
Abstract
Background:
The addition of neutrophil-to-lymphocyte ratio (NLR) and bone metastases to the International Metastatic RCC Database Consortium (IMDC) score (by the Meet-URO score) has been shown to better stratify pretreated metastatic renal cell carcinoma (mRCC) patients receiving nivolumab. This study aimed to validate the Meet-URO score in patients receiving cabozantinib to assess its predictivity and prognostic role.
Methods:
A multicenter retrospective analysis evaluated mRCC patients receiving ⩾second-line cabozantinib. NLR, IMDC score and bone metastases were assessed before the start of cabozantinib. The primary endpoint was overall survival (OS). Harrell’s c-index was calculated to compare the accuracy of the prediction of the two scores.
Results:
Overall, 174 mRCC patients received cabozantinib as second and third line (51.7% and 48.3%, respectively) with a median follow-up of 6.8 months. A shorter median overall survival (mOS) was observed for the IMDC poor-risk group, NLR ⩾3.2 and the presence of bone metastases, while the IMDC intermediate-risk group had a similar mOS to the favourable-risk one. Applying the Meet-URO score, three risk groups were identified: group 1 (55.2% of patients) with a score of 0–3, group 2 (38.5%) with a score of 4–8 and group 3 (6.3%) with a score of 9. Compared to group 1 (mOS: 39.4 months), a statistically significant worse mOS was observed in group 2 (11.2 months) and group 3 (3.2 months) patients, respectively. The Meet-URO c-index score was 0.640, showing a higher discriminative ability than the IMDC score (c-index: 0.568).
Conclusion:
This analysis showed that the Meet-URO score provides a more accurate prognostic stratification than the IMDC score in mRCC patients treated with ⩾second-line cabozantinib besides nivolumab. Moreover, it is an easy-to-use tool with no additional costs for clinical practice (web-calculator is available at: https://proviso.shinyapps.io/Meet-URO15_score/). Future investigations will include the application of the Meet-URO score to the first-line immunotherapy-based combination therapies.
Introduction
Tyrosine kinase inhibitors (TKIs) directed against the vascular endothelial growth factor receptor (VEGFR) are the treatment mainstay of metastatic renal cell carcinoma (mRCC), either as single agents or in combination with immune checkpoint inhibitors (ICIs), in untreated and pretreated mRCC patients.1,2 Cabozantinib is a potent multitargeted TKI that demonstrated to be superior in terms of progression-free survival (PFS) compared to sunitinib as first-line treatment in intermediate and poor International Metastatic RCC Database Consortium (IMDC) risk patients, as shown by the randomized phase 2 CABOSUN trial.3,4 Moreover, Cabozantinib resulted in being superior to everolimus in terms of response rate (RR), PFS and overall survival (OS) in the second or further treatment line, as shown by the phase 3 randomized METEOR trial, irrespective of the IMDC risk class.5,6
Despite the central role of TKI, ICIs have significantly improved the therapeutic scenario of patients with mRCC over the past years. However, their benefit is confined to a minority of them.1,2 Therefore, identifying biomarkers able to select patients most and least likely to benefit from immunotherapy is a clinically unmet need and topical for clinical research. 7
The IMDC score is currently the most used prognostic classification. It is based on a combination of clinical and laboratory factors.8,9 However, the IMDC score was developed in 2009 when most of the currently used systemic treatments were unavailable. 8 Hence, although it remains a milestone for the prognostic stratification of patients with mRCC, it might not accurately predict the prognosis of patients who are treated with novel agents and their combinations.
The Meet-URO score is a novel and clinically applicable index developed on a dataset of 571 patients with mRCC treated with nivolumab in the second or further treatment line (Meet-URO 15 study from the “Meet-URO: the Italian Network for research in Urologic-Oncology”). It incorporates the presence of bone metastases and baseline neutrophil-to-lymphocyte ratio (NLR) ⩾3.2 into the IMDC score. 10 The Meet-URO score stratifies patients into five prognostic categories and has better prognostic performance than the IMDC score, although its predictive value is still to be defined. 10
This retrospective analysis aims to assess the prognostic value of the Meet-URO score in a cohort of patients with mRCC treated with cabozantinib as second and third treatment line.
