
Abstract
Immune checkpoint inhibitors (ICIs) are the current guideline recommended treatment for many malignancies considered to be terminal. Despite considerable advances, their utility remains limited, and the field requires synergistic partners to further improve outcomes. Oncolytic viruses (OV) are emerging as contenders for the role of the synergistic agent of choice due to their multi-mechanistic effect on activating the tumor ‘cold’ immune microenvironment. Herpes simplex virus 1, a naturally selective OV, is the most advanced virotherapeutic compound in clinical applications for use in combination with ICI. We here present the case of a 72 year-old patient with a heavily pre-treated, advanced maxillary sinus squamous cell cancer with distant metastases who developed complete response (CR) with only three administrations of a programmed death 1 inhibitor after treatment interference by a severe herpes zoster infection, based on the related alpha-herpesvirus varicella zoster virus (VZV). This exceptional response has been followed and confirmed with imaging studies over more than 5 years. Although the patient had several favorable predictors for response to immunotherapy, we reason that the exceptional response may in part be secondary to the serendipitous VZV infection. Documented cases of cancer patients that achieved CR after few administrations of treatment with ICI are rare, with most reporting follow up of just over 1 year or less. In this case, it is conceivable that the interference of the infection with VZV, soon after the start of immunotherapy with ICI, led to a lasting antitumor immunity and sustained CR. This hypothesis is supported by the concept of ‘oncolytic immunotherapy’ which is reviewed in this manuscript. In addition, persistence of a TP53 mutation found in a liquid biopsy, despite clinical and radiologic remission, is discussed.
Keywords
Introduction
Immunotherapy with immune checkpoint inhibitors (ICIs) emerged as a much-awaited breakthrough for the treatment of incurable, recurrent, and/or metastatic cancers, extending survival for previously terminal cancer patients. The expectations, nonetheless, have been tempered by the limited response rates to ICI treatment. Less than 20% of patients with advanced head and neck squamous cell carcinoma (HNSCC) respond to ICI. Studies have shown that cancers resistant to ICIs display low innate and adaptative immune responses within the tumor, with low CD8 T-cell numbers, low production of interferon, and often a low programmed death-ligand 1 (PD-L1) level, referred to as a ‘cold immune phenotype’.1,2 Substantial research efforts have explored strategies to activate the tumor immune environment transforming an immunologically non-reactive ‘cold’ tumor into a responsive ‘hot’ tumor. The utilization of oncolytic viruses (OV) is considered one of the most promising avenues to increase the efficacy of ICIs. Developed initially to exploit direct oncolytic effect, the oncolytic viral therapy is now recognized as a viral immunotherapy because of the multiple mechanisms of immune response activation amassed by the anticancer effect.
Anecdotal evidence of cancers regressing after viral infection dates back to the 1900s. For example, one well-known case describes a 42-year-old female with chronic myeloid leukemia who displayed a dramatic reduction in her white blood cell count after a flu-like illness. 3 We here present the case of a patient with metastatic HNSCC treated with pembrolizumab, who developed a sustained complete response (CR) after a severe herpes zoster infection, and review the concept of exploiting OVs as ‘oncolytic immunotherapy’ with the focus on the herpes simplex virus-1 (HSV-1) as the primary clinically utilized tumor-selective OV.
Case Presentation
A 72-year-old non-smoking African American woman, with no personal or family history of cancer, was diagnosed with squamous cell carcinoma of the right maxillary sinus in 2012 and was initially treated with transoral resection. The cancer recurred in 2015 and the patient underwent right total maxillectomy including resection of the right orbital floor with reconstruction, and right neck dissection. She was staged as pT3N0 with positive margins and perineural invasion. PD-L1 tested in the primary tumor by IHC (using Dako 22C3 pharmaDx antibodies) was 70% by tumor proportion score. Tumor DNA analysis by the FoundationOne platform (Foundation Medicine, Cambridge, MA, USA) measured a tumor mutation burden (TMB) of 9, two TP53 mutations and a BRCA1 mutation, among others (Figure 1(c)). Genetic evaluation was negative for any inherited genetic abnormalities.
