
Abstract
Due to occupational asbestosis exposure, the incidence of malignant pleural mesothelioma (MPM) has continuously increased over the last 30 years, with a plateau anticipated around the year 2030 in Western countries. Molecular MPM carcinogenesis involves alterations of NF2, RASSF1, LATS2WT1, p16, as well as BAP-1tumor-suppressor genes, which usually regulate apoptosis, cell invasion, motility, cell division, chromatin remodeling, as well as control of DNA repair. In few selected patients, debulking surgery consisting of pleurectomy-decortication is carried out, resulting in unsatisfactory long-term results. For about 15 years, first-line chemotherapy has been primarily based on a doublet of pemetrexed and cisplatin. Adding the monoclonal antibody bevacizumab (Avastin®), which targets vascular endothelial growth factor (VEGF), has been shown to improve overall survival (OS) by nearly 19 months. The emergence of immune check-point inhibitors (ICIs) in MPM treatment has recently been associated with substantial survival improvements in both second- and first-line settings. Similarly to non-small-cell lung cancer (NSCLC) patients, on-going trials are presently exploring the chemotherapy-ICI combination in MPM management, and depending on their results, this combination could represent a further major advance in this previously orphan disease. The current article reviews recent clinical trial results, as well as future clinical developments in this moving field.
Introduction
In 2016, the randomized phase-3 trial ‘MAPS’ assessing pemetrexed–cisplatin–bevacizumab triplet in malignant pleural mesothelioma (MPM) demonstrated the superiority of such triplet over cisplatin and pemetrexed doublet. 1 However, median overall survival (OS) of the experimental arm was only 18.8 months, emphasizing the need of new therapeutic standards. Immune system targeting drugs then emerged as potentially interesting for MPM treatment. 2 Owing to chronic inflammation due to asbestosis fiber deposits in pleural space or deep lung, the immune system has been suspected to play a major role in the MPM pathogenesis, which is still imperfectly understood. Indeed, improved outcomes were reported to correlate with higher intra-tumor infiltration by cytotoxic CD8+ T-cells. 3 Conversely, high tumor expression of programmed cell death-ligand 1 (PD-L1, aka B7-homolog 1, B7-H1), which inhibits T-cell function via binding the programmed cell death-1 (PD-1) protein at the T-cell surface, was associated with poor prognosis in several retrospective series on mesothelioma patients. Among the different immunotherapies that have so far been evaluated owing to their ability to restore anti-tumor immune responses in cancer patients, immune checkpoint inhibitors (ICIs) have generated the most attention due to their clinical efficacy, particularly in melanoma and non-small-cell lung cancer (NSCLC) patients. 4 Cytotoxic T-lymphocyte-associated protein (CTLA-4) is one of these checkpoint inhibitor proteins, expressed at cell surface of naïve T-cells. This protein interacts with B7 protein expressed by antigen presenting cells (APCs) like dendritic cells, which was revealed to impair T-cell activation by APC. This interaction was reported to occur early in the immune response, at the so-called ‘priming’ phase, presumably within regional lymph nodes close to cancer sites. Generally, the PD-1/PD-L1 pathway is thought to play a role within the tumor microenvironment itself, at the effector phase of immune responses to cancer. 4 In contrast with historical studies using systemic or local intra-pleural interleukin 2 or vaccines, which are not addressed here, several studies focused on ICIs: targeting the PD-1/PD-L1 pathway have generated promising results that will be the topic of this review.
Biological background
Clinical ICI efficacy has been claimed to correlate with high tumor mutational burden, as in the case of melanoma or NSCLC patients, whereas mesothelioma was consistently reported to harbor low mutation numbers per megabase of genomic DNA. 5 However, instead of the mutational burden by itself, it is probably rather the type of mutated genes that enhances the mutational burden and plays a major role. We know very little about which genes could drive ICIs’ potential efficacy in MPM. Yet, it may be assumed that p16 (somatic mutations, deletions, or gene promoter methylation in 22% of MPM samples6,7) and BAP1(somatic mutation in 23% of MPM samples 5 ) could possibly drive such effect, given that they both regulate cell cycle arrest, DNA repair, or chromatin remodeling. Hippo gene pathway alterations (RASSF1A promoter gene methylation in 30% of MPM samples,8,9 NF2 truncation mutations in 19% of MPM cases, 5 MST1/hippo promoter gene methylation in 8.5% 10 of MPM cases, or LATS2 mutations in 11% or MPM)5,11 could influence anti-tumor immune responses by governing YAP transcriptional co-activator activity state. YAP actually controls transcription of multiple immune genes including cytokine CXLC5 able to attract CXRC2-expressing myeloid-derived suppressor cells (MDSCs), 12 while cross-talks between Hippo/YAP pathway and TGF-β or JAK-STAT pathways that are involved in immune response regulation have similarly been described. 13 However, based on the rich inflammatory stromal component of these tumors, especially in the sarcomatoid or biphasic subtypes, the common view of a so-called ‘hot’ tumor has emerged, with tumor stromal infiltration by mono-macrophage cells, T-lymphocytes, or even neutrophils.
