
Abstract
Background:
Liquid biopsy (LB) can detect actionable genomic alterations in plasma circulating tumor circulating tumor DNA beyond tissue testing (TT) alone in advanced non-small cell lung cancer (NSCLC) patients. We estimated the cost-effectiveness of adding LB to TT in the Canadian healthcare system.
Methods:
A cost-effectiveness analysis was conducted using a decision analytic Markov model from the Canadian public payer (Ontario) perspective and a 2-year time horizon in patients with treatment-naïve stage IV non-squamous NSCLC and ⩽10 pack-year smoking history. LB was performed using the comprehensive genomic profiling Guardant360™ assay. Standard of care TT for each participating institution was performed. Costs and outcomes of molecular testing by LB + TT were compared to TT alone. Transition probabilities were calculated from the VALUE trial (NCT03576937). Sensitivity analyses were undertaken to assess uncertainty in the model.
Results:
Use of LB + TT identified actionable alterations in more patients, 68.5 versus 52.7% with TT alone. Use of the LB + TT strategy resulted in an incremental cost savings of $3065 CAD per patient (95% CI, 2195–3945) and a gain in quality-adjusted life-years of 0.02 (95% CI, 0.01–0.02) versus TT alone. More patients received chemo-immunotherapy based on TT with higher overall costs, whereas more patients received targeted therapy based on LB + TT with net cost savings. Major drivers of cost-effectiveness were drug acquisition costs and prevalence of actionable alterations.
Conclusion:
The addition of LB to TT as initial molecular testing of clinically selected patients with advanced NSCLC did not increase system costs and led to more patients receiving appropriate targeted therapy.
Introduction
Personalized medicine has greatly impacted the management of advanced non-small cell lung cancer (NSCLC). The increasing number of actionable genomic alterations seen in advanced NSCLC has fostered the development of multiple targeted therapy options for these patients. 1 In order to guide treatment decision-making, routine testing for actionable alterations is now standard of care in patients with advanced NSCLC. Genomic testing using broad-based methods can comprehensively assess oncogenic targets, and a multigene next-generation sequencing (NGS) approach is increasingly recommended. 2 Tumor tissue has been the traditional biospecimen used for molecular analyses. However, tumor tissue limitations include inadequate tissue for comprehensive genomic profiling, inaccessible tumors, and tumor spatial and temporal heterogeneity in patients with progressive disease. 3
Liquid biopsy (LB) performs molecular profiling on circulating tumor DNA (ctDNA) and is emerging as a complementary approach to tissue biopsy for therapeutic decision-making. Due to its non-invasive nature and faster turnaround time, LB can overcome problems with tissue availability and accessibility. 3 It can also be the favored approach for gathering information on emerging resistance mechanisms in pretreated patients.
In advanced NSCLC, use of a comprehensive LB that identifies all guideline-recommended genomic targets can identify a greater number of patients eligible for targeted therapy. We previously reported that actionable targets were detected in 58% of advanced NSCLC patients using LB profiling, compared to 52% using standard tumor tissue profiling. 4 Despite the known benefits of LB, test cost is perceived as an added cost, limiting its widespread implementation. While clinical outcomes from the VALUE trial have been reported separately, 4 we also assessed the cost-effectiveness using LB in addition to standard tumor tissue profiling in clinically selected patients with newly diagnosed advanced NSCLC from the perspective of the Canadian public healthcare system.
Methods
Economic model structure and inputs
A decision analytic model was developed using TreeAge Pro 2022 (Williamstown, MA) to compare testing and treatment costs and quality-adjusted life-years (QALYs) of two strategies: LB added to TT versus standard of care TT alone (Figure 1). The target population was the VALUE study patients (see inclusion criteria below). Analysis was performed from the government payer perspective of the Canadian publically funded healthcare system, and the time horizon used was 2 years.

(a) Decision tree.
The TT alone strategy tested for actionable alterations exclusively through tissue specimens using institutional standard biopsy procedures and molecular pathology. Profiling methods used in VALUE patients included TruSight Tumor 15™ gene panel (TST15), single gene immunohistochemistry (IHC) for ALK and programmed death-ligand 1 (PD-L1) and fluorescent in situ hybridization, extended NGS panels, and partial gene panels (restriction fragment length polymorphism). Since the majority of VALUE patients got TST15 or single-gene IHC testing, TST15 sensitivity and specificity was used for the model inputs (94 and 99%, 5 respectively). It was estimated that 13% of initial biopsies required repeat biopsy based on previous data in patients with advanced NSCLC. 6 LB NGS was performed on ctDNA samples using the Guardant360™ platform, with a published sensitivity of 86% and specificity of 98.5%. 7 Other clinical inputs for the model were informed by the VALUE study, including the prevalence of actionable alterations identified by TT and LB.
VALUE study design
The VALUE study (NCT03576937) included 146 patients with advanced (incurable stage IIIB or IV), histologically proven, non-squamous NSCLC who were never- or light-smokers (⩽10 pack year smoking history) and were being considered for systemic therapy in the first-line setting at six Canadian cancer centers. 8 Patients underwent peripheral blood sampling for GUARDANT360™ testing which includes all currently actionable alterations in NSCLC including mutations, fusions, and copy number variations. Tumor tissue testing for genomic abnormalities was also performed in all patients as per institutional standard of care in a certified laboratory in Canada. Clinical results of the study have been presented elsewhere. 8
Overall survival (OS) and progression-free survival (PFS) with targeted therapy compared to non-targeted therapy (i.e. chemo-immunotherapy) were calculated from start of treatment, or treatment decision date for patients who received best supportive care (BSC). PFS was measured according to RECISTv1.1 9 by study investigators.
Costs of testing and treatment
All treatment costs used in the model are shown in Table 1. Targeted therapy was modeled as first-line osimertinib 80 mg orally daily if an activating EGFR mutation was detected, first-line alectinib 600 mg orally twice per day for ALK fusions, or first-line crizotinib 250 mg orally twice per day for ROS1 fusions. Costs of non-standard targeted therapies such as entrectinib and trastuzumab deruxtecan were also considered (Table 1). Final targeted therapy cost used in the model was calculated by averaging each of the above targeted therapy costs by the percentage of VALUE patients who received each therapy. In the model, patients without actionable alterations detected in tumor would receive first-line chemo-immunotherapy with carboplatin, pemetrexed, and pembrolizumab. This reflects current Canadian practice in advanced lung cancer patients with no or minimal smoking history, for whom chemo-immunotherapy is preferred over anti-PD-1 monotherapy even in those with high PD-L1 tumor expression levels. In the VALUE study, 9.6% of patients did not receive any therapy, and only received BSC. 8 Cost of BSC was determined through the literature and by estimating that 50% of BSC patients died at home and the remaining 50% of patients died in hospital.10,11
Costs and utility model inputs. Costs are valued in 2022 $CAD.
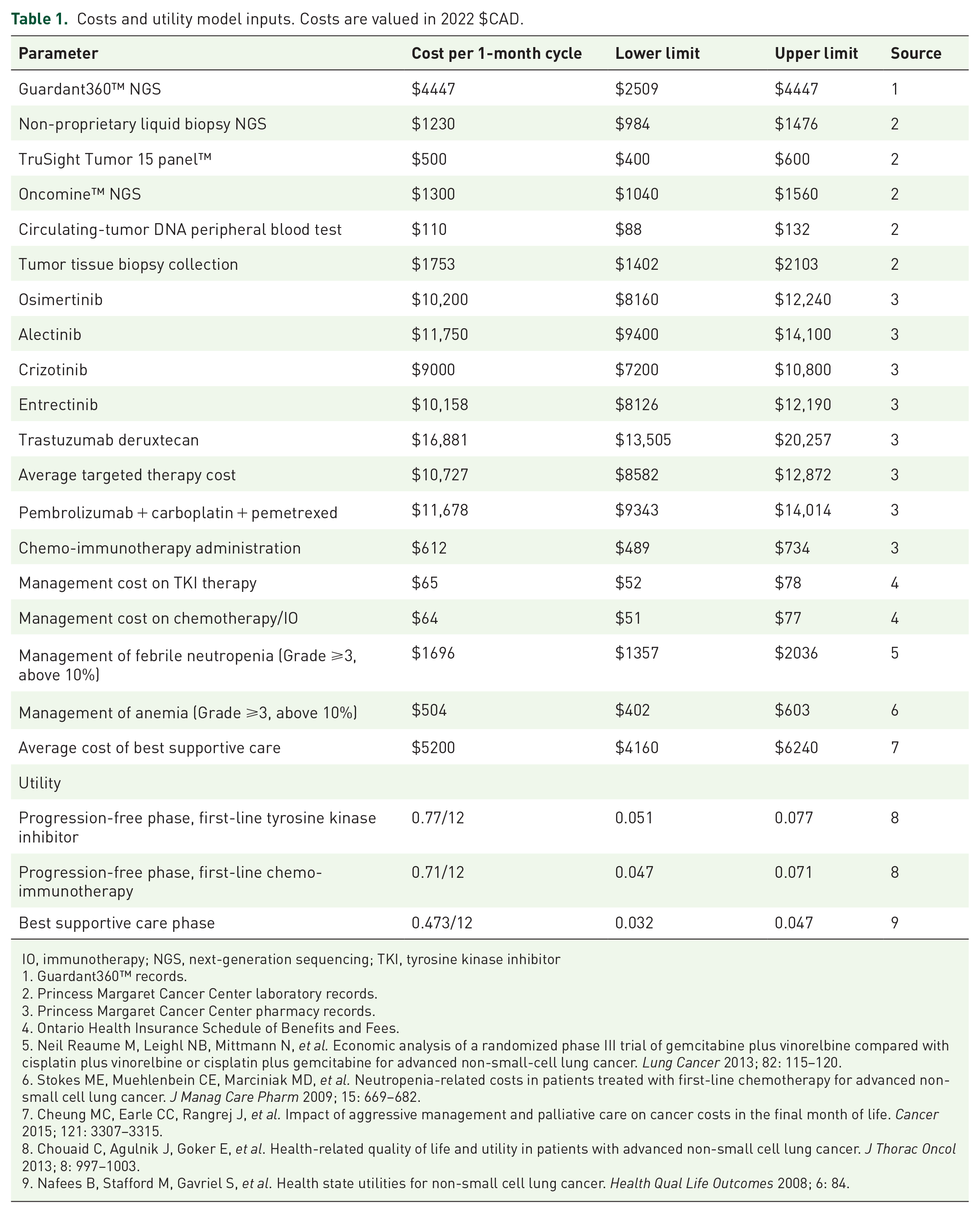
IO, immunotherapy; NGS, next-generation sequencing; TKI, tyrosine kinase inhibitor
1. Guardant360™ records.
2. Princess Margaret Cancer Center laboratory records.
3. Princess Margaret Cancer Center pharmacy records.
4. Ontario Health Insurance Schedule of Benefits and Fees.
5. Neil Reaume M, Leighl NB, Mittmann N, et al. Economic analysis of a randomized phase III trial of gemcitabine plus vinorelbine compared with cisplatin plus vinorelbine or cisplatin plus gemcitabine for advanced non-small-cell lung cancer. Lung Cancer 2013; 82: 115–120.
6. Stokes ME, Muehlenbein CE, Marciniak MD, et al. Neutropenia-related costs in patients treated with first-line chemotherapy for advanced non-small cell lung cancer. J Manag Care Pharm 2009; 15: 669–682.
7. Cheung MC, Earle CC, Rangrej J, et al. Impact of aggressive management and palliative care on cancer costs in the final month of life. Cancer 2015; 121: 3307–3315.
8. Chouaid C, Agulnik J, Goker E, et al. Health-related quality of life and utility in patients with advanced non-small cell lung cancer. J Thorac Oncol 2013; 8: 997–1003.
9. Nafees B, Stafford M, Gavriel S, et al. Health state utilities for non-small cell lung cancer. Health Qual Life Outcomes 2008; 6: 84.
Direct costs include the cost of disease management, treatment-related costs (pharmacy drug preparation, chemotherapy nursing administration, and chemotherapy daycare overhead costs), and cost of terminal care. Direct testing costs include cost of Guardant360™ NGS, cost of TST15 panel, cost of ctDNA peripheral blood test, and cost of TT collection. Testing costs were obtained from the Princess Margaret Cancer Centre (PMCC) pathology department. Drug acquisition costs for tyrosine kinase inhibitors (TKIs) and chemo-immunotherapy were obtained from the PMCC pharmacy, Canadian Agency for Drugs and Technologies in Health (CADTH) pan-Canadian Oncology Drug Review (pCODR). 12 Doctors’ fees, outpatient monitoring, and diagnostic testing costs (laboratory tests and imaging) were obtained from the Ontario Health Insurance Schedule of Benefits and Fees. 13 All costs and utilities were discounted at a rate of 1.5% per year as per CADTH guidelines. 14 All costs are presented in 2022 Canadian (CAD) dollars.
For chemo-immunotherapy, cost of febrile neutropenia and anemia was considered because Common Terminology Criteria for Adverse Events (CTCAE) grade ⩾3 events occurred in >10% in Keynote-189 patients, the landmark trial establishing chemo-immunotherapy as standard first-line treatment in advanced NSCLC with no actionable alterations. 15 Toxicity costs included clinic and hospital overhead costs, nursing time, physician fees, laboratory test costs, drug and supplies costs, and toxicity-specific direct costs (e.g. unit of packed red blood cells and granulocyte colony stimulating factor). BSC costs were applied to each patient entering the death state and were informed by the literature.10,11,16
Model probabilities and utilities
A Markov model was constructed to reflect the natural history of advanced NSCLC. Only first-line therapies were considered in the model due to the lack of standardization of therapy options post chemo-immunotherapy and post-osimertinib at the time of the study. During each 1-month cycle, patients cycled through the first-line therapy or progressed to death. BSC patients cycled through BSC or progressed to death. Health benefits were expressed as life-years and QALYs gained. A 2-year time horizon was used for the model because only first-line therapies were considered.
Transition probabilities were assigned to both strategies to estimate how patients progressed through the model. Individual patient data were generated from the Kaplan-Meier curves of OS from the VALUE trial. The probability of death was modeled with extrapolations based on exponential (targeted therapy), Weibull (chemo-immunotherapy), and log-normal (BSC) distributions. Distributions for OS were selected based on visual inspection and statistical goodness-of-fit, according to Akaike’s information criterion. Patients who transitioned out of the living state were assumed to have died.
Utility scores were derived from a mixed-model regression analysis for patients with advanced NSCLC undergoing the first-line TKI-targeted therapy in the progression-free state, and patients undergoing the first-line chemo-immunotherapy (Table 1).17,18
Sensitivity analyses
Model parameters were varied using one-way deterministic sensitivity and probabilistic (10,000 simulations) analyses to assess uncertainty in the model. For the one-way sensitivity analysis, the 95% upper and lower confidence intervals were used, when available. If unavailable, ±20% of base case values were used. The discount rate was varied from 1.5 to 5% per year. Unit costs of lab tests, physician visits, and imaging were obtained from the Ontario Health Insurance Plan fee schedule and thus, were considered to be fixed costs. Probabilistic sensitivity analysis (PSA) was performed by defining distributions for key parameters in the model that were not known with certainty (Supplemental Appendix). The key parameters included in the PSA were drug acquisition costs and utilities. Scenario analysis was conducted using Oncomine NGS™ for tissue profiling.
Results
The clinical results of the VALUE study have been previously presented and are summarized again here. 8 From February 13, 2019 to July 21, 2020, 146 patients that were light or never smokers with advanced lung non-squamous NSCLC were enrolled. The median age of study participants was 64, 64% were female, 80% had no prior history of smoking, and 78% had ECOG performance status ⩽1. 8 Actionable alterations were identified in 68.5% of patients using the LB plus TT approach, and 52.7% using standard TT alone. The majority of actionable alterations detected were EGFR sensitizing mutations or ALK fusions using both approaches (47% using the LB + TT approach, and 40% using the TT alone approach). The other alterations detected were EGFR exon 20 ins/dup mutations, KRASG12C, METex14 skip mutations, NRG-1 and ROS-1 fusions.
Costs, QALYs, and incremental cost
The LB + TT approach was associated with a cost savings of $3065 per patient (95% CI, 2195–3945) and a gain in QALYs of 0.02 (95% CI, 0.01–0.02) compared to the TT alone approach. Total 2-year cost of the LB + TT approach was $240,998, and $244,063 for the TT alone approach. Testing costs comprised 2.4% of total costs in the LB + TT strategy ($5890), and 1.0% of the TT alone strategy ($2390).
Costs due to chemo-immunotherapy were higher using the TT alone strategy, while costs due to targeted therapy were higher using the LB + TT strategy (Figure 2). Average cost of chemo-immunotherapy and targeted therapy were $123,906 and $107,184 respectively in the TT alone approach, and $77,564 and $147,254 in the LB + TT approach.

Cost of tissue plus liquid biopsy compared to cost of tissue biopsy alone. Costs in 2022 $CAD.
