
Abstract
Background:
Fertility preservation (FP) is a key aspect of care for young women with breast cancer (BC), as oncologic treatments can compromise future reproductive potential. Early counseling and access to FP strategies are essential to support long-term quality of life.
Objectives:
To evaluate the uptake of FP counseling, the choice of preservation techniques, and reproductive outcomes in women aged 18–39 years with BC.
Design:
A retrospective single-center cohort study was conducted at the Gemme Dormienti network between 2018 and 2023.
Methods:
A total of 100 BC patients underwent baseline ovarian reserve assessments, including hormonal and ultrasound evaluations. All received gonadotropin-releasing hormone agonist therapy prior to chemotherapy. Data on FP strategies—oocyte and/or ovarian tissue cryopreservation (OTC)—and pregnancy outcomes were collected.
Results:
Fifty-four percent of patients pursued FP procedures: 35% underwent oocyte cryopreservation, 55% OTC, and 10% both. Younger patients (18–29 years) were more likely to opt for combined techniques. Pregnancy rates were highest among women aged 35–39. Ovarian reserve indicators, including antral follicle count and endometrial thickness, showed an age-related decline.
Conclusion:
This study highlights the importance of early, personalized FP counseling for young BC patients. Age significantly influences both FP choices and reproductive outcomes, reinforcing the need to integrate fertility discussions into initial cancer care.
Plain language summary
This study examines fertility preservation (FP) practices among young women diagnosed with breast cancer (BC), with a particular focus on how age impacts decision-making and outcomes. As women age, their fertility declines due to a reduction in both the quantity and quality of oocytes. For women diagnosed with BC before menopause, preserving fertility before undergoing treatments like chemotherapy, which can damage ovarian function, becomes a critical concern. Common fertility preservation options include oocyte cryopreservation, ovarian tissue cryopreservation (OTC), and gonadotropin-releasing hormone (GnRHa) therapy. The study analyzed the medical records of 100 women aged 18-39 with BC, referred to Gemme Dormienti, a fertility counseling center in Rome, between 2018 and 2023. The findings revealed that FP practices varied significantly with age. Younger women (18-29 years) were more likely to combine GnRHa therapy with oocyte or ovarian tissue preservation, while older women (35-39 years) were less inclined to pursue these methods. Additionally, ovarian function, as assessed by hormone levels and follicle counts, showed a decline with age. Despite these age-related differences, 54% of participants opted for FP, with eight pregnancies reported afterward, particularly among the older age group. This highlights the crucial role of early, comprehensive fertility counseling for BC patients. Providing personalized guidance can empower women to make informed decisions about their fertility preservation options and help safeguard their chances of becoming mothers following cancer treatment.
Keywords
Introduction
Female fertility is mainly influenced by age-related changes in oocyte quality and quantity. 1 Age is the key factor in determining a woman’s fertility potential and the success of assisted reproductive techniques. As women age, fertility declines due to higher levels of follicle-stimulating hormone (FSH), lower levels of anti-Müllerian hormone (AMH), and increased oxidative stress and DNA damage that affect oocytes. AMH, which indicates follicular activity during the menstrual cycle, is currently the most reliable biomarker for assessing ovarian reserve. 2
In recent decades, ovarian aging has gained increasing attention as more couples choose to delay parenthood. 3 Many women are diagnosed with cancer before reaching natural menopause, with breast cancer (BC), melanoma, cervical cancer, Hodgkin’s and non-Hodgkin’s lymphoma, and leukemia being the most frequently diagnosed cancers in women under 40. 4 Approximately 7%–10% of BC cases occur in women younger than 40 at the time of diagnosis. 5 Advances in cancer treatments have led to improved survival rates; however, managing treatment-related adverse effects and addressing survivorship concerns, including fertility preservation (FP), remain significant challenges. 6 For many young patients with BC, FP, family planning, and sexual health are key areas of concern. 7 Consequently, it is strongly recommended that healthcare providers discuss FP options with patients and refer them to reproductive specialists when necessary.8,9
Reproductive-age patients with cancer should receive thorough oncofertility counseling before starting treatment to understand how it may affect fertility and to explore preservation options that could enhance their quality of life.10,11
Oocytes and embryos can be safely and effectively cryopreserved prior to the start of anticancer treatments. For cryopreservation of oocytes and embryos, 2 weeks of ovarian stimulation with gonadotropins are necessary, followed by follicle aspiration. It is the preferred FP method for women diagnosed with BC at age 40 or younger, as it provides the best chance of maintaining fertility. 12 The success of this technique depends mostly on a patient’s ovarian reserve and age.13,14
An alternative FP strategy is ovarian tissue cryopreservation (OTC), which involves the removal, freezing, storage, and reimplantation of ovarian tissue containing immature eggs. This method allows for the preservation of both fertility and ovarian function before chemotherapy or radiation treatments that may affect fertility. After reimplantation, the ovarian tissue can potentially resume its function.15,16
Gonadotropin-releasing hormone agonist (GnRHa) therapy during chemotherapy is recommended for premenopausal women aged 40 or younger to help preserve ovarian function; however, it should not be considered a stand-alone FP strategy.17,18
Despite increasing awareness of FP, barriers such as misinformation, misconceptions, and delayed or inadequate referrals to fertility specialists persist. 19
This study aims to explore the real-world experience of FP practices at the Gemme Dormienti network, a specialized FP counseling center in Rome, Italy, dedicated to providing medical care for young women undergoing gonadotoxic treatments. The study specifically focuses on FP adherence among patients with BC and investigates age-related differences in FP decisions and outcomes.
