
Abstract
Background:
Immune checkpoint inhibitors (ICIs) + chemotherapy became standard her2-GC first line treatment.
Objectives:
The aim of this study is to investigate whether ICIs + chemo provides benefit for patients with low programmed death-ligand 1 (PD-L1) expression.
Design:
This study is a systematic review and meta-analysis.
Data sources:
We searched PubMed, Embase, Web of Science, and Cochrane Library as well as the 2019 to 2024 Annual Meetings of the European Society for Medical Oncology, the American Association for Cancer Research, the American Society of Clinical Oncology (ASCO), and the ASCO Symposium on Gastrointestinal Oncology (ASCO-GI) and the ClinicalTrials.gov database.
Methods:
This systematic review included phase III randomized controlled trials comparing first-line immunotherapy combined with chemotherapy versus chemotherapy alone in advanced gastric cancer. KMSubtraction was used to estimate survival data for those trials that did not report data for the PD-L1 low-expression population.
Results:
We included a total of nine randomized clinical trials. In patients with combined positive score (CPS) < 1 and CPS < 5, monoclonal antibody + chemotherapy did not show an improvement in overall survival (OS) or progression-free survival (PFS) (CPS < 1 OS: hazard ratio (HR) = 0.91, 95% CI: 0.77–1.08; PFS: HR = 0.88, 95% CI: 0.73–1.07. CPS < 5 OS: HR = 0.92, 95% CI: 0.79–1.08; PFS: HR = 0.78, 95% CI: 0.53–1.14). However, in trials using dual antibodies, patients with PD-L1 CPS < 5 achieved improvements in PFS (HR = 0.64, 95% CI: 0.52–0.80). In trials using tumor area positivity (TAP) scoring, the subgroup with TAP < 5% did not achieve benefits in OS or PFS from immunotherapy plus chemotherapy (OS: HR = 0.92, 95% CI: 0.75–1.13; PFS: HR = 0.91, 95% CI: 0.74–1.13).
Conclusion:
Our study results indicate that in the first-line treatment of advanced gastric cancer, monoclonal antibody combined with chemotherapy does not provide a survival benefit compared to chemotherapy alone for patients with low PD-L1 expression. However, it is noteworthy that in the COMPASSION-15 trial, patients with CPS < 5 achieve significant improvements in OS and PFS, which may be related to the bispecific antibodies and needs to be validated by further studies.
Trial registration:
This study was registered in PROSPERO (CRD42024568972).
Keywords
Introduction
Gastric cancer (GC) is the fourth leading cause of global cancer-related deaths1,2 and ranks third in both incidence and mortality rates among all cancers in China. Each year, approximately 480,000 new cases are diagnosed nationwide. However, over 60% of patients are already at advanced stages when first detected, significantly limiting effective drug treatment options. 3 The median overall survival for these patients remains poor, averaging just 1 year. 4
Traditional first-line therapies for advanced GC rely heavily on chemotherapy drugs such as oxaliplatin and cisplatin. 5 While these regimens can temporarily control disease progression, they offer limited survival benefits and often compromise patients’ quality of life. To address this unmet need, the field is transitioning toward personalized treatment strategies. These approaches aim to tailor therapies based on molecular profiling, potentially improving survival outcomes while minimizing adverse effects. 6
In recent years, immune checkpoint inhibitors (ICIs) have revolutionized the treatment paradigm of cancer and have begun to be used earlier and earlier in a number of patients with specific characteristics of advanced gastric and gastroesophageal junction cancer. 7 Presently, evaluating PD-L1 expression levels remains a key predictive biomarker for gauging a patient’s response to immunotherapy, which is commonly measured by combined positive score (CPS), tumor area positivity score (TAP), and tumor proportion score (TPS). 8 Based on the results of CheckMate-649 and KEYNOTE 590, the US Food and Drug Administration has approved nivolumab for the first-line treatment of all advanced gastroesophageal adenocarcinoma and pembrolizumab for the first-line treatment of esophageal and gastroesophageal junction carcinoma.
However, not all experiments yielded consistent results. In ORIENT-16, 9 sintilimab in combination with chemotherapy showed an improved anti-tumor response in the overall population and in patients with CPS ⩾ 5. Global and Chinese subgroup 3-year follow-up data from the CheckMate-64910,11 study showed that nivolumab plus chemotherapy continued to demonstrate clinically meaningful improvements in OS and progression-free survival (PFS) compared to chemotherapy in patients with PD-L1 CPS ⩾ 5 and in all randomized subgroups. However, according to the final analysis of KEYNOTE-062 trial, 12 pembrolizumab plus chemotherapy was not superior to chemotherapy for the OS in the CPS ⩾ 1 and ⩾10 cohorts.