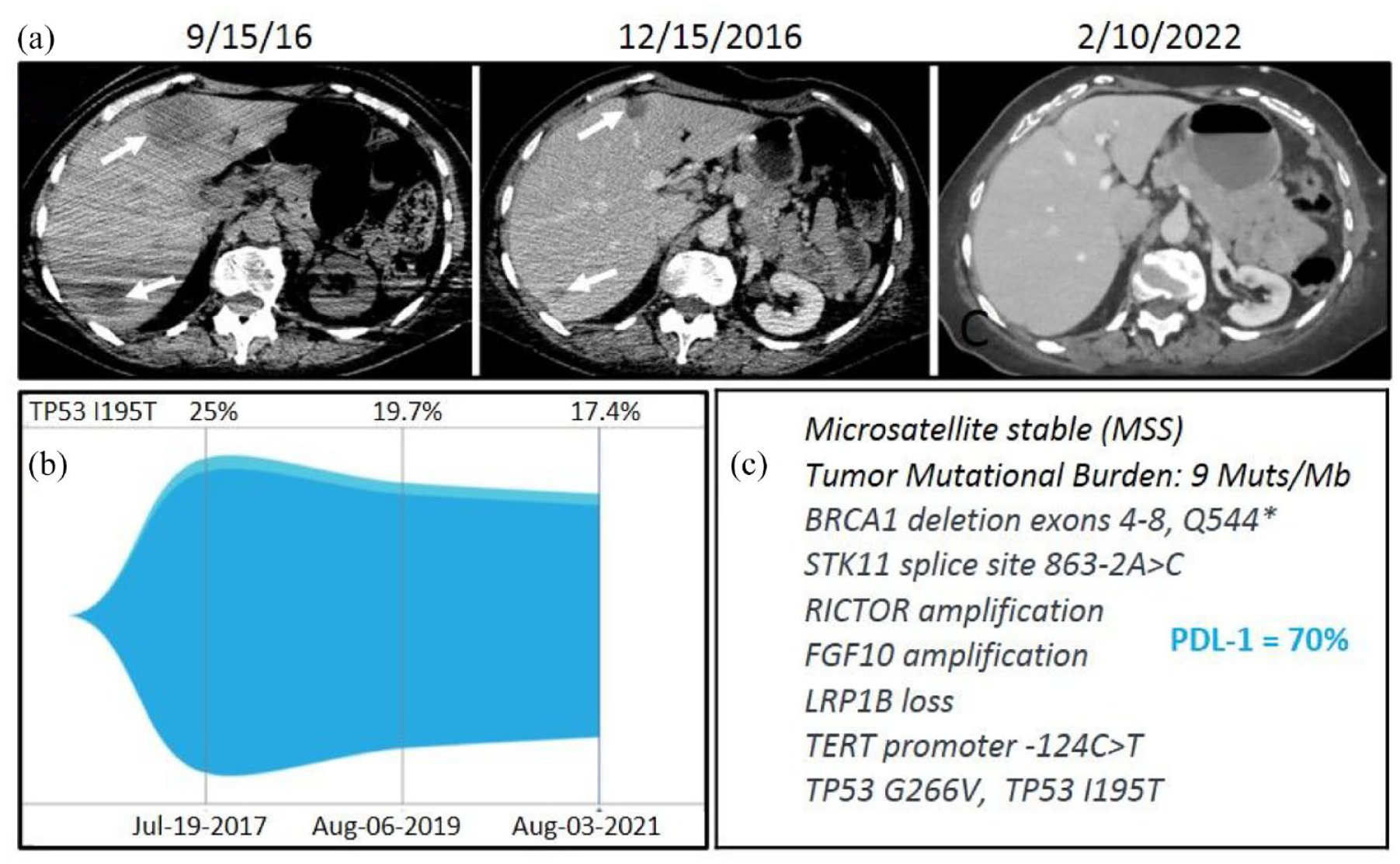
(a) Baseline (9/15/16) and 3-month follow-up (12/15/2016) CT of the abdomen demonstrate decrease in size of hepatic metastases (arrows) after three administrations of pembrolizumab. Subsequent follow-up CT acquired at 65 months (2/10/2022) demonstrates no measurable liver disease. (b) ctDNA monitored over time; (c) tDNA alterations and PD-L1 tested in primary tumor tissue.
Following surgery, she underwent adjuvant radiochemotherapy with 66 Gray and weekly cisplatin. Follow-up imaging demonstrated progression of metastatic cancer with lesions in the mediastinum, lung, and liver. The patient started palliative chemotherapy with weekly carboplatin and paclitaxel but progressed after 6 months with increased number and size of the metastases including a 3.5 cm mediastinal mass, a 3.8 cm left lower lobe (LLL) mass, and multiple liver masses measuring up to 5 cm (Figure 1A). Given her recurrent and metastatic status with progression on a platinum-based regimen, she was recommended palliative treatment with single-agent pembrolizumab (given at a dosage of 200 mg/m2 every 3 weeks) and began treatment in October 2016.
