
Abstract
Background and objectives:
Social distancing and quarantine implanted during the COVID-19 outbreak could have delayed the accession of oncologic patients to hospitals and treatments. This study analysed the management of sarcoma patients during this period in five Spanish hospitals.
Design and methods:
Clinical data from adult sarcoma patients, soft tissue and bone sarcomas, managed during the COVID-19 outbreak, from 15 March to 14 September 2020 (Covid cohort), were retrospectively collected and time for diagnosis, surgery and active treatments were compared with sarcoma patients managed during the same pre-pandemic period in 2018 (Control cohort).
Results:
A total of 126 and 182 new sarcoma patients were enrolled in the Covid and Control cohorts, respectively, who were mainly diagnosed as soft tissue sarcomas (81.0% and 80.8%) and at localized stage (80.2% and 79.1%). A diagnostic delay was observed in the Covid cohort with a median time for the diagnosis of 102.5 days (range 6–355) versus 83 days (range 5–328) in the Control cohort (p = 0.034). Moreover, a delay in surgery was observed in cases with localized disease from the Covid cohort with a median time of 96.0 days (range 11–265) versus 54.5 days (range 2–331) in the Control cohort (p = 0.034). However, a lower delay for neoadjuvant radiotherapy was observed in the Covid cohort with a median time from the diagnosis to the neoadjuvant radiotherapy of 47 days (range 27–105) versus 91 days (range 27–294) in the Control cohort (p = 0.039). No significant differences for adjuvant radiotherapy, neoadjuvant/adjuvant chemotherapy and neoadjuvant/adjuvant palliative chemotherapy were observed between both cohorts. Neither progression-free survival (PFS) nor overall survival (OS) was significantly different.
Conclusion:
Delays in diagnosis and surgery were retrospectively observed in sarcoma patients during the COVID-19 outbreak in Spain, while the time for neoadjuvant radiotherapy was reduced. However, no impact on the PFS and OS was observed.
Introduction
The new coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which started in December 2019 in Wuhan (Hubei, China), was spread worldwide and was declared a global pandemic by the World Health Organization on 11 March 2020.1,2 The clinical spectrum of COVID-19 was wide, distinguishing cases with asymptomatic infection, mild upper respiratory tract illness and severe viral pneumonia associated with respiratory failure and higher death risk.3,4 Sarcoma patients were particularly vulnerable in this period like all cancer patients, showing increased morbidity and mortality due to their immunosuppressed state caused by the neoplastic disease, chemotherapy, radiotherapy or surgery treatment but also by the disruption in the therapeutic plans.5–9 Social distancing and quarantine were implanted as containment measures to avoid transmission, and recommendations from the government and various scientific societies were focused on the necessity to minimize patient exposure to unnecessary hospital visits. However, these guidelines might have had an impact on the diagnosis and/or follow-up of sarcoma patients. It should be noted that patients with suspected high-grade malignancy required further evaluation in the clinic and immediate treatment, while for patients with low-grade malignancy and benign cases whose treatment was not urgent, telemedicine management might be a viable option.10–12
Several studies from different countries highly affected by the COVID-19 outbreak like Italy, Spain, France and Brazil have detected delays during the COVID-19 outbreak in the diagnosis or treatment of different cancer types, like ovarian, colorectal, bladder and prostatic cancer.13–17 Sarcoma patients have also been affected by diagnostic delays in Italy 18 or delays in performing biopsies in Poland 19 during this pandemic, although none of these studies detected changes in the survival of these patients. Other studies have detected an increase in the percentage of sarcoma patients affected by care modifications including telemedicine (74%), postponement of appointment (34%), scans (34%) and treatment (10%) in England 20 or in stopping/delaying surgery (20%) in Italy. 21
The aim of this study was to analyse if there were delays in the management of patients with soft tissue or bone sarcomas during the first peak of the COVID-19 outbreak in Spain, to improve the management of these oncologic patients in future similar situations.
