
Abstract
Gastrointestinal stromal tumours (GISTs) are mesenchymal tumours that originate from the interstitial cells of Cajal. GISTs are mainly driven by gain-of-function mutations in receptor tyrosine kinase or platelet-derived growth factor receptor alpha. Surgical resection is the only curative treatment for localized tumours and all currently approved medical GIST treatments are based on orally available tyrosine kinase inhibitors. Recent discoveries in the molecular and clinical features of GISTs have greatly impacted GIST management. Due to the provincially rather than nationally administered Canadian healthcare system, there have been inconsistencies in the treatment of GISTs across the country. Therefore, guidance on the latest knowledge, clinical management and treatment of GIST is needed to standardize the approach to GIST management nationwide. To establish pan-Canadian guidance, provide up-to-date data and harmonize the clinical practice of GIST management in high- and low-throughput centres across Canada; a panel of 20 physicians with extensive clinical experience in GIST management reviewed relevant literature. This included radiologists, pathologists, interventional radiologists, surgeons and medical oncologists across Canada. The structured literature focused on seven key domains: molecular profiling, radiological techniques/reporting, targeted localized therapy, intricacies of systemic treatments, emerging tests, multidisciplinary care and patient advocacy. This literature review, along with clinical expertise and opinion, was used to develop this concise and clinically relevant consensus paper to harmonize the knowledge and clinical practice on GIST management across Canada. The content presented here will help guide healthcare providers, especially in Canada, in terms of approaching and managing GIST.
Keywords
Introduction
Gastrointestinal stromal tumour (GIST) is the most common malignant mesenchymal tumour of the gastrointestinal tract, with an annual incidence of 11–19.6 per million population. 1 GISTs are mainly driven by gain-of-function mutations in receptor tyrosine kinase (KIT, 75% of cases) or platelet-derived growth factor receptor alpha (PDGFRA, 10% of cases), while these mutations are undetectable in 15% of cases (KIT or PDGFRA wild-type/succinate dehydrogenase (SDH) aberrant).2,3 The pathological diagnosis of GISTs relies on cellular morphology and immunohistochemistry (IHC), where KIT and/or discovered on gastrointestinal tumours-1 (DOG1)/transmembrane protein 16 4 stain positive for these markers in over 90% of cases. GISTs are best identified by computed tomography (CT), but can also be seen on abdominal ultrasound, magnetic resonance imaging (MRI) and positron emission tomography (PET) scan. 5
Chemotherapy and radiation have shown limited efficacy in GIST. 5 Surgical resection is the only curative treatment for localized tumours. 6 Following surgical resection, GISTs often recur locally, spread diffusely throughout the abdominal serosa and/or metastasize to the liver. Distant metastasis occurs in the advanced stages of GISTs. 1 All medical treatments currently approved for GISTs are based on orally available tyrosine kinase inhibitors (TKIs) targeting KIT and PDGFRA oncological activation. 2 Imatinib can be used as neoadjuvant, adjuvant and first-line therapy, achieving prolonged disease control and improving morbidity and mortality. Subsequent lines of TKI therapy (i.e. sunitinib, regorafenib) tend to be less effective, especially with the growing resistance to imatinib.2,5 Novel therapeutic strategies (i.e. ripretinib, avapritinib) focus on overcoming the heterogeneity of secondary mutations and provide more potent inhibition of specific mutations. 2 Other treatment options for metastatic GISTs (mGISTs) include hepatic artery embolization, chemoembolization and radiofrequency ablation (RFA). 3
Recent discoveries in the molecular and clinical features of GISTs have significantly informed the approach to GIST management. Due to the provincially rather than nationally administered Canadian healthcare system, there have been inconsistencies in the treatment of GISTs across the country. 7 This review provides a thorough consensus on the clinical management and treatment of GIST by Canadian GIST experts. Based on the latest research, this consensus report aims to harmonize the latest knowledge, clinical management and treatment of GIST nationwide.
Methods
A panel of 20 physicians across Canada, including radiologists, pathologists, interventional radiologists, surgeons and medical oncologists with extensive clinical experience in GIST management congregated for an open discussion regarding the inconsistencies in the treatment of GIST nationwide. A consensus-based list centred around areas of GIST requiring standardization in Canada was established amongst the experts. The physicians were divided into specialty-based groups where each group was allocated specific sections related to their respective clinical expertise. The physicians within each group collaboratively drafted their sections after reviewing relevant literature as well as discussing their clinical expertise and opinions amongst one another. The structured literature focused on seven key domains: molecular profiling, radiological techniques/reporting, targeted localized therapy, intricacies of systemic treatments, emerging tests, multidisciplinary care and patient advocacy. A complete draft of the paper was then disseminated amongst the 20 physicians for two rounds of extensive review and comments. After the comments were discussed, they were incorporated into the paper and re-disseminated amongst the experts. The physicians then provided a formal statement indicating their agreement with the contents of the paper, thus further establishing consensus.