Several retrospective series paved the way for our knowledge on PD-L1 mesothelioma cell expression. However, the use of different antibodies and immune-staining automats yielded contradictory results. Almost all pharmaceutical companies that have developed therapeutic anti-PD-1 or anti PD-L1 antibodies have also developed their own associated diagnosis assay, rendering cross-comparisons rather difficult. Indeed, Roche promoted the SP142 clone for Ventana autostainer pertaining to atezolizumab trials, providing tumor staining of lower intensity than the other antibodies, yet able to stain PD-L1 expressed by infiltrating immune cells. To develop pembrolizumab, Merck used the 22 C3 clone from Dako, along with Dako autostainer. Bristol Meyers Squibb (BMS) used either the SP263 clone from Roche-Ventana or 28.8 clone from Dako in the nivolumab trials, while Astra-Zeneca used only the SP263 clone. All these antibodies have been extensively compared in cross-comparison studies based on NSCLC samples.14–16 To summarize these studies, the only antibody with diverging quantitative and qualitative results is the SP142, whereas all other antibodies provide rather concordant results. For mesothelioma tissue samples, such systematic comparison has not yet been published, with tumor PD-L1 staining being overall weaker than in NSCLC samples. Nevertheless, the generalized use of SP263 and E1L3N antibodies for routine practice, whatever the histological tumor type, has actually smoothened the discrepancies among laboratories and studies, 16 along with protocols adapted to the different staining automats.
Mansfield et al. 17 reported a 40% PD-L1 (B7-H1) positivity rate in 106 patients, with a 5% cutoff, when both cytoplasmic and membranous staining were considered, but only 24% when the analysis was restricted to membranous staining. Cedres et al. 18 also found 20% positivity in their 77 specimens out of a 119 retrospective series when applying an E1L3N monoclonal antibody, with a generally admitted 1% positivity cutoff. More recently, an Australian group 2 employed tissue microarrays and E1L3N clone using 311 specimens, 30% of which were of non-epithelioid subtypes. While PD-L1 membranous expression in ⩾5% tumor cells, regardless of intensity, was revealed in 42% of patients, only 9.6% displayed PD-L1 positivity of moderate to high intensity in at least 50% tumor cells. This was shown to correlate with non-epithelioid histology. In this large series of patients, PD-L1 tumor expression reportedly correlated with a significantly worse OS (median OS: 5.33 months vs 11.33 and 13.5, in patients with highly positive, positive, and negative PD-L1 staining, respectively, hazard ratio (HR) = 2.37). In multivariate analysis, the worse prognosis was maintained when both histological categories including epithelioid and non-epithelioid types were analyzed separately.
In the MAPS Phase-3 study, 1 E1L3N clone was employed in diagnostic specimens from 214 patients with remaining available tissue that were accrued. In this study, with a cutoff set at 1% of membranous staining regardless of intensity, only 36% of patients turned out to be positive. Likewise, there was a significantly higher rate of positivity in sarcomatoid or biphasic tumors (68% of positive specimens vs 29.6% in epithelioid, p < 0.001). 19 With this 1% cutoff, median OS was 12.3 months in patients with PD-L1-positive tumors compared with 22.2 in PD-L1-negative tumor patients.
Raffit Hassan’s group studied PD-L1 expression on tumor cells and infiltrating lymphocytes using samples from 65 patients with malignant effusions from pleural and peritoneal mesotheliomas. 20 The authors found 41 (63%) patients to be PD-L1 positive based on a 5% cutoff for positivity, yet they provided no details on the antibody used. These patients were reported to exhibit a worse OS (median OS: 23.0 months vs 33.3 months), though the difference did not reach statistical significance. More interestingly, in nine mesothelioma effusion samples evaluated, the investigators found a fraction of floating cells expressing PD-L1 ranging from 12% to 83%. In seven patients with paired malignant effusion and peripheral blood mononuclear cell (PBMC) samples, PD-L1 expression was significantly higher on CD3-positive T-cells identified in malignant effusions, as compared with PBMCs (p = 0.016). The numbers of CD14-positive PD-1-positive cells were similarly increased in malignant effusions compared with PBMCs (p = 0.03).