Methods
Patients
In this retrospective study, 126 new sarcoma patients over 18 years old who were managed from 15 March to 14 September 2020 were enrolled in the Covid cohort, and 182 new sarcoma patients of the same pre-pandemic period in 2018 were enrolled in the Control cohort from five Spanish hospitals (University Hospital Virgen del Rocío, University Hospital General de Ciudad Real, University Hospital Miguel Servet, Hospital Clínico San Carlos and University Hospital Fundación Jiménez Díaz). Dates from the first symptom, diagnosis, surgery, radiotherapy and systemic treatment were collected for each patient. Only patients with at least one of these dates from 15 March to 14 September 2020 for the Covid cohort or 2018 for the Control cohort and the first symptom until 7 months before 15 March 2020 or 2018 were enrolled in this study. Sarcoma patients were treated with anthracyclines plus ifosfamide following standard of care, during both periods. The type or extension of the surgical resection was not collected in the database; thus, information regarding changes in the surgical planning due to delay is not available.
Data analysis
The median time for diagnosis was calculated in each cohort as the difference in days between the diagnosis and the first symptom dates, considering only sarcoma patients who showed the first symptom and/or the diagnosis from 15 March to 14 September 2020 for the Covid cohort or 2018 for the Control cohort. The median time for surgery was calculated in each cohort as the difference in days between the diagnosis and the surgery dates, considering only sarcoma patients who were diagnosed and/or operated on from 15 March to 14 September 2020 for the Covid cohort or 2018 for the Control cohort. Cases diagnosed from 15 March to 14 September but operated on at least 7 months after 15 September in 2020 for the Covid cohort or 2018 for the Control cohort or cases with excisional biopsy were not taken into account for this analysis. The median time for neoadjuvant treatment (radiotherapy, chemotherapy or palliative chemotherapy) was calculated in each cohort as the difference in days between the diagnosis and the neoadjuvant treatment dates, considering only sarcoma patients who were diagnosed and/or treated with neoadjuvant therapy from 15 March to 14 September 2020 for the Covid cohort or 2018 for the Control cohort. The median time for adjuvant