
Abstract
Background:
Despite treatment advances for patients with early-stage triple-negative breast cancer (TNBC) and hormone receptor (HR)-low/human epidermal growth factor receptor 2-negative (HER2−) breast cancer, treatments that improve clinical outcomes while mitigating toxicity are needed. Datopotamab deruxtecan (Dato-DXd), a TROP2-directed antibody-drug conjugate consisting of a humanized IgG1 monoclonal antibody attached via a plasma-stable cleavable linker to a topoisomerase-I inhibitor payload, has shown efficacy alone or in combination with durvalumab, a selective, high-affinity anti-programmed cell death ligand 1 antibody, in early-phase clinical studies.
Objectives:
The primary objective of TROPION-Breast04 is to evaluate the efficacy and safety of neoadjuvant Dato-DXd plus durvalumab followed by adjuvant durvalumab with or without chemotherapy versus standard of care in patients with previously untreated early-stage TNBC or HR-low/HER2− breast cancer.
Design:
This is an ongoing, international, phase III, open-label, randomized controlled study.
Methods and analysis:
Approximately 1728 patients (aged ⩾18 years) will be randomized 1:1 to eight cycles of neoadjuvant Dato-DXd (6 mg/kg intravenously (IV) every 3 weeks (Q3W)) plus durvalumab (1120 mg IV Q3W) followed by nine cycles of adjuvant durvalumab (1120 mg IV Q3W) with or without chemotherapy versus eight cycles of pembrolizumab (200 mg IV Q3W) plus chemotherapy followed by nine cycles of adjuvant pembrolizumab (200 mg IV Q3W) with or without chemotherapy. Dual primary endpoints are pathological complete response by blinded central review and event-free survival by investigator assessment. Secondary endpoints include overall survival (key), distant disease-free survival, patient-reported outcomes, and safety.
Ethics:
The study is approved by independent ethics committees and/or institutional review boards at each study site. All patients will provide written informed consent.
Discussion:
This study will evaluate the potential use of neoadjuvant Dato-DXd plus durvalumab followed by adjuvant durvalumab with or without chemotherapy versus standard of care in patients with previously untreated early-stage TNBC or HR-low/HER2− breast cancer. The findings of this trial could lead to promising treatment options for these patients.
Trial registration:
ClinicalTrials.gov identifier: NCT06112379.
Plain language summary
People with TNBC have neither estrogen receptors and/or progesterone receptors nor a protein called HER2 expressed on their cancer cells. Standard treatment for early-stage TNBC that has not spread to other parts of the body and can be removed by surgery is pembrolizumab (a drug that makes cancer cells more susceptible to being killed by the immune system) plus chemotherapy before surgery, and pembrolizumab after surgery. People with HR-low/HER2− breast cancer (BC) do not have HER2 but have low levels of estrogen/progesterone receptors on their cancer cells and may be treated similarly to those with TNBC. Some people with high-risk early-stage TNBC or HR-low/HER2− BC experience a recurrence of their cancer after standard treatment. Therefore, new therapies that stop cancer returning and improve long-term outcomes are needed. Datopotamab deruxtecan (Dato-DXd) is an antibody-drug conjugate that consists of an antibody (datopotamab) and an anticancer drug payload (DXd), joined via a stable cleavable linker. In people with TNBC that has spread to other parts of the body, promising outcomes have been observed with Dato-DXd alone or in combination with durvalumab (a drug that makes cancer cells more susceptible to being killed by the immune system). In the TROPION-Breast04 study, approximately 1700 people with early-stage TNBC or HR-low/HER2– BC who have not received previous treatment will be randomly assigned in equal numbers to receive Dato-DXd plus durvalumab followed by surgery and durvalumab with or without chemotherapy, or pembrolizumab plus chemotherapy followed by surgery and pembrolizumab with or without chemotherapy. TROPION-Breast04 will show if Dato-DXd plus durvalumab before surgery followed by durvalumab with or without chemotherapy after surgery can help people with early-stage TNBC and HR-low/HER2– BC live longer without their cancer returning versus pembrolizumab plus chemotherapy before surgery followed by pembrolizumab with or without chemotherapy.