Finally, a series of primary diffuse pleural mesotheliomas including the epithelioid (n = 148), biphasic (n = 15), and sarcomatoid (n = 12) histological types was recently evaluated using the E1LN3 antibody for cancer stem cell markers and for PD-L1.
21
Overall, 33% of analyzed tumors (57/175) contained PD-L1
Second-line trials using single-therapy with anti-CTLA-4 monoclonal antibodies
CTLA-4 was the first checkpoint targeted by clinical trials involving MPM patients (Table 1). First encouraging results were reported in patients with chemotherapy-resistant advanced malignant mesothelioma. Tremelimumab was employed in these trials. The open-label, single-arm, phase-2 trial (MESOTTREM- 2008) 24 assessed this selective human immunoglobulin IgG-2 monoclonal antibody directed against CTLA-4 in MPM patients. Performance status (PS) 0–2 patients with measurable lesions, received second-line tremelimumab 15 mg/kg intravenously once every 90 days until progressive disease or severe toxicity. The trial’s primary endpoint was overall response rate (ORR), aiming a 17% target ORR, yet without a central independent response assessment. Most patients (25/29, 86%) received a standard first-line treatment with platinum combined with pemetrexed. Overall, 23 (79%) of 29 patients had documented disease progression within 6 months of first-line platinum-based chemotherapy, and 15 (68%) of them progressed during chemotherapy. Thus, one-fifth of these patients (21%) displayed indolent disease, progressing beyond 6 months of platinum-based first-line treatment. Given that only two therapeutic responses were observed, this trial should have been considered negative. In seven patients, more stable disease was observed, resulting in a 31% of disease control rate (DCR). The trial’s authors interpreted these data as encouraging, in spite of recruiting patients with possibly slowly growing tumors. Median duration of disease control was estimated at 12.4 months. Notably, the two responder patients displayed long-lasting response over 6 months, which grabbed the investigators’ attention. Median progression-free survival (PFS) of the study’s whole cohort was 6.2 months, median OS was 10.7 months, with a 2-year survival rate of 37%. However, no data on subsequent therapies were reported that could have helped interpret the OS data. Tremelimumab’s safety profile was found to be favorable, with only 14% of patients exhibiting grade 3–4 toxicities.
Clinical trials assessing anti-CTLA-4 monoclonal antibody single-therapy in mesothelioma patients.
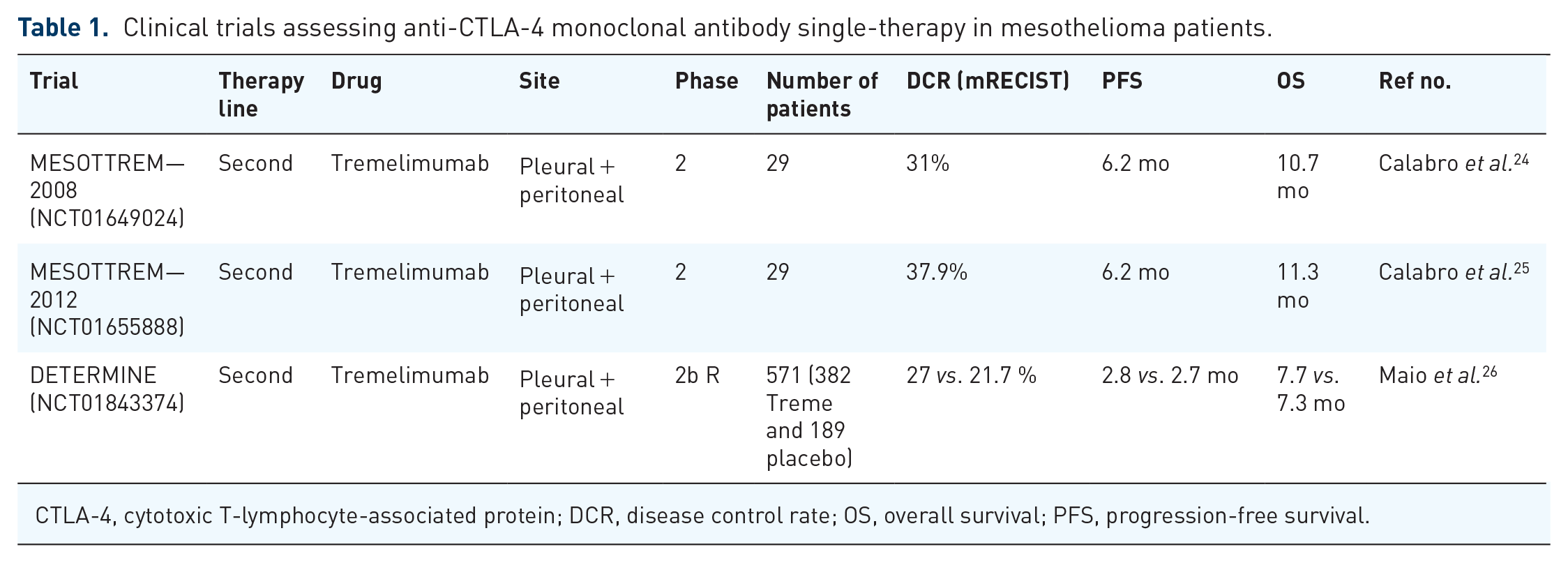
CTLA-4, cytotoxic T-lymphocyte-associated protein; DCR, disease control rate; OS, overall survival; PFS, progression-free survival.