Methods
This retrospective single-center study included patients with BC referred to the Gemme Dormienti network from January 2018 to January 2023. Eligible patients were those aged 18–39 years, diagnosed with BC, with no evident signs of ovarian metastasis, no previous chemotherapy, and no contraindications to FP techniques. Exclusion criteria included patients outside the age range of 18–39 years, those who had received previous treatments for a cancer diagnosis before FP counseling, or those with medical or ethical contraindications to FP methods.
The study was approved by the Ethics Committee of IDI IRCCS (Protocol No. 45/CE/2017), and all patients provided written informed consent. Patient privacy was maintained by anonymizing all data.
The study was conducted in accordance with the Declaration of Helsinki. We collected patients’ data, including age at diagnosis, tumor histology, germline BRCA status, comorbidities, and previous reproductive history.
Laboratory tests (AMH, FSH, 17β-estradiol (17βe)) were analyzed at baseline in the San Carlo di Nancy Hospital laboratory in Rome. AMH was evaluated using an enzyme-linked fluorescent assay, FSH, and 17βe using chemiluminescence immunoassay.
Pelvic or transvaginal ultrasound for right and left antral follicular counts (AFCr and AFCl) and endometrial thickness was performed by the same operator.
We collected data on the type of FP techniques used—including GnRHa, oocyte cryopreservation, OTC, and their combinations—as well as the efficacy of these methods and the occurrence of post-treatment pregnancies. The results were subsequently stratified by age into two main categories: pre-advanced maternal age (pre-AMA, <35 years) and AMA (>35 years). The pre-AMA group was further divided into Group 1 (ages 18–29 years) and Group 2 (ages 30–34 years), while the AMA group consisted of Group 3 (ages 35–39 years). This classification aligns with the natural fertility curve, which peaks between ages 20 and 30, gradually declines after 30, and accelerates more significantly beyond 35. 20
The three phases of the menstrual cycle (follicular from days 6 to 12, ovulatory from days 13 to 16, and luteal day 17 to premenstrual) were all represented in our sample; all patients were recruited at any phase of the menstrual cycle due to the short time available and the need to start cancer treatments immediately.
All continuous variables were evaluated by the Shapiro–Wilk test and expressed as median and standard deviation (SD). Categorical variables were expressed in numbers and percentages. Differences between groups were assessed using parametric and nonparametric tests (Chi-square test in case of categorical variables, t test and Mann–Whitney test, Wilcoxon signed-rank test, and Kruskal–Wallis test in case of continuous variables). For each statistical test, a p-value was calculated to assess the significance of the differences between groups; p-value <0.05, the result was considered statistically significant.
Confidence intervals were estimated at a 95% level, and all tests were two-sided, accepting p < 0.05 as indicating a statistically significant difference. The reporting of this study conforms to the STROBE statement. 21
Results
Patients population
The study population consisted of 100 participants, with an average age of 34.6 years, with a median follow-up of 30 months. The group was divided into three age ranges: 18–29, 30–34, and 35–39 years. In terms of education, the majority (60%) held a degree, while 28% had completed high school, and 12% had finished secondary school.
When looking at health conditions, 32% of participants had comorbidities, with a slightly higher prevalence in the older age group. A quarter of the women had experienced pregnancy before starting therapy, with this being more common among those aged 35–39.