Keywords
Introduction
In 2022, 2.3 million cases of breast cancer were recorded globally, 670,000 of which resulted in death. 1 Breast cancer is a heterogeneous disease and survival estimates vary. For example, 92.5% of patients with hormone receptor positive (HR+)/human epidermal growth factor receptor 2-negative (HER2−) breast cancer are alive 4 years after diagnosis, compared with 77% of patients with triple-negative breast cancer (TNBC), which lacks expression of estrogen (ER) and progesterone (PR) receptors and HER2. 2 TNBC is considered the most aggressive breast cancer subtype, and most patients are diagnosed with early-stage disease, which has limited treatment options.3–5 Approximately 25%–30% of patients with early-stage TNBC relapse with distant metastases, with a median time from diagnosis to distant metastases of approximately 2 years.4,5 Thus, improving treatment options for patients with early-stage disease may prevent recurrence and improve long-term outcomes. In addition, there is limited evidence demonstrating the benefit of endocrine therapy in patients with HR-low breast cancer, defined as 1% to <10% of cells staining positive for ER and/or PR.6–8 Several studies have shown that the prognosis for patients with HR-low/HER2− breast cancer and the biology of their tumors are comparable to TNBC and suggest that these patients could be treated similarly.9–12
Current treatment guidelines for early-stage TNBC recommend the combination of chemotherapy with or without immunotherapy as standard of care.8,13,14 This recommendation is based on the results of the phase III, randomized, double-blind KEYNOTE-522 study (NCT03036488).15,16 In KEYNOTE-522, 1174 patients with stage II or stage III TNBC (primary tumor stage (T) T1c, nodal stage (N) N1–2, or T2–4, N0–2, according to the American Joint Committee on Cancer staging criteria (AJCC), 7th edition) were randomized 2:1 to neoadjuvant pembrolizumab (an anti-programmed cell death 1 (PD-1) antibody) plus chemotherapy followed by surgery and adjuvant pembrolizumab (n = 784) or neoadjuvant placebo plus chemotherapy followed by surgery and adjuvant placebo (n = 390). The dual primary endpoints of pathological complete response (pCR) and event-free survival (EFS) were significantly improved in the pembrolizumab plus chemotherapy arm versus the placebo plus chemotherapy arm (patients with pCR: 64.8% vs 51.2%, respectively (p < 0.001); EFS at 18 months: 91.3% vs 85.3%, respectively (hazard ratio 0.63, 95% confidence interval (CI): 0.43–0.93) 15 ; 5-year EFS: 81.2% (95% CI: 78.3–83.8) vs 72.2% (95% CI: 67.4–76.4), respectively). 17 Additionally, overall survival (OS) was significantly improved in the pembrolizumab plus chemotherapy arm versus the placebo plus chemotherapy arm (5-year OS: 86.6% (95% CI: 84.0–88.8) vs 81.7% (95% CI: 77.5–85.2), respectively (p = 0.002)). 17 In the pembrolizumab plus chemotherapy arm, 77.1% of patients experienced a grade ⩾3 treatment-related adverse event (TRAE) and 34.1% experienced serious TRAEs. In the combined neoadjuvant and adjuvant phases, 27.7% of patients discontinued due to TRAEs. 16 In both study arms, most TRAEs occurred during the neoadjuvant phase, and the most frequent grade ⩾3 TRAEs were consistent with those typically observed with chemotherapy, suggesting that the TRAEs reported were mainly linked to the chemotherapy backbone.15,16
Despite the improvements observed in clinical outcomes, approximately 35% of patients receiving pembrolizumab plus chemotherapy had residual disease at the time of surgery, 15 and an exploratory analysis of KEYNOTE-522, as well as analyses of historical trials, have shown that patients who do not achieve pCR with neoadjuvant treatment have worse prognosis.16,18 Consequently, there remains a need to develop novel treatment approaches that improve pCR rates, reduce relapse, and increase long-term survival while reducing chemotherapy-associated toxicity.
Datopotamab deruxtecan (Dato-DXd) is an antibody-drug conjugate (ADC) consisting of a humanized anti-trophoblast cell-surface antigen 2 (TROP2) immunoglobulin G1 monoclonal antibody (datopotamab) attached to a highly potent topoisomerase I inhibitor payload (an exatecan derivative) via a tetrapeptide-based, plasma-stable, tumor-selective cleavable linker. 19 Dato-DXd binds to TROP2-expressing cells and is internalized and trafficked to the lysosome, where the DXd payload is released, leading to DNA damage and cell death by apoptosis. 19 Dato-DXd also exhibits a potent bystander effect where the payload affects surrounding tumor cells. 20 TROP2 is typically highly expressed in TNBC21–23 and, therefore, represents a viable target to deliver a cytotoxic payload to tumor cells while minimizing systemic toxicity.
