
Abstract
Background:
Despite the survival advantage, not all metastatic renal cell carcinoma (mRCC) patients achieve a long-term benefit from immunotherapy. Moreover, the identification of prognostic biomarkers is still an unmet clinical need.
Methods:
This multicenter retrospective study investigated the prognostic role of peripheral-blood inflammatory indices and clinical factors to develop a novel prognostic score in mRCC patients receiving at least second-line nivolumab. The complete blood count before the first cycle of therapy was assessed by calculating neutrophil-to-lymphocyte ratio (NLR), derived NLR (dNLR), lymphocyte-to-monocyte ratio (LMR), platelet-to-lymphocyte ratio (PLR), systemic inflammation index (SII), and systemic inflammation response index (SIRI). Clinical factors included pre-treatment International Metastatic RCC Database Consortium (IMDC) score, line of therapy, and metastatic sites.
Results:
From October 2015 to November 2019, 571 mRCC patients received nivolumab as second- and further-line treatment in 69% and 31% of cases. In univariable and multivariable analyses all inflammatory indices, IMDC score, and bone metastases significantly correlated with overall survival (OS). The multivariable model with NLR, IMDC score, and bone metastases had the highest c-index (0.697) and was chosen for the developing of the score (Schneeweiss scoring system). After internal validation (bootstrap re-sampling), the final index (Meet-URO score) composed by NLR, IMDC score, and bone metastases had a c-index of 0.691. It identified five categories with distinctive OSs: group 1 (median OS – mOS = not reached), group 2 (mOS = 43.9 months), group 3 (mOS = 22.4 months), group 4 (mOS = 10.3 months), and group 5 (mOS = 3.2 months). Moreover, the Meet-URO score allowed for a fine risk-stratification across all three IMDC groups.
Conclusion:
The Meet-URO score allowed for the accurate stratification of pretreated mRCC patients receiving nivolumab and is easily applicable for clinical practice at no additional cost. Future steps include its external validation, the assessment of its predictivity, and its application to first-line combinations.
Keywords
Introduction
Over the past 5 years, immune checkpoint inhibitors (ICIs) have significantly improved the therapeutic landscape of metastatic renal cell carcinoma (mRCC).1,2 Indeed, in 2015, nivolumab was the first ICI approved for the treatment of mRCC patients progressing on, or intolerant to, a vascular endothelial growth factor receptor tyrosine kinase inhibitor (VEGFR-TKI), based on the survival improvement observed over everolimus within the Checkmate-025 trial.3,4 More recently, ICI-based combinations have become the novel first-line therapy standard of care, across the three International Metastatic RCC Database Consortium (IMDC) prognostic groups,5,6 although a particular efficacy has been documented in intermediate and poor risk patients.
Furthermore, after a first-line VEGFR-TKI, nivolumab remains one of the two standard second-line treatment options.1,2
Despite their efficacy, not all mRCC patients achieve a long-term benefit from ICIs, either given as single agent or in combination (20–30%).5,6 It should be noted that mRCC is often associated with a highly-variable clinical course, spanning from indolent to rapidly-progressing disease, 7 as a reflection of its well-known heterogeneity. 9
As a result, the identification of biomarkers to select patients most and least likely to benefit from immunotherapy is a clinically unmet need and a critical issue of clinical research. 9 Although new potential biomarkers (e.g. molecular and genomic signatures) are under investigation, no validated biomarker has yet to reach everyday clinical practice. 9
Cancer-associated inflammation has been associated with worse outcomes and lower therapeutic responses in cancer patients across different tumor types.10,11 Easily-achievable peripheral blood parameters, reflecting an inflamed state, have been investigated as potential biomarkers in different tumors (including RCC), settings, and therapies.12–16
In the era of ICIs, inflammatory indices have mostly been studied in advanced melanoma and non-small lung cancer patients,17–21 while fewer and smaller studies have been conducted in patients treated with immunotherapy for genitourinary tumors,22–25 including mRCC.4,26–38
The Meet-URO 15 is a multicenter, retrospective study investigating the correlation of baseline peripheral blood inflammatory indices with efficacy and activity outcomes in pre-treated mRCC patients receiving nivolumab in clinical practice. This leads to the development of a composite clinical prognostic score.