In numerous clinical trials, patients with high PD-L1 expression inclined to benefit more from immunotherapy combined with chemotherapy. For instance, in the KEYNOTE-859 trial, 13 pembrolizumab achieved better clinical benefit in patients with CPS ⩾10 than in the CPS < 10 and CPS < 1 groups. In addition, the mean treatment effect observed in patients with CPS ⩾ 1 was also largely attributable to patients with CPS ⩾ 10. However, the low PD-L1 subgroup has been underexplored in previous studies, resulting in a lack of survival outcome data for this population. Hence, whether patients with low PD-L1 expression can benefit remains controversial. 14 In real-world settings, patients with PD-L1 CPS < 5 represent approximately half of the total GC population. Therefore, it is highly pertinent to investigate whether this subgroup could benefit from immune-combination chemotherapy. Although some results of low-expressing population have been reported in previous meta-analyses, the included trials were not comprehensive enough. 15
In this study, we reconstructed data for patients with low PD-L1 expression and included the most recent trials for pooled analyses to determine whether the PD-L1 low-expression subgroups could benefit from ICIs + chemotherapy. Ultimately, it is hoped that this will help such patients to further optimize their treatment and reduce unnecessary financial losses and toxic side effects.
Methods
Study selection
A systematic search was conducted in September 2024 in the databases of PubMed, Embase, Web of Science, and Cochrane Library based on the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines. 16 The studies were independently searched and screened by two reviewers, with a third reviewer involved in resolving any disagreements. The full search strategy is shown in Table S1. And a systematic review of conference abstracts presented at the 2019–2024 Annual Meetings of the European Society for Medical Oncology (ESMO), the American Association for Cancer Research (AACR), the American Society of Clinical Oncology (ASCO), and the ASCO Symposium on Gastrointestinal Oncology (ASCO-GI) was performed to identify relevant unpublished data. High-quality meta-analyses that had been published in the last 5 years were also reviewed to prevent omissions. In addition, we conducted a systematic review of the ClinicalTrials.gov database.
“Gastric cancer,” “Gastroesophageal junction adenocarcinoma,” “Chemotherapy,” “Immunotherapy,” “PD-1,” “PD-L1,” “CPS,” ICIs like nivolumab, pembrolizumab, and sugemalimab, and other chemotherapeutic agents are included in our search framework with Medical Subject Headings (MeSH) terms and free terms. Studies that met the following inclusion criteria were included: (1) randomized controlled trials of first-line treatment for adult patients with advanced gastric/gastroesophageal junction (GEJ) adenocarcinoma; (2) treatment with PD-1/PD-L1 inhibitors in combination with chemotherapy versus placebo plus chemotherapy; (3) primary outcome metrics including OS and PFS; (4) studies providing results stratified by PD-L1 CPS, TPS or TAP score; and (5) studies in English. In contrast, retrospective studies or studies that were non-randomized, non-first-line treatments, and studies that focused on outcome-effects analyses and healthy quality of life were excluded. The study protocol was prospectively registered with PROSPERO (CRD42024568972), and the review adhered to PRISMA 2020 Checklist guidelines 17 (Table S2).
Data extraction
Data for this study were derived from published articles, Supplemental Material, and conference abstracts, as well as data reconstructed using the KMSubtraction method for the PD-L1 low-expression population. The data were independently extracted by two authors and cross-verified. In case of any discrepancies, the original documents were reviewed, and the opinion of a third author was sought to reach a final decision. Basic information about each study was extracted including: study name, year of publication, patient ethnicity, histological type, intervention, sample size, PD-L1 assay method, and whether the original article provided data on low-expression subgroups. In addition, hazard ratios (HRs) and 95% confidence intervals (CIs) for PFS and overall survival (OS) of patients with different expression levels of PD-L1 were derived.
Risk of bias assessment and extraction of reported Kaplan Meier (KM) curves
Included trials were assessed for risk of bias using the Revised Cochrane risk-of-bias tool for randomized trials (RoB 2). 18 The KM curves of the total population and the PD-L1 high-expression subgroups were extracted from the included articles, and additionally, the KM curves of the subgroups with PD-L1 low expression were collected if they were provided.