The same investigators reported a second academic open-label, single-arm, phase-2 study (MESOTTREM- 2012), 25 using an ‘intensified’ tremelimumab schedule, at 10 mg/kg every 4 weeks for six doses, then every 12 weeks thereafter, until progression or toxicity. The primary endpoint was ORR based on iRECIST with a 17% ORR target rate. In this trial, patients with progressive disease at the first tumor assessment continued to receive tremelimumab if they did not suffer from deleterious clinical signs or progression symptoms. A pre-specified interim safety analysis did not detect any clinically relevant toxicity in the first 11 patients treated. Four patients displayed an immune-related partial response, including one at the first tumor assessment (12 weeks) and three others at the second tumor assessment (24 weeks). This resulted in only 13.8% ORR based on iRECIST, not clearly indicating significant activity. Even more puzzling, when the classical mRECIST for mesothelioma was applied, only one partial response was found. Using iRECIST, the proportion of patients with disease control was 51.7% (15 of 29 patients), with a consistent 10.9-month median duration of disease control. However, again, DCR was only 37.9% when applying mRECIST. Median immune-related PFS was 6.2 months, median OS was 11.3 months, and 1-year survival was 48.3%, all values being strictly comparable with the previous trial. Nevertheless, the seven patients with biphasic or sarcomatoid malignant mesotheliomas displayed a median OS of 15.8 months, which compared favorably with that observed in the seminal pemetrexed registration trial. Again, the safety profile was favorable, without any toxic death reported, and only a few and expected Grade 3–4 treatment-related adverse events (TRAEs).
Based on these data, tremelimumab was tested alone vs placebo in second- or third-line treatments in MPM patients in the DETERMINE large randomized Phase-IIb trial. 26 PS 0–1 patients with unresectable pleural or peritoneal malignant mesotheliomas and measurable lesions, having progressed after one or two previous systemic treatments for advanced disease, were eligible for inclusion. Patient randomization was stratified according to EORTC status (low risk vs high risk), therapy line (second-line vs third-line), and anatomic site (pleural vs peritoneal). Either intravenous tremelimumab at 10 mg/kg or placebo were given every 4 weeks for seven doses, and every 12 weeks thereafter, until progression or toxicity. About 571 patients were randomly assigned (2:1) by 105 study centers worldwide within 18 months to receive either tremelimumab or placebo. Overall, 382 patients were assigned to receive tremelimumab, and 189 received placebo. The patient median age was 66.0 years, with 95.5% displaying pleural mesotheliomas and 16.4% non-epithelioid subtype mesotheliomas. Of these patients, one-third had previously received two therapy lines, with 99% of them having received first-line pemetrexed-based therapy. Overall, 58% of patients displayed low-risk EORTC score and 95% Stage-IIIB/IV mesotheliomas. Patients were given a median number of three cycles. Nevertheless, no survival gain was obtained in the tremelimumab group, in comparison with the placebo group (median OS: 7·7 months vs 7·3 months, respectively; HR = 0.92; p = 0.408). Moreover, not a single patient subset did significantly benefit from tremelimumab, though non-significant trends were observed in the subgroup comprising 94 sarcomatoid and biphasic MPM (HR = 0.68) and in earlier-stage (⩽III) patients. Only eight patients exhibited confirmed partial response, supporting the total lack of tremelimumab single-therapy efficacy. Although 27% of patients had stable disease (⩾6 weeks post-randomization), the placebo arm behaved similarly, with 22% of patients displaying stable disease in this arm.