Material and methods
The study was approved by the regional ethical committee (Regional Ethical Committee of Liguria - registration number 068/2019) and was conducted in 34 Italian centers. It was performed according to the Declaration of Helsinki, Good Clinical Practice, and local ethical guidelines. All living patients enrolled in the study signed a written informed consent.
Study population
A multicenter retrospective analysis was conducted, collecting clinical data and laboratory parameters from mRCC patients receiving nivolumab in a real-world setting.
The main inclusion criteria included: cytologically or histologically confirmed mRCC and at least one completed infusion of nivolumab given, as standard clinical practice, as a second or further treatment line. Included among the exclusion criteria was a history of any previous immunotherapy.
Treatment
Nivolumab was initially administered intravenously at a dose of 3 mg/kg every 2 weeks and, since May 2018, at the fixed dose of 240 mg every 2 weeks, or 480 mg every 4 weeks, according to local clinical practice. The treatment was continued until disease progression, unacceptable toxicity, death, or patient choice. Patients with radiological disease progression who experienced clinical benefit could continue to be treated beyond progression in accordance with physician decision-making.
Inflammatory indices
A complete blood count (CBC) collected before the first cycle of nivolumab was assessed. From the CBC we calculated the following ratios: neutrophil-to-lymphocyte ratio (NLR), derived NLR (dNLR) [neutrophils/(white blood cells – neutrophils)], lymphocyte-to-monocyte ratio (LMR), and platelet-to-lymphocyte ratio (PLR).
In addition, two combinations of ratios were assessed: systemic immune-inflammation index (SII), calculated as platelet x neutrophil/lymphocyte, and systemic inflammation response index (SIRI), calculated as monocyte x neutrophil/lymphocyte.
Cut-off determination of the inflammatory indices
As many thresholds have been explored, but none validated, in mRCC patients treated with immunotherapy, the cut-off values for inflammatory indices were determined using time-dependent receiver operating characteristic (ROC) curves with the Liu approach, maximizing the concordance probability function.39–42 The ROC curve was calculated at the time point corresponding to the median overall survival (mOS). An internal validation using 500-times bootstrap re-sampling was performed. For each index, the area under the curve (AUC), the sensitivity, and the specificity according to the cut-offs were reported.
Study endpoints
The primary endpoint was overall survival (OS), which was calculated from first nivolumab administration until death, censored at last follow-up for patients who were alive.
The secondary endpoints included progression-free survival (PFS), overall response rate (ORR), disease control rate (DCR), and duration of response (DOR).
PFS was defined as the time from the first nivolumab administration until first radiographic/clinical progression or death, whichever occurred first, censored at last follow-up for patients who were alive without progression.
ORR and DCR were defined as the sum of complete response (CR) plus partial response (PR), and the sum of ORR and stable disease (SD), respectively, as the best response to treatment. The DOR was calculated from the date of CR/PR until first radiographic/clinical progression or death, whichever occurred first, censored at last follow-up for patients who were alive without progression.
Radiological assessments consisted of a computed tomography (CT) scan of the chest-abdomen-pelvis and of the head (whenever clinically indicated), performed at baseline and every 2–4 months of treatment, according to local clinical practice, or whenever progression was clinically suspected. Tumor response was assessed in each center, referring to the Response Evaluation Criteria in Solid Tumours (RECIST) criteria version 1.1 and defined as CR, PR, SD, and progressive disease (PD). 43
Statistical analysis
Patients’ characteristics were presented using absolute frequency and percentage for categorical variables and by median and range for quantitative variables.
The Kaplan–Meier method was used to estimate survival curves of OS, PFS, and DOR. 44 Differences were considered statistically significant when the p-value (p) was <0.05.
Univariable logistic regression analyses were used for the association of each index and clinical characteristics with ORR and DCR. Results were reported as odds-ratios (ORs) with a 95% confidence intervals (CIs).
Univariable and multivariable analyses were performed using the Cox proportional hazard-regression model, estimating hazard ratios (HRs) and their 95% CIs.