Reconstruction of time-to-event outcomes
When performing secondary analyses of published survival data, the most important thing was to obtain the raw data for each patient. The challenge of researchers not having access to raw data was solved by a two-stage improved iKM method proposed by Guyot et al. 19 and Liu et al. 20 The process involves extracting data points (time, survival probability) from KM curves and reconstructing IPDs using the iterative algorithm.
Matching of patients and derivation of unreported subgroups—KMSubtraction
For trials that did not provide KM curves of the PD-L1 low-expression population, their survival data were reconstructed using KMSubtraction, 21 an algorithm that includes three main functions, KMSubtractionMatch, KMSubtractionEvaluateMatch, and KMSubtractionError. Unmatched low-expression subgroups were retrieved by matching the overall cohort with patients from the high-expression subgroup. Therefore, it is possible to maximize the availability of survival data for the PD-L1 low-expression subgroup of patients. The minimum cost bipartite matching with the Hungarian algorithm was adopted as the main matching algorithm, and Monte Carlo simulations were used to evaluate the error limits of the original and reconstructed data.
Quality assessment of reconstructed data
Before performing the combined analyses, the quality of the reconstructed data was evaluated. The quality of the matches was assessed by Bland–Altman plots, empirical cumulative distribution plots, and KM plots. We further compared the reconstructed KM curves with the KM curves provided in the original article through curve shapes, marginal HRs, and risk tables.
Statistical analysis
When the match quality is good with small HR errors, subsequent secondary analyses can be performed. HRs and 95% CIs for OS and PFS were pooled, and then ln(HR) and SE(lnHR) were calculated. A fixed-effects model (Inverse variance method, I–V method) was used if heterogeneity was low (I2 < 50% and p > 0.1 for the Q-test), and conversely, a random-effects model (DerSimonian-Laird method, D-L method) was used if heterogeneity was high. The degree of heterogeneity between studies was explored using the I2 test, and p < 0.05 was considered statistically different. Additionally, to assess the heterogeneity and robustness of the studies, publication bias and sensitivity analyses were conducted. Publication bias was evaluated by constructing a funnel plot to examine its symmetry and further verified using Begg’s test and Egger’s test. Sensitivity analysis was performed by sequentially excluding individual studies and re-conducting the meta-analysis to determine whether the overall effect size changed significantly. Furthermore, all included studies assessed the proportional hazards assumption. For studies that did not meet the proportional hazards assumption, stratified analysis was applied for adjustment. All analyses were performed in R version 4.3.3 (R Foundation, Vienna, Austria) and Stata (Version 14, STATA Gorp, College Station, TX, USA). R packages, including tidyverse, ggplot2, survival, and survminer, were used.
Results
Research results
The process of literature selection is shown in the flowchart (Figure 1). A total of 1565 relevant articles were retrieved by searching databases, ESMO, AACR, and ASCO. After removing duplicates and performing a rough screening, 45 articles were selected for full text screening. Among them, 36 records were excluded due to retrospective studies, single-arm trial designs, and duplicate reporting of data. Finally, 7825 patients from 9 articles were included in our meta-analysis. All studies were phase III RCTs and the risk of bias was shown in Figure 2.

Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flowchart.

Quality assessment of included studies with full article published. GEMSTONE-303, COMPASSION-15 and SHR-1701 only provided meeting abstracts.
Study characteristics
The characteristics of the included studies are summarized in Table 1. All nine clinical trials were ultimately included comparing the efficacy of chemotherapy combined with ICIs versus chemotherapy plus placebo in adult patients with locally advanced, unresectable or metastatic GC/GEJC. All but the COMPASSION-15 and SHR-1701 trials used a single ICI, whereas COMPASSION-15 used Cadonilimab, a bispecific antibody against PD-L1 and CTLA-4, and the SHR-1701 trial used a bispecific antibody (Retlirafusp alfa) against PD-L1 and TGF-βR II.
Characteristics and interventions of studies included in the meta-analysis.

CAPOX, capecitabine and oxaliplatin; CPS, combined positive score; FOLFOX, fluorouracil, leucovorin, and oxaliplatin; G/GEJ A, gastric/gastroesophageal junction adenocarcinoma; ITT, intention-to-treat population; OS, overall survival; PFS, progression-free survival; TAP, tumor area positivity; TPS, tumor proportion score; XELOX, capecitabine and oxaliplatin.