Sensitivity and scenario analysis
One-way sensitivity analyses showed that the model was most sensitive to variations in the cost of chemo-immunotherapy and targeted therapy, and prevalence of actionable alterations (tornado plot, Figure 3). Incremental cost results ranged from a cost savings of $12,333 to a cost increase of $6203, across a range of one-way sensitivity analyses. The most influential parameter in the incremental cost variation was the cost of chemo-immunotherapy.

Incremental cost tornado diagram. Costs and utilities are monthly, and costs are in valued in 2022 $CAD. BSC, best supportive care; chemoIO, chemo-immunotherapy; PF, progression-free; TST15, TruSight Tumor 15 panelTM. Note: a negative incremental cost indicates a cost savings (LB + TT less costly than TT alone); a positive incremental cost indicates a cost increase (LB + TT more costly than TT alone).
In most scenarios, cost of LB + TT was lower than TT alone and thus, there was a cost savings. Cost of the LB + TT approach was higher in scenarios where the cost of chemo-immunotherapy and targeted therapy were higher, and when the prevalence of actionable alterations detected by LB + TT was higher. For example, at the upper limits of the monthly chemo-immunotherapy and targeted therapy costs of $14,825 and $12,872, the LB + TT approach was more costly and incremental cost was $6203 and $4660, respectively (Supplemental Appendix). At the lower limits of the monthly chemo-immunotherapy and targeted therapy costs of $9883 and $8581, the LB + TT approach was less costly and incremental cost was −$12,333 and −$11,273, respectively.
One-way sensitivity analysis for the cost of chemo-immunotherapy shows that as the cost of chemo-immunotherapy rises, the incremental cost associated with the LB + TT approach (i.e. cost of LB + TT minus cost of TT alone) remains low and hits a nadir (Figure 4). The incremental cost associated with the TT approach (i.e. cost of TT alone minus LB + TT) rises as the cost of chemo-immunotherapy increases.

One-way sensitivity analysis of cost of chemo-immunotherapy. Costs are monthly costs in 2022 $CAD. cChemoIO, cost of chemo-immunotherapy; Bx, biopsy.
Scenario analysis was conducted using Oncomine NGS™ for the tissue profiling. In this scenario, the LB + TT approach was associated with a cost savings of $2665 per patient (95% CI, 1848–3478) and a gain in QALYs of 0.02 (95% CI, 0.01–0.02) compared to the TT alone approach. Total 2-year cost of the LB + TT approach was $241,709, and $244,375 for the TT alone approach. Testing costs comprised 2.7% of total costs in the LB + TT strategy ($6594), and 1.3% of the TT alone strategy ($3064).
Discussion
Economic analysis of this multi-center, prospective cohort study showed that in a clinically selected population of advanced non-squamous NSCLC patients with never or light smoking history, LB in addition to tissue biopsy results in healthcare system cost savings of $3065 per patient compared to tissue biopsy alone. Increased detection of actionable alterations using LB was also associated with more patients being treated with targeted therapy. These results remained robust across plausible ranges of model inputs. To our knowledge, this is the first evaluation of the overall cost-effectiveness of adding comprehensive LB testing to the initial diagnosis of advanced NSCLC using a clinical trial designed to inform model inputs.
Dramatic advances in NSCLC have occurred largely due to the increasing number of targetable oncogene drivers.19,20 Plasma-based NGS will have an increasing footprint in personalized medicine due to its shorter turnaround time and reduced invasiveness. Pennell et al. 21 previously demonstrated the economic value of upfront tumor tissue NGS in patients with advanced NSCLC. In their analysis, upfront NGS was associated with substantial cost savings in comparison to hotspot panels or other more stepwise approaches to detecting actionable alterations. Our study compared plasma-based NGS to a hotspot panel performed on TT specimens. The findings further affirm the added value of NGS for furthering precision medicine in the advanced NSCLC population. Furthermore, the results here support LB NGS as a minimally invasive option for individualizing therapy in advanced NSCLC patients, whereas saving healthcare system dollars. Consideration of a blood-first testing paradigm could also potentially reduce costs of testing and procedures by limiting redundant tissue testing in cases where LB testing has already identified an actionable alteration. Detection of actionable alterations by plasma genotyping is susceptible to variables that limit shedding of tumor DNA, and a risk of false negatives can affect clinical decision-making.22–24 It is recommended that a LB test negative for oncogenic driver alterations, especially with variants at low allele fractions, be followed by a comprehensive tissue test. 25 While tissue biopsy will remain an integral part of cancer histopathological diagnosis, the overall cost-effective approach will incorporate comprehensive LB testing into the diagnostic algorithm.
Our study results demonstrate that the majority of costs from the TT alone approach were due to drug acquisition costs for chemo-immunotherapy. Genomic profiling testing costs comprised only 1.0% of overall costs in the TT alone arm. With the addition of LB costs, testing costs were still only 2.4% of the LB + TT approach. The major drivers in the overall cost-effectiveness profile were drug acquisition costs, and costs of chemo-immunotherapy exceeded targeted therapy costs. Prior data in advanced lung adenocarcinoma shows that personalized medicine becomes more cost-effective as the cost of non-targeted therapy increases. 26 Thus, as the cost of chemo-immunotherapy rises in our sensitivity analyses, it is not surprising that the LB + TT approach becomes more favorable.
The primary VALUE study limitation is that we clinically selected non-squamous NSCLC patients who had never smoked or had minimal smoking history, a group that has a higher prevalence of actionable alterations. Prior data in screening show that screening a highly enriched population is more cost-effective than screening an unselected population. 27 The drawback is that the same enrichment may miss some true positives within the unscreened group. To circumvent this, cheaper screening tests may make the cost-effectiveness profile more favorable if the reductions in testing costs balance the negative effects of the true positives that were missed. We explored the economic impact of various LB test costs in our model, and cost-effectiveness results continue to support the value of LB below costs of $5000.
Our results need to be interpreted within the context of modeling assumptions. Our model assumed that all patients had tissue profiling using a hotspot panel (TST15), although NGS and a variety of other tissue profiling methods were used at the different centers participating in the VALUE study. Scenario analysis assuming the use of NGS for tissue profiling preserved the cost savings and further affirms the cost saving effect of adding LB. Due to wide variability in options for subsequent therapies, we modeled first-line therapies only and the 2-year time horizon minimized potential overestimation of first-line treatment costs. Although patients who initially received first-line targeted therapy may be treated with the more costly chemo-immunotherapy beyond the 2-year time horizon, this would be a much smaller subset of patients. Chemo-immunotherapy was used in our model for patients without actionable alterations, but our findings would be similar if we used anti-PD-1 monotherapy instead for those with high tumor PD-L1 expression, as immunotherapy was by far the most expensive component of treatment. Our model did not take biopsy complication rates into consideration. Assuming that the TT alone approach would more readily perform biopsies and re-biopsies for molecular profiling, consideration of biopsy complication rates would increase the cost of the TT alone approach and strengthen the value of LB + TT even further. Finally, all drug treatments and costs were derived from Canadian sources and thus, caution must be used when generalizing to other markets.
Conclusion
In conclusion, our analysis showed that genomic profiling with LB in addition to tissue biopsy does not increase healthcare system costs. Although our analysis looked at the concurrent approach of performing LB in patients who already had a tissue diagnosis, several studies are already examining the impact of a plasma-first strategy,28,29 as well as its cost-effectiveness. 30 This may be preferred for patients in whom obtaining a tissue biopsy is too risky or difficult and may accelerate genomic testing and treatment initiation. However, it is important to recall that a plasma-first approach does not obviate the need for TT for pathologic diagnosis and studies such as PD-L1 expression. In our study, the majority of cost savings resulted from the larger proportion of patients who received targeted therapy with LB, reducing costs associated with the inappropriate use of costly chemo-immunotherapy. The main benefit of LB is that it increases the chances of patients receiving the most appropriate treatment. These results support the value of implementing LB in our study population, and further analysis in a cohort of all advanced NSCLC patients is warranted. Through this approach, timely initiation of molecularly guided therapy can improve patient outcomes without increasing system costs.
Supplemental Material
sj-docx-1-tam-10.1177_17588359221112696 – Supplemental material for The economic value of liquid biopsy for genomic profiling in advanced non-small cell lung cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359221112696 for The economic value of liquid biopsy for genomic profiling in advanced non-small cell lung cancer by Doreen A. Ezeife, Eldon Spackman, Rosalyn A. Juergens, Janessa J. Laskin, Jason S. Agulnik, Desiree Hao, Scott A. Laurie, Jennifer H. Law, Lisa W. Le, Lesli A. Kiedrowski, Barbara Melosky, Frances A. Shepherd, Victor Cohen, Paul Wheatley-Price, Rachel Vandermeer, Janice J. Li, Roxanne Fernandes, Aria Shokoohi, Richard B. Lanman and Natasha B. Leighl in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.