In the univariable analyses, each inflammatory and clinical factor was assessed in correlation with all endpoints. Only factors with a p < 0.10 at the level of univariable analysis were assessed in the multivariable analyses for OS. Due to a strict correlation among the inflammatory indices, those predictive of OS were included separately in the multivariable analyses, together with the clinical factors. Only factors with a p < 0.05 in the multivariable analysis were kept in the multivariable model.
For each multivariable model, the discriminatory ability as defined by the Harrell’s c-index was calculated: a higher c-index represented a better capability of the multivariable model to separate patients with and without the event. The stability of the c-index was guaranteed by a 500-times bootstrap resampling with replacement. Missing values for indices were imputed (see eMethods in the supplemental materials). The multivariable model with the highest c-index was chosen for being the basis of the prognostic score.
All statistical analyses were performed using the software Stata v.16 (StataCorp 2019) and R v.4.0.2.45,46
Prognostic score
The selection procedure for the prognostic score and the parameter estimation from the Cox model were internally validated using the bootstrap approach (see eMethods in the supplemental materials for details).
To consider the possible overfitting during building and estimation of the prognostic score, a bias-corrected estimate of the discriminatory ability (c-index) was calculated with 500 bootstrap samples using the design package in R.
The prognostic score was calculated using the regression coefficient-based (Schneeweiss) scoring system, where the weight assigned to each factor in the score was defined based on the regression coefficient obtained from the Cox regression model. 47
Finally, the prognostic score was stratified in risk strata according to the likelihood-ratio test and after checking of the survival estimates of the score.
Results
Patients’ characteristics
A total of 571 mRCC patients were included in the analysis. Patients’ characteristics are summarized in Table 1 and eFigure 1 in the supplementary material.
Patients’ characteristics.

IMDC, International Metastatic RCC Database Consortium; MSKCC, Memorial Sloan Kettering Cancer Center.
Most patients were male (70%), and the median age was 61 years (range: 49–73 years). The majority of patients had clear-cell RCC histology (84%), and previously underwent nephrectomy (88%).
From October 2015 to November 2019, 69% of patients started nivolumab as second-line therapy, 21% as third-line, and 10% as further lines. At the time of treatment with nivolumab, a IMDC risk-score was available for 556 patients: it was favorable, intermediate, and poor in 23%, 65%, and 12% of patients, respectively. Lymph node, visceral, and bone metastases were present in 53%, 89%, and 36% of patients, respectively.
Response and survival outcomes in the overall population
At the time of data cut-off (July 2020), with a median follow up of 16.3 months, 76% of patients experienced PD, 14% were treated beyond progression, 21% were still on treatment, and 45% had died. The mOS was 29.5 months (range: 22.7–45.6) while the median PFS (mPFS) was 7.3 months (range: 5.8–9.2). The ORR and DCR were 31% and 62% respectively, while the median DOR (mDOR) was 29.9 months (range: 20.3–36.1).
The identification of the indices’ cut-offs on OS
The cut-off values of the inflammatory indices identified were 3.2 for NLR, 1.8 for dNLR, 2.6 for LMR, 176 for PLR, 720 for SII, and 2078 for SIRI. For each cut-off, the c-index, the sensitivity, and the specificity are shown in eTable 1 in the supplementary materials.
Univariable analyses for OS
All 571 patients were evaluable for univariable analyses (eFigure 1 in supplemental material). The univariable analyses for OS with the included patients are presented in eTable 2 in the supplemental material.
All 6 inflammatory indices significantly correlated with OS: higher NLR, dNLR, PLR, SII, and SIRI were associated with worse OS (p < 0.001), while higher LMR was associated with longer OS (p = 0.009) (eFigure 2 in supplemental material).
Among clinical parameters, only the IMDC score and the presence of bone metastases significantly correlated with OS, while a trend toward statistical significance was observed with the presence of lymph node metastases (p = 0.05) (eTable 2 and eFigure 4 in supplemental material).
For the univariable analyses for PFS, ORR, DCR, and DOR (see eTable 3, eFigure 3, and eFigure 5 in supplemental materials).
Moreover, univariable analyses has been graphically summarized in two forest plots (see eFigure 6 and eFigure 7 in supplemental material).
Multivariable analyses for OS
Among 571 patients of the entire cohort, 556 patients (97%) were evaluable for multivariable analyses (eFigure 1 in the supplemental material). In the multivariable analyses, each inflammatory index, IMDC score, and bone metastases were confirmed as independent predictors of survival. Inflammatory indices with a value higher (or lower for LMR) than the cut-off, less favorable IMDC risk-group, and the presence of bone metastases were associated with lower OS. Among inflammatory indices, the multivariable models with NLR, PLR, and SII were those with the higher discriminative ability (Table 2).
Multivariable analysis of inflammatory indices (NLR, PLR, SII) and clinical features (IMDC score, bone metastases).
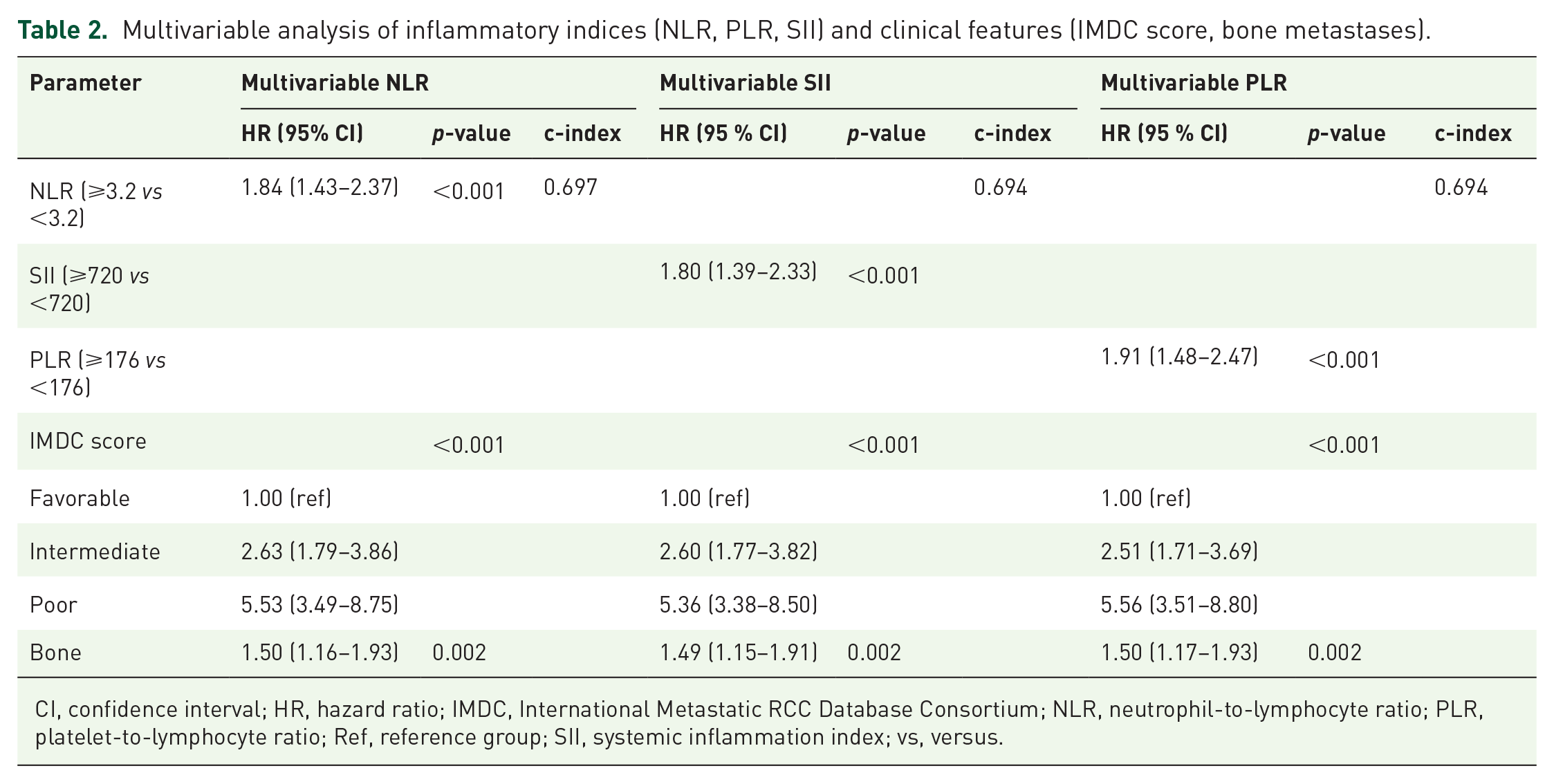
CI, confidence interval; HR, hazard ratio; IMDC, International Metastatic RCC Database Consortium; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; Ref, reference group; SII, systemic inflammation index; vs, versus.