Two of these studies provided survival data at different follow-up times or in multiple ethnic subgroups. CHECKMATE-64910,11,22,29 presented data from the global and Chinese subgroups at 2- and 3-year follow-up; and the KEYNOTE-06212,25,30 study offered data about the global and Asian subgroups. Ultimately, we only included data from the 2-year follow-up of the global subgroup of CHECKMATE-649, and the global subgroup of KEYNOTE-062. Regarding the scoring system for PD-L1 expression levels, seven studies used the CPS score, ATTRACTION-4 24 used the TPS score, and RATIONALE-305 26 used the TAP scoring system.
Reconstruction of time-to-event outcomes
Since KEYNOTE-859 did not report PFS KM curves for patients with PD-L1 CPS score < 1, SHR-1701 did not report OS and PFS curves for patients with CPS score < 5. In order to obtain as much survival data as possible for the low-expression population, we extracted KM curves for the total population and the subgroups of patients with CPS scores ⩾1 and CPS ⩾5 to reconstruct the IPD, and applied KMSubtraction to ultimately obtain the results of time to event for patients with CPS scores <1 and <5 (Figure 3). KM curves were reconstructed and HR values and 95% CIs for OS and PFS were derived.

Survival curves for the reconstructed low-expression subgroups. (a) KEYNOTE-859 CPS < 1 subgroup PFS, (b) SHR-1701 CPS < 5 subgroup OS, (c) SHR-1701 CPS < 5 subgroup PFS.
Quality assessment of trials and reconstructed data
Except for the CheckMate-649, GEMSTONE-303 and COMPASSION-15 trials, which had a risk of bias with some concerns, the other six studies had a low risk. By comparing risk tables, marginal HRs and visual inspection, the reconstructed KM curves for the ITT population and the PD-L1 high-expressing population were in high agreement with those provided in the original studies (Table S3). For the subgroup with low PD-L1 expression, KMSubtraction yielded HRs, which were similar or even identical to previously reported results. For example, the ORIENT-16 trial published an HR and 95% CI of 0.88 (0.65–1.19) for OS in those with PD-L1 CPS < 5, whereas our reconstruction of the data yielded 0.92 (0.67–1.25; Table S4). This provided confidence in the continued application of reconstructed data for survival analyses.
The empirical cumulative distribution functions showed good overlap between matched pairs. On the Bland–Altman plots, mean absolute differences in follow-up time between matched pairs were small (differences were around 0; Table S5). For each KMSubtraction implementation, over 1000 Monte Carlo iterations simulations showed that the converted error limits were reasonable (Table S6).
Overall survival
Given the variety of immunological drugs used across different clinical trials, we conducted separate pooled analyses for trials involving monoclonal antibodies and bispecific antibodies to minimize bias and compare the results. In the pooled analysis of the overall population, we found that both monoclonal antibody-based combination chemotherapy (HR = 0.80, 95% CI: 0.74–0.86, p < 0.001) and bispecific antibody-based combination chemotherapy (HR = 0.64, 95% CI: 0.55–0.75, p < 0.001) significantly improved OS compared to chemotherapy alone. Notably, the bispecific antibody group showed a more pronounced improvement in OS (Figure 4). In trials that used CPS to determine PD-L1 scores, we focused on analyzing subgroups with CPS < 1 and CPS < 5. In the subgroup of CPS < 1 and CPS < 5, immunotherapy plus chemotherapy did not prolong patients’ median OS compared with chemotherapy alone (monoclonal antibody: CPS < 1 HR = 0.91, 95% CI: 0.77–1.08, p = 0.277; monoclonal antibody: CPS < 5 HR = 0.92, 95% CI: 0.79–1.08, p = 0.322; bispecific antibodies: CPS < 5 HR = 0.83, 95% CI: 0.58–1.20, p = 0.323; Figure 5). Notably, in the COMPASSION-15 trial, cadonilimab + chemotherapy prolonged OS in the subgroup of patients with CPS < 5 compared with chemotherapy alone (HR = 0.70, 95% CI: 0.51–0.95, p = 0.011). In trials using the TAP score, the subgroup of patients with a TAP < 5% also did not benefit from immune combination therapy (HR = 0.92, 95% CI: 0.75–1.13; the p-value was not provided in the original text).

Forest plot comparing overall survival with ICIs plus chemotherapy versus chemotherapy alone in the total population. (a) Monoclonal antibody trials. (b) Bispecific antibodies trials.