Materials and methods
The Meet-URO score, consisting of the pretreatment IMDC score, NLR value and presence of bone metastases, as previously described, 10 was assessed by a retrospective analysis of a real-world series of pretreated patients with mRCC who received cabozantinib. The study was performed according to the Declaration of Helsinki, Good Clinical Practice, and local ethical and legal regulations. The Regional Ethical Committee of Marche approved the analysis (registration number 2019-403). All living patients enrolled in the study signed written informed consent.
Study population
Clinical data and laboratory parameters from patients’ electronic medical records and paper charts were collected among 10 centres. The study population included adults with clear-cell or non-clear-cell mRCC, treated with at least one cycle (i.e. 28 days) of cabozantinib given as second- or third-line therapy between May 2014 and January 2019.
Treatment
Cabozantinib was orally administrated, aiming at starting dose of 60 mg once daily. Dose reductions (to 40 mg, then 20 mg) or treatment interruption were considered to manage adverse events. The treatment was administered until clinical or radiological disease progression, unacceptable toxicity, death or patient’s choice. As per local clinical practice, follow-up usually consisted of monthly physical examination and laboratory analysis. Radiological assessments consisted of computed tomography (CT) scan of chest-abdomen-pelvis and the head (if clinically indicated), performed at baseline and every 2–4 months of treatment or at the time of clinical progression.
Prognostic factors
To calculate the Meet-URO score, clinical and laboratory prognostic factors were assessed at baseline, before the first cycle of cabozantinib, including IMDC prognostic risk group (favourable, intermediate, poor), metastatic sites (for the presence or absence of bone metastases) and complete blood count (from which the NLR was calculated). The scoring system of the Meet-URO score was available as a web-calculator at: https://proviso.shinyapps.io/Meet-URO15_score/.
Study endpoint
The primary endpoint was OS, which was calculated from the start of cabozantinib until death, censored at last follow-up for alive patients.
Statistical analysis
Patients’ characteristics were reported using absolute frequency and percentage for categorical variables and median and range for quantitative variables.
The Kaplan–Meier (KM) method was used to estimate survival curves of OS for the three prognostic factors (NLR, IMDC score and presence of bone metastases) included in the Meet-URO score and their combination in the Meet-URO score itself. Differences were considered statistically significant when the p-value was <0.05.
Univariable analyses for the association of the three prognostic factors of the Meet-URO score (NLR, IMDC score and presence of bone metastases) with OS were performed using the Cox proportional hazard regression model. A multivariable Cox model was also performed to adjust for characteristics that showed a difference among the Meet-URO risk groups with a p value <0.10 at the univariable analysis.
Using the weights obtained for each prognostic factor in developing the Meet-URO score, we calculated the score for each patient. Only patients with available information on all prognostic factors composing the Meet-URO score were included in this analysis.
A survival receiver operating characteristic (ROC) analysis and a visual inspection of survival curves were adopted to identify potential cut-offs that better stratify the total score in risk groups. The number of risk groups originally used in the Meet-URO score could have changed according to the different sample sizes of the population treated with cabozantinib.
Harrell’s c-index was calculated for the Meet-URO score and compared with the c-index calculated for the IMDC score. All statistical analyses were performed using the software Stata v.16 (StataCorp 2019). 11
Results
Patients’ characteristics
We identified 174 patients affected by mRCC with available data for the three prognostic factors of the Meet-URO score (i.e. baseline IMDC score, NLR and presence/absence of bone metastases). Patients’ characteristics are summarized in Table 1. Most patients were male (74.7%) and treated with previous nephrectomy (78.2%). The median age was 64.2 years (range: 30–86 years) and the most common histology was clear-cell RCC (81.6%).
Patients’ characteristics.

IMDC, International Metastatic RCC Database Consortium; N, number of patients; NLR, neutrophil-to-lymphocyte ratio.
Cabozantinib was given as second and third treatment line in 51.7% and 48.3% of patients, respectively. IMDC score was favourable, intermediate and poor in 25.3%, 60.9% and 13.8% of patients, respectively. Baseline NLR was ⩾3.2 in 46.6%, and bone metastases were present in 30.5% of patients.
Survival outcomes in the overall population
At the time of data cut-off (July 2020), with a median follow-up of 6.8 months [interquartile range (IQR): 3.0-11.1 months], 58 patients (33.3%) had died, 49 patients (28.2%) were censored within 6 months and other 42 (24.1%) within the window of 6–12 months. The median overall survival (mOS) was 15.3 months [95% confidence interval (CI): 11.1–44.8] with an OS at 6 months of 78.3% (95% CI: 70.6–84.2).