Second-line trials using single therapy with anti-PD-1 or PD-L1 monoclonal antibodies
As different anti-PD-L1 commercially available antibodies were used in the different studies listed below, the Tables 2 and 3 present the monoclonal antibody (mAb) clones employed to either select or stratify patients, with such anti-PD-L1 staining appearing more versatile in MPM than in NSCLC samples, with subsequently a debatable predictive impact.
Clinical trials assessing anti-PD-1 or PD-L1 monoclonal single antibody therapy in mesothelioma patients.

DCR, disease control rate; MPM, malignant pleural mesothelioma; NA, not available; OS, overall survival; PD-1, programmed cell death-1; PD-L1, programmed cell death-ligand 1; PFS, progression-free survival.
Keynote-158 is a large basket trial in which 118 MPM patients were enrolled.
Companion diagnosis assays for PD-L1 IHC in anti-PD-1 single-drug second-line trials.

IHC, immunohistochemistry; PD-1, programmed cell death-1; PD-L1, programmed cell death-ligand 1; UNK, unknown.
The first data originated from a Phase-Ib large multicenter, non-randomized, open-label, and multi-cohort ‘basket’ trial (Keynote 028), with an MPM stratum including 25 patients with PD-L1-expressing MPM; these patients were treated with the anti-PD-1 antibody pembrolizumab from Merck, at 10 mg/kg intravenously every 2 weeks. 27 To be included into the study, patients had to be PS 0-1, have measurable disease and histological MPM diagnosis, have failed to respond to standard therapy, or be considered ‘unable to receive chemotherapy’. PD-L1 expression was assessed using the 22C3 antibody (Merck, Kenilworth, NJ, USA) assay, with a cutoff set at ⩾1% of tumor cells or associated inflammatory cells upon using membranous staining, regardless of intensity. Among 83 patients with evaluable histological specimen, median age was 65.0 years, two-thirds were men, 72% displayed epithelioid histology, and one-third had received at least two previous therapy lines, with two patients entirely naive of any treatment. About 84% had previously been treated with pemetrexed and 88% been exposed to a platinum salts. Primary endpoint was an ORR exceeding 10% at an overall one-sided 8% alpha-level. Overall, 25 patients were eventually accrued, receiving at least one pembrolizumab dose. Safety was considered manageable, with classical immune-related adverse events (IRAEs) in 12% of patients, with a dose reduction required in only one patient. Moreover, Grade-3 AEs were recorded in only 20% of patients, and there was no Grade 4 or 5 at all.
The results turned out to be encouraging, reflected by 20% ORR, with 52% of patients exhibiting stable disease. Even more convincing was the durability of responses, given that the median duration of response (DOR) was 12 months (95% CI: 3·7-not reached (NR)), while the durability of stable disease (5.6 months) was in accordance with the duration observed in the DETERMINE placebo arm. Median OS was 18 months, with 62.6% of patients being alive at 1 year and two patients having received the maximal treatment length of 24 months, whereas two other responders were still under treatment at 22 months. Even more strikingly, four patients exhibited ⩾70% decrease in their tumor burden, clearly supporting drug activity, which had not be reported in previous anti-CTLA-4 trials.
Final results from a U.S. Phase-2 single-arm trial assessing the activity of fixed-dose pembrolizumab (200 mg every 3 weeks) in second-line setting (KEYNOTE-139, NCT02399371) confirmed both the activity and tolerability of such anti-PD-1 agent in pre-treated MPM patients. 28 Overall, 35 MPM patients, PS = 0–1, with disease progression after 1–2 prior regimens, one of which including pemetrexed-platinum doublet, and measurable disease and were treated using pembrolizumab 200 mg intravenously q21 days with first computer tomography (CT)-scan evaluation at 9 weeks. Their median age was 68 years, while 53% were PS = 0; epithelioid histology was revealed in 77%, 12% had peritoneal while 61% of patients had received only one prior treatment. Partial response according to mRECIST was observed in 14 patients (22%), while 26 displayed stable disease (56%), providing a 63% DCR at 9 weeks. Toxicity was estimated manageable using a centrally assessed 22C3 antibody-based immunohistochemistry assay, PDL1 expression was available for 62 patients: 45% were found negative (<1%) and 32% displayed low PD-L1 expression (1%–49%), whereas 23% presented with high expression (⩾50%). When used as a continuous marker, higher PD-L1 expression was associated with a higher response rate (ROC area under the curve = 0.69; 95% CI: 0.53–0.84). In patients with high PD-L1 expression, ORR was higher and PFS longer compared with those comprising no or low PD-L1 expression (0.021 and 0.034, respectively). Nevertheless, OS was not influenced by PD-L1 tumor content. Overall, 1-year PFS was 40.2% in high PD-L1 expression patients vs 9.3% in the others (p = 0.019).