The cohort consisted of 69 patients (69%) with hormone receptor-positive, HER2-negative BC, 15 patients (15%) with HER2-positive disease, and 16 patients (16%) with triple-negative BC. Regarding disease stage, 10 patients (10%) were diagnosed at stage I, 52 patients (52%) at stage II, and 38 patients (38%) at stage III. A total of 88 patients (88%) received chemotherapy, of which 76 patients (86%) were treated with a sequential regimen that included anthracyclines, cyclophosphamide, and taxanes. In addition, five patients (6%) received taxane monotherapy, four patients (5%) were treated with both taxanes and carboplatin, and three patients (3%) received an anthracycline-only regimen (fluorouracil, epirubicin and cyclophosphamide). Among the chemotherapy group, 15 patients (13%) also received trastuzumab, while 12 patients (12%) underwent adjuvant endocrine therapy without prior chemotherapy, based on tumor biology.
Surgical treatment was also widespread, with 80% of patients undergoing quadrantectomy and 20% opting for mastectomy.
Radiotherapy was administered to just over half of the participants (51%).
Regarding genetic predisposition, BRCA testing showed that 12% of patients carried a BRCA1 mutation, while 2% were BRCA2-positive. However, the vast majority (86%) had not been tested or had unknown BRCA status. These data provide a comprehensive overview of the study population, offering valuable insights into the factors that may influence treatment choices and patient outcomes (Table 1).
Demographic and clinical characteristics.

Baseline ovarian function
AMH levels showed a decreasing trend with age, with median overall values of 6.0 ng/mL in the 18–29 age group, 2.9 ng/mL in the 30–34 group, and 4.0 ng/mL in the 35–39 group (p = 0.099).
FSH levels, indicative of ovarian function, were higher in older age groups, with median overall values of 3.6, 5.6, and 5.9 mU/mL for the three respective age groups (p = 0.323).
17βe levels also exhibited variation, with the highest values observed during ovulation across all groups.
Baseline levels of AMH, FSH, and 17βe across different age groups and menstrual cycle phases are displayed in Figure 1 and Table 2.

Boxplot showing variations in AMH, FSH, and 17βe across different age groups.
Baseline laboratory test: AMH, FSH, and 17βe levels at baseline (overall and according to the menstrual cycle phase).

AMH, anti-Müllerian hormone; FSH, follicle-stimulating hormone; 17βe, 17β-estradiol.
The baseline instrumental test results reveal significant differences in ovarian reserve and endometrial thickness across age groups. The AFCr was highest in the youngest group (18–29 years) with a median ± SD of 7.0 ± 5.3 (range: 3.0–23.0), decreasing to 4.0 ± 2.5 (1.0–10.0) in the 30–34 age group, and further declining to 3.0 ± 4.2 (1.0–18.0) in those aged 35–39 (p = 0.012).
A similar trend was observed for the AFCl, which showed a statistically significant decline from 7.0 ± 3.1 (5.0–15.0) in the youngest group to 4.0 ± 3.1 (1.0–13.0) in the 30–34 age group and 3.5 ± 2.5 (1.0–11.0) in the oldest group (p < 0.001).
Endometrial thickness also decreased with age, measuring 11.0 ± 2.9 mm (3.0–12.0) in the 18–29 group, 9.0 ± 3.1 mm (3.0–13.6) in the 30–34 group, and 6.5 ± 3.0 mm (0.0–14.0) in the 35–39 group (p = 0.022).
Baseline levels of AFCr, AFCl, and endometrial thickness across different age groups and menstrual cycle phases are displayed in Figure 2 and Table 3.

Boxplot showing variations in AFCr, AFCl, and ET across different age groups.
Baseline instrumental test: AFCr, AFCl, and ET.

p-Value: Kruskal Wallis test—p < 0.05 significant.
AFCl, left antral follicular counts; AFCr, right antral follicular count; ET, endometrial thickness; SD, standard deviation.
FP techniques
All individuals (100%) received GnRHa treatment, regardless of age. However, additional FP strategies varied. The combination of GnRHa with oocyte preservation was most common in the youngest group (18–29 years), with 40% opting for this approach, compared to 38.5% in the 30–35 age group and only 21.7% among those aged 36–39. Similarly, GnRHa combined with ovarian tissue preservation was significantly more frequent in younger individuals, with 46.7% undergoing the procedure compared to just 13% in older groups (p = 0.008). The preservation of both oocytes and ovarian tissue was rare, occurring in 26.7% of the youngest participants and nearly absent in older age groups.
Post-therapy pregnancy outcomes showed that eight participants became pregnant, with the highest rate (15.2%) observed in the 36–39 age group. Among those who conceived, 43% did so spontaneously, while 57% required medically assisted reproduction.
These findings highlight differences in FP choices across age groups and provide valuable insights into post-treatment reproductive outcomes, which may help guide counseling and decision-making for patients undergoing cancer therapy (Table 4).
Fertility preservation techniques.