Forest plot comparing overall survival with ICIs plus chemotherapy versus chemotherapy alone in the PD-L1 low-expression subgroup. (a) CPS < 1 monoclonal antibody trials. (b) CPS < 5 monoclonal antibody trials. (c) CPS < 5 bispecific antibody trials.
Progression-free survival
In a pooled analysis of the total population, ICIs in combination with chemotherapy significantly prolonged patients’ PFS compared with chemotherapy plus placebo (monoclonal antibody: HR = 0.74, 95% CI: 0.69–0.80, p < 0.001; bispecific antibodies: HR = 0.55, 95% CI: 0.48–0.63, p < 0.001) (Figure 6). In the CPS < 1 and CPS < 5 subgroup, there was no difference in PFS between monoclonal antibody + chemotherapy compared with chemotherapy alone (CPS < 1:HR = 0.88, 95% CI: 0.74–1.06, p = 0.193; CPS < 5: HR = 0.78, 95% CI: 0.53–1.14, p = 0.200; Figure 7). Encouragingly, in clinical trials using dual antibodies, an improvement in PFS was seen in patients with CPS < 5 compared to the placebo group (HR = 0.64, 95% CI: 0.52–0.80, p < 0.001) (Figure 8). Notably, in the COMPASSION-15 trial, the addition of ICIs improved PFS in the CPS < 5 subgroup of patients (HR: 0.60, 95% CI: 0.45–0.79, p < 0.001). In the subgroup with TAP < 5%, there was no statistically significant difference in PFS between ICIs plus chemotherapy and chemotherapy alone (HR = 0.91, 95% CI: 0.74–1.13, the p-value was not provided in the original text).

Forest plot comparing progression-free survival of ICIs plus chemotherapy versus chemotherapy alone in the full population. (a) Monoclonal antibody trials. (b) Bispecific antibodies trials.
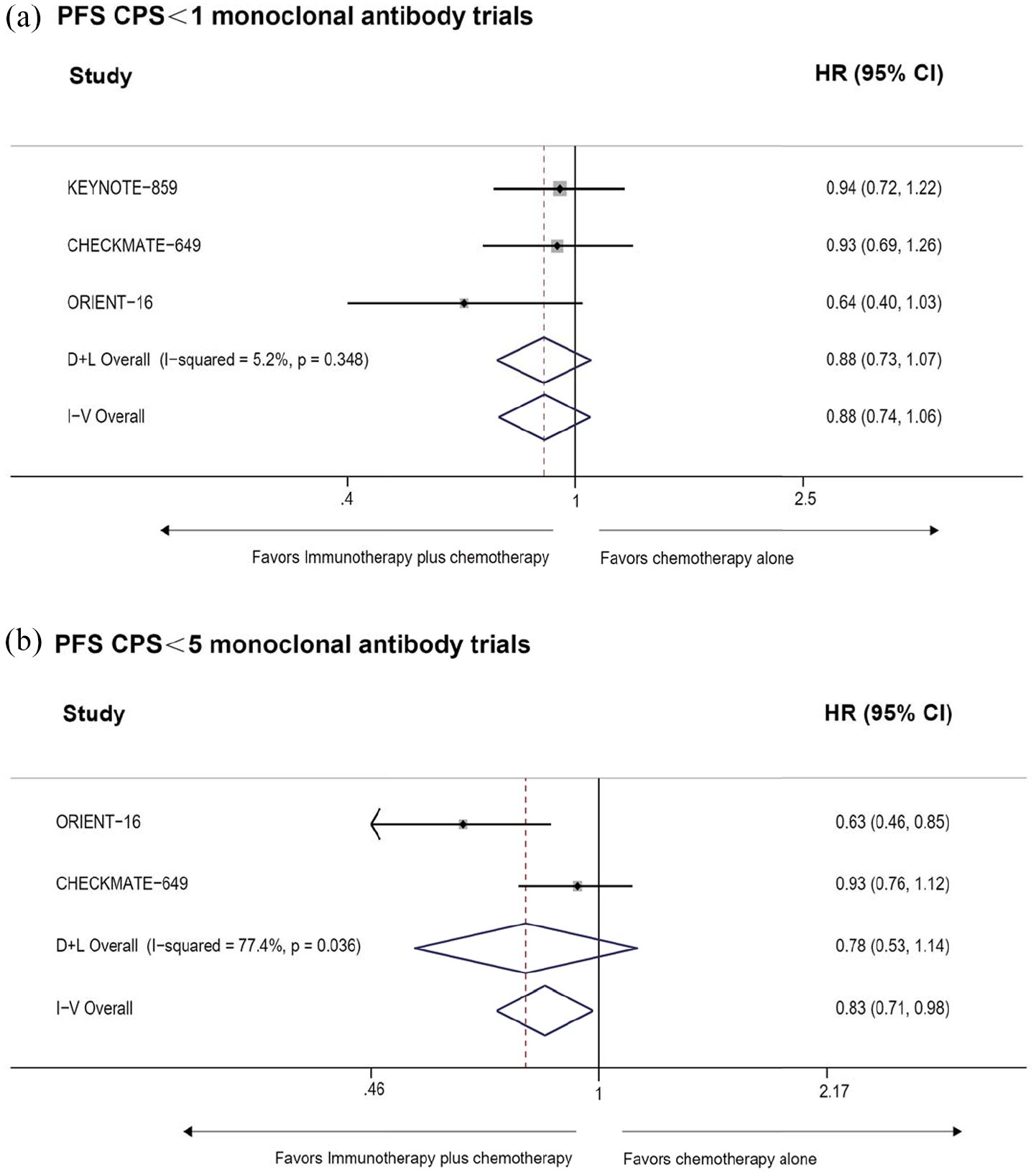
Forest plot comparing progression-free survival of monoclonal antibody plus chemotherapy versus chemotherapy alone in the PD-L1 low-expression subgroup. (a) CPS < 1. (b) CPS < 5.

Forest plot comparing progression-free survival of bispecific antibodies plus chemotherapy versus chemotherapy alone in the PD-L1 CPS < 5 subgroup.
Publication bias and sensitivity analyses are detailed in Table S7 and Figure S1. The funnel plot is approximately symmetrical, and neither Begg’s test nor Egger’s test showed significant publication bias. The results of the sensitivity analysis indicate that in the subgroup with CPS < 5, the summary results of PFS from ORIENT-16 and CHECKMATE-649 exhibit strong heterogeneity. After excluding the ORIENT-16 study, the estimated confidence interval is relatively wide, ranging from approximately 0.46 to 1.34. This suggests that excluding this study has a considerable impact on the meta-analysis estimate, leading to increased uncertainty in the overall estimate. Given the small number of studies in this subgroup and the high heterogeneity, a random-effects model was applied. Additionally, there is significant heterogeneity between the SHR-1701 and COMPASSION-15 studies. After excluding SHR-1701, the estimated confidence interval becomes very wide (approximately 0.51–1.49), which may be attributed to differences in study designs. Additionally, due to the limited number of studies, subgroup analysis cannot be conducted at this time. In short, the results show that this meta-analysis is statistically stable.
Discussion
In recent years, immunotherapy has developed rapidly, and the combination of chemotherapy and immunotherapy has gradually become a new strategy against advanced gastric and GEJ adenocarcinoma. 31 Satisfactory clinical benefits have been achieved in many randomized controlled trials,9,13 especially in populations with high PD-L1 expression. This was consistent with the results of our pooled analysis, which showed that the immune-combination chemotherapy arm delivered significant OS and PFS benefit relative to the chemotherapy arm for the CPS score ⩾ 5 subgroup and the ITT population (Figures S2 and S3 and Figures 4 and 6). Notably, trials using bi-antibodies, including SHR-1701 and COMPASSION-15, prolonged patients’ OS and PFS more than other trials using monoclonal antibodies. CheckMate-649 study opened new era of immunotherapy for first-line treatment of advanced GC. Four-year follow-up data from the Chinese subgroup presented at the 2024 Gastrointestinal Cancer Symposium of the ASCO GI 2024) showed that in patients with PD-L1 CPS ⩾5, the 4-year OS rate for nivolumab plus chemotherapy reached 25%, compared to 11% in the chemotherapy group. 32 This suggested that patients with advanced GC can achieve durable benefit from the use of nivolumab in the first-line setting, particularly in Chinese population.