Keynote-158 trial was another large basket, pembrolizumab second- or further-line trial, which accrued 118 MPM patients, with results published in 2021. 35 In these heavily pretreated patients (52% of patients with ⩾ two previous lines), only 10 (8%) exhibited an objective response with a median duration of 14.3 months, while nearly two-thirds were still on-going at 12 months. Median OS was encouraging at 10.0 months (95% CI: 7.6–13.4), yet median PFS was only 2.1 months (2.1–3.9). In total, TRAEs occurred in 14 (12%) patients. Overall, 19 (16%) patients suffered from Grade 3–4 TRAEs, the most common of which were colitis reported by three patients and pneumonitis displayed by two.
Finally, a Swiss registry analysis involving 48 MPM patients, PS 0-2, having progressed after pemetrexed-based single-line treatment, who were then treated with pembrolizumab off-label, was presented at 2017 ESMO meeting. 29 An investigator-based response analysis according to mRECIST found a 25% ORR and 53% DCR (11% for PS 2 patients vs 42% for the 19 PS 0-1 patients; 33% vs 72% for ORR and DCR, respectively). In the whole cohort, median PFS was 3.6 months and median OS 7.2 months, whereas PS 0-1 patients had a median OS of 10.2 months. Indeed, such retrospective data, without any central response assessment, should be considered cautiously, although such ‘real-life’ data could possibly support the Phase I–II activity data pertaining to second-line pembrolizumab. In this series, PD-L1 assessment revealed a clear correlation between pembrolizumab activity and increasing PD-L1 tumor cell expression, with all four patients >50% PD-L1 tumor cell expression exhibiting disease control, in comparison with 32% for PD-L1-negative patients (<1% PD-L1 stained tumor cells), with a significant 0.27 HR for PFS.
Convinced by these preliminary data, the ETOP group launched the ETOP 9–14 PROMISE-Meso trial. This study sought to compare, following one previous chemotherapy line, pembrolizumab 200 mg fixed-dose intravenously, given at Day 1 of each 3-week cycle, until progressive disease by iRECIST, for maximally 2 years, versus second-line single-agent chemotherapy by institutional choice, being either gemcitabine 1000 mg/m2 Day 1/Day 8, q3w, IV; vinorelbine 30 mg/m2 Day 1/Day, q3w IV; vinorelbine 60 mg/m2 Day 1/Day 8 q3w per os, with a cross-over permitted at progression. This Phase-3 trial was aimed to increase PFS data, as based on an independent review, from 3 to 6 months (HR = 0.58), requiring 142 patients to be accrued. The trial’s disappointing results were recently published. 33 Overall, 144 patients, PS 0-1, were randomized, with both arms being well-balanced in terms of demographical characteristics, resulting in no statistically significant difference between the pembrolizumab and chemotherapy arms in terms of PFS (3.4 months vs 2.5, respectively) or OS (10.7 months vs 11.7 months, respectively), even after adjusting for cross-over (63% of chemotherapy patients). Nevertheless, the best overall response, which was centrally reviewed, was significantly higher in the pembrolizumab arm (22%), compared with the chemotherapy arm (6%, p = 0.004 stratified). Indeed, median response duration of pembrolizumab was short, being 4.6 months, as compared with 11.2 months in chemotherapy-treated patients. PD-L1 tumor expression, which was assessed using E1L3N antibody, was not found to be associated with efficacy, irrespective of the cutoff selected (0%, 1%, or 50%). Moreover, no PFS or OS differences according to PD-L1 positivity defined by 1% cutoff were revealed. Indeed, this finding was weakened by the lack of evaluable PD-L1 results in 25–30% in the two arms, respectively. No specific safety signal was recorded, with 1.4% of TRAEs leading to death (n = 1) in each arm. In addition, 19.4% of Grade 3–5 TRAEs were reported in pembrolizumab patients versus 24.3% in chemotherapy-treated patients. Indeed, such disappointing results could be explained by a substantial number of patients being refractory to second-line therapy, meaning patients with disease progression during either pemetrexed-based first-line chemotherapy or within 3 months of completing such first-line treatment.