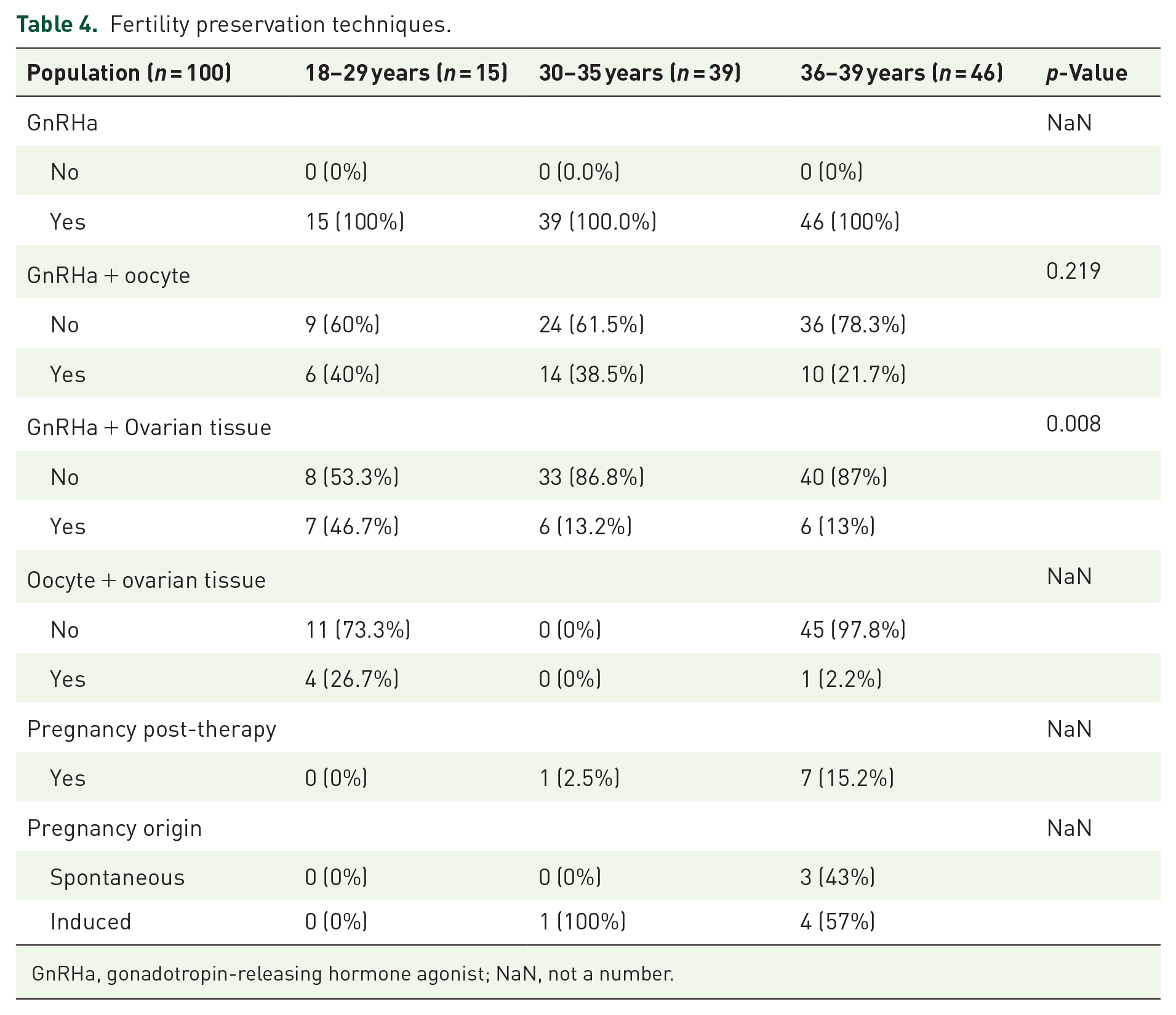
GnRHa, gonadotropin-releasing hormone agonist; NaN, not a number.
Discussion
FP plays a crucial role in the care of young patients with BC, ensuring informed decision-making, access to specialized FP networks, the right to motherhood, and a high quality of life both during and after cancer treatment. Patients must be promptly guided through the complex FP process before initiating gonadotoxic therapies.22,23
This retrospective study examines the use of FP techniques in patients with BC and explores how age influences decision-making and the success of these procedures, highlighting the need for personalized FP management. While antral follicular count (AFC) and endometrial thickness showed significant age-related changes in our study population, basal ovarian function laboratory tests, including AMH, FSH, and 17βe, exhibited notable but nonlinear variations, with no statistically significant differences.