Histopathology of GISTs
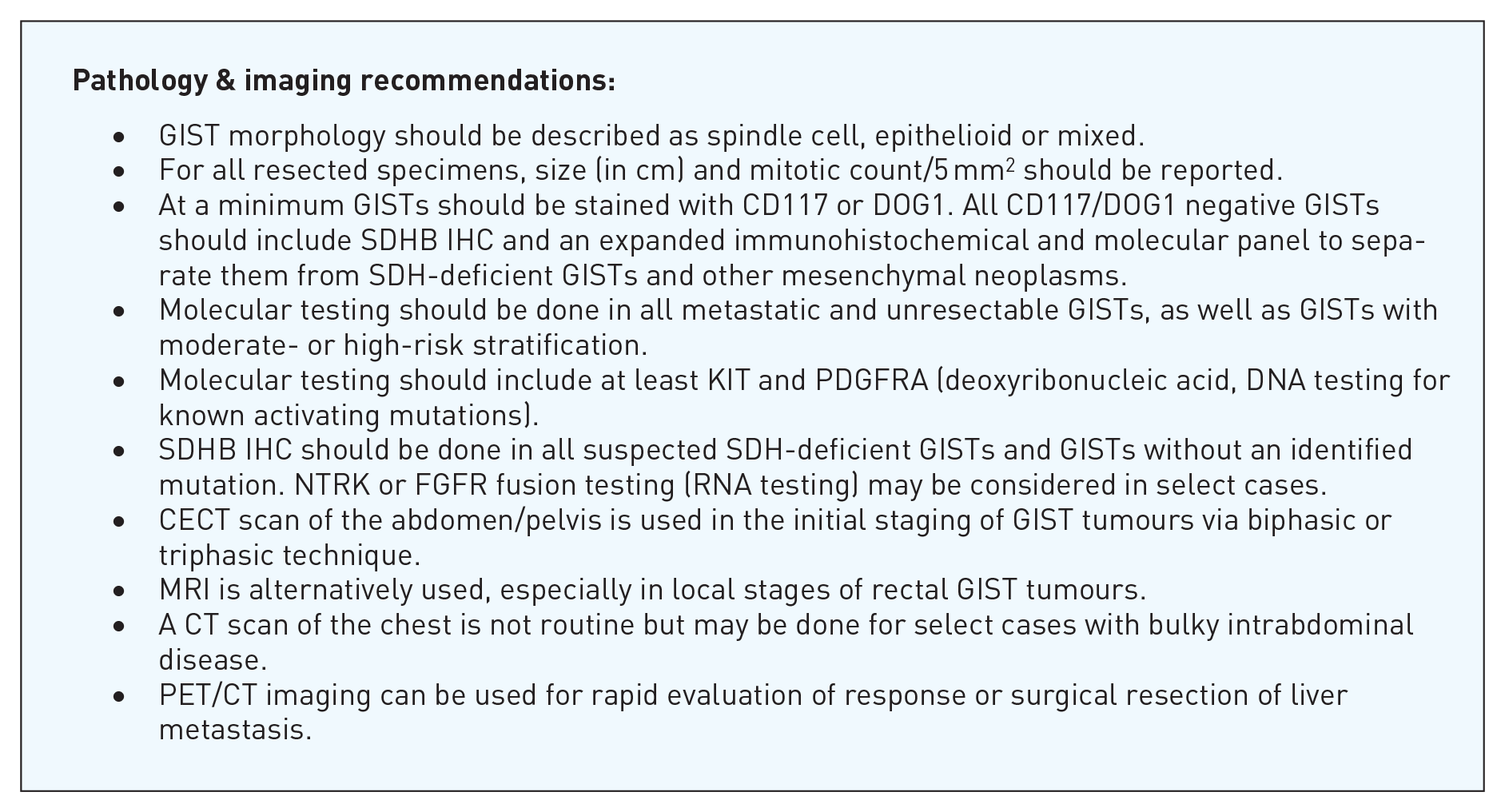
GISTs are mesenchymal tumours that arise from the interstitial cells of Cajal. They can arise anywhere in the gastrointestinal tract and demonstrate a wide range of morphologic appearances. 8 The morphology should be described as spindle-cell, epithelioid or mixed. SDH-deficient GISTs typically occur in younger patients and may have a distinct morphological appearance (multinodular with plexiform mural invasion) and behaviour (lymphatic metastasis). 9 A total of 5%–10% of GISTs can occur in association with hereditary syndromes (most commonly SDH-deficient GISTs) and the examination of resected specimens should include a review for hyperplasia or nodularity involving the interstitial cells of Cajal in areas separate from the tumour.10,11 The behaviour of GISTs is best determined using risk stratification based on mitotic activity, tumour size and anatomic location (Table 1). 12 Mitotic count is conducted over an area of 5 mm2; while historically described as mitotic count per 50 high-power fields (hpf), this corresponds to 20–25 hpf (40× objectives) for modern microscopes. 13
Risk stratification of GISTs by mitotic count, size and location. 12

Source: Adapted from Demetri et al. 12
While there is insufficient evidence to properly risk stratify GISTs arising from the duodenum or rectum, these tumours behave more aggressively and are best stratified similarly to GISTs arising from the ileum or jejunum.
GIST, gastrointestinal stromal tumour.
Diagnosis and classification of GISTs
Pathological diagnosis and molecular testing of GISTs
IHC plays a key role in the diagnosis of GISTs. The vast majority of GISTs stain positively for KIT (CD117, 90%–95%) and DOG1 (95%–97%). Positivity can be seen with CD34, caldesmon and smooth muscle actin (SMA) with rare tumours showing positivity for desmin, S100 or keratin. As CD117 and DOG1 IHC staining are not specific, a panel of immunohistochemical stains is recommended to exclude other CD117-positive tumours (i.e. malignant melanoma, some sarcomas).14,15 SDHB IHC should be performed in cases where SDH-deficient GISTs are suspected and GISTs in which driver mutations are not found. SDH-deficient GISTs lose expression of SDHB protein, irrespective of which SDH subunit is mutated, as a result, SDHB IHC alone is sufficient for SDH-deficient GISTs. 16
Molecular testing should be done on all GISTs in which therapy is being considered (all metastatic, unresectable GISTs and GISTs with moderate- or high-risk stratification). As there are a number of potential drivers and molecular changes can include mutations, insertions, deletions and duplications, a wide panel is recommended over targeted sequencing.
Approximately 75% of GISTs have mutations in KIT (most commonly in exon 11 or 9; rare mutations can be found in exons 13 and 17), and about 10% have mutations in PDGFRA (exon 18 with rare mutations in exons 12 and 14). 17 The most common findings in KIT/PDGFRA wild-type GISTs are alterations in the SDH genes (either mutations or promoter methylation) with rare mutations identified in Neurofibromatosis 1 (NF1), V-Raf Murine Sarcoma Viral Oncogene Homolog B (BRAF) or Kirsten Rat Sarcoma. Neurotropic Receptor Tyrosine Kinase 3 (NTRK3) or Fibroblast Growth Factor Receptor 1 (FGFR1) fusions (ribonucleic acid testing (RNA)) are very rare in GISTs, and testing may be considered in select clinical situations to separate GISTs from other mesenchymal neoplasms and to direct therapy.2,18–21
Imaging techniques for tumour staging
Contrast-enhanced CT scan (CECT) forms the backbone of GIST tumour imaging with other modalities used when there is a contraindication to CECT or in specific locations/circumstances. In the staging setting, the upper abdomen should be covered optimally by a biphasic (arterial and venous) or triphasic technique (pre-contrast, arterial and venous) to assess the primary tumour and any liver lesions, incidental or otherwise. Oral contrast may be omitted, or water can be used. For follow-up of tumours and surveillance imaging, a single venous phase scan with positive oral contrast or a biphasic CT (both strategies to improve detection of peritoneal disease) is recommended. 22
A CECT scan of the abdomen and pelvis is recommended in the initial staging of GIST tumours. MRI may be used as an alternative modality especially in the local staging of rectal GIST tumours. Chest imaging may be performed with a plain radiograph of the chest or CT scan. CT scan of the chest may be reserved for patients with bulky intra-abdominal disease. 23 PET or PET/CT imaging is not a necessity but, because of its high sensitivity to viable tumour, can be used in special circumstances such as where rapid evaluation of response is necessary or surgical resection of liver metastases is considered. 24
Surgical treatment of GISTs
Surgical resection of non-metastatic GISTs
The goal of surgical therapy for primary resectable, non-metastatic GISTs is complete resection with microscopic and macroscopic negative margins (R0 resection).25,26 Active surveillance may be considered for GISTs < 2 cm in the stomach, due to the very indolent behaviours of these tumours.26,27 Conversely, European Society of Medical Oncology (ESMO) guidelines suggest all GISTs, even gastric GISTs < 2 cm should be resected if acceptable morbidity, with active surveillance suggested as a possible alternative. 24 However, active surveillance as the primary approach may be more appropriate due to the indolent behaviour of these tumours.26,27 Patients with extensive comorbidities that would preclude their ability to tolerate a general anaesthetic and surgical resection as well as those with technically inoperable disease (e.g. infiltration of great mesenteric vessels) are not surgical candidates. Neoadjuvant imatinib may be recommended for GIST cytoreduction to avoid highly morbid surgeries.
Resections may be segmental if negative margins are feasible; anatomical resections (e.g. total gastrectomy) are not mandated unless necessary due to tumour size/location. Enucleation is contraindicated, however. Multivisceral resections may be necessary. Lymph node involvement is rare in GISTs, and lymph node resection is not indicated. Endoscopic, laparoscopic and robotic approaches may be considered in appropriately selected patients if the appropriate oncologic approach is taken with respect to margins and tumour rupture.
The association of R1 margins with reduced survival is controversial. Microscopic positive margins may not have a negative effect on overall survival (OS) or relapse-free survival (RFS).25,28,29 Adjuvant imatinib may obviate any potential negative effects (section ‘Adjuvant therapy post-surgical resection’). 30 The exception may be rectal GISTs, where positive margins are associated with poor outcomes and reduced survival. 31
Tumour rupture is associated with poor outcomes following surgery for GISTs and therefore great care must be taken to avoid iatrogenic intra-operative rupture.25,32 Occasionally, tumour rupture occurs prior to surgery. Tumour rupture does not include minimal damage of the lesion surface without spillage, including those associated with needle biopsy without complication.32,33

Medical therapy for localized GIST
Considerations for neoadjuvant therapy
Neoadjuvant therapy may be considered in patients where there may be increased risk or morbidity with upfront resection or clinical suspicion of multi-organ involvement. 34 Increased risk may be secondary to location, where cytoreduction may lead to organ and/or sphincter preservation. 26 Risk may be related to the feasibility of negative margin resection, 25 especially in larger tumours or those with specific anatomic considerations including rectal GISTs.26,31 Furthermore, the increased risk may be related to the potential for tumour rupture in large, friable tumours that might be mitigated by pre-treatment with a TKI.
In cases of neoadjuvant therapy, it is critical to obtain mutational analysis prior to initiating treatment. 35 One important consideration is that risk stratification after surgery may be affected by neoadjuvant therapy including reduced size or mitotic rate, but generally, 3 years of treatment with imatinib is advocated. 24
Adjuvant therapy post-surgical resection
Adjuvant therapy should be considered for those with resected GIST based on recurrence risk and tumour molecular genotyping. Several prognostic nomograms have been developed to assess the risk of recurrence post-surgery. These are typically based on tumour size, mitotic index and primary tumour location. The most used nomograms include the Armed Forces Institute of Pathology prognostic model 17 as well as the Memorial Sloan Kettering Cancer Center nomogram. 36 Other clinical variables observed to be poor prognostic factors include tumour rupture and incomplete surgical resection. Although eligibility for reported adjuvant trials did not include tumour molecular subtyping, results if available are commonly considered in recommending adjuvant therapy. There is a lack of consensus between ESMO and the National Comprehensive Cancer Network (NCCN) in recommending adjuvant therapy for those with wild-type tumours or patients with mutations in PDGFRA. NCCN does not exclude patients for adjuvant imatinib therapy based on the presence of specific mutations 27 although the ESMO guidelines specifically PDGFRA-D842V-mutated GISTs should not be treated with any adjuvant therapy given their lack of in vitro and in vivo resistance to imatinib. 24 Adjuvant therapy is not recommended for patients with wild-type (no KIT or imatinib sensitive PDGFRA mutation) GIST. Even if a molecular driver with a targeted therapy available is identified, there is a paucity of evidence to recommend use of such an agent in the adjuvant setting.
Three major randomized phase III studies have demonstrated the benefit of adjuvant imatinib post-surgery. American College of Surgeons Oncology Group Alliance study (ACOSOG Z9001) 28 was a double-blind, randomized study of 713 patients with resected tumours at least 3 cm in size. Accrual was stopped early as the interim results significantly prolonged RFS for those on imatinib (98% vs 83% at 1 year, hazard ratio (HR) = 0.35, p < 0.0001). Based on these results, adjuvant imatinib was given accelerated Food and Drug Administration (FDA) approval in 2008. The Scandinavian Sarcoma Group (SSG) XVIII trial 37 was an open-label trial comparing 36 versus 12 months of adjuvant imatinib (400 mg daily) in 400 patients with high-risk resected GIST as defined by at least one of the following criteria: tumour > 10 cm, mitotic figure count > 10 per 50 hpf, tumour size > 5 cm and mitotic count > 5, or tumour rupture. After a median follow-up of 54 months, 3 years of therapy was associated with a significant improvement in RFS (the primary endpoint, 5-year RFS 66% versus 48%, HR 0.46, 95% CI 0.32–0.65). In addition, OS favoured the 3-year group (5-year OS 92% versus 82%, HR 0.45, 95% CI 0.22–0.89). With longer follow-up, 3 years of adjuvant imatinib led to a reduction in the number of deaths by approximately half during the first 10 years of follow-up after surgery. European Organization and Treatment of Cancer (EORTC 62024) 38 was an open-label multicentre phase III trial that randomized 908 patients with intermediate- or high-risk resected GIST to observation or 2 years of adjuvant imatinib. Risk was defined by the 2002 National Institutes of Health criteria and also included those with R0 and R1 resections. 39 OS was the initial primary endpoint which was modified to Imatinib Failure Free Survival. Patients treated with adjuvant imatinib had longer RFS, but no significant survival benefit was observed with a median follow-up of 4.7 years. In those with intermediate- or high-risk disease, there was only one patient with imatinib-sensitive mutations that had a recurrence, but which occurred after discontinuation therapy. However, half of the patients discontinued treatment early due to patient choice. There is no high-level data to recommend more than 3 years of adjuvant imatinib. However, long-term adjuvant imatinib therapy can be discussed in select cases (i.e. tumour rupture). 40

Medical management of advanced GIST
First-line medical treatment
The landscape of treating advanced GISTs has significantly evolved in the past two decades, thanks to our understanding of the genetic mutations underlying these tumours. Initial management begins with tumour genotyping which is highly recommended to guide treatment decisions. 42 However, for a majority of patients with advanced, unresectable or mGISTs, as well as those who have experienced relapse following adjuvant imatinib therapy, the standard first-line therapy is imatinib at a daily dose of 400 mg.
Imatinib, a TKI, has been a ground-breaking advancement in GIST treatment. It targets KIT (CD117), which is mutated and activated in the majority of GISTs. Imatinib’s effectiveness is evident in the expected median progression-free survival (mPFS) of 24 months, with an impressive 53.7% of patients achieving a partial response.43,44 This level of success has made imatinib the cornerstone of GIST therapy for more than two decades.
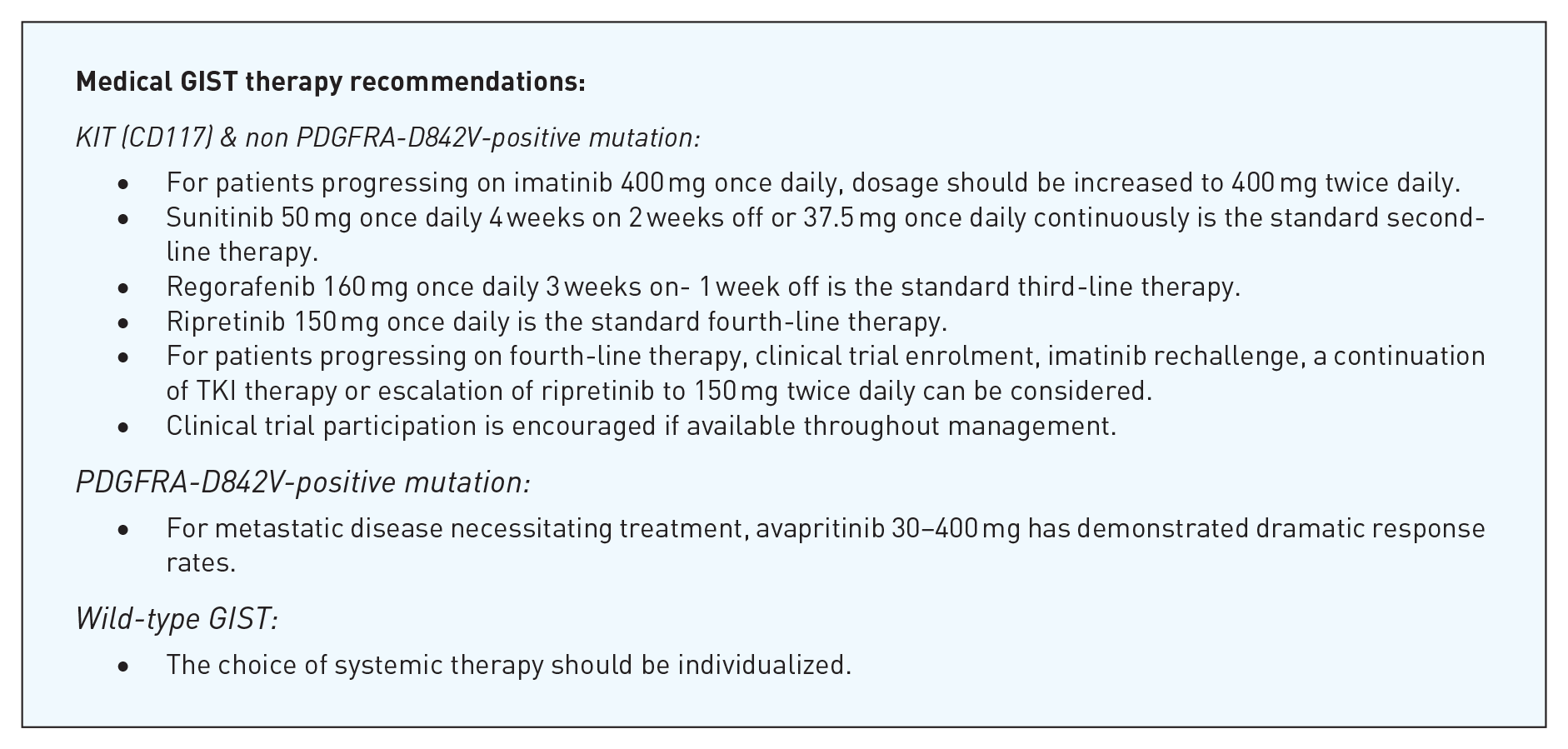
Recent research has shed light on the complexity of GIST management, particularly in patients with specific mutations. Studies comparing daily dosing to a twice-daily schedule have revealed intriguing insights, especially in patients harbouring a KIT exon nine mutations. 45 This subgroup exhibits a higher response rate and extended PFS with the twice-daily approach. While no OS benefit has been observed, certain expert groups now recommend initiating treatment with 400 mg twice daily for these specific patients. Furthermore, for those with the KIT exon nine mutation who experience disease progression on 400 mg daily, increasing the dose to 400 mg twice daily has shown benefits, albeit with a higher incidence of toxicity. Given these observations, a prudent approach may be to commence treatment with 400 mg daily for patients with KIT exon nine mutations, with dose escalation to twice daily considered in cases of progression or patients tolerating imatinib with no significant toxicity.
Remarkably, up to 10% of patients with mGIST treated with imatinib can have long-term durable response and disease stability. 46 However, the question of whether therapy can be safely discontinued for this subset remains unanswered. Consequently, it is advisable to continue therapy indefinitely for these patients until further evidence emerges, as the safety of long-term duration of imatinib therapy did not demonstrate new reports of toxicity or adverse events in SWOGS003 and extended B2222 studies.
Mutation-related imatinib resistance
Approximately 10%–15% of GIST patients are inherently resistant to imatinib therapy, making genotyping an indispensable initial assessment (Tables 2 and 3). 42 In specific situations, an initial period of observation may be warranted before initiating a treatment. Certain types of wild-type GISTs associated with NF1 or SDH deficiency in addition to PDGFRA-D842V GISTs can initially present with a more indolent course of disease. Therefore, active surveillance may be preferred as the initial approach. Patients with known primary imatinib-resistant mutations should be offered alternative therapies known to be active for their specific mutation.
Wild-type GIST molecular sub-groupings and treatment.
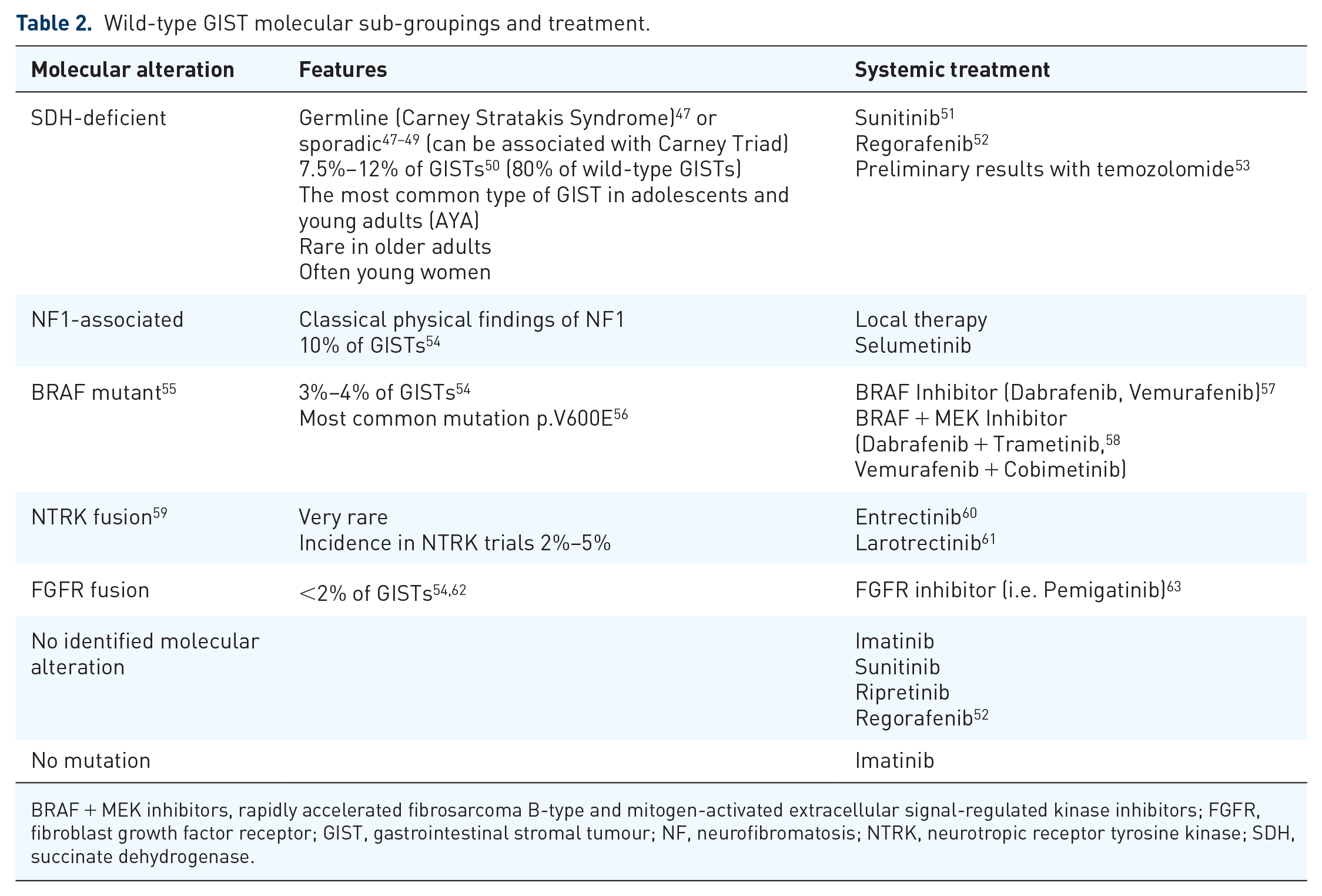
BRAF + MEK inhibitors, rapidly accelerated fibrosarcoma B-type and mitogen-activated extracellular signal-regulated kinase inhibitors; FGFR, fibroblast growth factor receptor; GIST, gastrointestinal stromal tumour; NF, neurofibromatosis; NTRK, neurotropic receptor tyrosine kinase; SDH, succinate dehydrogenase.
Preferred first-line GIST treatment based on mutation.

GIST, gastrointestinal stromal tumour; PDGFRA, platelet-derived growth factor receptor alpha.
Wild-type GIST
A small proportion, 10%–15%, of GISTs do not have a molecular alteration in KIT and PDGFRA, and this group is defined as ‘wild-type GIST’. Comprehensive next-generation sequencing (NGS), including BRAF, NTRK, FGFR, SDH, NF1, is strongly recommended for such tumours. With improved molecular testing, it has become clear that these GISTs are heterogeneous and defined by rare molecular drivers (Table 2). The majority of wild-type GISTs are SDH deficient (up to 80% in some published series). 64 While SDHB loss can be demonstrated by IHC, NGS is required to determine the exact mechanism and subunit responsible for SDH deficiency.
Irrespective of their specific molecular driver, it is well accepted that wild-type GISTs follow a different treatment paradigm than KIT/PDGFRA mutant GISTs.
The treatment of wild-type GISTs is often driven by the biology of the disease given that limited effective systemic options exist for this heterogeneous subtype. For asymptomatic patients with proven indolent disease biology (i.e. NF1-associated GIST), surveillance can be employed. Treatment is reserved for symptomatic disease and/or metastasis near critical sites. For oligometastatic disease, local therapy (i.e. ablation, surgery, radiation) remains a cornerstone of management due to the limited effective systemic treatments for this subtype. For patients with disease not amenable to local therapy, systemic therapy for each subtype is summarized (Table 2).
PDGFRA-D842V
While not specifically defined as wild type, GISTs with PDGFRA-D842V mutations are well established to be imatinib resistant. 65 There is no role for adjuvant therapy in GISTs with D842V mutations. For patients with unresectable or metastatic disease, surveillance can be considered due to the often indolent biology of this subtype. For patients with metastatic disease necessitating treatment, avapritinib has demonstrated dramatic response rates (100% partial response by Choi criteria) across all dose levels tested (30–400 mg). 66 It has been recommended in both advanced and neoadjuvant settings by NCCN. However, access to avapritinib remains challenging internationally, despite its FDA approval on January 9, 2020.
Alternate lines of TKI therapy upon progression on imatinib
Despite the initial promise of imatinib therapy, approximately 50% of patients are expected to develop secondary resistance to this agent within the first 24 months of treatment. For patients who fall outside the scope of KIT exon nine mutations, increasing the imatinib dose to 400 mg twice daily offers limited benefit. 67 In such cases, transitioning to an alternative therapeutic approach is recommended (Table 3), with sunitinib emerging as the preferred choice.
Sunitinib, another TKI, targets KIT and PDGFRA, offering a different mechanism of action compared to imatinib. It boasts an objective response rate (ORR) of nearly 10% and a mPFS of 6 months. 68 The standard dosing regimen involves 50 mg once a day on an intermittent schedule of 4 weeks followed by 2 weeks off. Subsequently, continuous daily dosing of sunitinib at 37.5 mg daily has shown comparable activity with improved tolerance, making it a valid alternative. 46
For patients who progress on sunitinib, regorafenib emerges as the next standard of treatment. This oral multikinase inhibitor, with activity against KIT and PDGFRA, has demonstrated a mPFS of 4.8 months and an ORR of 4.5% at a dosing of 160 mg daily, following a schedule of 3 weeks on and 1 week off. 69
However, for patients who have exhausted three lines of therapy and are faced with the challenge of fourth-line treatment, ripretinib has emerged as the standard fourth-line therapy. Ripretinib, a novel oral TKI, has become the new standard of care in this setting. Administered at a daily dose of 150 mg, ripretinib offers an mPFS of 6.3 months and an ORR of 9.4%. 70 These encouraging outcomes offer renewed prospects for patients who have faced numerous treatment regimens.
Notably, the three aforementioned TKIs exhibit varying degrees of activity against secondary resistant mutations. Selecting subsequent lines of therapy based on the identification of these acquired mutations through tissue biopsy or liquid biopsy remains an experimental but promising avenue (section ‘The emerging role of liquid biopsy in GISTs’).
Progression in fourth-line therapy
In the case of progression of mGISTs after multiple lines of TKI therapy, patients should be considered for participation in clinical trials of new therapies or combinations. There is prospective evidence that patients who have already progressed on imatinib may benefit when rechallenged with the same drug. 71 Likewise, there is evidence that patients who continued treatment with a TKI despite progression continue to have a better quality of life than patients who stopped altogether.
In a follow-up analysis of INVICTUS, dose escalation of ripretinib to 150 mg twice daily was evaluated in 43 patients who experienced disease progression while on ripretinib at 150 mg daily (Blay et al. 70 – This study demonstrated the significantly longer PFS of ripretinib after three-line TKIs, leading to the FDA approval of ripretinib as the fourth-line therapy for advanced GIST). The median overall survival (mOS) was 18.4 months for patients who switched to ripretinib at 150 mg twice daily, compared with 14.2 months for patients from INVICTUS who experienced disease progression but did not undergo dose escalation. The mPFS after receiving the first dose of 150 mg twice daily was 3.7 months. Dose escalation of ripretinib to 150 mg twice daily may be an option for patients who experience disease progression while on ripretinib at 150 mg daily. A summary of the patient treatment pathway is summarized in Figure 1.

Treatment pathways of GIST patients.
Management of TKI-related adverse events and dose modifications
Because TKIs are administered for prolonged periods of time in patients with GISTs, proper management of TKI-associated side effects is important. Since most adverse events (AEs) are mild-to-moderate, clinicians should always try not to reduce or stop the TKI and focus on other options to treat and reduce the incidence of AEs. In severe cases, dose interruption is usually the first line of treatment (with pharmacological and non-pharmacological interventions). Rechallenge with the same dosage should usually be done depending on the gravity of the AEs. Dose reduction is the last option and should be reserved for severe AEs or AEs recurring despite other measures and impacting the patient’s quality of life. Most TKI-related AEs improve with ongoing duration of treatment.
Gastrointestinal toxicity
Mucositis and stomatitis are reported mainly with sunitinib and regorafenib in 15%–38% of cases.68,69 Mild-to-moderate cases can usually be managed with oral hygiene, mouth rinses (with or without analgesic), systemic analgesics and avoidance of irritating food. 72
Nausea is a common (16%–54%) side effect reported with all TKIs. Vomiting is reported in 13%–18% of cases with fewer than 1% being grade 3–4 in both cases.68–70,73,74 A few non-pharmacological options can help patients reduce the incidence of nausea such as taking the medication at bedtime, splitting the dose into two times a day (BID, imatinib) and taking the drug with food. 75 In cases in which symptoms are still present, anti-nausea medication such as ondansetron, olanzapine and prochlorperazine can be used. 76
Diarrhoea is also very common (20%–50%) but with very few grades 3–4 (1%–5%).68–70,73,74 Dietary change with the use of loperamide should be tried first. Other agents that could be used in more severe cases are narcotics, octreotide, and atropine sulphate/diphenoxylate hydrochloride. 77
Fatigue
Fatigue is common (29%–39%),68–70,73,74 and patients should receive education, physical and nutritional interventions to reduce other sources of fatigue. Cancer Care Ontario guidelines are a useful tool for clinicians. 78
Fluid retention
Fluid retention with peripheral oedema, especially periorbital oedema, is among the most common side effects of imatinib. 79 Often most prominent in the morning, it often decreases during the day with an upright posture. In severe cases, pleural effusion and ascites may occur, especially in those with pre-existing cardiac disease. Management includes dietary salt restriction, while diuretics are of limited value. Severe cases are managed with dose interruptions, often with resumption at lower starting doses.
Cutaneous toxicity
Imatinib-related skin rash is usually mild, maculopapular and sometimes pruritic. 80 Severe cases often necessitate temporary drug discontinuation and a short course of oral glucocorticoids.
Hand-foot syndrome (HFS) is a common side effect of both sunitinib and regorafenib.80,81 Often painful, severe HFS can have a significant impact on patients’ quality of life. As such prophylactic management should include aggressive use of emollients containing urea, avoidance of skin irritants and softening/removal of hyperkeratotic skin prior to initiation of treatment. Treatment often requires temporary drug discontinuation if severe. Seek dermatological consultation for severe persistent symptoms.
Ripretinib is associated with the development of skin malignancies (including squamous cell carcinoma and melanoma), and as such, regular skin surveillance while on treatment is necessary. 82
Musculoskeletal toxicity
Myalgias and muscle cramps are common (up to 40% of patients) with imatinib treatment, often involving lower extremities and hands. 83 Anecdotal treatments include calcium and magnesium supplementation (including pickle juice), in addition to quinine (tonic water).
Cardiotoxicity
Although several retrospective studies have suggested a risk of heart failure associated with imatinib use, prospective studies have suggested the risk is very low or negligible in those without an antecedent history of heart disease. 84 Both ripretinib and sunitinib have been associated with a modest decline in ejection fraction (EF).85,86
Treatment-related hypertension is commonly seen with sunitinib and regorafenib. The American Heart Association (AHA) has published guidelines on the diagnosis and management of cancer therapy-related hypertension. 87 Patients with severe treatment-related cardiotoxicity (including hypertension) should be referred to cardio-oncology services where available.
Invasive treatment options available for mGISTs
The cornerstone of treatment for metastatic disease is systemic therapy; however, in select patients with low-volume disease, limited progression and otherwise well controlled systemic treatments, locoregional treatments such as metastasectomy, stereotactic body radiation therapy and/or other ablative procedures could be considered.88–90 Metastases are most commonly in the liver and/or peritoneal cavity. 27
Locoregional therapies
Locoregional therapies provided by interventional radiology (IR) to treat GISTs include thermal ablation and catheter-directed therapies.24,27,91 These may be indicated in hepatic metastatic disease with the treatment goal of no active disease (NAD) or to prolong survival in non-operative candidates.24,27 IR-guided treatment of primary hepatic GISTs has been reported but limited data exist and it should be reserved for non-operative candidates or palliation. 92
Image-guided ablation includes RFA, microwave ablation (MWA) and cryoablation; these techniques can be performed percutaneously or at the time of surgery. Most ablation data in GISTs are for RFA, likely given its longer track record versus MWA and cryoablation, and it can be used for treatment towards NAD, to prolong survival in oligometastatic disease and oligoprogressive disease, or for tumour debulking.93–97 However, compared to surgical resection for hepatic metastases, RFA has shorter PFS. 93 Ablation may be considered for oligoprogressive disease on a background of stable hepatic metastases following a multidisciplinary review. Intra-operative ablation may be performed in conjunction with surgical resection of metastases. 98 Complications related to RFA for hepatic GIST metastases include post-ablation syndrome, haemorrhage or tract seeding. 96 Limited data exist on the treatment of GISTs with other ablation techniques, but the principles of thermal ablation apply.99,100 Lesion size considerations and thermal ablation technique should be determined based on local expertise, but generally lesions <4.0 cm may be amenable to ablation.93,95,97,101 In summary, following multidisciplinary treatment planning, ablation may be used in a treatment plan towards NAD, treatment of oligoprogressive disease for prolonged survival or for palliative debulking.
Catheter-directed therapies include bland transarterial embolization (TAE), transarterial conventional chemoembolization (TACE), drug-eluting-bead transarterial chemoembolization (DEB-TACE) and transarterial radioembolization (TARE). These therapies can be applied to metastatic disease for prolonged survival, with the intent of downgrading/NAD in conjunction with surgery, or palliation.102–104 Conventional TACE and TAE are safe and effective, resulting in tumour response in hepatic metastatic disease for patients receiving TKIs.102–105 Similarly, with progressive imatinib-resistant hepatic metastatic disease, TACE or TARE may be provided as a salvage.106,107 The AEs in embolotherapy include post-embolization syndrome, hepatic abscess and liver failure.105,106 In summary, catheter-directed therapies may be indicated to treat hepatic metastases in patients with progressive disease or for whom operative management is not a consideration, with the goal of NAD in conjunction with surgery or to prolong survival. Selection of embolic agent should be based on local expertise and availability.
Palliative treatments are dependent on individual patient presentation. Both ablative and catheter-directed therapies may be offered to debulk metastatic or primary tumour burden, as described above. In the setting of acute haemorrhage, TAE has been shown to be safe and effective. 108 Gastrointestinal stenting may be considered if tumour bulk leads to obstruction. 109
Metastasectomy
Metastasectomy is generally reserved until after treatment with TKI with the goal of resection of residual metastatic disease. 24 Lack of response to TKI is associated with poor outcomes.88,110 Patients undergoing metastasectomy with complete resection (R0/R1) have better outcomes than patients with gross residual disease. 88 Consideration of metastasectomy may be given when there is limited, focal progression while systemic therapy and resection would have acceptable morbidity.24,111 Patients being considered for surgical resection in the metastatic setting need to be reviewed in multidisciplinary teams at expert centres (section ‘Multidisciplinary approach to GIST management’). 89
Monitoring for treatment response and relapse
Treatment responses in GISTs are significantly different from conventional chemotherapy.112,113 On CECT, responding lesions may display a decrease in density, including near-cystic attenuation, with little or no change in size, reflecting the histopathological changes of cellular depletion and myxoid degeneration. Some lesions may even increase in size with a change in density which occurs due to intratumoural haemorrhage. Therefore, for both CT and MRI, a decrease in the degree of tumour enhancement without a decrease in size may be counted as a response, particularly early in the treatment course. MRI responses in GIST treatment also involve increased signal on T2-weighted images with decreased enhancement, while diffusion-weighted imaging with apparent diffusion coefficient (ADC) maps aid early response detection. 114
Accurate early detection of relapse in GISTs is critical to adjust therapy.115,116 It most commonly occurs in the liver or peritoneal cavity. Relapse may manifest with new lesions. In the subset of patients with residual cystic metastases, recurrence is detected when treated cystic lesions enlarge or demonstrate the ‘nodule within a cyst’ pattern of progression. 117 MRI plays a crucial role in the early accurate characterization of suspicious lesions on CT, providing superior soft-tissue resolution and dynamic enhancement characteristics. This means that detection of new vascularized tumour within previously cystic/necrotic tumour may be more facile by MRI than CT scan.
PET effectively detects therapy response within 24 h of initiating imatinib, correlating with prognosis. PET can differentiate treatment-related CT changes, such as increased lesion size, from true progression based on the absence of metabolic activity. 118
Frequency of imaging
Neo-adjuvant setting
Imaging may be performed every 3 months until disease stability is achieved.
Adjuvant/metastatic disease/R2 resection
Imaging should be performed every 3–6 months, with 6-month interval especially encouraged when R0 resection has been achieved or disease remains stable. For very low-risk (<2 cm) GIST tumours that are not resected, an initial follow-up scan at 3 months, followed by increasing intervals between scans to reach annual frequency. 24 Some very low-risk tumours may be visible sonographically and therefore ultrasound may be used to monitor tumour size.
Surveillance
For intermediate- and high-risk GISTs, the risk of recurrence is highest closest to the cessation of adjuvant therapy but diminishes thereafter, allowing for titration of imaging frequency. 119 We recommend a schedule based on a decreasing frequency of surveillance, such as guidelines proposed by Alessandrino et al. with a CT scan every 3 months for year 1, every 6 months for years 2–3 and every 6–12 months for years 4–10. 22 For low-risk GISTs, decreased frequency and duration of surveillance are recommended, for example, every 6 months for 5 years. For treated very low-risk GIST, surveillance may not be required or at most one CT at 1-year post-resection.
The emerging role of liquid biopsy in GISTs
The liquid-based (mainly from blood) testing of plasma-derived circulating tumour DNA (ctDNA) has been increasingly recognized in the field of oncology as an important ancillary and/or alternative clinical tool especially when solid tissue biopsy is insufficient or unattainable. It has several additional advantages over tissue biopsy including avoiding invasive procedures and shorter turn-around times, thereby improving clinical utility and efficacy. It has been explored for real-time monitoring of response to treatment and proven beneficial in not only identifying potential actionable predictive but more importantly emerging resistant biomarker(s).120,121 When compared to tissue biopsy, a liquid biopsy of ctDNA testing is better able to capture tumour heterogeneity both spatially and temporally, thereby guiding the management of various cancers including mGIST.122–125
Another important area of application of liquid-based ctDNA testing is the detection of postsurgical minimal residual disease (MRD) which refers to ctDNA positivity without radiographic evidence of disease.126,127 MRD has been proven to be the strongest prognostic predictor of disease recurrence compared with other established clinicopathological risk factors and its validity in guiding adjuvant treatment is emerging and actively being investigated in clinical trials of many cancer types, with resected colon cancer being the leader in this field. 128 One notable limitation of this technology is that there is variable ctDNA shedding in certain tumours based on tumour type, stage and disease activity.126,127 Localized GISTs are prone to release technically undetectable ctDNA fractions; therefore, the role of ctDNA for early detection of tumour relapse after GIST surgery and/or adjuvant imatinib has yet to be determined. 125 Ultimately, the use of liquid biopsy in terms of assessing treatment and MRD in GIST is considered experimental; thus, its role is yet to be determined.
Multidisciplinary approach to GIST management
The optimal management of mGISTs requires a multidisciplinary approach. Concentrating GIST management in specialized high-volume centres is imperative due to the rare and unique characteristics of these tumours. Specialized centres can offer a pool of experienced oncologists, surgeons, radiologists and pathologists who possess a deep understanding of the intricacies involved in treating mGISTs. They allow seamless teamwork among these experts, ensuring that patients receive comprehensive and personalized treatment that not only enhances the overall quality of care but also fosters ongoing research and innovation, contributing to the development of more effective treatment strategies.
The apparent simplicity of administering oral TKIs such as imatinib, and their efficacy in the first-line setting might lead to the perception that GIST management is straightforward. Consequently, many patients are treated at less specialized or less experienced centres where adequate molecular biomarker testing may not be performed, and available treatments may not be used optimally due to inaccurate determination of disease progression or inadequate management of treatment toxicity. Moreover, patients who are not treated at or linked with specialized centres may not be considered for surgery or ablative therapy at primary or metastatic disease sites – interventions that have been shown in several retrospective studies to be associated with prolonged OS.88,90 They may also miss opportunities to be enrolled in clinical trials. In a real-world study, of mGIST patients treated at three specialized high-volume sarcoma centres in France, nearly half of the patients were enrolled in trials and/or received metastasis-directed therapy with a mOS of approximately 7 years. 89 In comparison, long-term follow-up of patients treated in the first-line setting reported mOS of 3.9 years. 46

Patient advocacy of GISTs in Canada
The introduction of targeted therapy for GISTs has coincided with the widespread use of email and the Internet. GIST patients and caregivers quickly developed online platforms for the dissemination of news (i.e. the availability of clinical trial sites) and mutual support. The pace of clinical trials accelerated – and, without a doubt, lives were saved – as a result.
Canada’s vast geography and the fragmented nature of the Canadian healthcare system (managed separately by 10 provinces, three territories and multiple federal bureaucracies) present several challenges to GIST cancer patients. For example, a drug may be approved for provincial funding in one province but not in another. Many provinces provide out-of-hospital cancer drug benefits, but others still do not. Mutational testing has been implemented only in a stepwise fashion. Radiology tools such as PET scanning are not always accessible in every region.
GIST Sarcoma Life Raft Group Canada (LRGC) was formed as a not-for-profit corporation in 2008 and received charitable status. The Canadian group cooperates closely with parallel organizations in the United States, Europe and other countries. LRGC provides a ‘virtual home’ where Canadian GIST patients can find emotional support from their peers and learn more about how to live with GISTs. Ongoing activities of the group include the following: holding in-person and virtual gatherings, including an annual ‘GIST Day of Learning’; maintaining a website; funding GIST research at Canadian universities and hospitals; submitting input to the Canadian Agency for Drugs and Technologies in Health, when public reimbursement of GIST drugs is under consideration; providing pertinent information to regulators and administrators; and, perhaps most importantly, acting as a forum where persons living with GIST can interact with and support one another.
Conclusion
The provincial-led nature of the Canadian healthcare system has resulted in inconsistencies in GIST management. The consensus recommendations in this paper are based on literature review, clinical expertise and opinions, to establish a more standardized approach.
It is recommended that GISTs be stained with CD117 or DOG-1, and molecular testing be done for unresectable mGISTs and GISTs with moderate- or high-risk stratification. CECT remains the backbone of GIST imaging for staging, follow-up and surveillance. 22
In primary resectable, non-metastatic GISTs, complete surgical resection is required.25,26 Neoadjuvant therapy is considered when there is an increased risk of morbidity with upfront resection or multi-organ involvement. 34 Adjuvant therapy is recommended for those with intermediate- to high-risk resected GISTs.38,40
Tumour genotyping prior to initial medical management is advised to guide therapy. 42 While imatinib is the first-line therapy in most patients, 10%–15% are imatinib resistant, and their options for systemic treatment are summarized in Table 2. 46
Patients with KIT-mutant metastatic disease who experience disease progression on imatinib should have their dose escalated. 67 Sunitinib is recommended as second-line therapy for patients who develop secondary imatinib resistance. 46 If disease progression continues on sunitinib, regorafenib and ripretinib can be used as third- and fourth-line therapies, respectively.69,71 If patients continue to progress on fourth-line therapies, options such as enrolment in clinical trials, rechallenge with imatinib, 71 continuation of therapy or dose escalation can be considered. Reducing or stopping TKIs is inadvisable in patients with mild-to-moderate AEs. In severe cases, dose interruption and rechallenging are recommended. Although systemic therapy is the cornerstone for mGISTs, locoregional therapies or metastasectomy should be considered in select patients.88,89 A summary of patient treatment options and pathways is summarized in Figure 1.
To optimize GIST patients’ access to treatment options and improve outcomes, early referrals to specialized high-volume centres are recommended. Additional support comes from the LRGC which provides patient advocacy, funding for GIST research, input for funding submissions and information for regulators/administrators. Furthermore, the role of liquid-based testing of plasma-derived ctDNA is emerging in GISTs and has been proven to be beneficial for evaluating treatment response, identifying resistant biomarker(s),120,121 guiding treatment122–125 and detecting postsurgical MRD but has not yet been implemented into routine standard of care practices.126,127
The availability of IHC and molecular tests, along with the discovery of oncogenic kinase mutations and kinase inhibitor therapies, have advanced our understanding of GIST and significantly impacted the approach to GIST management. 1 As new treatments and diagnostic tools become available in the future, the management of GIST will continue to evolve and may lead to further need for standardization in Canada.