Another anti-PD-1 antibody, nivolumab (Nivo), was evaluated in second- or third-line settings in the NivoMes study, by a group from the Netherlands. 30 To be included in that trial, patients should have progressed after ⩾1 line therapy. Primary endpoint was DCR at 12 weeks, and the study sought to increase DCR from 20% to 40%. Patients received nivolumab 3 mg/kg, q2weeks, and were to undergo repeated biopsy and PBMC sampling at 6 weeks. Accrual was fast, with 34 patients, exhibiting 28 epithelioid and six sarcomatoid/biphasic types, enrolled in less than 1 year. Patients displayed standard epidemiological features, with a median age of 68 years, and 28 males. The trial was clearly positive, given that DCR was 29% at 6 months including two pseudo-progression cases, with an 23.5% ORR (n = 8) and 3.6-month PFS. The safety profile was as expected, with 26% Grade3–4 IRAEs yet one treatment-related death due to pneumonitis. Responses were seen in all groups, irrespective of PDL1 expression, although the small patient numbers precluded any definitive conclusion to be drawn.
A Japanese multicenter trial, MERIT (ONO-4538-41/JapicCTI-No.163247), assessed nivolumab in second- or third-line settings, in 34 advanced or metastatic MPM patients, with resistance or intolerance to pemetrexed and platinum-based combination therapy. 31 Primary endpoint was OR, and nivolumab was used at 240 mg flat dose q2weeks. The expected response rate was 19.2%, giving an 80% power at 5% alpha-level. Median age was 68.0 years, 29.4% of patients received two previous treatment lines, 79.4% exhibited epithelioid MPM, and 61% were PS1. The trial was positive, with 29.4% ORR and 67.6% DCR at 6 months, without any unexpected safety concerns. With a median follow-up of 16.8 months, median PFS was 6.1 months and median OS 17.3 months. PD-L1 status, which was determined using the Dako PD-L1 IHC 28-8 pharmDx test, clearly influenced survival. Indeed, median PFS was 7.2 months in PD-L1 tumor expression >1% patients, compared with 2.9 months for PD-L1-negative patients; median OS was 17.3 months in PD-L1-positive patients versus 11.6 months for PD-L1-negative patients. Grade-3 interstitial pneumonia or pneumonitis occurred in three of the 20 PD-L1-positive patients (15%). Based on the MERIT study results, nivolumab was approved in Japan for unresectable advanced or recurrent MPM patients, having progressed upon previous chemotherapy.
Results from the MPM strata of the multicenter non-randomized, open-label, and multicohort ‘basket’ Phase-Ib trial ‘JAVELIN’ (NCT01772004) were presented as a poster session at 2018 ASCO meeting. 32 This trial assessed the anti-PD-L1 fully humanized IgG1 avelumab in around 2,200 patients suffering from more than 15 cancer types. Overall, 53 patients exhibited unresectable pleural or peritoneal mesotheliomas, having progressed after platinum-pemetrexed combination therapy. These patients were then treated using avelumab, 10 mg/kg intravenously Q2W, until progression, unacceptable toxicity, or withdrawal. Patients had previously received one (n = 18), two (n = 15), or ⩾three (n = 20) therapy lines. After a median 24.8-month follow-up, an only 9.4% ORR was confirmed, with a median 15.2-month response duration, clearly contrasting with previous data. It must, however, be stressed that a greater number of patients were highly pretreated in this series. DCR was 58.5%, which is modest, median PFS was 4.1 months, and median OS only 10.9 months. However, in evaluable patients with PD-L1 + (n = 16) tumors (⩾5% tumor cell cutoff), ORR was 18.8%, whereas 6-month PFS did not differ compared with the whole series. Safety profile was acceptable, without any treatment-related death reported.