Data from the phase I TROPION-PanTumor01 study (NCT03401385) demonstrated that Dato-DXd monotherapy had encouraging preliminary efficacy in patients with heavily pretreated advanced/metastatic TNBC. In this study, the confirmed objective response rate (ORR) was 32% in all patients and 40% in patients who were naïve to topoisomerase I inhibitors and who had measurable disease at baseline. 24 A disease control rate of 80% was reported, and the median duration of response was 16.8 months (95% CI: 5.6–not calculable (NC)). 24 Median progression-free survival (PFS) by blinded independent central review was 4.4 months (95% CI: 3.0–7.3) and median OS was 13.5 months (95% CI: 10.1–16.3). 24 Recent data from the open-label, randomized, phase III TROPION-Breast01 study (NCT05104866) also demonstrated that, in patients with previously treated inoperable/metastatic HR+/HER2− breast cancer, Dato-DXd monotherapy was associated with a statistically significant and clinically meaningful improvement in PFS compared with investigator’s choice of chemotherapy (ICC; hazard ratio 0.63 (95% CI: 0.52–0.76); p < 0.0001). 25 In these studies, Dato-DXd had a manageable safety profile. TRAEs with Dato-DXd were reported in 97.7% of patients with TNBC in TROPION-PanTumor01. 24 The most common TRAEs (any grade, grade ⩾3) were stomatitis (72.7%, 11.4%), nausea (65.9%, 2.3%), and fatigue (34.1%, 6.8%). 24 In the TROPION-Breast01 study, the most common TRAEs (any grade, grade ⩾3) with Dato-DXd were nausea (51.1%, 1.4%), stomatitis (50.0%, 6.4%), and alopecia (36.4%, 0%). The rate of grade ⩾3 TRAEs with Dato-DXd was less than half that with ICC (20.8% vs 44.7%) and TRAEs led to fewer dose reductions and interruptions in the Dato-DXd arm versus the ICC arm (20.8% vs 30.2% and 11.9% vs 24.5%, respectively). Treatment discontinuations due to TRAEs were reported in 2.5% of patients in the Dato-DXd arm. 25
Preclinical evidence has demonstrated that the combination of Dato-DXd and PD-(L)1 inhibitors provides additional benefit compared with Dato-DXd monotherapy. 26 ADCs can trigger immunogenic cell death and immune cell recruitment, including T-cells, to tumor sites, complementing the ability of immune checkpoint inhibitors to enhance the antitumor function of those T-cells.27–30 Furthermore, preclinical studies have shown that the activity of PD-(L)1 inhibitors may be increased when combined with ADCs due to increased PD-L1 expression, dendritic cell activation, and enhanced neoantigen formation in the tumor microenvironment. 31 Given these data, there is a rationale that the combination of Dato-DXd and immune checkpoint inhibitors may lead to improved clinical responses (Figure 1). Durvalumab is a selective, high-affinity, human immunoglobulin G1 anti-PD-L1 monoclonal antibody that is approved either alone or in combination therapies in various settings, including lung, urothelial carcinoma, hepatocellular carcinoma, biliary tract cancer, and endometrial cancer indications.32–38 Durvalumab in combination with neoadjuvant chemotherapy has also shown antitumor activity in patients with early-stage TNBC, based on results of the randomized phase II GeparNuevo study (NCT02685059). 39 Exploratory analyses reported improvements in long-term outcomes with the addition of durvalumab: 3-year invasive disease-free survival (DFS) was 85.6% with durvalumab versus 77.2% with placebo (hazard ratio 0.48 (95% CI: 0.24–0.97); p = 0.036); distant DFS was 91.7% versus 78.4% (hazard ratio 0.31 (95% CI: 0.13–0.74); p = 0.005); and OS was 95.2% versus 83.5% (hazard ratio 0.24 (95% CI: 0.08–0.72); p = 0.006) with durvalumab versus placebo, respectively. 39 Preliminary clinical data for durvalumab in combination with Dato-DXd were reported in the phase Ib/II BEGONIA study (NCT03742102), which demonstrated robust and durable tumor responses in patients with previously untreated advanced/metastatic TNBC (ORR: 79% (n = 49 of 62, including six complete responses); median follow-up 11.7 months, median duration of response 15.5 months, and median PFS 13.8 months) irrespective of PD-L1 expression. 40 The safety profile reported in the BEGONIA study was consistent with the known safety profiles of both agents when given as monotherapy, with no new safety signals reported. 40 Subsequently, data from the phase II I-SPY2.2 study also demonstrated promising efficacy of up to four cycles of neoadjuvant Dato-DXd plus durvalumab in the breast cancer setting, including in patients with TNBC. 41 In patients with TNBC, 62% achieved pCR, of which 54% were achieved after the patients received Dato-DXd plus durvalumab only. 41

Mechanism of action of Dato-DXd and durvalumab.