Prognostic score
The multivariable model with NLR as inflammatory index, IMDC score, and bone metastases has the highest c-index (0.697); as a result, it was chosen for the development of the prognostic score (eFigure 1 in supplemental material). The discriminative ability was higher compared with the IMDC score (c-index: 0.642; 95% CI: 0.614–0.673) and the presence of bone metastases (c-index: 0.585; 95% CI: 0.553–0.618) when considered in a univariable analysis.
After 500 bootstrap replications, in 457 replications (91.4%) all three prognostic factors were included, while in 43 replications (8.6%) only NLR and IMDC score were included, confirming the stability of the multivariable model. The regression parameters and HRs calculated from the 500 bootstrap samples were very similar to those obtained from the original Cox model, suggesting an excellent internal validation (eTable 4 in supplemental material). The bias-corrected c-index for optimism from possible overfitting was 0.688 by the bootstrap procedure.
According to the bootstrapped Cox model coefficients and the Schneeweiss scoring system, 1 point was assigned to the presence of bone metastases, 2 points for a NLR ⩾ 3.2, 3 points for an IMDC intermediate-risk score, and 6 points for a IMDC poor-risk score. The prognostic score ranged from a minimum of 0 to a maximum of 9 points.
After checking the survival estimates for each point of the score, the 9 prognostic groups were combined into five prognostic categories characterized by very distinctive OSs. (Table 3, Figure 1). The reduction of the prognostic score to these five categories was also supported by a similar likelihood of the Cox regression model with the score in the original scale (0–9) or in the reduced form (likelihood-ratio test: 1.53; p = 0.91). The final prognostic score, called “Meet-URO score”, had a c-index of 0.691 (95% CI: 0.659–0.720).
Prognostic groups as the combination of an inflammatory index (NLR) and clinical features (IMDC prognostic groups and bone metastases).

2y-OS, overall survival rate at 2 years; CI, confidence interval; HR, hazard ratio; IMDC, International Metastatic RCC Database Consortium; mOS, median overall survival; n, number of patients; NLR, neutrophil-to-lymphocyte ratio; NR, not reached; Ref, reference group.

Kaplan–Meier curves for the OS of the prognostic score, according to 5 prognostic groups.
According to the Meet-URO score (Table 3, Figure 1), patients with no prognostic factors or the only presence of bone metastases were classified in group 1 (15%), with a mOS not reached and a OS rate at 2 years (2y-OS) of 83.3%. Patients with NLR ⩾ 3.2 or IMDC intermediate-risk score belonged to group 2 (35%), with a mOS of 43.9 months and a 2y-OS rate of 59.7% (p = 0.001).
Patients with an IMDC intermediate-risk score and one of the other two factors were classified in group 3 (28%), with a mOS of 22.4 months and a 2y-OS rate of 47.7% (p < 0.001).
Patients with an IMDC intermediate-risk score and the other two factors, or IMDC poor-risk score alone, or with one of the other two factors belonged to the prognostic group 4 (17%), with a mOS of 10.3 months and a 2y-OS rate of 26.7% (p < 0.001).
Patients with all factors (NLR ⩾ 3.2, IMDC poor-risk score, bone metastases) were classified in group 5 (17%), with a mOS of 3.2 months and a 2y-OS rate of 11.1% (p < 0.001).
The Meet-URO score is available online as web calculator at http://bit.ly/Meet-URO15_score.