Association of the prognostic factors with OS
Univariable Cox regression analysis on OS for the three prognostic factors included in the Meet-URO score is reported in Table 2.
Univariable Cox regression analysis for OS including the parameters of the Meet-URO score.
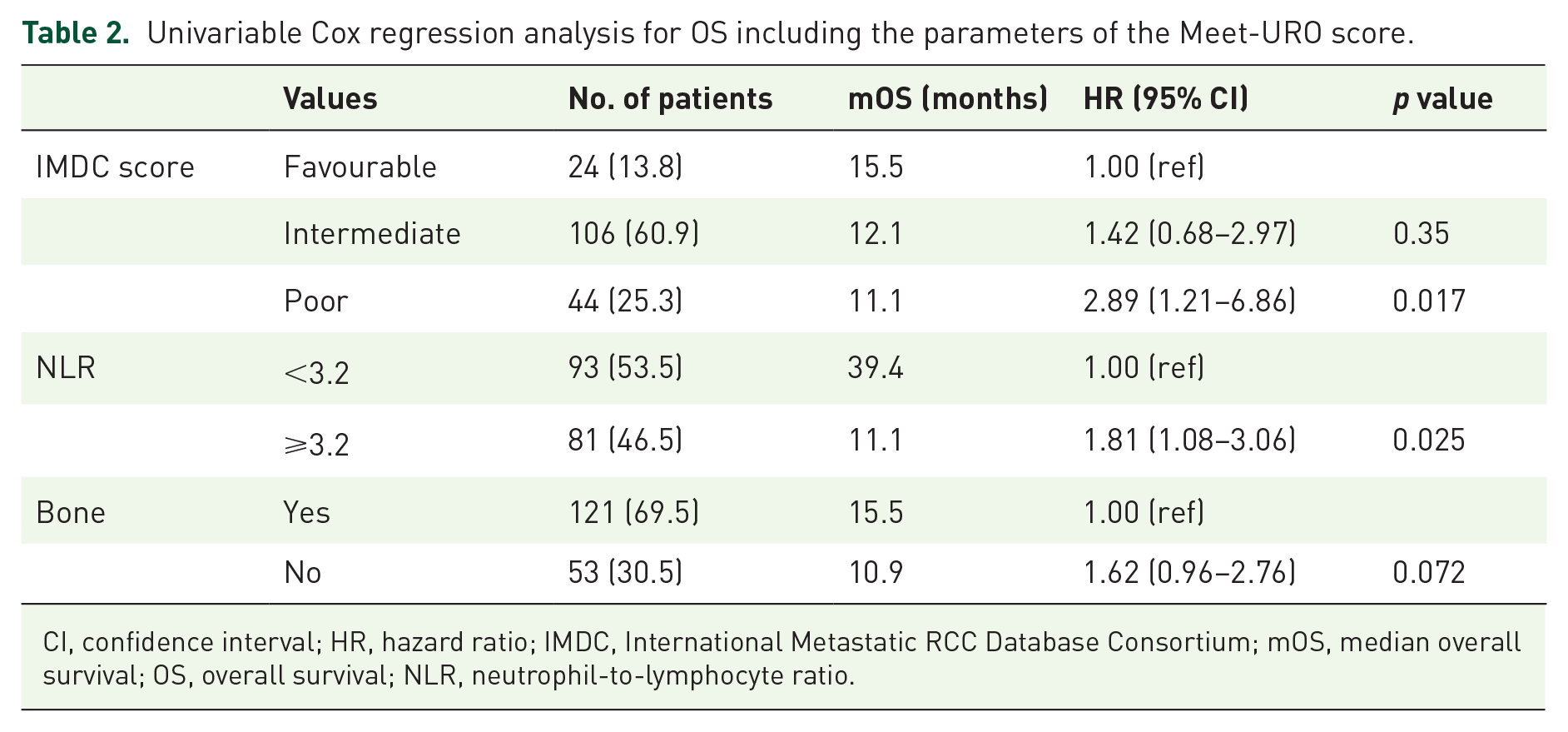
CI, confidence interval; HR, hazard ratio; IMDC, International Metastatic RCC Database Consortium; mOS, median overall survival; OS, overall survival; NLR, neutrophil-to-lymphocyte ratio.