Here, we describe the design of TROPION-Breast04, which aims to evaluate the efficacy and safety of neoadjuvant Dato-DXd plus durvalumab followed by adjuvant durvalumab with or without chemotherapy, versus neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab with or without chemotherapy in patients with previously untreated early-stage TNBC or HR-low/HER2− breast cancer.
Methods
Study design
TROPION-Breast04 (NCT06112379) is an ongoing, international, phase III, open-label, randomized controlled study investigating the efficacy and safety of neoadjuvant Dato-DXd plus durvalumab followed by adjuvant durvalumab with or without chemotherapy, compared with standard of care neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab with or without chemotherapy in patients with previously untreated early-stage TNBC or HR-low/HER2− breast cancer (Figure 2). An anticipated 1728 patients will be enrolled and randomized 1:1 to each of the study arms (Table 1). In both arms, adjuvant chemotherapy may be given if patients have residual disease; adjuvant therapy will be determined by the investigator based on the available options in the respective treatment arm. In the Dato-DXd plus durvalumab arm, adjuvant chemotherapy may be four cycles of doxorubicin or epirubicin plus cyclophosphamide followed by four cycles of paclitaxel and carboplatin; four cycles of doxorubicin or epirubicin plus cyclophosphamide followed by four cycles of paclitaxel; four cycles of carboplatin plus paclitaxel; or eight cycles of capecitabine. In the pembrolizumab plus chemotherapy arm, eight cycles of adjuvant capecitabine may be given. For patients with germline BRCA-positive tumors and residual disease, adjuvant olaparib may be given for a total period of 1 year; administration of olaparib may overlap with the nine adjuvant cycles of durvalumab or pembrolizumab, but olaparib may not be given concurrently with chemotherapy. Randomization will be stratified by lymph node status (positive vs negative), tumor stage (cT1 to cT2 vs cT3 to cT4), HR status (negative (ER and PR <1%) vs low (ER and/or PR 1% to <10%; neither may be ⩾10%)), and geographic location (United States/Canada/Europe/Australia vs other geographic regions). Treatment will be assigned using a randomization scheme via an Interactive Response Technology/Randomization and Trial Supply Management system. The randomization scheme will be generated by a computer software program and will comprise a blocked randomization list with randomization codes assigned sequentially for each stratum.

Study design.
Study interventions.

60 mg/m2 IV Q3W; [b]90 mg/m2 IV Q3W; [c]600 mg/m2 IV Q3W; [d]AUC 5 mg/mL/min IV Q3W or AUC 1.5 mg/mL/min IV QW (based on investigator preference); [e]80 mg/m2 IV QW; [f]1000 or 1250 mg/m2 (based on standard institutional practice) PO BID on Days 1–14, Q3W; [g]300 mg PO BID for 1 year; [h]there is no mandatory testing for gBRCA status; gBRCA status will be collected when applicable and if available.
AUC, area under the curve; BID, twice daily; Dato-DXd, datopotamab deruxtecan; gBRCA, germline breast cancer resistance gene; IV, intravenous; PO, orally; QW, weekly; Q3W, every 3 weeks.
The study is being performed in accordance with the Declaration of Helsinki, International Council for Harmonisation/Good Clinical Practice, and applicable regulatory requirements; all patients will provide written, informed consent. The reporting of this study conforms to the SPIRIT 2013 Statement 42 (Supplemental File).