The correlation between the Meet-URO score and the IMDC score
The joint frequency distribution between the Meet-URO score and the IMDC risk groups is shown in Table 4. According to our prognostic score, all patients within group 1 belonged to the IMDC favorable-risk group, in group 2 to the IMDC favorable and intermediate-risk group (22% and 78% respectively), in group 3 to the IMDC intermediate-risk group, in group 4 to the IMDC intermediate and poor-risk group (57% and 43% respectively), and in group 5 to the IMDC poor-risk group.
Correlation between prognostic score and IMDC risk groups.

IMDC, International Metastatic RCC Database Consortium; n, number of patients.
According to the IMDC score, the IMDC favorable-risk group was represented by groups 1 and 2 of the Meet-URO score (67% and 33%, respectively), while the IMDC intermediate-risk group was subdivided into groups 2, 3, and 4 (42%, 43%, and 15%, respectively). Finally, the IMDC poor-risk group was represented by groups 4 and 5 (61% and 39%, respectively).
Discussion
With the Meet-URO 15 study, we investigated the prognostic role of clinical factors combined with inflammatory indices in a real-world cohort of mRCC patients treated with immunotherapy. We found that pre-treatment inflammatory indices from peripheral blood, together with some clinical features, were associated with lower OS. The final prognostic score derived from these parameters is easy to obtain and provides a widely applicable prognostic tool for clinical practice at no additional costs. The additional value of the Meet-URO score lies in the identification of five prognostic groups with very distinctive OSs; thereby improving the accuracy of the well-known IMDC score. The latter was developed and validated in mRCC patients treated with different anti-angiogenic therapies and represents the gold standard for risk-stratification of mRCC patients in clinical practice and trials and in the first-line and second-line setting.5,48 The IMDC score, however, allows for a brief glance at the real (and much more complex) biology of a given RCC in a given patient; indeed, if time from diagnosis to treatment gives us an idea about tumor aggressiveness, all the other variables considered (i.e. Karnofksy Performance Status, hemoglobin levels, corrected calcium levels, neutrophil count, and platelet count) could be regarded as indirect indicators of an inflamed status.
Our score allows for an accurate risk stratification across all three IMDC groups, with the addition of the assessment of NLR, as a more precise indicator of inflammation, and the presence of bone metastases. Although their negative prognostic values are well-known in mRCC patients,15,49 both these two features emerge from our study as new prognostic factors for ICIs treatment, not included in the IMDC score.
Furthermore, our score splits each IMDC groups into two or three subgroups, allowing for the identification of those patients at the highest and lowest risk. This finding is the most innovative: the Meet-URO score allows for the identification of a subgroup of patients (group 1, 15%) within the IMDC favorable-risk group for which immunotherapy alone may be highly effective, and another subgroup of patients (group 5, 17%) within the IMDC poor-risk group for which immunotherapy would not be the best option; instead, a TKI or even best supportive care would be preferable. Despite the low numbers in the IMDC poor-risk group, this is in line with that reported in clinical trials in the same therapeutic setting (e.g. the Checkmate 025 trial and the Italian Expanded Access Program),3,50 and conclusions about these patients should be interpreted carefully.
Interestingly, the Meet-URO score has also identified a subgroup of patients with bone metastases, but in the IMDC favorable-risk category, and who have low NLR (group 1) associated with a very good prognosis. This shows that the prognostic value of bone metastases should be integrated into the clinical (IMDC score) and immunological context (NLR) of the patient.
In addition, our score subdivides the intermediate IMDC group into three prognostically distinct subgroups with a mOS ranging from 10 to 44 months: only group 3 mirrors the IMDC intermediate-risk group, while groups 2 and 4 are prognostically similar to the IMDC favorable and poor-risk groups, respectively. This is in line with previous evidence on the heterogeneity of the IMDC intermediate-risk group and the possibility to prognostically stratify it according to clinical or biological factors. It also reflects the need to identify clinical or biological factors to better stratify the prognosis of patients currently belonging to this group.51–53
In addition to the higher prognostic discriminative ability, the Meet-URO score is derived from a homogeneous population of patients treated with the same immunotherapeutic agent, better reflecting the current treatment scenario. This recognizes that the IMDC score was born in the pre-ICIs era.