In addition, in the RATIONALE-305 study using TAP scoring, the combination of tislelizumab and chemotherapy provided a superior survival benefit compared to chemotherapy alone in both the ITT population and the TAP ⩾ 5% population. 26 Notably, tislelizumab was originally designed to completely eliminate FcγR binding capacity, resulting in more durable remissions in responsive populations. 33 It has been approved for first-line treatment of locally advanced unresectable or metastatic gastric and gastroesophageal junction (G/GEJ) adenocarcinoma. In the GEMSTONE-303 trial, the combination of sugemalimab with CAPOX significantly improved PFS and OS, with manageable safety, potentially becoming a new first-line treatment option for advanced G/GEJ adenocarcinoma patients with PD-L1 expression ⩾ 5%. 28
However, the efficacy of ICIs in combination with chemotherapy in the low PD-L1 expression population has not yet yielded consistent results. Since the low PD-L1 subgroup was not the focus of many previous studies, survival curves, HRs, and 95% CIs for OS and PFS in this subgroup were not reported in most studies. Nevertheless, in the real world, GC patients with PD-L1 CPS < 5 account for approximately half of all GC patients, highlighting the significant need to investigate whether such patients can benefit from immune-combination therapy.
Therefore, this study utilized the KMSubtraction method to extract as much data as possible for a pooled analysis. Our analysis indicated that neither the CPS < 1 subgroup nor the CPS < 5 subgroup benefited from monoclonal antibody combination therapy in terms of OS and PFS. In the RATIONALE-305 study, patients who were defined in a post-hoc exploratory analyses with TAP < 1, accounting for 11% of the total population, had no benefit from the addition of tislelizumab to chemotherapy. However, in trials using dual antibodies, patients with PD-L1 CPS < 5 achieved greater improvements in PFS. Especially in the COMPASSION-15 trial, cadonilimab improved OS and PFS relative to chemotherapy alone in the subgroup of patients with CPS < 5. The possible reasons are as follows. First, cadonilimab is the world’s first PD-1/CTLA-4 bispecific antibody, with higher affinity binding to tumor-infiltrating lymphocytes co-expressing PD-1 and CTLA-4.34,35 It reduces tumor cell activation of related immune suppression pathways and enhances T-cell-mediated immune responses, demonstrating significant efficacy across various tumors.36,37 Second, the populations included was Asian. Previous studies have suggested that Asian patients may benefit more from ICIs than patients of other races.9,38
It was worth noting that the COMPASSION-15 study, 27 presented at the AACR in April 2024, showed that Cadonilimab (AK104) in combination with oxaliplatin and capecitabine (XELOX) reduced the proportion at risk of death by 44% in those with PD-L1 CPS ⩾ 5. Even in patients with PD-L1 CPS < 5, the combination therapy also significantly reduced the risk of death by 30%. This breakthrough overcomes the limitations of previous ICIs combined with chemotherapy, which have shown little benefit in low PD-L1 populations, and provides a promising new first-line treatment for advanced GC patients with low PD-L1 expression (CPS < 5). Currently, AK104 combined with XELOX for first-line treatment of advanced GC (HER2-negative) has been included in the CSCO Guidelines for the Clinical Use of ICIs (2024) as a level III recommendation (Class 1A).
In addition, the results of SHR-1701 offer novel insights for oncologists to explore immunotherapy options for GC in the future. SHR-1701, as the first drug to demonstrate positive outcomes in the PD-L1/TGF-β dual-antibody combination, significantly prolonged OS in the intention-to-treat (ITT) population as well as in those with PD-L1 CPS ⩾ 5, effectively controlling disease progression. Notably, this benefit was even more pronounced in patients with PD-L1 CPS ⩾ 5.
Overall, the available data support that the survival benefit of adding immunotherapy in patients with advanced gastric and GEJ adenocarcinoma is related to the level of PD-L1 expression.9,13 However, PD-L1 is a dynamic biomarker, and a variety of other factors can affect the measurement of PD-L1. In addition, we should also realize that the variation in response to immunotherapy in different GC patients is far from being explained by the level of PD-L1 expression alone.39,40 GC is an extremely heterogeneous malignant tumor, and the tumor microenvironment (TME) varies greatly among different ethnicities, genders and ages.38,41,42 Recent studies have also indicated numerous potential biomarkers and mechanisms influencing the effectiveness of immunotherapy in GC.43–45 For example, Jinsong Wang et al. found that the expression levels of three hub genes, CDH6, EGFLAM, and RASGRF2, differed significantly in GC patients, which might be one of the reasons for the differences in susceptibility to immunotherapy and immune resistance among patients. 46
Additionally, it is important to select an appropriate CPS cut-off value to ensure that only patients who are most likely benefit from the treatment receive it. For example, the results of CheckMate-649 suggest that selecting a cut-off value of CPS ⩾ 1 is the most reasonable choice. Yet the European Medicines Agency (EMA) has only approved Nivolumab for patients with PD-L1 CPS ⩾ 5.
