
Abstract
Over a decade of sequencing-based genomics research has unveiled a diverse somatic mutation landscape across patients with pancreatic ductal adenocarcinoma (PDAC), and the identification of druggable mutations has aligned with the development of novel targeted therapeutics. However, despite these advances, direct translation of years of PDAC genomics research into the clinical care of patients remains a critical and unmet need. Technologies that enabled the initial mapping of the PDAC mutation landscape, namely whole-genome and transcriptome sequencing, remain overly expensive in terms of both time and financial resources. Consequentially, dependence on these technologies to identify the relatively small subset of patients with actionable PDAC alterations has greatly impeded enrollment for clinical trials testing novel targeted therapies. Liquid biopsy tumor profiling using circulating tumor DNA (ctDNA) generates new opportunities by overcoming these challenges while further addressing issues particularly relevant to PDAC, namely, difficulty of obtaining tumor tissue via fine-needle biopsy and the need for faster turnaround time due to rapid disease progression. Meanwhile, ctDNA-based approaches for tracking disease kinetics with respect to surgical and therapeutic interventions offer a means to elevate the current clinical management of PDAC toward higher granularity and accuracy. This review provides a clinically focused summary of ctDNA advances, limitations, and opportunities in PDAC and postulates ctDNA sequencing technology as a catalyst for evolving the clinical decision-making paradigm of this disease.
Keywords
Introduction
Pancreatic cancer incidence has steadily increased over recent years to become the third-leading cause of cancer-related death in the United States. 1 Paluri et al. recently reported that over 60% of patients diagnosed with pancreatic ductal adenocarcinoma (PDAC), the most common form of pancreatic cancer, were diagnosed with incurable metastatic disease and that this number has increased to nearly 70% during the COVID-19 pandemic. 2 As many patients diagnosed with metastatic PDAC are too unwell to be treated with systemic therapy, 3 the average patient survival is approximately 2–3 months. 4
The past decade of sequencing-based genetic research in PDAC has shown a diverse mutational landscape across patient tumors, with approximately 20% of tumors bearing mutations considered therapeutically actionable and capable of improving individual patient survival when used to guide therapy.5,6 Despite these advances in the academic field, accessibility continues to impede the delivery of genomics-guided medicine to the majority of patients with PDAC, as sequencing-based technologies capable of detecting actionable mutations are often restricted to a subset of patients receiving care through large-center clinical trials in major academic centers. Moreover, the application of bulk tissue sequencing to the clinical management of PDAC faces additional and unique challenges when compared to other cancer types, including difficulty in tissue biopsy procedure and rapid decline in patient health precluding biopsy and often utility of genomic results. As a result, the majority of patients diagnosed with PDAC do not receive any genomics testing, and clinical decision-making in PDAC remains largely centered around cytotoxic chemotherapy regimens guided by patient performance status.
Recent advances in circulating tumor DNA (ctDNA) sequencing technology present an opportunity to evolve the current clinical paradigm of PDAC care to leverage the growing knowledge base of actionable mutations through a genomics-based assay that is less invasive while having faster turnaround times and lower cost, though necessary improvements in the sensitivity and specificity of contemporary ctDNA panels remain ongoing. This review aims to delineate recent advances and ongoing limitations of ctDNA sequencing in PDAC, while positioning ctDNA-based technology as a promising catalyst for the much-needed evolution of routine clinical decision-making in PDAC.
The clinical actionability landscape of PDAC
For over a decade, DNA sequencing-based profiling of cancer using bulk tumor tissue biopsies has unveiled complex and diverse mutational landscapes across many cancer types including PDAC.7–10 Actionable mutations, in which mutation presence confers sensitivity to specific targeted agents, are harbored in approximately 20% of PDAC tumors11,12 and include alterations such as NRG1 fusion (targeted agents include afatinib 13 and zenocutuzumab 14 ), NTRK fusion (entrectinib, 15 larotrectinib 16 ), ALK fusion, DNA damage repair mutation (such as germline PALB2/BRCA mutation; PARP inhibition 17 ), and KRAS G12C mutation (sotorasib, 18 adagrasib 19 ). Consequently, a surge of clinical trials aimed at demonstrating the efficacy of molecular-targeted drugs have emerged and include examples such as CRESTONE (NRG1 fusion inhibitor; NCT04383210), CodeBreak100 (G12C inhibitor; NCT03600883), and NAVIGATE (NTRK1 fusion inhibitor; NCT02576431). Ability to enroll eligible patients into such molecular-targeted trials, however, is faced with several ongoing challenges that greatly slow the adoption of novel therapeutics into PDAC clinical care.
Challenges faced by molecular-targeted clinical trials in PDAC
The frequency of a specific targetable mutation is low among the total population of patients diagnosed with PDAC and can vary greatly across different cohorts of patients, with NRG1 fusion rates, for example, varying from 0 of 195 patients, 9 3 of 47 patients 13 (6%), and 3 of 17 patients 20 (18%). Despite their low frequency, however, the number of patients with PDAC capable of benefiting from targeted treatments should not be understated. In 2022, there is estimated to be 62,210 new cases of pancreatic cancer in the United States alone, and this number has risen over past years.1,21 The question remaining, then, lies in how the subgroup of patients with actionable mutations may be better identified. Exploratory, bulk tissue-based next-generation sequencing (NGS) technologies, such as whole-genome sequencing (WGS), were fundamental in establishing the current knowledge base of PDAC mutation landscapes. Continuing to apply such methods to the unselected patient population in hopes of identifying patients eligible for subgroup-targeted PDAC clinical trials, however, is suboptimal given the required time and financial costs of bulk tissue sequencing.22–24 While ctDNA sequencing offers improvement in terms of cost-effectiveness, sequencing would remain unproductive for the roughly 80% of patients with PDAC who do not harbor targetable alterations. Meanwhile, it is well established that the majority of targetable alterations are highly enriched among the approximately 10–15% of PDAC tumors that lack oncogenic KRAS mutation, 25 and studies of NRG1 fusions in PDAC, for instance, have converged on the observation that such fusions are exclusively found in the KRAS wild-type subgroup of patients.13,20 For patients newly diagnosed with PDAC, clinical testing of KRAS mutation status followed by deployment of further sequencing-based testing for those with KRAS wild-type tumors represents a tiered and reflexive approach that would build upon what we have learned in PDAC genomics to better guide the appropriate subpopulation of patients toward genetic testing and greatly aid clinical trial enrollment.
Clinical trial enrollment for patients with PDAC is further hindered by inherent aggressiveness of the disease, which manifests as rapid clinical deterioration. Identification of patients with PDAC who are eligible for subgroup-targeted clinical trials is therefore time-sensitive and with turnaround times ranging between 19 and 52 (median 35) days from time of biopsy 9 ; bulk tissue WGS is not well suited for this application. Apart from time required to perform tissue sequencing, complexities surrounding tissue biopsy further delay sequencing-based guidance in care. For a cohort of 116 patients with PDAC, Deshwar et al. reported a median diagnostic time (time from first medical visit to diagnosis) of 22 days, and individuals with longer diagnostic times were significantly less likely to be suitable candidates for resection. 26 Meanwhile, delays in tissue biopsy are included among the list of negative effects by which the COVID-19 pandemic has impacted clinical care for patients with PDAC. 27 While WGS possesses the breadth to cover nearly all detectable mutations in a sample, ctDNA panels are subdivided into two main categories based on how their more limited catalog of ascertainable mutations are chosen. Tumor-naïve panels rely on a predetermined list of genes commonly implicated across many cancer types, such as the 54- and 500-gene Guardant360 and GuardantOMNI (respectively) panels,28,29 while tumor-informed panels require upfront tissue biopsy and sequencing to identify the tumor mutation landscape of the individual patient, which is then used to tailor the list of ascertainable mutations. As a more rapid technology that requires only blood-based sampling, tumor-naïve ctDNA sequencing improves upon the time limitations of tissue-based WGS and offers more promise in the deliverance of sequencing-informed care for patients with PDAC. In colorectal cancer, comparison between tumor-naïve ctDNA-based GOZILA (Guardant360; n = 1687 patients) and tissue-based (non-ctDNA; mutation panel) GI-SCREEN (n = 5621) studies showed that ctDNA analysis increased the relative proportion of patients enrolled in clinical trials by 132% while shortening the median time between sample collection and trial enrollment (1.1 months for ctDNA versus 20.2 months for tissue 30 ). Meanwhile, other tumor-naïve ctDNA studies have reported average turnaround times (from sample collection to results reporting) of 9 (Guardant360; various advanced cancer types 31 ), 9.5 (Guardant360; various advanced rare cancers 32 ), and 15 (Guardant360; advanced lung adenocarcinoma 33 ) days. While the clinical benefit of reduced genomics turnaround times is certainly intuitive, clinical trials focused on ctDNA-based treatment decision-making in PDAC are currently needed to measure the degree to which clinical outcome is improved for patients receiving ctDNA versus tissue sequencing.
Rapid clinical deterioration introduces an additional challenge when identifying patients with targetable mutations, as repeat tissue biopsy procedures, the majority being fine-needle aspirate biopsy of metastatic lesions of the liver, are often too invasive for patients that have progressed on first-line therapy. Inability to perform progression biopsies represents a distinct missed opportunity in PDAC, as the evolution of tumors over time during treatment (in which acquired mutations not present in initial biopsy sampling emerge) is well known.16,34,35 The utility of minimally invasive blood sample-based ctDNA sequencing is therefore very promising for repeat tumor sampling for patients with PDAC.
ctDNA-based mutation profiling in PDAC
Cell-free, tumor-derived DNA fragments circulating in the blood stream (ctDNA) provide a window into the mutational landscape of a tumor. Early studies showed that circulating DNA levels were significantly more pronounced in plasma samples from patients with pancreatic cancer compared to healthy donors and were compatible with the notion that DNA from tumor cells could be shed into the peripheral blood stream.36,37 With the emergence of DNA sequencing technology, it was later confirmed that plasma-derived, cell-free DNA (cfDNA) detected in patients with PDAC could be attributed to tumor cells based on the presence of mutant KRAS.38,39 ctDNA typically represents only a small proportion of the total cfDNA in a plasma sample. In colorectal cancer, the proportion of ctDNA has been quantified at approximately 1% of total cfDNA, 40 and this level has been shown to vary greatly across patients. 41 Correlation between ctDNA levels and tumor stage is perhaps intuitive, as later tumor stages involve increased circulatory system infiltration which facilitates metastasis, and increased ctDNA levels in metastatic compared to localized tumors have been shown for several cancer types including pancreas. 42 Recently, a 2022 study benchmarking ctDNA assays from five different vendors showed that variant allele frequency and DNA input levels affected accuracy at varying degrees in each of the different ctDNA platforms. 43 Taken together, factors such as disease stage, sample input, and sequencing platform are reasons for which the ability to detect true genomic alterations or sensitivity has been perhaps the most challenging aspect of ctDNA sequencing that continues to impede its adoption into routine clinical practice.
Clonal, oncogenic KRAS mutations are present in approximately 90% of PDAC and represent a reasonable surrogate for assessing ctDNA sensitivity. Between 2015 and 2020, plasma-based sequencing studies in PDAC have reported KRAS mutation frequencies ranging from 40 to 77%44–49 (with a mean of 59%). More recent studies conducted in 2021 reported KRAS mutation rates of 55 and 53% across ctDNA PDAC patient cohorts of size 104 (Guardant360) and 100 (in-house NGS of plasma), respectively,50,51 while a study in 2022 reported a KRAS mutation frequency of 77% (PredicineATLAS; tumor-naïve). 52 A summary of studies reporting ctDNA-based KRAS mutation frequencies is provided in Table 1. Taken together, these data indicate a need for better sensitivity of ctDNA sequencing in PDAC to adequately capture the expected number of KRAS mutations. Quality control (QC) metrics of ctDNA sequencing data typically require a minimum threshold of detectable ctDNA or circulating tumor fraction (CTF) in order to successfully pass QC and be included in downstream data analysis. Samples with inordinately low CTF may lack mutations due to limited sensitivity (therefore bearing an increased number of false negatives). By iteratively setting increasingly stringent CTF thresholds at which samples are excluded from analysis, the KRAS mutation rate of a ctDNA dataset can be brought closer to the expected 90% by excluding samples for which the lack of KRAS mutation may be attributed to data quality. 52 While this sacrifices the number of analyzable samples for increased sensitivity, such a strategy may be required for near-term adoption of ctDNA sequencing in clinical care of patients with PDAC until these technologies further improve.
Summary of ctDNA-based KRAS mutation rates across studies.