After the third administration of pembrolizumab, the patient presented to an outside hospital with a vesicular skin rash associated with severe neuropathic pain and pruritis of the left lower extremity from the thigh down to the shin in a L4-L5 dermatomal distribution. The patient was not vaccinated against herpes zoster virus (HZV). Given the typical clinical presentation (unilateral vesicular skin rash in a restricted dermatomal pattern associated with severe neuritis), the patient was diagnosed with herpes zoster infection and was prescribed valacyclovir. After 7 days of treatment, the skin lesions and pain continued leading to extension of valacyclovir treatment. Given the acute viral infection, pembrolizumab was held. The vesicles gradually improved, but the patient had persistent pain and ultimately developed new open wounds. She was admitted in the hospital where Infectious Disease and Dermatology services were consulted. A biopsy was performed, which was consistent with pyoderma gangrenosum. This was considered to be an isomorphic reaction related to the previous zoster infection. The patient was started on treatment with prednisone. She gradually recovered and prednisone was tapered over 2 months.
Follow-up computed tomography (CT) scans performed 1 month after the diagnosis of herpes zoster infection (going along with discontinuation of pembrolizumab application) showed improvement in all targeted metastatic lesions. At this time, the mediastinal mass measured 2.7 cm, the LLL mass was replaced with an area of consolidation, and the liver lesions sizes decreased with the largest now measuring 1.7 cm (Figure 1(a)). After another 4 months, the skin lesions healed, and plans were made to resume immunotherapy due to concerns for tumor progression during the long treatment break. Repeated imaging, however, demonstrated stable tumor disease, and as the patient was recovering with limited performance status, resumption of ICI treatment was paused in favor of close imaging monitoring.
Follow-up CT scans were obtained after another 3 months and demonstrated further decreased sizes of the lung and liver lesions and no measurable disease in the mediastinum or LLL. At this time, the largest liver lesion measured 1.1 cm. On this basis, the decision was made to continue active surveillance and resume treatment only upon progression. From then on, imaging was repeated every 3–4 months, and at the 1-year post-treatment scans a complete disappearance of mediastinal and liver lesions was observed, beyond that the residual LLL lesion was considered atelectatic.
In February 2019, concerns for recurrence in the LLL were raised due to the increase in size of the lung lesion with increased metabolic activity on a positron emission tomography scan. However, the patient still was completely asymptomatic. Two lung biopsies, one transbronchial and one transthoracic, were found to be completely negative for tumor cells; on the contrary, only signs of an acute inflammation (first biopsy) as well as a chronic inflammation (second biopsy) were detected. Further follow-up imaging showed that the lung lesion decreased in size to baseline, and the associated metabolic activity had resolved spontaneously. The patient remains in complete imaging remission to date, now 5-year post-treatment (Figure 1(a)). Circulating tumor mutations have been monitored using the Guardant360 platform (Guardant Health, Redwood City, CA, USA) over the last 4 years and the patient continues to present a circulating TP53 clone, although the percentage has been slowly decreasing (Figure 1(b)).
Discussion
This case illustrates an exceptional response to pembrolizumab. A patient with heavily pre-treated recurrent primary maxillary sinus SCC with extensive metastatic disease in the mediastinum, lungs, and liver, achieved a durable complete response (CR) after only three administrations of this ICI compound.