Over time, the predictive role of hormonal markers in FP has been reassessed. Although basal FSH and AMH levels are widely used to estimate reproductive potential, their predictive value differs by age.
FSH is more informative for younger women (<35 years), while AMH is a better predictor in older patients (>35 years). However, both AMH and FSH are involved in regulating oocyte competence and contribute to age-related declines in oocyte quality. 24
Studies have shown that higher AMH levels are associated with a greater number of retrieved oocytes, better oocyte quality, and improved embryo transfer and fertilization rates.25,26 More recently, the predictive role of AMH has been reconsidered. While serum AMH levels correlate with cumulative live birth rates after in vitro fertilization (IVF), no definitive threshold exists, meaning low AMH levels alone should not exclude patients from IVF, particularly young women. 27 Although young women with low AMH may still choose FP, public awareness campaigns are necessary to educate individuals about age-related fertility decline. 28
While some studies have indicated a linear-age-related decline in AFC, and others have proposed a biphasic pattern of decline, our study found a steady, linear decrease across all age groups. 29
In this study, eight pregnancies were reported, the majority of which occurred in the oldest group, reflecting a relatively low pregnancy rate in patients with BC. 30 Recent evidence supports the safety of pregnancy following BC treatment. 31 Women with a history of BC, including those with hormone receptor-positive disease or BRCA mutations, should not be discouraged from pursuing pregnancy, reinforcing the importance of FP access.32,33 Prior research indicates that only about one in three patients with BC seek fertility counseling, and fewer than one in five proceed with cryopreservation. 34 Our findings emphasize the need for FP counseling in patients with BC, as all participants in our study received GnRHa treatment during chemotherapy, and 54 opted for cryopreservation.
However, the women who accepted fertility counseling likely had a strong personal motivation for motherhood. Despite this, some declined OTC and oocyte cryopreservation.
Several factors influence a woman’s decision to pursue FP after counseling. Concerns about delaying cancer treatment and the potential impact of FP procedures on cancer prognosis may discourage some patients from pursuing these options. 35 Nevertheless, our analysis indicates that younger patients are generally more inclined to consider FP. 36
Therefore, improving FP counseling is essential to clarify the factors that shape fertility-related decisions in cancer patients. Decision aids, such as educational materials, can support patients in making informed choices, reducing decisional conflict without increasing anxiety. 37
Personalized FP in clinical practice should focus on customizing strategies according to each patient’s risk factors, medical conditions, and reproductive goals. Advances in ovarian reserve testing, new insights into the impact of medications on fertility, and genetic screening allow for optimized treatments that enhance outcomes and FP-related risks. In addition, ethical and psychosocial factors, including emotional support, must be incorporated into FP planning to ensure a comprehensive, patient-centered approach to care. 38
Currently, few networks specialize in delivering comprehensive FP services. As demand for these treatments continues to rise, it is increasingly recognized that patients require expert supervision within structured care pathways. The Gemme Dormienti Association plays a crucial role in this context, providing medical assistance for FP, raising public and professional awareness in Italy, and promoting a healthcare culture that supports young women navigating FP decisions. 22
Early counseling on FP is crucial in helping patients make informed and proactive decisions regarding their reproductive options. Future research should focus on refining counseling methodologies and exploring the long-term outcomes and effectiveness of these strategies.
Several limitations should be considered when interpreting the findings of this study. The retrospective design of the study may introduce selection bias, as the study population consists of patients who actively sought fertility counseling and opted for FP, potentially overestimating the adherence rate to FP strategies. In addition, data were collected from a single specialized center, which may limit the generalizability of the results to broader populations, particularly those in different healthcare systems or with varying levels of access to FP services. The study follow-up was relatively short, preventing a comprehensive assessment of long-term reproductive outcomes, including live birth rates and the effectiveness of different FP techniques over time. Future research with extended follow-up would be necessary to evaluate the long-term success of oocyte and OTC and the impact of FP decisions on patients’ reproductive choices after cancer treatment.
Nonetheless, this study provides valuable insights into an FP network for patients with BC, offering centralized FP counseling and ovarian function evaluation through standardized laboratory and instrumental testing.
Conclusion
Our study showed an important need for FP techniques in patients with BC, with more than half accepting to undergo a cryopreservation technique. The basal ovarian function was not significantly affected by age, while there were noticeable differences in instrumental value according to patient age. Younger patients showed a high adherence to the FP program, although, due to the short follow-up, pregnancies were more frequent in the older group. Our study provides evidence on the importance of the FP counseling network in patients with BC and creates a social culture to guarantee a good quality of life to cancer survivors.