All these data supported the nivolumab versus placebo Phase-III academic UK ‘CONFIRM’ trial (Cancer Research UK trial number CRUK/16/022) in second- and third-line settings, which was recently presented at 2021 WCLC virtual meeting by Dean Fenell et al. 34 In this double-blind trial, nivolumab 240-mg intravenously q2w was compared with placebo in 332 mesothelioma patients in second-line setting, PS = 0–1, using a 2:1 randomization ratio. This resulted in 221 nivolumab-treated patients versus 111 placebo-treated patients, until progressive disease or toxicity. This trial met its co-primary PFS and OS endpoints, without any specific safety signals. After a median 17-month follow-up for the nivolumab arm, median OS was 9.2 months (95% CI: 7.5–10.8) for nivolumab-treated patients versus 6.6 months (95% CI: 0.55–0.94; HR = 0.72; p = 0.01) for placebo-treated patients. The 12-month OS was 39% and 26.9% in the nivolumab and placebo arms, respectively. Median PFS was 3.0 months in the nivolumab arm versus 1.8 months in the placebo arm (95% CI: 0.48–0.77, p < 0.001). Surprisingly, in epithelioid subtype patients, the median OS was 9.4 months (95% CI: 7.7–10.9) compared with 5.9 months (95% CI: 3.6–18.4) in non-epithelioid subtype patients, with even placebo-treated patients doing better than the latter (median OS = 6.7 months). PD-L1 tumor expression was not found to influence OS. Nevertheless, PD-L1-negative tumor patients did numerically better with nivolumab than with placebo, with a median OS of 9 months (95% CI: 6.6–11.1) versus 6.4 months with placebo (95% CI: 4.5–8.5).
Trials using combination therapy consisting of anti-PD-1 or PD-L1 and anti-CTLA-4 monoclonal antibodies
As in NSCLC or melanoma, a putative synergy was expected between anti-CTA-4 antibodies, acting at priming phase by impairing dendritic and T-cells interaction, and anti-PD-1 antibodies, acting at the effector phase by impairing T-cell inactivation by tumor cells. With this background in mind, IFCT 1501 MAPS2 trial (NCT 02716272) was launched. This randomized, non-comparative Phase-2 trial assessed the usefulness of anti-PD-1 mAb nivolumab, either as single therapy or in combination with the anti-CTLA-4 mAb ipilimumab (ipi) from BMS, in second- or third-line settings in MPM patients (Table 4). 36 These were MPM patients, PS 0-1, with histologically confirmed pleural unresectable mesothelioma, and measurable, documented progression (all CT-scanners were centrally reviewed). The patients were randomized according to 1:1 ratio between nivolumab (nivo) 3 mg/kg, q2weeks and nivolumab 3 mg/kg, q2weeks plus ipilumumab (ipi) at 1 g/kg q6 weeks. They were treated until progression or unacceptable toxicity for up to 2 years. Patient accrual was impressively fast, resulting in 125 patients recruited within 5 months in 25 French centers. Overall, 63 patients were allocated to nivolumab and 62 to the combination. Median age was slightly higher than in previous studies (72.3 and 71.1 years, respectively), likely reflecting less patient selection. Overall, 84% patients exhibited epithelioid histology, two-thirds were PS = 1, with slightly more males in the combination arm (85 vs 75%, respectively, not significant) and more patients having progressed beyond 3 months after last chemotherapy completion (66 vs 59%, respectively, not significant). Roughly 70% were second-line patients, with 86.4% having Stage III–IV tumors. PD-L1 tumor cell expression was centrally assessed, using both 28.8 Dako PharmDX™ and SP-263 Ventana™ assays with ⩾1% cutoff, and 41.4% and 45.2% of specimens were scored positive, respectively, with a surprisingly low concordance kappa index (κ = 0·56) while the same pathologists evaluated both assays. Drug delivery was good, yet better in the single-therapy arm, given that 49.2% and 38.7% of patients received at least 10 injections. The safety profile was, again, not unexpected, as reflected by slightly higher toxicity in the combination arm compared with the nivolumab arm, reflected by 26.2% Grade 3–4 AEs vs 12.7%. Three toxic deaths occurred, including one fulminant hepatitis and one encephalitis case, all in the combination arm.
Clinical trials assessing combination therapy of anti-PD-1 or PD-L1 plus anti-CTLA-4 monoclonal antibody in mesothelioma patients.

DCR, disease control rate; IHC, immunohistochemistry; NA, not available; OS, overall survival; PD-1, programmed cell death-1; PDL1, programmed cell death-ligand 1; PFS, progression-free survival.
The trial met its primary endpoint in both arms, with 44.4% DCR in the first 54 eligible patients in the nivolumab arm, versus 39.7% in the 63 ITT group patients; DCR was 50.0% in the first 54 eligible patients of the combination arm versus 51.6% in the 62 intention-to-treat group patients. Objective response rates were 18·5% (n = 10) and 27·8% (n = 15) in nivolumab and nivolumab + ipi, respectively. ORR was significantly increased in the PD-L1 positive patient subset, with both assays applied. