
Abstract
Background:
The response rate to sorafenib is limited for unresectable hepatocellular carcinoma (HCC). Little is known about the long-term outcomes of objective responders. The role of second-line therapies on the survival of sorafenib-responders is unclear. We aimed to delineate the long-term outcomes and the role of subsequent treatment after responding to sorafenib.
Methods:
From September 2012 to December 2019, 922 patients who received sorafenib treatment for unresectable HCC were retrospectively reviewed. Of these, 21 (2.3%) achieved a complete response (CR) and 54 (5.9%) had a partial response (PR) based on mRECIST criteria. Factors associated with survivals were analyzed.
Results:
During the median follow-up of 35.3 months, the median duration of response was 18.3 months (range: 2.3–45.5) for patients achieving CR and 10.0 months (range: 1.9–60.3) for PR. The median overall survival (OS) was 39.5 months [95% confidence interval (CI): 28.4–50.5] including values not yet estimable for CR and 25.8 months for PR. Patients who experienced treatment-related adverse events (TRAEs) had better median OS than those without (44.9 versus 18.1 months, p = 0.003). Eventually, 53 patients developed tumor progression; 30 patients received second-line systemic treatment including nivolumab (n = 8), regorafenib (n = 15), and chemotherapy (n = 7). Sorafenib–nivolumab sequential therapy provided the best median OS versus sorafenib–regorafenib and sorafenib–chemotherapy in these patients (55.8, 39.5, and 25.5 months), respectively.
Conclusions:
The response is durable for advanced HCC patients with CR or PR to sorafenib. Subsequent immunotherapy seems to provide the best survival. This information is important for characterizing outcomes of sorafenib-responders and the choice of sequential treatment.
Introduction
Hepatocellular carcinoma (HCC) is the sixth most common cancer and the fourth leading cause of cancer-related death worldwide. 1 HCC is most prevalent in East Asia and Africa, which are endemic areas of chronic viral hepatitis B and C. However, the incidence and mortality rates are rapidly rising in the United States and Europe in recent years imposing substantial health economic burdens.2,3 Despite the implementation of surveillance, hepatitis B vaccination, and hepatitis C direct-acting antiviral treatment, many patients still have unresectable and advanced-stage HCCs that require systemic therapy. 4
Sorafenib is a multikinase inhibitor and the first front-line systemic therapy approved for the treatment of unresectable HCC based on the results of two multicenter, randomized, phase III studies.5,6 However, the results are still limited for cases of objective tumor responses even after a long period of treatment experience (over 10 years). Previous studies and reports have presented sporadic HCC cases with complete response (CR) or partial response (PR) to sorafenib treatment.7–11 Nevertheless, there is little information on the duration of response and long-term outcomes of objective responders. In addition, several second-line treatments have been used for patients who failed sorafenib in recent years.12,13 The therapeutic efficacy and benefits of sequential systemic therapies for sorafenib objective responders are unclear. Here, we aimed to investigate the long-term outcomes of HCC patients who had objective tumor responses to sorafenib treatment and the factors associated with survival benefits in these patients.
Materials and methods
Populations
A total of 922 consecutive patients who received sorafenib treatment for unresectable HCC in Taipei Veterans General Hospital were retrospectively enrolled. The diagnosis of HCC was according to the criteria of American Association for the Study of Liver Diseases (AASLD) treatment guidelines for HCC. 14 Among patients who had the following radiologic evaluation, 21 (2.3%) had a complete response (CR) and 54 (5.9%) had a partial response (PR) according to modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria 15 and serum alpha-fetoprotein (AFP) levels. These 75 objective responders were evaluated for long-term treatment outcomes by sorafenib. In addition, the efficacy of post-sorafenib sequential systemic therapies was investigated in 30 patients who failed sorafenib treatment because of tumor progression. The algorithm of patient selection is shown in Figure 1. This study was approved by the Institutional Review Board (IRB), Taipei Veterans General Hospital (IRB number: 2014-03-009AC, 2019-10-001BC and 2021-04-006BC). The informed consent was waived by the IRB as a result of retrospective design and most enrolled patients died.
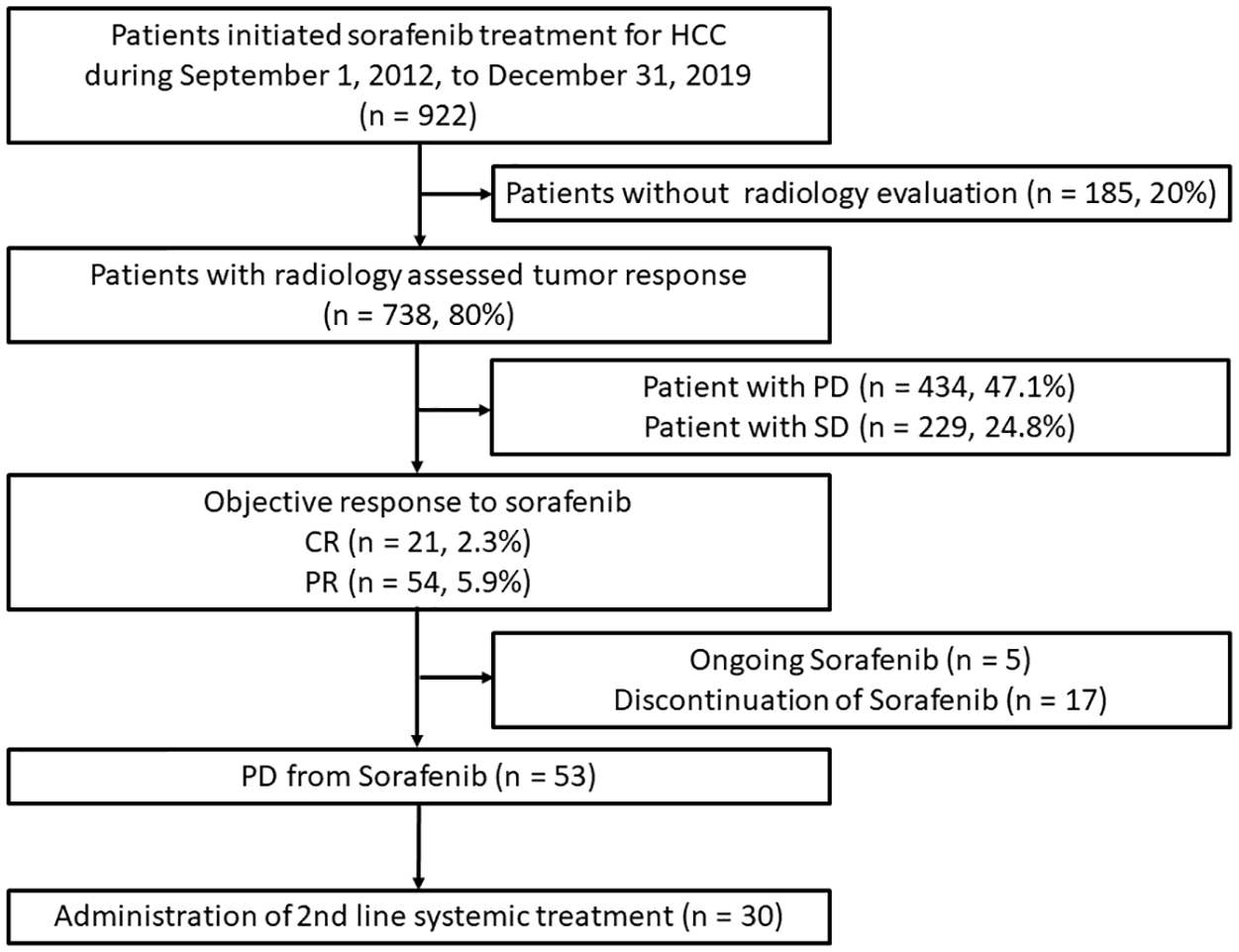
Patient selection algorithm.
Intervention
According to the national health insurance criteria in Taiwan, sorafenib is reimbursed for HCC patients with Child-Pugh A liver function and extrahepatic metastasis or tumor invasion to major vessels, including the main portal vein and its first branch. 4 Patients with HCC refractory to transarterial chemoembolization (TACE) (treatment failure after repeated TACE for at least three times within 12 months) and Child-Pugh A liver reserves have also been reimbursed for sorafenib since November 2016. 16
Sorafenib was initiated at 400 mg twice daily, and the dose was reduced or temporarily interrupted upon development of treatment-related adverse events (TRAEs) or hepatic deterioration. 4 The option of second-line therapy after tumor progression was based on the Taiwan FDA-approved treatments, shared decision-making between the clinicians and patients, and the criteria of Taiwan National Health Insurance. During the study period, regorafenib was reimbursed for the patients with sorafenib-failed HCC in Child-Pugh A status. Besides, nivolumab was reimbursed during April 2019 to March 2020 with the same criteria for regorafenib. Regorafenib was administered orally 160 mg per day during the first 3 weeks of each 4-week cycle, 12 and nivolumab was intravenously used at a dose of 2–3 mg/kg every 2 weeks.13,17 Fluorouracil-based or gemcitabine plus platinum-based chemotherapies18,19 were prescribed to eligible patients who did not meet the timing or criteria of reimbursed targeted agents after sorafenib failure. The dosage of second-line agents was adjusted according to the severity of TRAE and patients’ condition. Treatment was terminated with the occurrence of tumor progression, liver function deterioration, intolerable adverse events, or death.
Comparison
This retrospective study is designed to analyze the survival and clinical outcomes of sorafenib-responders. A comparison group was not defined in this study.
Outcomes
The long-term clinical outcomes and survival benefits were analyzed in objective responders to sorafenib treatment. Besides, the efficacy of post- sorafenib sequential systemic therapies was investigated in 30 patients who failed sorafenib treatment because of tumor progression. In addition, the most common TRAE of sorafenib, including hand–foot skin reaction (HFSR), diarrhea, and hypertension, were recorded and considered for survival analysis. Hand–foot skin reaction was characterized by erythema, dysesthesia, or paresthesia on the palms and soles together with rash. 20 Diarrhea was characterized by an increase in frequency and loose or watery bowel movements, or both. The AE of hypertension was defined as new-onset of high blood pressure (>140/90 mmHg) in the cases without underline hypertension or more increased blood pressure that needs addition of medications in subjects with underlying hypertension. 21 All TRAEs were documented and graded according to the Common Toxicity Criteria for Adverse Effects (CTCAE) version 4.0.
Time
The duration of patient collection was from September 2012 to December 2019, and the following data cutoff was on December 31, 2020.
Statistical analysis
Continuous variables were expressed as medians [interquartile ranges (IQR)] while categorical variables were analyzed as frequency and percentages. The Pearson chi-square analysis or Fisher’s exact test was used to compare categorical variables while the Mann–Whitney U test was applied for continuous variables. Overall survival (OS) and progression-free survival (PFS) from the beginning of sorafenib treatment to death or tumor progression, as well as post-sorafenib survival (PSS) from the time documented for sorafenib failure to death, were estimated via the Kaplan–Meier method and compared by a log-rank test. We also applied Prediction Of Survival in Advanced Sorafenib-treated HCC (PROSASH)-II score to differentiate OS of our patients. 22 In addition, Cox’s proportional-hazard model was used to identify prognostic factors for survival. Schoenfeld residuals were used to test the assumption of proportional hazards (Supplemental Figure 1); p < 0.05 was considered statistically significant for all analyses. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS 26.0 for Windows, SPSS Inc, Chicago, IL, USA) and GraphPad Prism 8 (GraphPad Software, San Diego, CA, USA).
Results
Demographic characteristics of the patients
The entire cohort of sorafenib-treated HCC (n = 922) was male-predominant (78.9%) and most had chronic hepatitis B virus (HBV) infection (57.6%). Most patients were within Child-Pugh class A (86.1%); more than half of them were classified beyond albumin-bilirubin (ALBI) grade 1 (66.3%); 86.0% of tumors were at Barcelona Clinic Liver Cancer (BCLC) stage C; 57.9% with macroscopic vascular invasion, and 56.6% presented extrahepatic metastasis. The detailed baseline characteristics of the cohort are shown in Table 1.
Baseline characteristics of total HCC patients treated with sorafenib.

AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; AL(S)T, alanine(aspartate) aminotransferase; BCLC, Barcelona Clinic Liver Cancer; INR, international normalized ratio; PVI, portal vein invasion; RFA, radiofrequency ablation; TACE, transarterial chemoembolization.
Continuous variables were expressed as median (interquartile).
Of the 75 objective responders (21 CR, 54 PR) to sorafenib treatment, three complete responders were at BCLC stage B and received sorafenib due to TACE failure. The maximal tumor size was smaller in CR patients (median size 2.5 versus 4.7 cm, p = 0.001). The prevalence of macrovascular invasion or extrahepatic metastasis was comparable between CR and PR groups. Patients with complete tumor response had a longer treatment duration than patients with PR (751 versus 401 days, p = 0.001); more patients with CR to sorafenib had experienced a dose reduction for more than 25% of the recommended dose (95.2% versus 70.4%, p = 0.021). None of them received aspirin during sorafenib treatment. Detailed demographic characteristics and treatment conditions are shown in Table 2.
Basic characteristics of HCC patients with objective responses to sorafenib.

AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; AL(S)T, alanine(aspartate) aminotransferase; BCLC, Barcelona Clinic Liver Cancer; CR, complete response; HCC, hepatocellular carcinoma; INR, international normalized ratio; LRT, local regional treatment; PR, partial response; PVI, portal vein invasion; RFA, radiofrequency ablation; TACE, transarterial chemoembolization.
Continuous variables were expressed as median and range.
Treatment outcomes of objective responders
Of the 21 complete responders, the median time to response (TTR) and duration of response (DOR) were 4.3 and 18.3 months, respectively. The median TTR and DOR of PR patients were 2.8 and 10.0 months, respectively (Table 3). During the median follow-up period of 35.3 months (IQR, 16.6–46.3), five (6.7%) objective responders had ongoing sorafenib treatment at the data cutoff date. Eventually, 53 patients (70.6%) developed tumor progression and 43 patients died. The median PFS and OS were 18.8 (95% CI, 12.7–25.0) and 39.5 months (95% CI, 28.4–50.5), respectively. Figure 2(a) and (b) shows that patients with CR had a significantly longer PFS and OS than PR patients (median PFS: 29.3 versus 15.1 months, p = 0.011; median OS: not reached versus 25.8 months, p < 0.001). However, no significant difference of OS could be identified according to the PROSASH-II model in these objective responders (Supplemental Figure 2).

Survival benefits of HCC responders to sorafenib treatment according to tumor response: (a) progression-free survival (PFS) and (b) overall survival (OS) of HCC responders according to the tumor responses to sorafenib treatment.
Clinical responses and outcomes of HCC with objective response to Sorafenib.

CI, confidence interval; CR, complete response; DOR, duration of response; HFSR, hand–foot skin reactions; PFS, progression-free survival; PR, partial response; OS, overall survival; TTR, time to response.
TRAE-associated survival benefits
Most (88.0%) objective responders experienced sorafenib-related adverse events during treatment. The most common TRAE was HFSR (69.3%) followed by diarrhea (42.7%) and hypertension (26.7%). The incidence of AEs was comparable between CR and PR patients (Table 3). Figure 3(a) shows that patients who experienced TRAE had significantly longer OS than those without AE (median OS: 44.9 versus 18.1, p = 0.003). A significantly better OS was also observed in patients who developed diarrhea (median OS: 56.4 versus 30.5, p = 0.031) or hypertension (median OS: 85.2 versus 35.3, p = 0.013) during sorafenib treatment. No significant survival difference was noted according to the presence of HFSR [Figure 3(b)–(d)].

Overall survival (OS) of HCC responders to sorafenib treatment according to the presence of treatment-related adverse events (TRAEs). OS according to the presence of (a) all TRAEs, (b) hand–foot skin reactions (HFSR), (c) diarrhea, and (d) hypertension.
In addition, marginally longer PFS was observed in patients who developed TRAE than the others (median PFS: 21.0 versus 8.6 months, p = 0.064). Patients who suffered from sorafenib-related diarrhea had significantly better PFS than the counterparts (median PFS: 18.8 versus 17.2 months, p = 0.048). The benefits of HFSR or hypertension to PFS were marginal without statistical significance (Supplemental Figure 3). However, nearly all patients in this study had reduced sorafenib dose during the treatment course; no significant differences of PFS or OS was observed according to dose reduction (Supplemental Figure 4).
Outcomes of sequential systemic therapies
Of the 53 patients who discontinued sorafenib treatment because of tumor progression, 30 patients received sequential second-line systemic therapies including regorafenib (n = 15), nivolumab (n = 8), and chemotherapy (n = 7). Figure 4(a) and (b) shows that sequential nivolumab monotherapy provided significantly better PSS and OS versus chemotherapy. Comparable survival benefits were observed between nivolumab and regorafenib in patients with sorafenib-failed HCC (median PSS: not yet reached versus 15.5 months, p = 0.088; median OS: 55.8 versus 39.5 months, p = 0.064). In multivariate analyses, nivolumab sequential therapy [hazard ratio (HR): 0.083, p = 0.030] was independently associated with a better OS in sorafenib-failed HCC (Table 4).
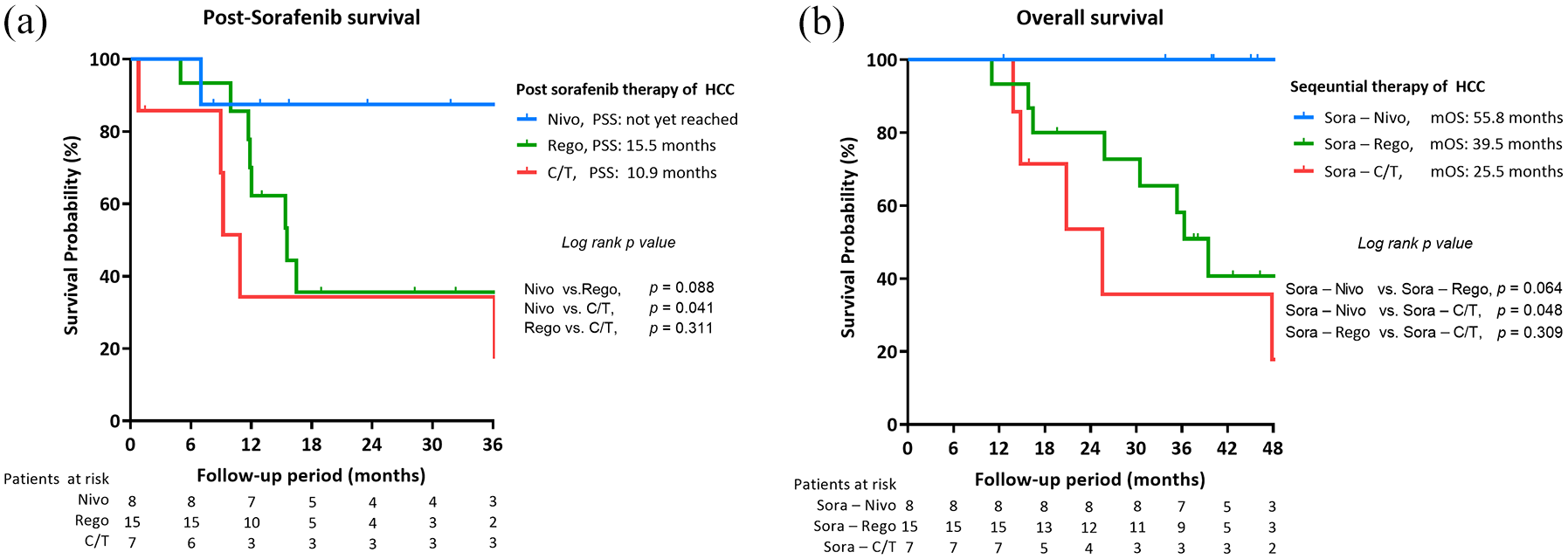
Survivals of HCC responders to sorafenib treatment according to the administration of second-line systemic therapy: (a) postsorafenib survival (PSS) and (b) overall survival (OS) according to the different subsequent therapies after sorafenib failure.
Factors associated with overall survival in 30 HCC patients received sequential systemic therapy.
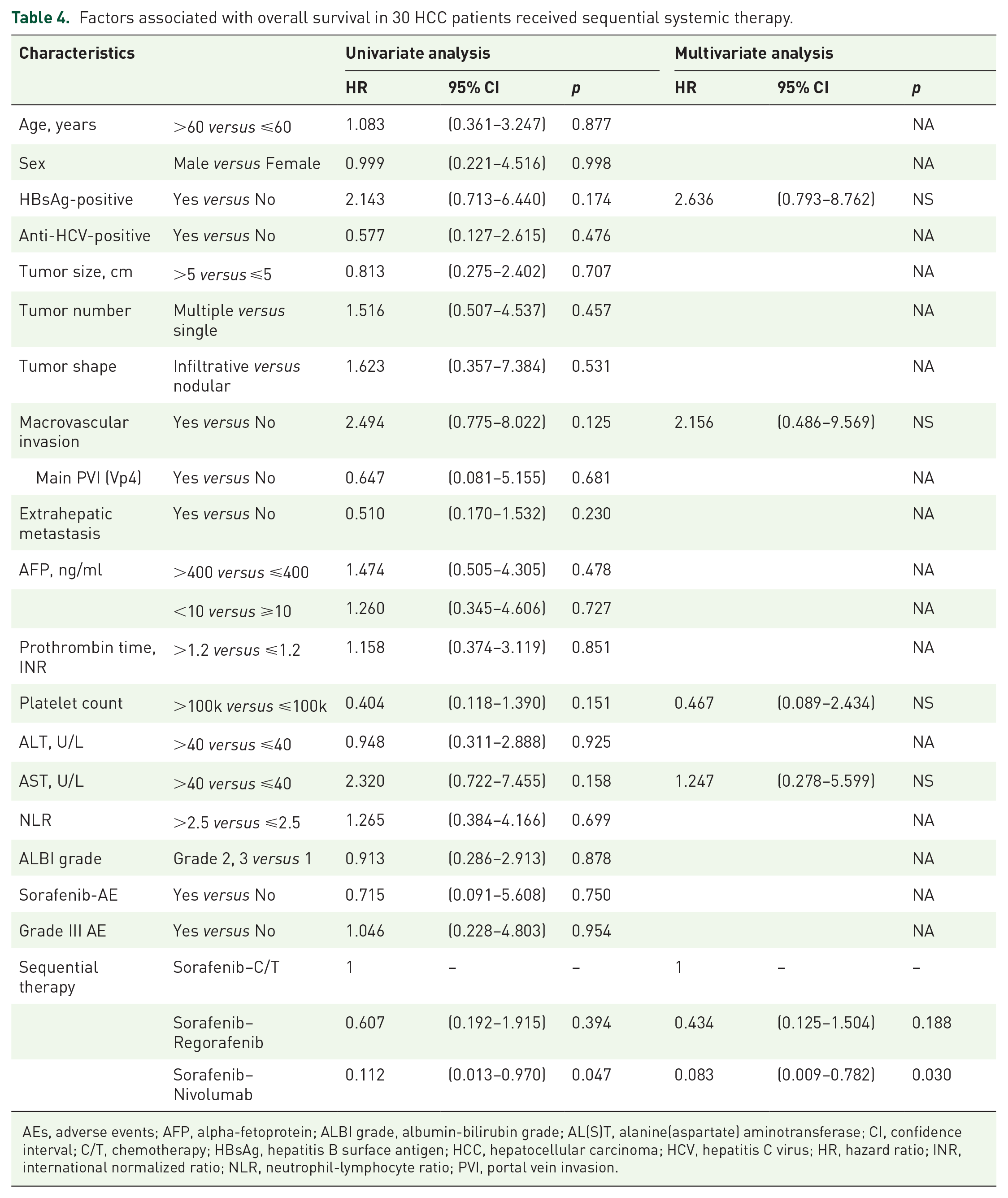
AEs, adverse events; AFP, alpha-fetoprotein; ALBI grade, albumin-bilirubin grade; AL(S)T, alanine(aspartate) aminotransferase; CI, confidence interval; C/T, chemotherapy; HBsAg, hepatitis B surface antigen; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HR, hazard ratio; INR, international normalized ratio; NLR, neutrophil-lymphocyte ratio; PVI, portal vein invasion.
Discussion
This is the largest real-world cohort of Asian patients with unresectable HCC treated by sorafenib to date; 8.2% of patients had an objective tumor response by radiological assessment. For advanced HCC patients with response to sorafenib, the duration of response could last for 1 year; the median OS was 39.5 months. Presence of TRAE, particularly diarrhea and hypertension, and administration of subsequent immunotherapy were associated with better survival benefits in sorafenib-responders.
A low tumor response rate is the main disadvantage of sorafenib treatment for HCC. In the SHARP and Asian-Pacific study, only 2% and 3.3% of patients had partial response; no complete response was reported.5,6 According to an Italian multicenter study that enrolled 296 HCC patients, the overall objective response rate was 8%, including two patients (1%) with CR and 22 with PR (7%). 7 In a Spanish multicenter retrospective study, 12 (1%) complete responders were identified from 1119 patients; the outstanding OS reached 85.8 months. 11 Of the real-world cohorts in Taiwan, approximately 5–7% of HCC developed objective responses to sorafenib treatment.8,10,23 Similar to previous studies, the objective response rate of our cohort was low, but the therapeutic efficacy was durable in the sorafenib-responders.
According to clinical trials and real-world studies, the most common TRAEs of sorafenib included diarrhea, arterial hypertension, fatigue, and dermatological toxicities, mainly as HFSR.5–7,24–26 Previous studies suggested that the presence of adverse events may be of prognostic and predictive importance in sorafenib-treated HCC.27–33 Here, we found that the presence of diarrhea and hypertension were associated with better OS in the objective responders to sorafenib. Diarrhea was also associated with a better PFS. In contrast, no significant survival benefits of HFSR could be identified in these responders probably because most (69.3%) had expressed HFSR during sorafenib treatment. This finding confirms that optimal management of sorafenib-related AEs would prolong treatment duration and improve patients’ survival. 34
Dose reduction was often carried out in clinical practice in approximately 26–45% of patients, even the majority of AEs were grades 1–2.5–7,25,26 According to a previous study, sorafenib dose reduction can improve HCC survival and increase patients’ tolerance and adherence coupled with longer duration and a higher cumulative dose. 35 In this study, most (96.0%) objective tumor responders had experienced a dose reduction, and 77.3% of them underwent a more than 25% dose reduction during sorafenib treatment. Dose reductions did not lead to survival differences probably because of the high application rate of this practice.
Aspirin use was reported in association with better clinical outcomes and survival benefits in patients who received sorafenib treatment for HCC. 36 As to our patients, none of sorafenib-responders had used aspirin during the sorafenib or subsequent therapies for HCC. Therefore, we did not include aspirin use in the analysis. PROSASH-II score was suggested as the most-effective prognostic classification model for patients with sorafenib-treated HCC. 22 However, no significant survival difference could be identified according to PROSASH-II model in our objective responders. It is possible that our patients were objective responders to sorafenib; consequently, PROSASH-II scores could not further differentiate them.
Nivolumab and regorafenib have demonstrated their therapeutic effectiveness for the sorafenib-failed HCC according to the Checkmate-040 and RESCORCE trials in 2017.12,13 According to a Korean study, comparable efficacy and safety between nivolumab and regorafenib were observed in patients with sorafenib-failed advanced HCC. The median OS was 5.9 and 6.9 months for nivolumab and regorafenib, respectively. Nivolumab sequential therapy was independently associated with prolonged OS. 37 Another retrospective study in Taiwan showed that subsequent nivolumab and regorafenib provided promising and comparable benefits to sorafenib-failed HCC. 38 The OS was 14 and 11 months from the time of nivolumab and regorafenib commencement and 21.9 and 17.3 months in the nivolumab and regorafenib group since the beginning of sorafenib treatment. 38 Here, subsequent nivolumab treatment provided an optimal PSS (not yet reached at data cutoff on December 31, 2020) that was better than the survival observed in the Asian cohort of Checkmate-040 trial (14.9 months). 39 The median OS from initiation of sorafenib to death in patients who received sorafenib–nivolumab sequential therapy was up to 55.8 months. A comparable survival benefits attributed to subsequent regorafenib was also observed in our patients (median PSS: 15.5 months, median OS from sorafenib initiation: 39.5 months) similar to the results of RESCORCE trial (10.6 and 26.0 months, respectively).12,40 Real-world data of sorafenib–regorafenib showed median OS around 28.5 to 38.4 months.41,42 Our study focusing on responders to sorafenib, showed a median OS of 39.5 months by sorafenib–regorafenib sequencing. These data suggest that nivolumab and regorafenib have promising treatment efficacy and survival benefits as second-line therapies particularly in sorafenib-responders.
There are several limitations in this study. First, this is a retrospective study that only enrolled patients in single hospital. However, our hospital is the main leading tertiary medical center in Taiwan. The large case numbers and long-term follow-up period of this cohort as well as regular tumor reassessment and clinical evaluation ameliorates information bias as well. Second, the trough concentration of sorafenib was not checked in our patients, although it might predict the occurrence of serious AE, tumor response, and survival in patients with HCC. 43 Third, most of our patients had chronic hepatitis B as the underlying hepatic disease. We should cautiously apply our experience to other populations. Finally, as a retrospective study, the genetic mutations of tumor, such as the specific BRAF alterations, 44 and the tumor microenvironment, involving the pathophysiology of hypoxia-induced angiogenesis and immunosuppression, 45 were not available. Precision and individualized approaches for systemic therapy of HCC are still in unmet need to select multikinase inhibitor-preferred or immune checkpoint inhibitor-preferred patients. Further clinical trials with precision and individualized approaches focusing on the genetics and microenvironment of tumor as well as the HCC etiology are needed to elucidate these issues.
In conclusion, although the objective response rate of HCC to sorafenib is low, the long-term benefit is durable. The presence of TRAE (particularly diarrhea and hypertension) was associated with better OS. Sequential therapy with nivolumab or regorafenib after sorafenib failure could provide promising and comparable benefits to HCC patients who had previous responses to sorafenib treatment. This information is important for characterizing outcomes of sorafenib-responders and the choice of sequential treatment.
Supplemental Material
sj-docx-1-tam-10.1177_17588359221099401 – Supplemental material for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma
Supplemental material, sj-docx-1-tam-10.1177_17588359221099401 for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma by Kuo-Wei Huang, Pei-Chang Lee, Yee Chao, Chien-Wei Su, I-Cheng Lee, Keng-Hsin Lan, Chi-Jen Chu, Yi-Ping Hung, San-Chi Chen, Ming-Chih Hou and Yi-Hsiang Huang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tif-2-tam-10.1177_17588359221099401 – Supplemental material for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma
Supplemental material, sj-tif-2-tam-10.1177_17588359221099401 for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma by Kuo-Wei Huang, Pei-Chang Lee, Yee Chao, Chien-Wei Su, I-Cheng Lee, Keng-Hsin Lan, Chi-Jen Chu, Yi-Ping Hung, San-Chi Chen, Ming-Chih Hou and Yi-Hsiang Huang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tif-3-tam-10.1177_17588359221099401 – Supplemental material for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma
Supplemental material, sj-tif-3-tam-10.1177_17588359221099401 for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma by Kuo-Wei Huang, Pei-Chang Lee, Yee Chao, Chien-Wei Su, I-Cheng Lee, Keng-Hsin Lan, Chi-Jen Chu, Yi-Ping Hung, San-Chi Chen, Ming-Chih Hou and Yi-Hsiang Huang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tif-4-tam-10.1177_17588359221099401 – Supplemental material for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma
Supplemental material, sj-tif-4-tam-10.1177_17588359221099401 for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma by Kuo-Wei Huang, Pei-Chang Lee, Yee Chao, Chien-Wei Su, I-Cheng Lee, Keng-Hsin Lan, Chi-Jen Chu, Yi-Ping Hung, San-Chi Chen, Ming-Chih Hou and Yi-Hsiang Huang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-tif-5-tam-10.1177_17588359221099401 – Supplemental material for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma
Supplemental material, sj-tif-5-tam-10.1177_17588359221099401 for Durable objective response to sorafenib and role of sequential treatment in unresectable hepatocellular carcinoma by Kuo-Wei Huang, Pei-Chang Lee, Yee Chao, Chien-Wei Su, I-Cheng Lee, Keng-Hsin Lan, Chi-Jen Chu, Yi-Ping Hung, San-Chi Chen, Ming-Chih Hou and Yi-Hsiang Huang in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We thank the patients and their families/caregivers, the study investigators and their staff, and the Clinical Research Core Laboratory, Department of Medical Research, Taipei Veterans General Hospital.
Ethics approval and consent to participate
This study was approved by the Institutional Review Board (IRB), Taipei Veterans General Hospital (IRB number: 2014-03-009AC, 2019-10-001BC and 2021-04-006BC). The informed consent was waived by the IRB as a result of retrospective design and most enrolled patients died.
Consent for publication
The informed consent was waived by the IRB as a result of retrospective design
Author contribution(s)
Funding
This study is supported by grants from Taipei Veterans General hospital (V109C-048, V110C-144, and V111C-107).
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.