Eligibility criteria
Key inclusion and exclusion criteria for TROPION-Breast04 are summarized in Table 2. Eligible patients include adults (aged ⩾18 years) with previously untreated histologically confirmed stage II–III (T1b/c, N1–2; T2, N0–2; T3, N0–2; T4a–d, N0–2) unilateral or bilateral primary invasive TNBC or HR-low/HER2− breast cancer (per AJCC staging criteria, eighth edition 43 ). TNBC and HR-low/HER2− breast cancer will be defined according to the American Society of Clinical Oncology-College of American Pathologists guidelines.6,44 TNBC will be defined as ER and PR <1% on immunohistochemistry (IHC); negative for HER2 with 0 or 1+ intensity on IHC, or 2+ intensity on IHC and no evidence of amplification on in situ hybridization (ISH). HR-low/HER2− breast cancer will be defined as ER 1% to <10% and/or PR 1% to <10% (neither HR may be ⩾10%); negative for HER2 with 0 or 1+ intensity on IHC, or 2+ intensity on IHC and no evidence of amplification on ISH. Eligible patients must have an Eastern Cooperative Oncology Group performance status of 0 or 1 and adequate bone marrow reserve and organ function. Patients with a history of another primary malignancy, including any prior invasive breast malignancy and except for malignancy treated with curative intent with no known active disease for 5 years, and patients with evidence of distant disease, are ineligible. Other key exclusion criteria include: evidence of severe or uncontrolled systemic diseases; active or prior autoimmune or inflammatory disorders; active or uncontrolled hepatitis B or C, human immunodeficiency virus infection that is not well controlled, or active tuberculosis infection; suspected, current, or previous noninfectious interstitial lung disease (ILD) or pneumonitis requiring steroids; clinically significant corneal disease. Patients with any prior or concurrent surgery, radiotherapy, or systemic anticancer therapy for TNBC or HR-low/HER2− breast cancer are also excluded from the study.
Key eligibility criteria.

ADC, antibody-drug conjugate; AJCC, American Joint Committee on Cancer; ASCO/CAP, American Society of Clinical Oncology/College of American Pathologists; ECG, electrocardiogram; ECOG PS, Eastern Cooperative Oncology Group performance status; ER, estrogen receptor; FFPE, formalin-fixed paraffin-embedded; HER2, human epidermal growth factor receptor 2; HIV, human immunodeficiency virus; HRT, hormone replacement therapy; HR-low, hormone receptor-low; ICF, informed consent form; IHC, immunohistochemistry; ILD, interstitial lung disease; ISH, in situ hybridization; IV, intravenous; ms, millisecond; PD-L1, programmed cell death ligand-1; PR, progesterone receptor; QTcF, QT interval corrected by Fridericia’s formula; TNBC, triple-negative breast cancer; TROP2, trophoblast cell-surface antigen 2.