High PD-L1 expressed by the patient’s tumor is an established marker of response to ICIs. In addition, the intermediate level of the TMB and the mutations in TP53, BRCA1, LRP1B, and TERT promoter genes have been associated with increased responses to ICIs in different cancers.4–9 While this patient’s response to ICI may have been reflective of a perfect genomic storm, the probability that this is the sole determining factor does not find support in the literature. Few patients with recurrent/metastatic HNSCC have been reported to achieve CR in the clinical trials with single-agent ICI: pembrolizumab (Keynote 012 – eight of 192 patients 10 ; Keynote 055 – one of 171 patients 11 ; Keynote 040 – four of 247 patients 12 ; and Keynote 048 – six of 301 patients 13 ); nivolumab (Checkmate 141 – seven of 240 patients 14 ); and durvalumab (EAGLE – six of 240 patients 15 ; HAWK – one of 111 patients 16 ). While the number of ICI drug administrations for each patient is not specified in the published reports, there are no mentioned cases of patients achieving a durable CR with a limited number of treatment doses. There are several reports of patients who achieved complete pathologic response after 1–2 doses of ICI in the neoadjuvant setting (Ferris 17 ; Wise-Drapper 18 ; Upalluri 19 ; and Shoenfeld 20 ). In contrast to the case presented here, these reports include patients with early stage, therapy-naive HNSCC, who were treated with surgery after the administration of ICI, and, importantly, lacked reported outcome after long-term follow-up. An in-depth literature review revealed several cases with exceptional response to short duration treatment with ICIs. For example, a patient with recurrent and possibly metastatic adenoid cystic carcinoma, achieved radiologic CR sustained over 10 months after one administration of nivolumab with ipilimumab. 21 Another patient with extensive stage small-cell lung cancer achieved radiologic CR after two administrations of pembrolizumab, which was followed for 8 months. 22 Finally, a patient with metastatic bladder cancer achieved CR sustained over 1 year, after four administrations of sintilimab. 23 No comparable response regarding reports of cases with HNSCC were identified. In addition, the case presented here remains unique due to the long duration of sustained CR. We postulate that the severe intercurrent herpes zoster infection taking place while the patient was on immunotherapy, synergized with the ICI treatment resulting in this exceptional outcome. This hypothesis is supported by current clinical research efforts to exploit OVs, and especially HSV-based OVs, as antitumor immune-activating agents, able to amplify the immune response incited by ICIs. HSVs (HSV-1 and HSV-2) and varicella zoster virus (VZV) as the agent of herpes zoster infection, are members of the same family of alpha-herpesviruses and share a similar structure and pathogenic behavior. 24
As the diversity of cancer treatment modalities continues to expand, the emerging application of oncolytic virotherapy, with more than 200 OVs currently under investigation, is anticipated to play an important role in cancer eradication. Combining OVs with ICIs piques the highest interest. Immunotherapy has recently challenged the concept of ‘terminal cancer’ by significantly extending survival. Despite this, the limitation in the response rate is disappointing, triggering efforts to inflame the ‘immune cold’ phenotype. Now considered as ‘oncolytic immunotherapy’ or ‘immunovirotherapy’ agents, OVs are no longer utilized as simple oncolytic agents. Instead, OVs are immune stimulating drivers that can enhance the tumor microenvironment (TME) immune behavior, thereby theoretically leading to synergy with ICIs and subsequent tumor eradication. 25 Like immunotherapy, selective OVs are tumor agnostic. They are considered clever and versatile anticancer weapons that utilize direct oncolytic and indirect immunogenic strategies to attack tumor tissue. 26 Clinically graded OVs selectively replicate in cancer cells. Wild-type viruses exploit oncogenic defects in the antivirus interferon, tumor necrosis factor, other cytokine pathways, and translational regulation, while normal cells that lack such defects are spared.27,28 Further specificity can be added by engineering viral inserts to target receptors specific to cancer cells. 27 The resulting viral oncolysis is considered an immunogenic cell death. Infected cell death releases tumor antigens, viral antigens, and damage-associated molecular patterns in the TME triggering a strong innate and adaptive immune response not only inside the primary addressed tumor site, but also systemically.1,26,27 Indeed, the intra-tumoral activation of tumor-specific immune response has the potential to travel to uninfected tumors and to synergize with systemic immunotherapy in eradicating metastatic cancers. 29 This immune response, in addition to release of cascading inflammatory cytokines, significantly change the TME. This change increases tumor vulnerability to activated effector immune cells. In addition, some OVs trigger immunosuppressive PD-L1 production, 27 while other OVs carry inserts that express immune-enhancing molecules such as granulocyte-macrophage colony-stimulating factor (GM-CSF) and interleukins, adding more layers of immunogenic effects.27,29
Although an adenovirus was the first OV graded for clinical testing, clinical oncolytic immunotherapy is currently dominated by the HSV variants, and especially the clinically graded HSV-1. As an OV, HSV-1 has several advantages. It has a well-described structure and life cycle and high genomic stability. It has a rapid life cycle that favors efficient oncolysis before antivirus mechanisms fully develop, which supports adequate production for clinical use. 30 HSV-1 infects a wide variety of cancer cell types through increased expression of multiple receptors including herpesvirus entry mediator and nectin-1. 27 Its oncolytic activity exploits the oncogenically modified interferon and protein kinase R pathways that protect normal cells. 31 Recombinant variants allow incorporation of large therapeutic transgenes as well as modification or deletion of HSV’s neurotropic glycoproteins, to enhance the safety, efficacy, and selective oncolysis. Novel recombinant oncolytic HSV-1 virotherapeutics have also demonstrated the ability to induce significant alterations in the amount and distribution of infiltrating immune cells, as well as circulating immune cells, by exerting positive antitumor immune responses.30,32 Intralesional injection of a recombinant HSV-1 in patients with melanoma significantly impacted the TME by decreasing the concentration of regulatory T cells, T-suppressor cells, and myeloid-derived suppressor cells and increasing melanoma antigen recognized by T-cells 1 (MART-1)-specific CD8+ T-cell infiltration and the concentration of cytotoxic T cells in the peripheral blood, thereby suggesting a systemic antitumor immunity activation. 34 In a phase I study, an increase in the cytotoxic CD8+ T cell infiltration in the tumor TME was observed after the administration of the HSV-1 virotherapy in combination with an anti-PD-1 antibody. 1 These findings suggest that recombinant oncolytic HSV-1 virotherapeutics can improve the efficacy of ICIs when combined, and that similar mechanisms could work in the context of natural infection with wild-type HSV-1, as observed in our patient.
Talimogene laherparepvec (T-VEC) is the first OV approved in United States and Europe for intra-tumoral administration in patients with inoperable melanoma. This modified HSV-1 viral vector has two viral genes deleted, one to enhance viral safety (ICP34.5, the herpes virus neurovirulence factor gene, non-essential for viral replication but critical for the neurotropism) and the other to enhance viral efficacy (ICP47 gene that plays a role in reducing virally mediated suppression of antigen presentation). Furthermore, through the engineered expression of GM-CSF, T-VEC enhances antitumor immune activation by promoting stem cell differentiation into immune cells in the TME. 28 A second recombinant HSV-1, Teserpaturev, triple-mutated to eliminate neurovirulence and to enhance specific antitumor immunity, has recently received conditional approval in Japan for the treatment of patients with malignant glioma. 35
HSV-1, like other OV, has shown limited anticancer efficacy as monotherapy, with rare cases of durable response. 30 T-VEC was the first oncolytic immunotherapy to be evaluated in a phase III clinical trial in melanoma patients. This trial demonstrated a durable response rate of 16.3%, an overall response rate of 26.4%, and medial overall survival of 23.3 months. These results are similar to studies in which treatment is pursued with single agent ICI. 36 The rationale for synergism between HSV ‘oncolytic immunotherapy’ and ICI has compelled further studies dedicated to investigating the safety and efficacy of a combined approach. Combined treatment with virotherapy and ICI has been tested in preclinical models with promising results.37–39 A phase II randomized clinical trial of T-VEC combined with the cytotoxic T-lymphocyte-associated antigen-4 inhibitor ipilimumab is the only published study and focused on a population of patients with unresectable melanoma. This study confirmed expected clinical and tissue results, with objective response significantly higher in the combination arm (39%) comparative with single agent ICI (18%) without additional safety concerns. 40 T-VEC combined with pembrolizumab is being investigated in the phase Ib-III Masterkey clinical studies with reported overall response rate of 67% and CR of 43%, with a median follow-up of 36.8 months, in the 21 patients enrolled in the Phase Ib portion.35,41 Clinical trials are ongoing with several HSV-based OVs and PD-1 inhibitors (Table 1). The case presented here makes a compelling argument for anticipating positive outcomes. Interestingly, the optimal sequence of the combination has been an important topic of research. Preclinical models suggest that the timing of the OV and ICI administration affects the results, and the most promising sequence is hypothesized to be an OV lead-in followed by concurrent therapy with ICI. 42 The presented case of exceptional serendipitous success, with a natural viral infection by VZV intervening after three administrations of pembrolizumab and followed by no further treatment, argues for consideration of other scenarios and ultimately a possible personalized approach guided by immune markers. Another interesting aspect of the presented case is the persistent circulating TP53 mutation despite apparent clinical and radiologic CR, raising question about a residual tumor (possibly in the persistent LLL atelectatic area) that is kept in check by a durable immune activation. ‘Functional cure’ with long-term duration of disease control secondary to sustained immune activation, 43 in our case postulated to be triggered by the infection with HZV, might become a common scenario following the emergence and application of results of ongoing OV and ICI combination clinical trials. Alternatively, tumor senescence reported to be triggered by immunotherapy 44 or by viruses45,46 could explain a ‘dormant tumor’ clinical presentation, but still able to release tumor cell DNA mutations into the circulation.
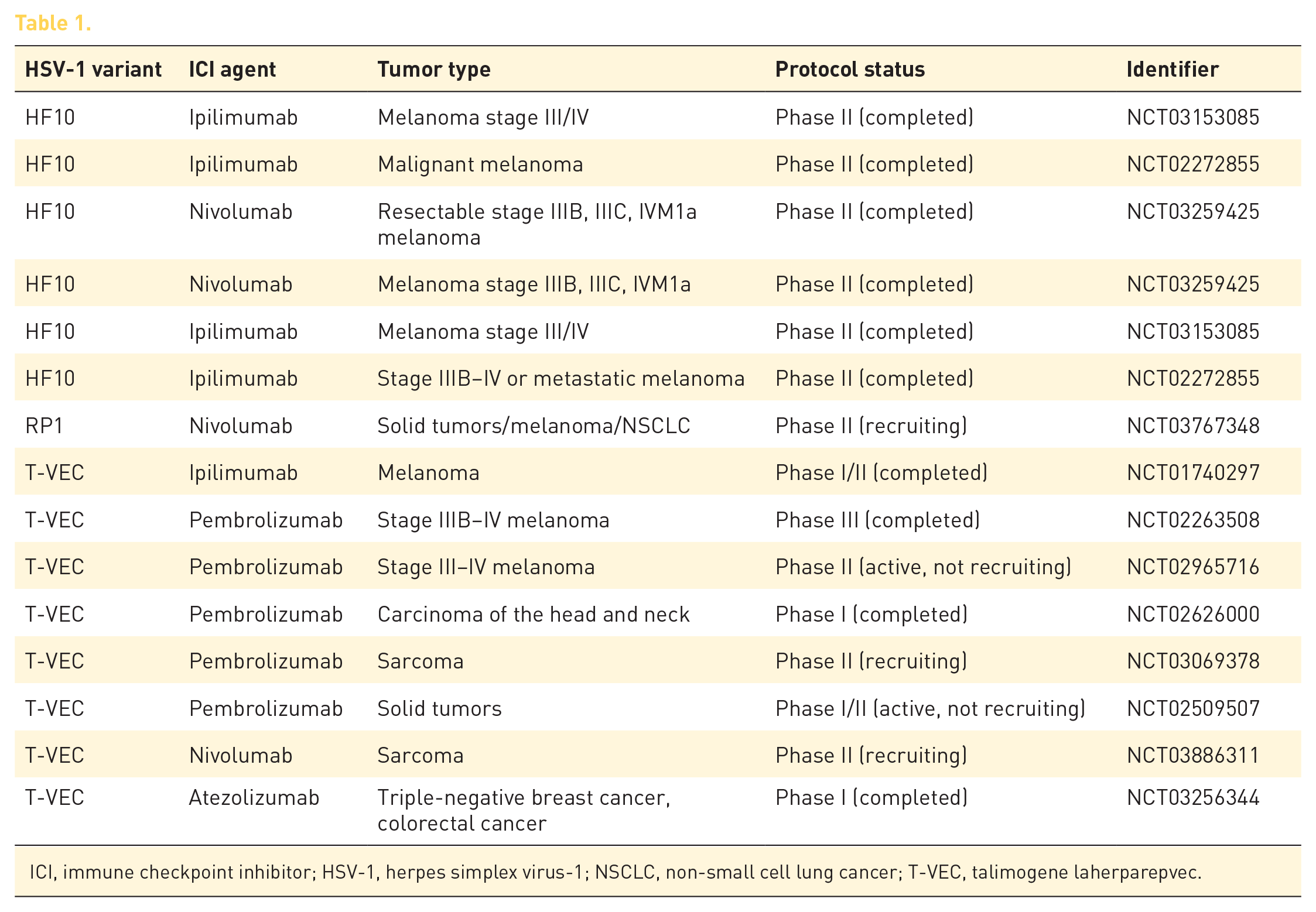
ICI, immune checkpoint inhibitor; HSV-1, herpes simplex virus-1; NSCLC, non-small cell lung cancer; T-VEC, talimogene laherparepvec.
Overall, the evidence of association between the herpes zoster infection and exceptional tumor response to pembrolizumab in the presented case is feeble. However, it does support preclinical evidence and ongoing clinical evaluation of synergism between OVs and ICIs in cancer control.
Conclusions
Our case of exceptional response to pembrolizumab in the setting of a severe natural herpes zoster infection relates to the rationale, research efforts, and growing body of literature supporting expansion of immunotherapy to include OVs, and the utility of combining ICIs with OVs. Additional topics of interest such as the schedule of combined regimens and non-standard outcomes are raised by the discussions of this case.