No significant difference in the mOS was observed between the IMDC intermediate- and the favourable-risk groups (p = 0.35), while poor-risk patients showed significantly shorter mOS than favourable-risk patients (11.1 versus 15.5 months; p = 0.017; Figure 1(a)). The IMDC score showed a c-index of 0.596.

Kaplan–Meier curves for OS according to the (a) IMDC score, (b) NLR and (c) bone metastases.
A high NLR (⩾3.2) was associated with significant shorter mOS (11.1 versus 39.4 months, p = 0.025) than low (Figure 1(b)). The presence of bone metastases indicated a non-significant trend towards reduced OS (mOS: 10.9 versus 15.5 months; p = 0.072) (Figure 1(c)).
Application of the Meet-URO score
The Meet-URO prognostic score was calculated for each patient using weights obtained during the development of the Meet-URO score for each prognostic factor. The distribution of the Meet-URO score results is shown in Figure 2. The highest frequency was observed for score 3 (32.8%), followed by score 6 (17.2%); 11 patients (6.3%) had all negative prognostic factors with a total score of 9. According to the Cox model, the Meet-URO scores from 0 to 9 showed a discriminant index (c-index) of 0.648.

Distribution of the Meet-URO score from groups 0 to 9.
However, some Meet-URO prognostic classes showed overlapping survival curves making the original division in five risk groups not replicable.
Using survival ROC analysis, a Meet-URO score cut-off between 3 and 4 allowed the identification of two distinctive prognostic groups: one ranging 0–3 and the other with a score ⩾4. Moreover, the worst prognosis was observed for the group with a score of 9 separately.
In consideration of these results, three risk groups were selected (Table 3): group 1, including 96 patients (55.2%) with a score of 0–3; group 2, including 67 patients (38.5%) with a score of 4–8; group 3, including 11 patients (6.3%) with a score of 9. The characteristics of these groups are reported in Table 1. Group 3 patients received less commonly previous nephrectomy and had a higher rate of metastatic disease at diagnosis (p < 0.001 for both comparisons). Group 1 was also associated with the lowest rate of bone metastases and <3.2 NLR values (p < 0.001 for both comparisons). No significant differences were observed in terms of age and histologic subtype.
Prognostic groups as the combination of NLR, IMDC prognostic groups and bone metastases.

CI, confidence interval; HR, hazard ratio; IMDC, International Metastatic RCC Database Consortium; mOS, median overall survival; N, number of patients; NLR, neutrophil-to-lymphocyte ratio; NR, not reached; Ref, reference group.
Significantly worse OS was observed in patients belonging to group 2 (mOS: 11.2 months; p = 0.026) and 3 (mOS: 3.2 months; p < 0.001), when compared to group 1 (mOS: 39.4 months) (Figure 3) (Table 3). These results were also confirmed after adjustment for age, histologic subtype, nephrectomy and metastases at diagnosis [hazard ratio (HR) group 2 versus group 1 = 2.13, 95% CI: 1.13–3.99; HR group 3 versus group 1 = 5.28, 95% CI: 1.96–14.17] in the multivariable analysis.

Kaplan–Meier curves for OS according to the Meet-URO score.
Comparison between the Meet-URO score and the IMDC score: populations
The joint frequency distribution between the Meet-URO and IMDC risk groups and their correlation with mOS is shown in Table 4.
Comparison between the Meet-URO prognostic score and IMDC risk groups.

IMDC, International Metastatic RCC Database Consortium; mOS, median overall survival; N, number of patients.
mOS of the overall population.
The bold values are only the median OS.
According to the Meet-URO score, group 1 patients belonged to the IMDC favourable- and intermediate-risk (45.8% and 54.2%, respectively); patients of group 2 belonged to the IMDC intermediate and poor-risk (80.6% and 19.4%, respectively); all patients of group 3 belonged to the IMDC poor-risk patients (100%).
According to the IMDC score, the IMDC favourable-risk patients were all included in the Meet-URO group 1; IMDC intermediate-risk patients belonged to the Meet-URO group 1 and 2 (49.1% and 50.9%, respectively); IMDC poor-risk patients belonged to the Meet-URO group 2 and 3 (54.6% and 45.8%, respectively).
Comparison between the Meet-URO score and the IMDC score: OS
The c-index of the three-class categorized by Meet-URO score was 0.640, with higher discriminative ability than the IMDC score (c-index previously reported: 0.568). This is also more evident observing the mOS of the prognostic groups calculated according to the Meet-URO and the IMDC score (Table 4 and Figure 1).