One of the strengths of our work is the analysis of different inflammatory indices, which, individually, are significantly statistically associated with OS. This is, by far, the most important endpoint in oncological studies; as a whole, this brings to the study a strong internal consistency.
The inflammatory index NLR has been widely-investigated in RCC patients for its prognostic value, and slightly different thresholds have been reported.15,54,55 For this heterogeneity, we decided to calculate the inflammatory indices’ cut-offs from our homogeneous and large cohort. The cut-off identified in our analysis for NLR (3.2) is in line with those reported in the literature (range 2.5–5, mainly around 3) and this brings high plausibility to our study.15,54,55
High plausibility can also be derived from the presence of a rich body of literature on the prognostic role of inflammatory indices in different type of tumors and in different therapeutic settings.14,15 Similar studies on inflammatory indices in mRCC treated with nivolumab reported comparable results; however, it should be noted that they are mainly monocentric analysis investigating only one or few indices in a lower number of patients.4,26–38
Of course, limits should also be acknowledged: first and foremost, the retrospective nature of our study. In addition, it is important to reflect on the somewhat preliminary nature of these results, which necessitate external validation.
We plant to externally validate the Meet-URO score in an external cohort of patients treated with nivolumab to reinforce its prognostic value. In addition, we would also want to test our score on a VEGFR TKI-pretreated mRCC population to assess its potential predictive value, looking for a tool able to help us to select a VEGFR TKI or an ICI in at least the second-line setting.
The prognostic assessment of the early variation of the inflammatory indices or the score during treatment is planned. In addition, the Meet-URO score will be applied to the first-line ICI-based combinations to optimize mRCC patient selection in the context of the current complex treatment landscape. In fact, many different ICI-based combinations, both ICI+ICI and ICI+TKI, are emerging on the therapeutic horizon and therapeutic sequences are becoming an increasing clinical issue. This score, finely stratifying mRCC patients, could help to address the treatment choice in clinical practice and the design of ad-hoc clinical trials. Considering the prognostic discrimination ability of the Meet URO score, we believe that it could be used as a stratification factor in future prospective randomized trials and/or as part of eligibility criteria in studies assessing different oncological treatments according to specific prognostic groups.
The consideration that ‘very prognostically favorable’ patients could benefit from less aggressive therapies (ICI or TKI monotherapy) while ‘more prognostically unfavorable’ patients could be addressed to more aggressive combination therapies (ICI+ICI and ICI+TKI) should not be overlooked.
Conclusion
In this large Meet-URO 15 multicenter, retrospective study, we investigated simultaneously the prognostic role of clinical factors and inflammatory indices in pre-treated mRCC patients receiving nivolumab monotherapy. This novel score allows for the accurate prognostic stratification of mRCC patients treated with nivolumab, providing an easily and widely-applicable tool for clinical practice at no additional costs. Future plans include the external validation of the prognostic value and the assessment of its predictivity. The Meet-URO score will, in future, be applicated in patients receiving first-line ICI-based combinations.
Supplemental Material
sj-docx-1-tam-10.1177_17588359211019642 – Supplemental material for Inflammatory indices and clinical factors in metastatic renal cell carcinoma patients treated with nivolumab: the development of a novel prognostic score (Meet-URO 15 study)
Supplemental material, sj-docx-1-tam-10.1177_17588359211019642 for Inflammatory indices and clinical factors in metastatic renal cell carcinoma patients treated with nivolumab: the development of a novel prognostic score (Meet-URO 15 study) by Sara Elena Rebuzzi, Alessio Signori, Giuseppe Luigi Banna, Marco Maruzzo, Ugo De Giorgi, Paolo Pedrazzoli, Andrea Sbrana, Paolo Andrea Zucali, Cristina Masini, Emanuele Naglieri, Giuseppe Procopio, Sara Merler, Laura Tomasello, Lucia Fratino, Cinzia Baldessari, Riccardo Ricotta, Stefano Panni, Veronica Mollica, Mariella Sorarù, Matteo Santoni, Alessio Cortellini, Veronica Prati, Hector Josè Soto Parra, Marco Stellato, Francesco Atzori, Sandro Pignata, Carlo Messina, Marco Messina, Franco Morelli, Giuseppe Prati, Franco Nolè, Francesca Vignani, Alessia Cavo, Giandomenico Roviello, Francesco Pierantoni, Chiara Casadei, Melissa Bersanelli, Silvia Chiellino, Federico Paolieri, Matteo Perrino, Matteo Brunelli, Roberto Iacovelli, Camillo Porta, Sebastiano Buti and Giuseppe Fornarini in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors wish to really thank Dr. Luca Carmisciano of the Department of Health Sciences (DISSAL), Section of Biostatistics of University of Genoa, for developing the web calculator of the Meet URO score.