In the future, we need to continue exploring biomarkers for predicting the efficacy of immunotherapy in GC. 44 We should thoroughly analyze the characteristics of the immune microenvironment, determine the immune status of GC patients and investigate the mechanisms of adaptive immune resistance (AIR) 47 in these patients. More careful consideration should be given to triple-targeted immunotherapy, dual immunotherapy, T-cell receptor-engineered T-cell therapy (TCR-T), innovative drug therapies and other new combinations and strategies.41,48 Efforts are being made to overcome ICIs resistance, achieve precision treatment of GC, and improve the survival prospects of patients with advanced GC, including those with low PD-L1 expression.
There are five limitations in our study, first in reconstructing the KM curves, although we used a series of quality checks to keep the reconstructed HRs as close as possible to the reported HRs, we recognized that there were still some small differences. Second, different trials have taken varying approaches to measuring PD-L1 levels, ranging from TAP scoring using the VENTANA PD-L1 (SP263) assay, to combined positivity scoring (CPS) scoring using the immunohistochemistry 28-8 pharmDx kit. Although the consistency of the measurements had been reported, 27 we performed the statistical analyses separately. Third, the reconstructed IPD method has certain limitations. For instance, it typically focuses only on time and event status, and does not account for covariates such as gender, age, and disease stage. Additionally, the method relies heavily on the accuracy of data extraction, which can introduce errors into the results. Moreover, it lacks real individual data as a gold standard, making it challenging to conduct sufficient validation. Fourth, the included trials utilized two distinct chemotherapy regimens. Pooling these regimens for analysis may introduce increased heterogeneity in the effect sizes. Although both regimens are standard first-line treatments for GC and demonstrate comparable clinical efficacy, it is important to acknowledge that such pooling may mask potential underlying differences between the drugs. Additionally, due to the limited number of trials, subgroup analyses are not currently feasible. Finally, our inclusion criteria were limited to studies published in English, which may affect the comprehensiveness of the results. Since English is still the international common language, formal and large-scale clinical trials are often registered and reported in English. Based on the above considerations, we believe that this limitation has a minimal impact on the conclusions. Future research could systematically search multilingual databases to enhance the global applicability of the results.
Conclusion
In summary, this meta-analysis updates the most recent data and reconstructs survival data for patients with low PD-L1 expression using the KMSubtraction approach. The results suggest that the addition of a single ICI to conventional chemotherapy is less effective in patients with low PD-L1 expression. This generally aligns with the EMA recommendation to approve Nivolumab only for patients with PD-L1 CPS⩾5. Currently, consensus recommends CPS ⩾ 5 as the diagnostic threshold for high PD-L1 expression in GC patients. For those with low (CPS < 5) PD-L1 expression, chemotherapy combined with bispecific antibodies based on PD-1 targets (e.g., Cadonilimab) may be considered for treatment. 49 Pooled analyses demonstrated that dual-antibody therapy not only significantly improved OS and PFS in ITT population and CPS ⩾ 5 subgroup, but also enhanced PFS in patients with CPS < 5, compared to monoclonal antibody treatments. All in all, current guidelines recommend that patients with PD-L1 expression < 1 should not be treated with PD-L1 inhibitors. The optimal treatment regimen for patients with scores between 1 and 10 remains a significant challenge. Dual antibodies may offer a more effective option for those with scores >5.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251336627 – Supplemental material for Comparison of immune checkpoint inhibitors in combination with chemotherapy versus chemotherapy alone in the first-line treatment of advanced gastric cancer patients with low PD-L1 expression: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tam-10.1177_17588359251336627 for Comparison of immune checkpoint inhibitors in combination with chemotherapy versus chemotherapy alone in the first-line treatment of advanced gastric cancer patients with low PD-L1 expression: a systematic review and meta-analysis by Yuxin Wang, Tong Xie, Shuai Xiang, Cheng Liu, Siyuan Cheng, Bohan Zhang, Yifan Zhang, Yang Feng, Yingxuan Wang, Donghe Yu, Hongchao Gao, Erke Gao, Lin Shen and Zhi Peng in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.