >8000 RMB/month, OR = 1.26; 95% CI = 1.07–1.48; p = 0.005), and family residing in rural areas (OR = 1.31; 95% CI = 1.09–1.58; p = 0.004). Significantly higher anxiety levels between pre-RT and 6 months post-RT were consistently associated with poor family income (compared to the average family income, OR = 1.67; 95% CI = 1.30–2.13; p < 0.001), family residing in rural areas (OR = 1.46; 95% CI = 1.15–1.85; p = 0.002), and menopausal symptoms (OR = 1.36; 95% CI = 1.11–1.67; p = 0.003).
Factors without time × variable interaction associated with a higher depression level over time based on GEE analysis.

CI, confidence interval; GEE, generalized estimating equation; OR, odds ratio; PHQ-9, 9-item Patient Health Questionnaire.
Bold p-value indicates a statistically significant difference less than 0.01.
Factors without time × variable interaction associated with a higher anxiety level over time based on GEE analysis.
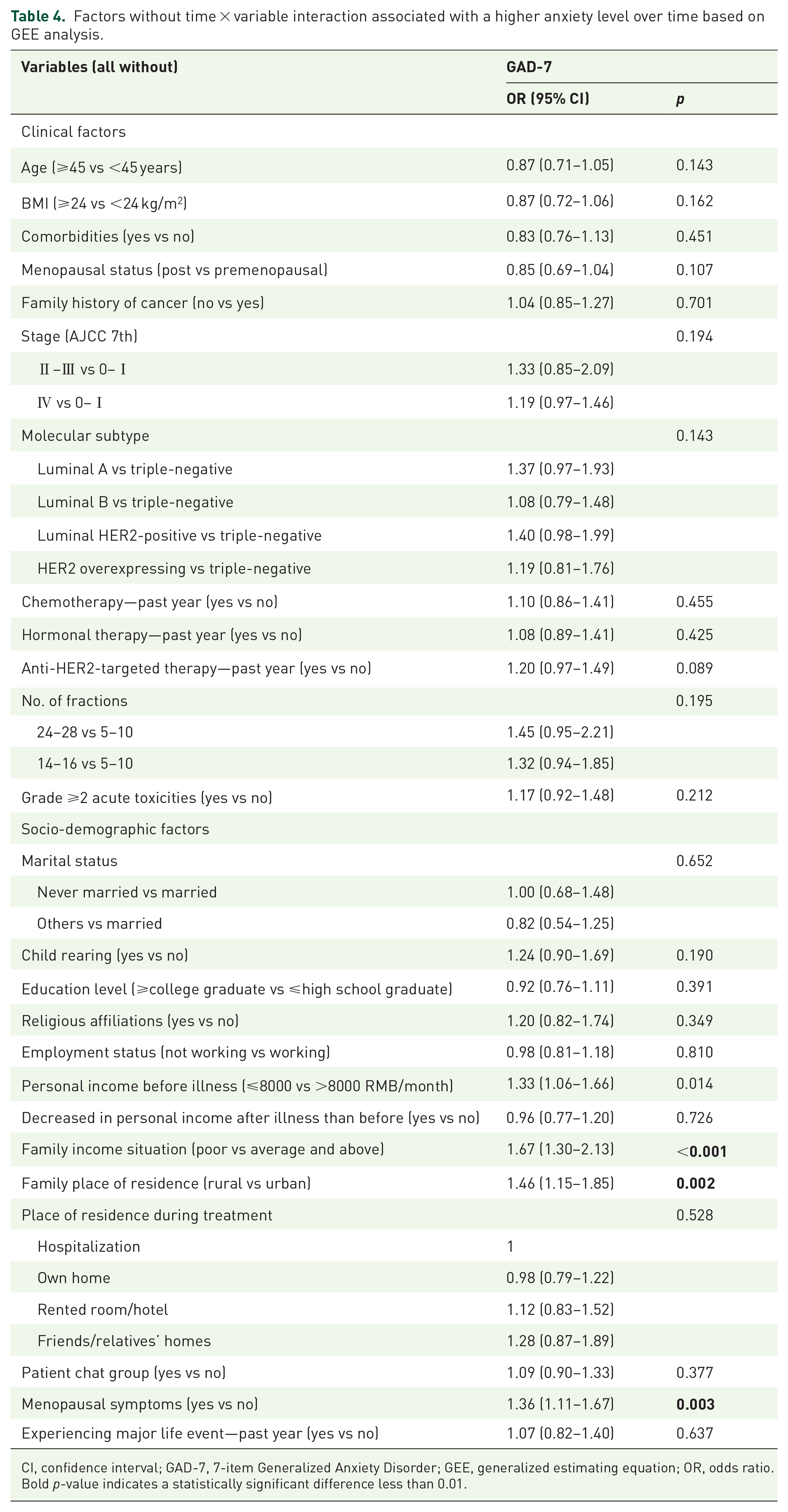
CI, confidence interval; GAD-7, 7-item Generalized Anxiety Disorder; GEE, generalized estimating equation; OR, odds ratio.
Bold p-value indicates a statistically significant difference less than 0.01.
Discussion
We conducted this prospective observational study to enhance understanding of the prevalence and longitudinal changes in depression and anxiety among Chinese patients with breast cancer from pre-RT to 6 months post-RT. We found that: (1) the prevalence of depression decreased gradually from 37.3% before RT to 28.4% at 6 months post-RT; and (2) the prevalence of anxiety decreased from 26.0% before RT to 18.3% after RT, which then increased to 20.3% at 6 months post-RT. We also obtained a comprehensive understanding of the risk factors associated with depression and anxiety in this population before receiving RT. Moreover, we identified variables that were associated with higher levels of depression and anxiety over time, which can contribute to the early identification of and interventions for high-risk patients.
The results of the present study indicate that the prevalence of depression and anxiety among Chinese patients with breast cancer ranged, respectively, from 28.4% to 37.3% and 20.3% to 26.0%, between pre-RT and 6 months post-RT. The prevalence rates we observed are within the range of rates reported in a 2004 review, which showed that 21%–54% of patients with cancer experienced anxiety and 12%–31% experienced depression during the course of RT. 14 Additionally, the prevalence of depression observed in our study is comparable to that reported in a recent meta-analysis of 53,513 Chinese patients with breast cancer, which found a pooled prevalence of 38% (95% CI, 33%–44%). 6 However, the prevalence of anxiety in our study is lower than the 38% (95% CI, 27%–50%) reported in that review. 6 This discrepancy may be explained by patients’ relief following a lengthy treatment process and their adaption to their diagnosis over time, in view of the fact that over 80% of the patients had already received surgery and chemotherapy, which typically was 6 months to a year, prior to participating in our study. Our results highlight the high prevalence of depression and anxiety among Chinese patients with breast cancer who receive RT during both treatment and follow-up periods, which emphasizes the need for active screening for depression and anxiety to facilitate timely interventions. Further research is warranted to assess the clinical benefit and cost-effectiveness of implementing a procedure for routine screening in clinical practice.
Both the depression and anxiety levels of patients with breast cancer in our study were highest before RT, and decreased persistently throughout treatment and up to 6 months post-RT. Table 5 summarizes the studies that have focused on exploring the course of depression and anxiety among patients with breast cancer who received RT. Consistent with our study, most previous studies conducted in different countries with different sample sizes have also found a declining trend in depression and anxiety throughout the course of RT.12,13,28 One possible explanation for this trend after RT may be patients’ relief about completing RT.12,28 Another explanation may be that most patients become accustomed to the treatment over time. A recent study of patients with breast cancer in the United States supports our speculation, in that it found a similar decreasing trend throughout the course of RT in English-speakers, but an increasing trend in Spanish-speakers over time. 29 The authors believed that language-concordant physician care could improve medical understanding. 29 Therefore, we suspect that the provision of effective communication and appropriate information throughout treatment may help reduce levels of depression and anxiety, as proposed by another study. 30 Our findings are also consistent with previous studies that reported a significant decline in the levels of depression and anxiety during the follow-up period after surgery or chemotherapy, compared to the start of RT.7–10 However, few studies have specifically conducted continuous follow-up assessments of depression and anxiety after RT for breast cancer. Two studies that had small sample sizes found no significant changes in depression or anxiety during the follow-up period post-RT, compared to pre-RT.31,32
Summary of published observational studies on the course of depression or anxiety among breast cancer patients receiving RT.

RT, radiotherapy.
Consistent with the overall trends observed in the PHQ-9 and GAD-7, we found that most of the individual items measuring depression and anxiety improved after treatment. On the PHQ-9, item Q3, which measured sleep problems, persistently showed the highest score across all five time-points, followed by Q4 (feeling tired). On the GAD-7, item Q1 (feeling nervous) and Q3 (worrying too much) ranked as the top two items during the treatment period, while Q6 (annoyed or irritable) ranked at the top at 1 and 6 months post-RT. The results of a study that assessed depression and anxiety among patients with breast cancer (from preoperative to 6-month postoperative) are broadly similar to our findings. 9 As far as we know, no study to date has specifically concentrated on changes in the individual items of the PHQ-9 or GAD-7 among patients with breast cancer receiving RT, making direct comparisons between studies difficult.