The prognostic group with the longest mOS is the Meet-URO group 1, which, as previously described, is composed of IMDC favourable-risk and intermediate-risk patients. Notably, the mOS of the Meet-URO group 1 is also higher than the IMDC favourable-risk group 1 (39.4 versus 14.5 months). Conversely, the prognostic group with the worst mOS is the Meet-URO group 3, with a shorter mOS than the IMDC poor-risk group (3.2 versus 11.1).
Discussion
Over the past 5 years, an increasing number of novel drugs and immunotherapy-based combinations have been approved for the treatment of mRCC.12,13 In addition to improved activity, these therapies have different pharmacokinetic characteristics and mechanisms of action compared to the pre-existing targeted therapies (e.g. sunitinib, sorafenib, pazopanib and axitinib), which were the treatments available at the time the IMDC prognostic classification was developed. 8 Therefore, the IMDC score might no longer be a reliable tool for the prognostication of mRCC treated within either clinical trials or clinical practice, particularly in the second-line setting and beyond.
The multicentric retrospective Meet-URO 15 study, based on 571 patients treated with nivolumab as second or beyond treatment line, demonstrated the prognostic accuracy of the IMDC score could be improved by the incorporation of NLR and the presence of bone metastases (e.g. the Meet-URO score), which are well-known prognostic factors in mRCC,14,15 in the immunotherapy setting. 10 In the present study, we aimed to confirm the prognostic value of the Meet-URO score in a similar disease setting but with a different TKI-based treatment.
Noteworthy, differently from what was observed with nivolumab, 10 neither the IMDC score nor the presence of metastases, but the NLR was able to significantly stratify patients’ prognosis in this treatment setting, at the univariate analysis. In particular, the OS of IMDC favourable- and intermediate-risk groups did not differ significantly, confirming previous findings from retrospective analyses of large real-life series of patients treated with cabozantinib.16,17 Since cabozantinib is a new-generation multitarget therapy not included in the development of the IMDC score, a more accurate and updated prognostic score is needed.
Regarding the lack of significant survival difference by the presence of bone metastases, this is in line with the subgroup analysis of the METEOR trial and a recent meta-analysis, both showing similar survival outcomes with cabozantinib irrespective of the presence of bone metastases.18,19 Conversely, NLR showed the most significant prognostic value with the highest magnitude of survival difference between the two groups (i.e. NLR ⩾3.2 versus <3.2, Δ 28.3 months, or more than 2 years). The role of NLR may rely on the correlation between the host immune system, for which NLR may represent an easy-to-measure parameter and the tumour pro-angiogenic mechanisms at the basis of the progression of mRCC.7,20 This interplay is known for the immunomodulatory effects of the anti-angiogenic drugs and represents the biologic rationale for the novel immunotherapy-based combinations.21,22
As a result of the different weight of these three prognostic variables and the small number of patients in the current TKI-based series, compared to the previous immunotherapy-based one, 10 the application of the Meet-URO score with its original five prognostic categories was not applicable, due to the overlap of survival curves for some of those prognostic groups. Nevertheless, the implementation of the IMDC score with the addition of NLR and the presence of bone metastases showed better accuracy in the prediction of OS than the IMDC score alone, confirming the prognostic value of the Meet-URO score and, likely, its lack of predictive value for immunotherapy.
Similar to the previous series with nivolumab, 10 the Meet-URO score allowed a better risk stratification of IMDC intermediate- and poor-risk groups. In particular, the intermediate IMDC group was classified by the Meet-URO score into two prognostically distinct subgroups [with mOS: not reached (NR) versus 11.2 months]. This is supported by previous evidence on the heterogeneity of the IMDC intermediate-risk group. 23 The IMDC poor-risk group was classified by the Meet-URO score in two different groups, with a subgroup of patients (group 3) with all three negative prognostic factors (IMDC poor-risk, NLR ⩾ 3.2, bone metastases) for whom cabozantinib, as well as nivolumab, 10 probably are not the best treatment option and would be better candidate for supportive care only.
All the above findings could be relevant in clinical practice for two reasons.
First, cabozantinib is currently a mainstay in the treatment of mRCC and the most effective TKI for both untreated and pretreated patients with mRCC as either single-agent or combination therapies. 24 Hence, applying the Meet-URO score to patients being considered for cabozantinib could help the oncologist better estimate their prognosis, especially in the context of different treatment options.
Second, few efforts have been made to identify new prognostic factors for mRCC patients treated with novel agents, and none has been translated into clinical practice. The analysis of plasma biomarkers obtained from patients with mRCC treated with cabozantinib in the METEOR trial reported that low levels of circulating HGF, ASXL6 and VEGFR were associated with better OS and PFS. 25 Although relevant, these findings are yet preliminary and not easily applicable in clinical practice. Moreover, a retrospective analysis of 87 patients treated with cabozantinib developed a risk scoring system based on clinical and inflammatory variables, similar to the Meet-URO score. 10 However, this study included fewer patients treated with cabozantinib compared to the current study.
We acknowledge among limitations of the present analysis its retrospective nature, the relatively small size of the population, the short median follow-up and the lack of validation in a prospective, sample-sized and possibly randomized study. A potential selection bias could not be ruled out in this retrospective analysis as only patients with available data for the analysis scope were included in the data set. Furthermore, some potentially helpful prognostic information could have been missed during the data collection, like the presence of visceral metastases or previous therapies. The relatively short follow-up of the study could have affected the precision of the prognostic discrimination into all the original Meet-URO score subgroups. 10 However, the overall prognostic value of the Meet-URO score stratification in three subgroups was maintained. The Meet-URO score was developed as a prognostic tool. Its predictive value remains undetermined, as there is no control arm in both the investigations we conducted (i.e. with nivolumab in our previous validation 10 and cabozantinib in the present study). Moreover, a predictive role seems unlikely, considering that the prognostic value observed in the present study with cabozantinib was similar to that of nivolumab. 10 A prospective analysis is planned to validate the prognostic and assess the predictive value of the Meet-URO score in an mRCC population treated with immunotherapy combinations. Moreover, due to the relatively long study duration, the possibility that new front-line treatments (like immunotherapy combinations) might also impact prognostic factors while prolonging patients’ survival outcomes has to be considered. On the contrary, it is unlikely that the two independent prognostic factors added by the Meet-URO score to the IMDC classification, or the presence of bone metastases and the NLR, could be influenced by those treatments. Moreover, both of those factors resulted as clinical characteristics significantly different among the three risk patients’ subgroups confirming, although indirectly, their prognostic value in a different treatment setting.
Nevertheless, the present analysis confirms the higher prognostic accuracy of the Meet-URO than IMDC score in esteeming the prognosis of patients with mRCC treated with novel target therapy besides immunotherapy. Moreover, the Meet-URO variables are readily available, non-invasive and may be easily and freely calculated with the online web-calculator (available at: https://proviso.shinyapps.io/Meet-URO15_score/). These results may pave the way for future investigations of this score, especially in the emerging field of immune-based combination therapies.
Footnotes
Acknowledgements
S.E.R. and G.F. would like to thank the Italian Ministry of Health (Ricerca Corrente 2018–2021 grants) that financially support their current research focused on the identification of prognostic and predictive markers for patients with genitourinary tumours.
Authors’ note
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: S.E.R. received honoraria as speaker at scientific events and advisory role by Bristol-Myers Squibb and Astellas. U.D.G. serves as advisory/board member of Astellas, Bayer, Bristol-Myers Squibb, IPSEN, Janssen, Merck, Pfizer and Sanofi; received research grant/funding to the institution from AstraZeneca, Roche and Sanofi; and received travel/accommodations/expenses from Bristol-Myers Squibb, IPSEN, Janssen and Pfizer. G.P. serves as advisory boards/consulting for Astellas, AstraZeneca, Bayer, Bristol-Myers Squibb, Janssen, IPSEN, Merk, MSD, Novartis and Pfizer. G.L.B. reports personal fees from AstraZeneca, Janssen-Cilag, Boehringer Ingelheim and Roche and non-financial support from Bristol-Myers Squibb, AstraZeneca, MedImmune, Pierre Fabre and IPSEN, outside the submitted work. S.B. received honoraria as speaker at scientific events and advisory role by BMS, Pfizer, MSD, Ipsen, Roche, Eli Lilly, AstraZeneca, Pierre Fabre and Novartis. G.F. serves as advisory boards for Astellas, Janssen, Pfizer, Bayer, MSD and Merck and received travel accommodation from Astellas, Janssen and Bayer. The other authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.