treatment (radiotherapy, chemotherapy or palliative chemotherapy) was calculated in each cohort as the difference in days between the surgery and the adjuvant treatment dates, considering only sarcoma patients who were operated on and/or treated with adjuvant therapy from 15 March to 14 September 2020 for the Covid cohort or 2018 for the Control cohort. Treatments were considered neoadjuvant or adjuvant therapies if they were applied until 6 months before or after the surgery, respectively. Cases with palliative chemotherapy after 7 months from 15 September 2020 for the Covid cohort or 2018 for the Control cohort were not taken into account for this analysis. Statistical analyses were carried out using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA) applying the Mann–Whitney test.
Time-to-event variables, progression-free survival (PFS) and overall survival (OS) were estimated by the Kaplan–Meier survival analysis. PFS was assessed by median time and measured from surgery date until progression or death. OS was assessed by median time and measured from the diagnostic date until death.
Results
Patients’ characteristics
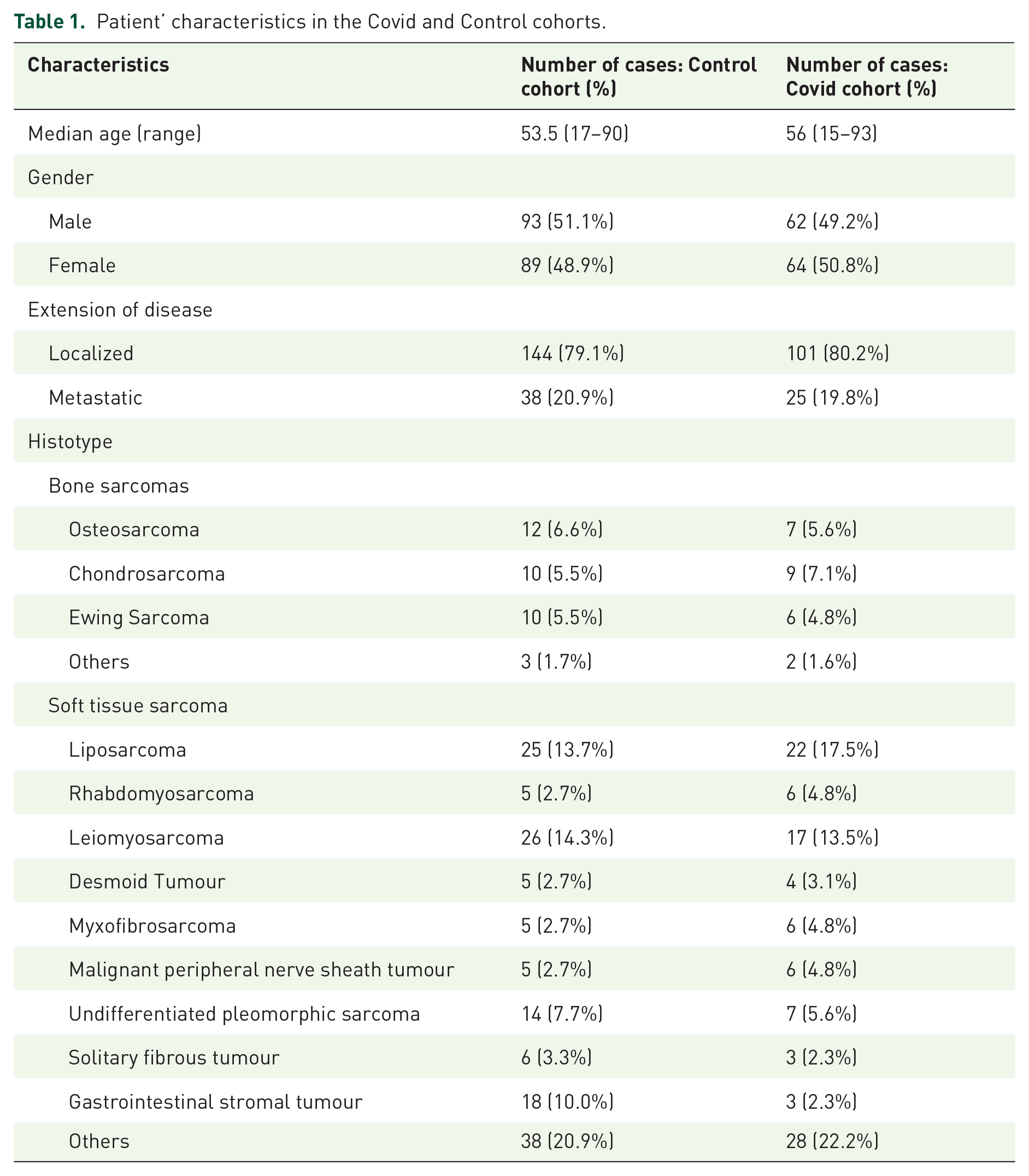
A total number of 126 new sarcoma patients managed in terms of first symptom, diagnosis, surgery or active treatment during the first peak of the COVID-19 outbreak in 2020, from 15 March to 14 September, were enrolled in the Covid cohort and 182 new patients from the same period in 2018 were enrolled in the Control cohort. The median age at diagnosis was 56 years (range 15–93) in the Covid cohort and 53.5 years (range 17–90) in the Control cohort, with a 49/51 or 51/49 proportion of male/female, respectively (Table 1). The most frequent stage at diagnosis was localized disease in both cohorts representing 80.2% and 79.1% of the cases in the Covid or Control cohort, respectively. The majority of the cases were diagnosed as soft tissue sarcomas in the Covid and Control cohorts (81.0% and 80.8%), among them, the most frequent types were liposarcoma (17.5% and 13.7%), leiomyosarcoma (13.5% and 14.3%) and undifferentiated pleomorphic sarcoma (5.6% and 7.7%). Among the bone sarcomas in the Covid and Control cohorts (19.2% and 19.0%), the most frequent types were chondrosarcoma (7.1% and 5.5%), osteosarcoma (5.6% and 6.6%) and Ewing sarcoma (4.8% and 5.5%; Table 1).
Patient’ characteristics in the Covid and Control cohorts.
Diagnostic and therapeutic delay during the COVID outbreak
A diagnostic delay was observed in the Covid cohort, with a median time from the first symptom to the diagnosis of 102.5 days (range 6–355) versus 83 days (range 5–328) in the Control cohort (p = 0.034, Table 2). Moreover, a delay in surgery was observed in the Covid cohort when only cases with localized disease were considered, with a median time from the diagnosis to the surgery of 96 days (range 11–265) versus 54.5 days (range 2–331) in the Control cohort (p = 0.034). When all the cases (localized and metastatic) were taken into account, a similar delay in surgery was observed in the Covid cohort versus the Control cohort [95 days (range 4–265) versus 55 days (range 2–331)] but nearly significant (p = 0.065; Table 2). However, a lower delay in the treatment with neoadjuvant radiotherapy was observed in the Covid cohort, with a median time from the diagnosis to the neoadjuvant radiotherapy treatment of 47 days (range 27–105) versus 91 days (range 27–294) in the Control cohort (p = 0.039). All the cases treated with radiotherapy or chemotherapy were in the stage of localized disease at diagnosis. No significant differences in the median time for the treatment of adjuvant radiotherapy, neoadjuvant chemotherapy or adjuvant chemotherapy were observed between both cohorts (Table 2). There was also no significant difference in the median time for the treatment of palliative chemotherapy, even when it was used as neoadjuvant or adjuvant therapy, between both cohorts (Table 2). The majority of cases treated with palliative chemotherapy were metastatic at diagnosis in the Covid (75.9%) and Control (67.6%) cohort. Treatment regimens and duration followed the standards for clinical practice in both cohorts, without variation in the pandemic period.
Diagnostic and treatment delays in sarcoma patients between the COVID and Control cohort.

Loc, localized disease; Met, metastatic disease; p-value, Mann–Whitney test.
Survival analysis
After a median follow-up of 33 months (range 2–38) and 55 months (range 0–63) in the Covid and Control cohorts, respectively, no significant differences in PFS or OS were observed, taking into account all the sarcoma patients (PFS: p = 0.238; OS: p = 0.424) or only cases with localized disease (PFS: p = 0.194; OS: p = 0.113; Figure 1). There was also no difference in PFS or OS independently in soft tissue or bone sarcomas (Supplemental Figure 1S).
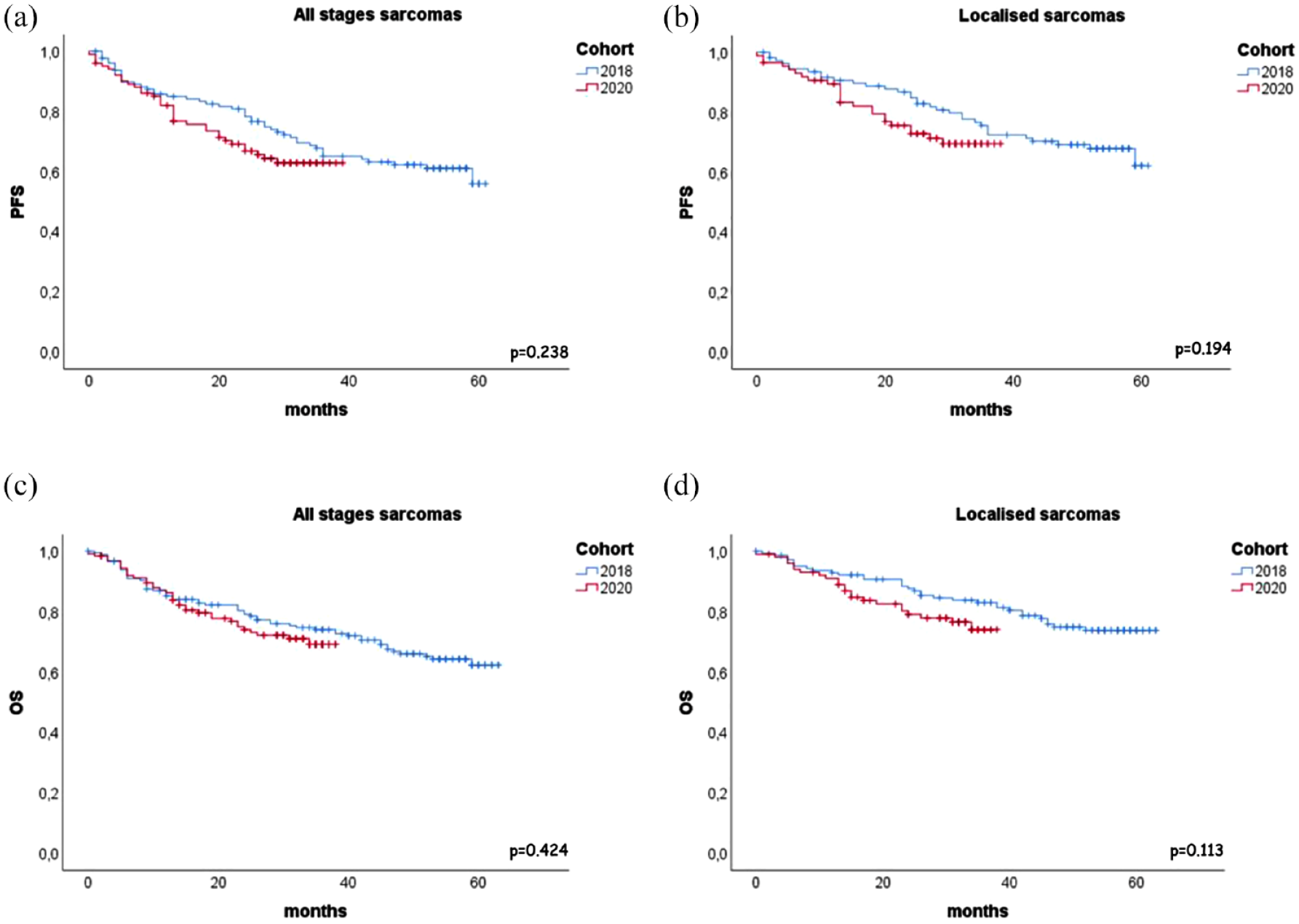
PFS and OS in sarcoma patients from the Covid and Control cohort. Kaplan–Meier curve for PFS in sarcomas of the Covid (red) and the Control (blue) cohort, irrespective of the stage at diagnosis (a) or in localized sarcomas (b). Kaplan–Meier curve for OS in sarcomas of the Covid (red) and the Control (blue) cohort, irrespective of the stage at diagnosis (c) or in localized sarcomas (d).
Discussion
The treatment and management of sarcoma patients during the COVID-19 peak of the pandemic have been challenging because healthcare systems had to attend to the high number of patients affected by the severe acute respiratory syndrome and as a consequence were forced to prioritize the rest of medical activities. Although most oncologic activities were considered not deferrable, changes like a larger use of schedules with longer intervals, a preference for oral treatments over intravenous ones, a larger use of neoadjuvant therapy to delay surgery, the use of hypofractionated radiotherapy and an earlier shift towards supportive care have been introduced22,23 based on expert opinions and not on objectives data. 24 Specifically for sarcomas, different prioritizing recommendations were established for diagnostic, care and follow-up procedures across different sarcoma contexts.11,12,25–27
This retrospective analysis in the management of sarcoma patients from five Spanish hospitals showed a diagnostic delay during the first pandemic peak in Spain, with an increase of 19.5 days in the median time for the diagnosis versus the Control cohort. This diagnostic delay is similar to that reported in Italy, the first country most affected during the first COVID-19 peak in Europe followed by Spain, with 13 days of delay in the definitive diagnostic or even 27 days of delay for the first histological diagnosis during the third trimester of 2020. 18 In Poland, only a delay to perform a biopsy of 5.5 days was observed, 19 but this country was not one of the most affected during the first pandemic peak in Europe. The median time for diagnosis of 12 weeks observed in our Control cohort is similar to previously reported in other studies for soft tissue and bone sarcoma, although it depends on the subtype. 28 Moreover, a surgical delay was observed in the Covid cohort with an increase of 41.5 days in the median time for surgery. The surgical delay was also observed in other studies, 29 although in general it was not recommended for operable patients without COVID-19 symptoms, in particular for grade 2–3 soft tissue sarcoma, bone sarcoma, gastrointestinal stromal tumour (GIST) and visceral sarcoma. 27 However, a decrease of 44 days in the median time for the neoadjuvant radiotherapy treatment was observed which was applied to new cases with localized disease and could be in concordance with recommendations of use to delay surgery or as hypofractionated radiotherapy.22,23,27,30 Additionally, it was observed that a higher percentage of cases were treated with neoadjuvant radiotherapy in the Covid cohort versus the Control cohort (11.9% versus 4.9%) and neoadjuvant chemotherapy (23.0% versus 4.9%), while similar percentages were observed in adjuvant radiotherapy (13.5% versus 14.1%) and chemotherapy (11.9% versus 12.5%). However, no significant differences were observed in the median time for the neoadjuvant chemotherapy and adjuvant radiotherapy or chemotherapy treatment. Despite the delays in diagnosis and surgery in the Covid cohort, no significant differences in survival were observed, like it was reported in the studies from Italy and Poland.18,19 However, it is known that diagnostic delay is a cause for a higher clinical stage at diagnosis and a poorer prognosis in oncology patients,31,32 affecting the treatment response and survival.33,34 No significant survival differences in the Covid cohort of our study could be explained because delays in diagnosis and surgery did not necessarily affect the same sarcoma patients and because delays in treatment were not observed. However, it could be interesting to continue the follow-up of these patients.
The lower number of new cases enrolled in the Covid cohort versus the Control cohort was due to the original design of this study allowed for the collection also sarcoma patients who were followed up from 15 March to 14 September 2020, although they were diagnosed and/or treated some years before. These cases underwent mainly changes to telemedicine (60.4%) as has been reported in other studies 20 and delays in image probes (13.7%), medical appointment (17.2%), diagnosis of relapse (8%), chemotherapy (11.1%) and radiotherapy (6.25%) treatment or in surgery (2.3%). Changes to telemedicine (31%) also were observed in the Covid cohort.
This retrospective study has the limitation of collecting the data on different dates, some of them could not be available or clearly annotated in the clinic history of each patient.
In conclusion, this study reports a diagnostic and surgery delay in the management of sarcoma patients during the COVID outbreak in the Spanish population. However, a lower delay in neoadjuvant radiotherapy was observed. Despite these changes, no significant differences were observed in the survival of these patients during the COVID-19 outbreak.
Supplemental Material
sj-png-1-tam-10.1177_17588359231220611 – Supplemental material for Delays in diagnosis and surgery of sarcoma patients during the COVID-19 outbreak in Spain
Supplemental material, sj-png-1-tam-10.1177_17588359231220611 for Delays in diagnosis and surgery of sarcoma patients during the COVID-19 outbreak in Spain by Jaime Carrillo-García, Serena Lacerenza, Nadia Hindi, Irene Carrasco García, Gloria Marquina, Juana María Cano Cano, Javier Martínez Trufero, Alberto Rafael Sevillano Tripero, Tania Luis García, Manuel Jorge Cuesta Rioboo, David S. Moura, Marta Renshaw, Jose L. Mondaza-Hernández, Davide Di Lernia, Antonio Gutierrez and Javier Martin-Broto in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-png-2-tam-10.1177_17588359231220611 – Supplemental material for Delays in diagnosis and surgery of sarcoma patients during the COVID-19 outbreak in Spain
Supplemental material, sj-png-2-tam-10.1177_17588359231220611 for Delays in diagnosis and surgery of sarcoma patients during the COVID-19 outbreak in Spain by Jaime Carrillo-García, Serena Lacerenza, Nadia Hindi, Irene Carrasco García, Gloria Marquina, Juana María Cano Cano, Javier Martínez Trufero, Alberto Rafael Sevillano Tripero, Tania Luis García, Manuel Jorge Cuesta Rioboo, David S. Moura, Marta Renshaw, Jose L. Mondaza-Hernández, Davide Di Lernia, Antonio Gutierrez and Javier Martin-Broto in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.