Anti-HER2-targeted therapy was associated with both baseline depression symptoms and higher depression levels over time in our study. Previous studies with large sample sizes have consistently failed to identify significant associations between treatment-related variables and depression or anxiety,8,20,22 whereas several studies found such associations, particularly those focusing on a certain group of patients with breast cancer.28,32,33 For example, several studies found that adjuvant chemotherapy was associated with depression and anxiety during, but not after, treatment.8,28,32 This may indicate that what matters to patients most is the side effects or the financial burden caused by treatment rather than the treatment itself. 22 This assumption is supported by our different results regarding patients receiving chemotherapy and anti-HER2-targeted therapy, as all patients in our study had completed chemotherapy and were receiving anti-HER2-targeted therapy at the time of enrollment. Additionally, several studies reported that receiving hormonal therapy was a risk factor for depression and anxiety, suggesting that this association may be attributed to menopausal symptoms resulting from the hormonal therapy.28,34 Note that none of these studies collected information on menopausal symptoms.20,28,34 In our study, self-reported menopausal symptoms were independently associated with baseline anxiety and higher anxiety levels over time, suggesting that self-reported menopausal symptoms may be a more direct and better predictor of depression and anxiety. Furthermore, we found that poor financial status (low household or personal income) was also an important risk factor for not only depression and anxiety levels before RT but also for higher depression and anxiety levels over time. Our results are consistent with previous research conducted in both developing and developed countries, which reported that patients with breast cancer who have less financial support are more vulnerable to depression or anxiety.17,18,20,22 This is logical because patients who have a low income face not only the symptoms of the illness itself and the side effects of treatment but also psychological pressure resulting from severe economic burden. Furthermore, previous cross-sectional studies reported that patients with breast cancer living in rural areas were about 2–4 times more likely to experience depression and anxiety than those in urban areas, due to the fact that rural populations have poor access to healthcare. 19 This finding is supported by our longitudinal analysis. Compared with urban areas, rural areas have a lower population density (rural vs urban, <1500/km2 vs ⩾1500/km2) and their economic structure is dominated by agriculture. This corresponds to fewer pharmacies and medical facilities, making it difficult for the rural population to access healthcare. Moreover, this situation may be exacerbated by unreliable transportation and poor road infrastructure in rural areas.
To our knowledge, this is the largest prospective study, and the first study conducted in China, to assess depression and anxiety longitudinally among patients with breast cancer receiving RT. Our study fills an important gap in the existing literature regarding the longitudinal changes in depression and anxiety among patients with breast cancer between pre-RT and 6 months post-RT, which may facilitate the implementation of individualized and optimal approaches in clinical practice. Moreover, based on clinical practice and a literature review, we collected baseline clinical and sociodemographic variables as comprehensively as possible, and we had an adequate sample size to control for and assess multiple covariates.
Our research provides insight into identifying certain groups who may experience depression and anxiety before RT and higher levels of these conditions over time. Such understanding may help guide clinicians to implement targeted interventions for at-risk patients at an early stage. However, interpretation of our study’s findings may be limited by its observational design; in particular, the identified associations should not be interpreted as causal. Moreover, our findings are limited by their single-center design, and multicenter studies are necessary to confirm the generalizability of our results. However, the patients included in this study came from all over the country, which may help minimize this bias. In the future, we will conduct a multicenter study to verify our findings.
Conclusion
The prevalence of depression and anxiety was high in patients with breast cancer receiving RT, and it decreased over time from pre-RT to 6 months post-RT, which highlights the need for routine assessments during both the treatment and follow-up periods. Within this patient population, particular attention should be given to those with a family history of cancer, receiving anti-HER2-targeted therapy, premenopausal status, self-reported menopausal symptoms, poor financial status, or living in rural areas.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251345930 – Supplemental material for Depression and anxiety in patients with breast cancer receiving radiotherapy: a longitudinal study
Supplemental material, sj-docx-1-tam-10.1177_17588359251345930 for Depression and anxiety in patients with breast cancer receiving radiotherapy: a longitudinal study by Shi-Jia Wang, Xin Feng, Wei Zhang, Guang-Yi Sun, Hui Fang, Hao Jing, Yu Tang, Tao Li, Shu-Nan Qi, Yong-Wen Song, Wen-Wen Zhang, Ning-Ning Lu, Yuan Tang, Yue-Ping Liu, Bo Chen, Xin Liu, Ye-Xiong Li, Yi-Rui Zhai and Shu-Lian Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-2-tam-10.1177_17588359251345930 – Supplemental material for Depression and anxiety in patients with breast cancer receiving radiotherapy: a longitudinal study
Supplemental material, sj-pdf-2-tam-10.1177_17588359251345930 for Depression and anxiety in patients with breast cancer receiving radiotherapy: a longitudinal study by Shi-Jia Wang, Xin Feng, Wei Zhang, Guang-Yi Sun, Hui Fang, Hao Jing, Yu Tang, Tao Li, Shu-Nan Qi, Yong-Wen Song, Wen-Wen Zhang, Ning-Ning Lu, Yuan Tang, Yue-Ping Liu, Bo Chen, Xin Liu, Ye-Xiong Li, Yi-Rui Zhai and Shu-Lian Wang in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
None.
Declarations
Supplemental material
Supplemental material for this article is available online.
Role of the funder/sponsor
The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.