Endpoints
Study endpoints are summarized in Table 3. The dual primary endpoints of TROPION-Breast04 are pCR by blinded central evaluation and EFS by investigator assessment. pCR rate is defined as the percentage of patients who have no residual invasive cancer or lymphovascular invasion on hematoxylin and eosin evaluation of the complete resected breast specimen and all sampled regional lymph nodes following completion of neoadjuvant systemic therapy (i.e., ypT0/Tis ypN0) per AJCC staging criteria (eighth edition). 43 EFS is defined as time from randomization until any of the following events: disease progression precluding surgery, disease recurrence (local, regional, distant, or contralateral), second primary invasive cancer (other than squamous or basal cell skin cancer) or relapse from prior malignancy, or death by any cause (in the absence of recurrence).
TROPION-Breast04 endpoints.
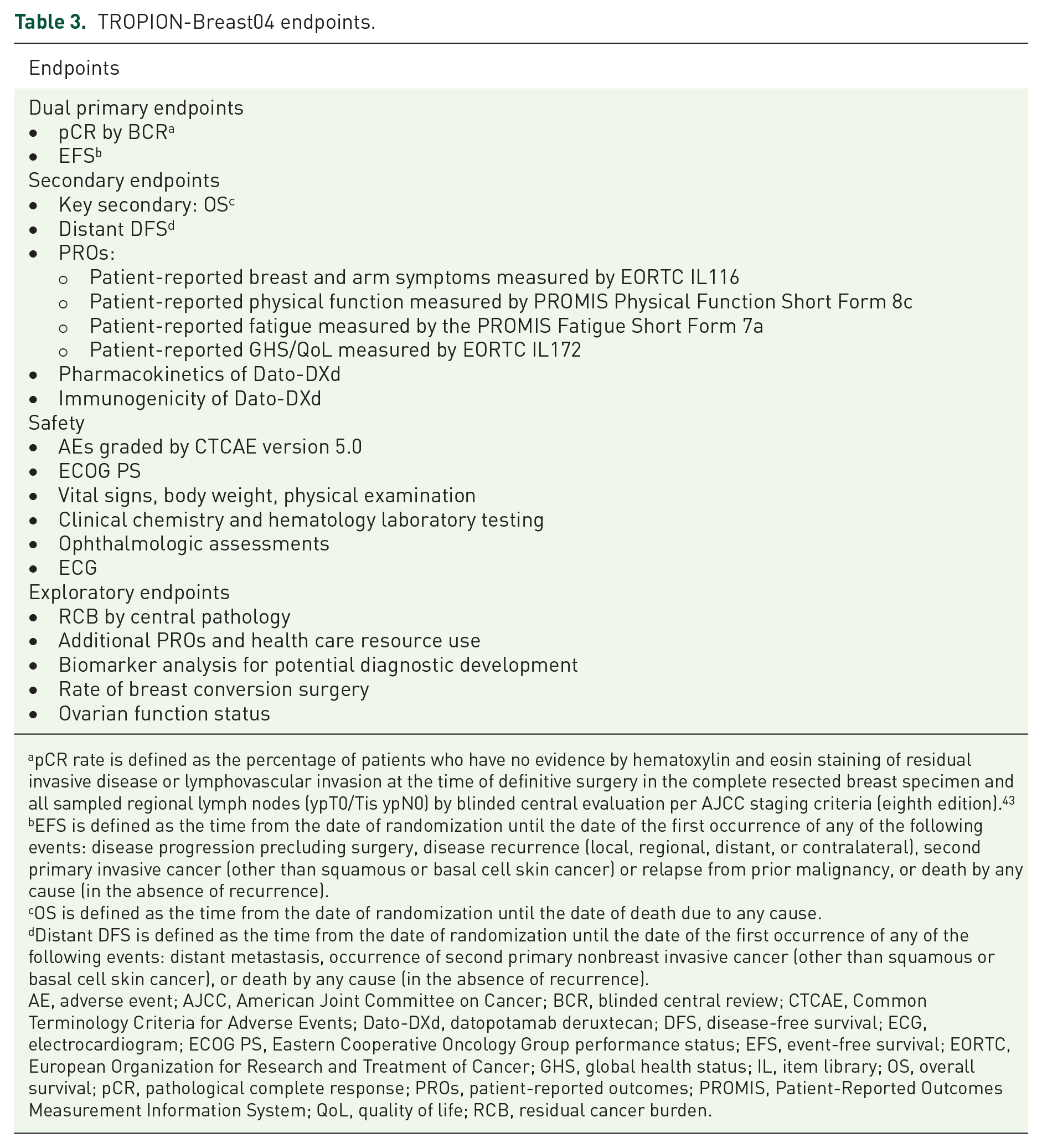
pCR rate is defined as the percentage of patients who have no evidence by hematoxylin and eosin staining of residual invasive disease or lymphovascular invasion at the time of definitive surgery in the complete resected breast specimen and all sampled regional lymph nodes (ypT0/Tis ypN0) by blinded central evaluation per AJCC staging criteria (eighth edition). 43
EFS is defined as the time from the date of randomization until the date of the first occurrence of any of the following events: disease progression precluding surgery, disease recurrence (local, regional, distant, or contralateral), second primary invasive cancer (other than squamous or basal cell skin cancer) or relapse from prior malignancy, or death by any cause (in the absence of recurrence).
OS is defined as the time from the date of randomization until the date of death due to any cause.
Distant DFS is defined as the time from the date of randomization until the date of the first occurrence of any of the following events: distant metastasis, occurrence of second primary nonbreast invasive cancer (other than squamous or basal cell skin cancer), or death by any cause (in the absence of recurrence).
AE, adverse event; AJCC, American Joint Committee on Cancer; BCR, blinded central review; CTCAE, Common Terminology Criteria for Adverse Events; Dato-DXd, datopotamab deruxtecan; DFS, disease-free survival; ECG, electrocardiogram; ECOG PS, Eastern Cooperative Oncology Group performance status; EFS, event-free survival; EORTC, European Organization for Research and Treatment of Cancer; GHS, global health status; IL, item library; OS, overall survival; pCR, pathological complete response; PROs, patient-reported outcomes; PROMIS, Patient-Reported Outcomes Measurement Information System; QoL, quality of life; RCB, residual cancer burden.
The key secondary endpoint is OS, defined as time from randomization until death due to any cause. Additional secondary endpoints include distant DFS (determined by the investigator and defined as time from randomization until distant metastasis, occurrence of second primary invasive cancer (other than squamous/basal cell skin cancer), relapse from prior malignancy, or death by any cause (in the absence of recurrence)) and patient-reported outcomes. Patient-reported outcomes will include breast and arm symptoms (via European Organisation for Research and Treatment of Cancer (EORTC) item library (IL) 116), physical function and fatigue (via Patient-Reported Outcomes Measurement Information System (PROMIS) Physical Function Short Form 8c and Fatigue Short Form 7a, respectively), and Global Health Status/Quality of Life (GHS/QoL) (via EORTC IL172). Pharmacokinetics and immunogenicity of Dato-DXd will also be investigated. Safety and tolerability will be evaluated. AEs will be graded using the National Cancer Institute Common Terminology Criteria for Adverse Events Version 5.0.
Study assessments and procedures
After completion of neoadjuvant treatment or early discontinuation of neoadjuvant treatment, patients will undergo definitive surgery according to local standard of care (e.g., breast conservation surgery or mastectomy with or without axillary lymph node dissection). Surgical specimens at definitive surgery will be collected from all patients for pCR assessment. Patients who do not undergo breast or axillary surgery (sentinel lymph node biopsy or axillary lymph node dissection) will be counted as nonresponders for pCR. All surgical specimens, including primary tumors, lymph nodes, and margins will be assessed locally, before sending for central assessment of pathologic response. While the primary efficacy endpoint of pCR will be measured by blinded central pathologists, adjuvant treatment decisions will be based on local assessment.
All patients will be assessed for disease recurrence/progression by reviewing medical history, physical examinations, and clinical signs and symptoms every 3 months for the first 2 years after randomization, every 6 months from Year 3 to Year 5, and then annually until death, withdrawal of consent, or end of the study. Bilateral mammogram or breast magnetic resonance imaging will be performed at screening (at diagnosis) and at least annually on any remaining breast tissue until recurrence/progression. For patients with no remaining breast tissue who underwent a bilateral mastectomy, a physical examination is sufficient, and imaging will not be required.
Patient-reported outcomes will be assessed via several different quality-of-life questionnaires and reporting tools, which will be self-administered electronically via handheld devices or the internet, at baseline and at various prespecified timepoints throughout the study. Breast and arm symptoms, via EORTC IL116, will be assessed every 3 weeks (Q3W) during the neoadjuvant treatment period, until presurgery safety follow-up or end of treatment (whichever occurs first). Physical functioning, fatigue, and GHS/QoL, via PROMIS and EORTC IL172, will be assessed Q3W throughout neoadjuvant and adjuvant treatment periods until end of treatment, then every 3 months in Years 1–2 and every 6 months in Years 3 and 4, until progression. After progression, PROs will be assessed every 3 months for 6 months.
Blood samples will also be collected at various time points and will be used for pharmacokinetic, immunogenicity, and biomarker analysis in the Dato-DXd arm. Ovarian function is an exploratory endpoint. Anti-Mullerian hormone (if feasible), follicle-stimulating hormone, luteinizing hormone, and estradiol-level measurements will be performed in females of child-bearing potential at screening, at the presurgery safety follow-up, at the end of adjuvant treatment, and at safety follow-up visits, and annually at 1 and 2 years after end of treatment. For postmenopausal patients, menopausal status will be assessed at screening only.
AEs and serious AEs will be monitored throughout the study and for 90 days after discontinuation of all study treatments; ILD or pneumonitis, regardless of severity, will be followed up beyond this period until event resolution. An independent data monitoring committee comprised of independent experts will review safety data and make recommendations to continue, amend, or stop the study based on safety findings. AEs will be managed according to the Dato-DXd and durvalumab toxicity management guidelines. AE-related dose delays are permitted for all study treatments, but dose reductions are not permitted for durvalumab and pembrolizumab. For suspected ILD or pneumonitis, if new or worsening pulmonary symptoms or radiological abnormality suggestive of ILD/pneumonitis is observed, Dato-DXd and/or durvalumab will be delayed and a full investigation will be required. For ILD/pneumonitis events of grade ⩾2, Dato-DXd will be permanently discontinued. A daily oral care protocol for stomatitis prophylaxis will be provided to all patients; a steroid-containing mouthwash (dexamethasone, or an alternative per local guidelines) is highly recommended for patients randomized to Dato-DXd or Dato-DXd in combination with durvalumab, and prophylactic cryotherapy (e.g., ice chips or ice water held in the mouth) during Dato-DXd infusion should also be considered. Ophthalmologic assessments will be carried out for all patients at screening and presurgery safety follow-up, and as clinically indicated. In addition, for all those randomized to Dato-DXd, ophthalmologic assessments will be conducted in the neoadjuvant phase (at cycle 4 and 7). Patients receiving Dato-DXd will be advised to use artificial tears daily and to avoid the use of contact lenses. Prophylactic antiemetic agents will be highly recommended before infusion of Dato-DXd and on subsequent days as needed.