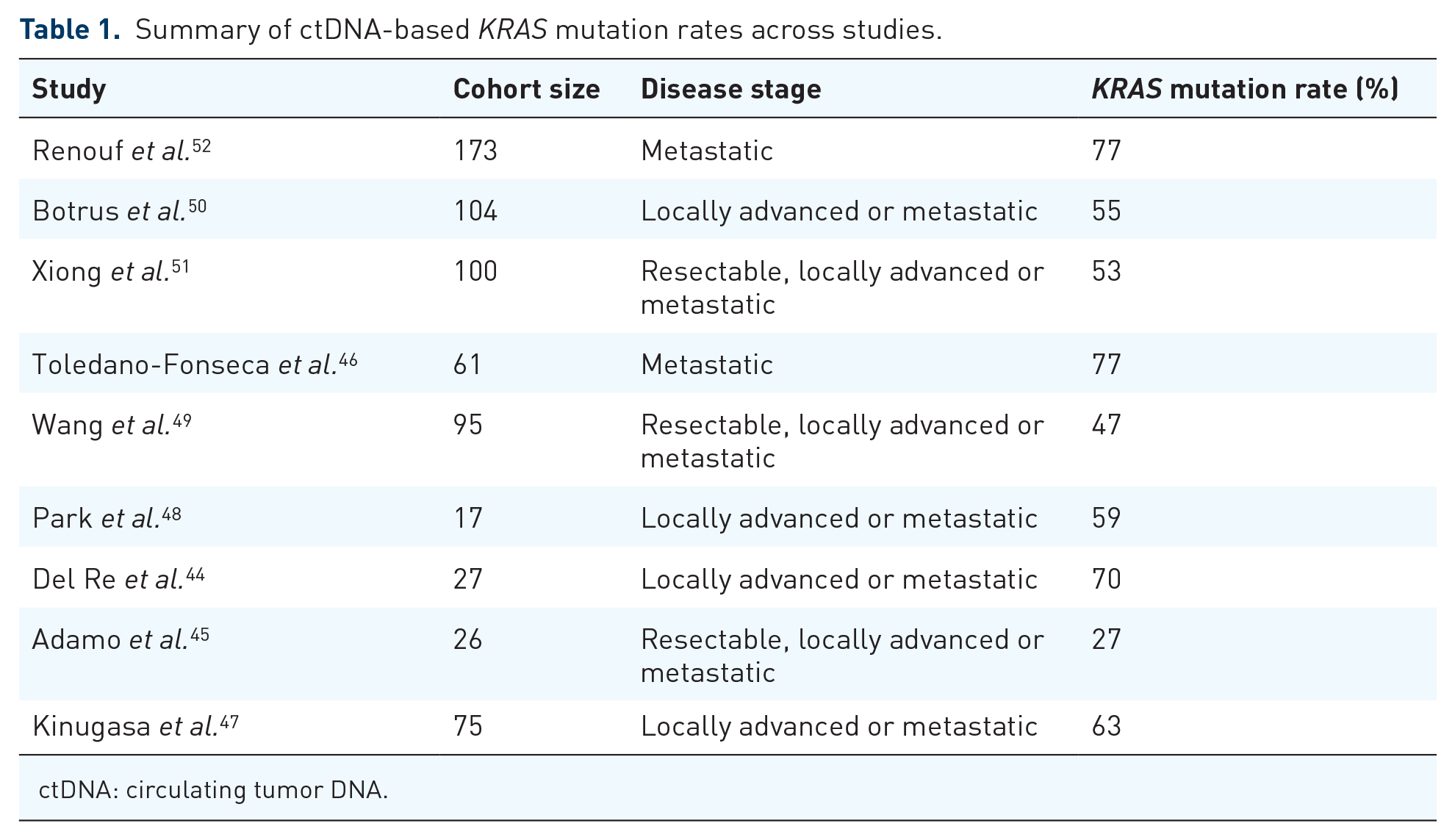
ctDNA: circulating tumor DNA.
Existing strategies for tracking disease kinetics in PDAC are unsatisfactory
There is a high risk of disease recurrence in patients with surgically resectable PDAC. From a cohort of 692 patients diagnosed with PDAC undergoing pancreatectomy, Groot et al. found that 76.7% of patients had disease recur within a median of 11.7 months, with the majority of recurrences detected at distant organ sites. 53 In the metastatic setting, FOLFIRINOX and GEMABR have been associated with disease progression at a median of 6.4 and 5.5 months, respectively.54,55 As with other cancers, optimal clinical management of PDAC is primarily governed by alignment between therapeutic timing and disease progression and requires tools capable of granular and accurate disease monitoring, which remain a critical and unmet need in PDAC. The current paradigm for clinical disease monitoring in PDAC consists of radiographic CT scan imaging and the blood-based biomarker carbohydrate 19-9 antigen (CA19-9). While capable of high granularity due to being a blood-based test, CA19-9 is unsatisfactory for PDAC disease monitoring due to having a low sensitivity and specificity of approximately 80%.56,57 Meanwhile, CT scans benefit from higher accuracy (sensitivity and specificity of 90 and 87%, respectively 58 ) but are resource intensive.
ctDNA to monitor disease recurrence in PDAC
Minimal residual disease (MRD), the quantification of residual tumor DNA in a sample following surgical or therapeutic intervention, represents an emerging application in ctDNA sequencing technology focused on monitoring of disease progression. Given the inherent challenge of detecting minute residual ctDNA levels, studies of MRD in PDAC to date have largely focused on detection of oncogenic KRAS mutations as they occur as frequent and highly clonal events. In resectable PDAC, KRAS-based MRD detection by ctDNA sequencing has been shown to provide prognostic information as overall or progression-free survival (OS or PFS) in patients with MRD positivity either before or after surgery is significantly lower compared to patients that are MRD-negative. In the preoperative setting, Yamaguchi et al. demonstrated reduced OS [hazard ratio (HR) = 2.35, p = 0.008] in 24/97 (25%) patients that were ctDNA-positive, 59 while Groot et al. showed decreases in both the PFS (19 months versus 8 months, p < 0.001) and OS (not reached versus 14 months, p = 0.009) of 29/59 (49%) patients with ctDNA positivity. 60 Additionally, Lee et al. also showed reduced PFS (HR = 4.1, p = 0.002) and OS (HR = 4.1, p = 0.015) in 23/37 (62%) of patients with preoperative ctDNA positivity. 61 Postoperatively, Groot et al. demonstrated reduced PFS (15 months versus 5 months, p < 0.001) in 11/41 (27%) ctDNA-positive patients, 60 while Lee et al. also showed reduced PFS (HR = 5.4, p < 0.0001) and OS (HR = 4.0, p = 0.003) in 13/35 (37%) of ctDNA-positive patients. 61 In the metastatic disease setting, Kruger et al. showed the utility of ctDNA-based MRD monitoring of KRAS mutation kinetics in predicting early response to chemotherapy, with significantly higher accuracy of KRAS-mutant ctDNA detection (83% sensitivity, 100% specificity) compared to several CA19-9 and CEA biomarker thresholds (p < 0.05). 62 While preliminary, these studies show significant promise for how ctDNA technologies may transform the clinical paradigm in PDAC, as accurate and molecular-informed prognostication currently remain unavailable. A major limitation of these studies, however, is that they do not apply to the approximately 10% of patients with PDAC who harbor KRAS-wild-type tumors. Jiang et al. demonstrated the prognostic significance of MRD in resectable PDAC using a ctDNA assay extending beyond oncogenic KRAS mutations, detecting clonal mutations in other genes commonly mutated in PDAC such as TP53, CDKN2A, and SMAD4. 63 Using an expanded MRD panel that included other genes in addition to KRAS, the authors demonstrated a reduction in disease-free survival (HR = 5.2, p = 0.019) in 9/27 (33%) postoperative ctDNA-positive patients. The design of studies such as these, capturing a wider breadth of mutations beyond KRAS, will be important as ctDNA-based MRD monitoring moves toward clinical practice.
Besides providing prognostic information, one of the most impactful goals of ctDNA-based MRD monitoring in PDAC is to guide treatment decision-making, such as initiation, dosage, therapy switching, and precision onco-surgery. 11 In the resectable and borderline resectable disease setting, surgical resection via the Whipple procedure is highly invasive and is carried out with the primary goal of eliminating a tumor prior to circulatory system infiltration and subsequent spread to distant organ sites. For patients who have completed neoadjuvant chemotherapy and are scheduled for surgical resection, ctDNA-positive status prior to surgery would indicate a high likelihood of micrometastatic disease, and such patients could be spared invasive surgical resection when such a procedure is likely futile. Meanwhile, post-surgery, changes to therapy could be considered for patients on adjuvant chemotherapy that experience persistent increases in MRD levels while on therapy, thereby avoiding prolonged treatment-related toxicities when such treatments have ceased working. Ongoing trials of chemotherapy timing in PDAC that generate retrospective ctDNA datasets will provide important insight into the utility of ctDNA during chemotherapy and include the PAC3 trial (NCT04340141) of perioperative versus adjuvant FOLFIRINOX in patients with resectable PDAC.
RNA sequencing-based molecular subtypes of metastatic PDAC have been correlated with differential response to first-line chemotherapy, such that patients with “basal-like” tumors receiving FOLFIRINOX may be better off receiving GEMABR instead. 9 As RNA-based profiling is unavailable for patients with PDAC outside of a select few large-center clinical trials, sustained increases in ctDNA-based MRD levels in patients with metastatic PDAC receiving first-line FOLFIRINOX may serve as a more feasible sentinel for immediate first-line therapy switching to GEMABR.
The role of ctDNA-based sequencing in prognostication and therapeutic decision-making in PDAC remains highly preliminary and is limited by the lack of randomized, prospective clinical trial data. In stage II colorectal cancer, the DYNAMIC trial (ACTRN12615000381583) randomized patients to have postoperative treatment guided by ctDNA sequencing results versus standard clinicopathological features. Results of the trial demonstrated the ability for ctDNA-based monitoring to spare ctDNA-negative patients from unnecessary adjuvant chemotherapy while not compromising their recurrence-. 64 In pancreatic cancer, DYNAMIC-pancreas (ACTRN12618000335291) remains ongoing and is poised to determine the utility of ctDNA sequencing for informing adjuvant chemotherapy in patients with early stage pancreatic cancer. Additional ongoing ctDNA-based pancreatic cancer trials are summarized in Table 2 and include observational studies such as NCT05052671, NCT04616131, and PROJECTION (NCT04246203), each of which are noninterventional studies aimed at exploring the relationship between ctDNA levels with respect to pre/postsurgery timepoints and prognosis.
Summary of ctDNA-based clinical trials in PDAC.

CA19-9: carbohydrate 19-9 antigen; ctDNA: circulating tumor DNA; PDAC: pancreatic ductal adenocarcinoma; PFS: progression-free survival; OS: overall survival.
ctDNA in early detection of PDAC
Germline mutations affecting key DNA damage repair genes, such as BRCA1/2, as well as chronic pancreatitis, have been established as features that predispose individuals to developing PDAC.65–67 Individuals bearing these features are therefore considered as a high-risk group and would benefit from screening procedures capable of accurately capturing early onset of PDAC. While an early study of mutation-based ctDNA screening for early PDAC development did not show improvement compared to using CA19-9 alone, 68 a more recent study demonstrated higher accuracy when ctDNA and protein biomarkers were used in combination (64% sensitivity, 99.5% specificity 69 ). Apart from mutation-based profiling, DNA methylation-based ctDNA assays may also offer promising clinical utility in the early detection of PDAC in high-risk individuals. DNA methylation is a form of epigenetic control in which segments of DNA are structurally regulated, thus affecting transcriptional machinery access, without changes to nucleotide composition. Similar to somatic mutations affecting key genes such as KRAS and TP53, recurrent disease-associated methylation patterns have been identified in PDAC, and the utility of using ctDNA-based promoter methylation biomarkers for early PDAC detection has been demonstrated for ADAMTS1 (87.2% sensitivity, 95.8% specificity) and BNC1 (64.1 and 93.7%). 70 Similar to ongoing trials in ctDNA-based detection of early tumorigenesis in colorectal cancer, such as the ECLIPSE trial (NCT04136002), prospective clinical trials investigating the utility of ctDNA-based screening are currently needed in PDAC.
Concluding remarks
Taken together, opportunities for incorporating ctDNA sequencing-based analyses into routine clinical management of patients with PDAC include mutational profiling for personalized treatment selection, molecular-based prognostication, and tracking of disease kinetics (Figure 1). Each of these address critical needs imposed by the nature of the disease such as rapid deterioration in patient health and lack of biomarkers that are both granular and accurate. In the context of mutational profiling for personalized medicine, ctDNA sequencing offers a more rapid and less invasive alternative to tissue-based sequencing techniques. Meanwhile, pending advances in therapeutic decision-making in PDAC can be represented as a nexus of therapy selection, timing, dosage, and prognostication. While prospective clinical trials are in early stages, emerging demonstrations of the utility of ctDNA sequencing to successfully guide clinical management in colorectal cancer demonstrate highly promising avenues for the clinical utility of ctDNA in PDAC.
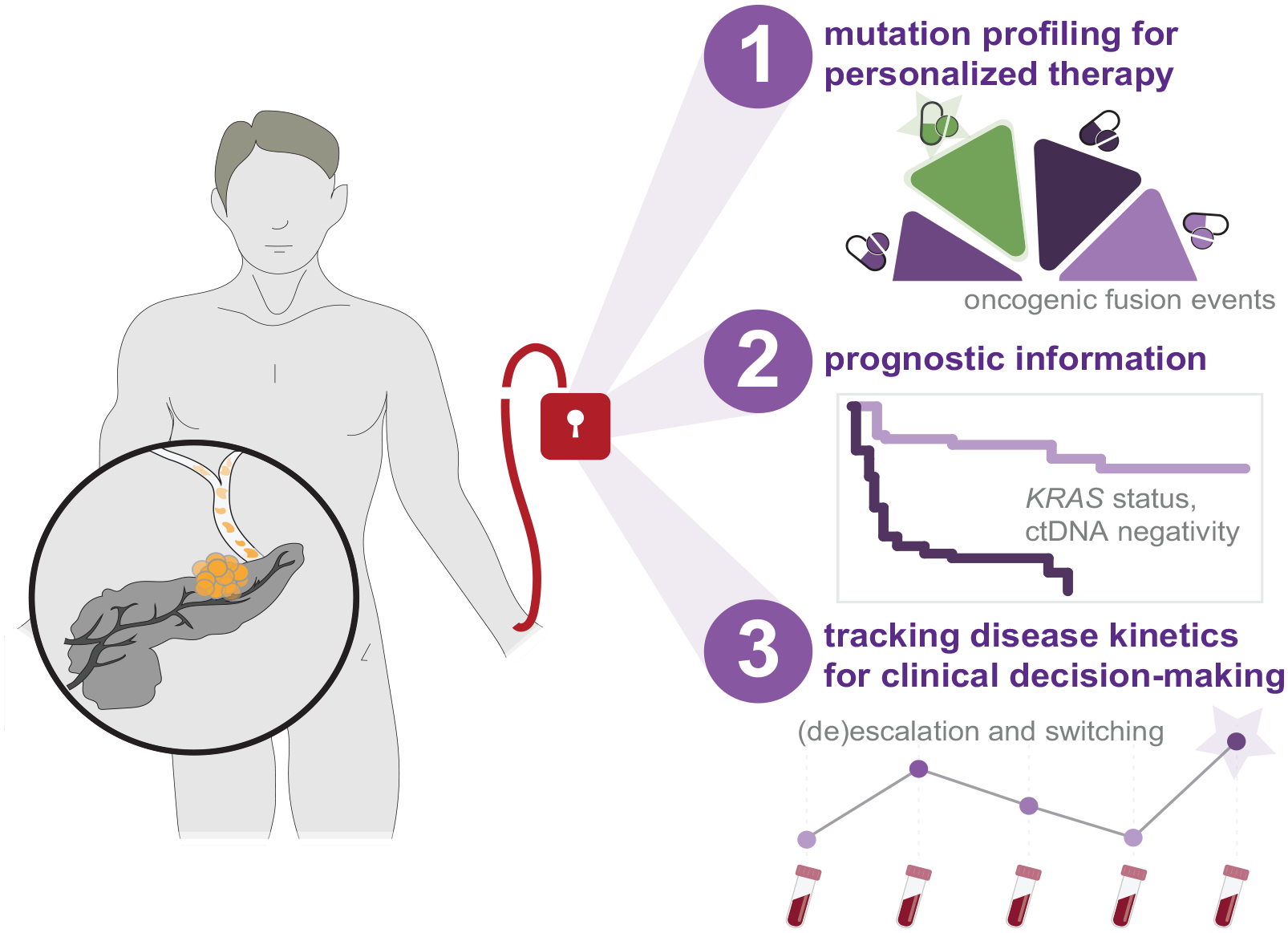
Strategies concerning the incorporation of ctDNA sequencing-based analyses into clinical management of PDAC. Emerging studies provide indication for ctDNA sequencing to improve the clinical paradigm for patients diagnosed with PDAC through mutational profiling for personalized therapy selection, molecular-based prognostication, and tracking of disease kinetics to guide therapeutic decision-making.
Footnotes
Acknowledgements
Not applicable.