Meeting presentation
Partial preliminary analyses were accepted as poster presentations and online abstracts at the Genitourinary (GU) Cancers Symposium American Society of Clinical Oncology, 13–15 February 2020 and at the American Society of Clinical Oncology Virtual Annual Meeting, 29–31 May 2020.
Author contributions
Study concept and design was conducted by S.E.R., G.F., S.B., A.S., and G.L.B; G.F. and S.B. contributed equally as senior authors; A.S. and G.L.B contributed equally.
Acquisition and curation of data, all authors; statistical analysis, A.S.; interpretation of data, S.E.R., G.F., S.B., A.S. and G.L.B; drafting of the manuscript, S.E.R. and A.S.; critical revision of the manuscript for important intellectual content: S.E.R., G.F., S.B., A.S., G.L.B, C.P. and R.I; supervision, S.E.R., G.F. All authors have read and agree to the published version of the manuscript.
Conflict of interest statement
Dr Fornarini services advisory boards for Astellas, Janssen, Pfizer, Bayer, MSD, and Merck, and received travel accommodation from Astellas, Janssen, and Bayer. Dr Buti received honoraria as a speaker at scientific events and in an advisory role by BMS, Pfizer; MSD, Ipsen, Roche, Eli Lilly, AstraZeneca, Pierre-Fabre, Novartis. Dr Banna reports personal fees from AstraZeneca, Janssen-Cilag, Boehringer Ingelheim, Roche, and non-financial support from Bristol-Myers Squibb, AstraZeneca, MedImmune, Pierre Fabre, IPSEN, outside the submitted work. Dr De Giorgi services as an advisory/board member of Astellas, Bayer, Bristol-Myers Squibb, IPSEN, Janssen, Merck, Pfizer, and Sanofi, received research grant/funding to the institution from AstraZeneca, Roche, Sanofi, and travel/accommodations/expenses from Bristol-Myers Squibb, IPSEN, Janssen, and Pfizer. Dr Zucali services advisory boards/consulting for Pfizer, Bristol-Myers Squibb, MSD, IPSEN, Novartis, Roche, Amgen, AstraZeneca, Sanofi, Janssen, and Astellas. Dr Masini received personal fees as a speaker from Astellas, as a consultant from IPSEN, MSD, and Janssen, and for travel accommodation from BMS, Pfizer, Astellas, Janssen, and IPSEN. Dr Procopio services advisory boards/consulting for Astellas, AstraZeneca, Bayer, Bristol-Myers Squibb, Janssen, IPSEN, Merk, MSD, Novartis, and Pfizer. Dr Cortellini receives speaker fees/grant consultancies from Astrazeneca, BMS, MSD, Roche, Novartis, and Astellas. Dr Morelli received grants from MSD and Pfizer. Dr Bersanelli received research funding to the institution from Roche, Pfizer, Seqirus UK, AstraZeneca, Bristol-Myers Squibb, Novartis, and Sanofi, and received personal fees for advisory role, copyright transfer, consultancies, and as speaker at scientific events from Sciclone Pharmaceuticals, Bristol-Myers Squibb, AstraZeneca, Pierre-Fabre, Novartis, and Pfizer. The other authors have no conflicts of interest to disclose.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Italian Ministry of Health (Ricerca Corrente 2018–2021 grants) that financially support their current research focused on the identification of prognostic and predictive markers for patients with genitourinary tumors.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.