Statistical methods
Efficacy analyses will be performed in the intent-to-treat (ITT) population, defined as all patients who are randomized to study intervention, regardless of the treatment received. The safety analysis set will include all patients who received any amount of study treatment.
Over 2300 patients will be screened to randomize approximately 1700 patients. The study is powered to demonstrate the superiority of neoadjuvant Dato-DXd plus durvalumab followed by durvalumab-based adjuvant therapy versus neoadjuvant pembrolizumab plus chemotherapy followed by pembrolizumab-based adjuvant therapy, as measured by the dual primary endpoints (pCR, EFS) and key secondary endpoint (OS) in the ITT population. A multiple testing procedure for pCR, EFS, and OS endpoints will be implemented to control the type I error (alpha) across tested hypotheses. Group sequential methods will be used to allocate the assigned alpha between the interim and final analyses for EFS and OS.
The difference in pCR rates between the study arms will be assessed using the stratified Miettinen–Nurminen method. 45 EFS, OS, and distant DFS will be assessed using a log-rank test adjusting for stratification factors at randomization. A stratified Cox proportional hazards model will be used to estimate the hazard ratio and associated CIs, and Kaplan–Meier plots will be presented by treatment arm. Safety data will be summarized descriptively.
Discussion
Despite recent advances in treatment, such as the combination of immune checkpoint inhibitors and chemotherapy, there remains a need to improve outcomes and tolerability of treatment for patients with TNBC or HR-low/HER2− breast cancer. TROP2-directed ADCs have emerged as a promising treatment option in this setting, and the combination of these agents with anti-PD-L1 checkpoint inhibitors may increase therapeutic benefits.
The TROPION-Breast04 study will evaluate neoadjuvant Dato-DXd in combination with durvalumab followed by adjuvant durvalumab with or without chemotherapy versus standard of care neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab with or without chemotherapy in patients with previously untreated early-stage TNBC or HR-low/HER2− breast cancer. Enrollment began in November 2023 and the study is ongoing. This study expands on the positive preliminary evidence of the efficacy and safety of Dato-DXd in combination with durvalumab in previously untreated advanced/metastatic TNBC in the BEGONIA study. 40 In the ongoing phase II ISPY2.2 trial, neoadjuvant Dato-DXd in combination with durvalumab has shown promising efficacy in early-stage TNBC, further demonstrating the potential of this combination. 41 TROPION-Breast04 will also provide much-needed information on the treatment of patients with HR-low/HER2− breast cancer, a population that is clinically challenging owing to limited data regarding treatment options. 9 Dato-DXd is also being explored across various indications in TNBC, both with and without durvalumab, in the TROPION-Breast02 (NCT05374512), TROPION-Breast03 (NCT05629585), and TROPION-Breast05 (NCT06103864) studies.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251316176 – Supplemental material for TROPION-Breast04: a randomized phase III study of neoadjuvant datopotamab deruxtecan (Dato-DXd) plus durvalumab followed by adjuvant durvalumab versus standard of care in patients with treatment-naïve early-stage triple negative or HR-low/HER2− breast cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359251316176 for TROPION-Breast04: a randomized phase III study of neoadjuvant datopotamab deruxtecan (Dato-DXd) plus durvalumab followed by adjuvant durvalumab versus standard of care in patients with treatment-naïve early-stage triple negative or HR-low/HER2− breast cancer by Heather L. McArthur, Sara M. Tolaney, Rebecca Dent, Peter Schmid, Jamil Asselah, Qiang Liu, Jane Lowe Meisel, Naoki Niikura, Yeon Hee Park, Gustavo Werutsky, Giampaolo Bianchini, Jay C. Andersen, Robert Kozarski, Nana Rokutanda, Barbara Pistilli and Sibylle Loibl in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Medical writing support for the development of this manuscript, under the direction of the authors, was provided by Ella Spencer and Mark Holland of Ashfield MedComms (Macclesfield, UK), an Inizio company, and was funded by AstraZeneca in accordance with Good Publication Practice (GPP) guidelines (![]() ).
).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.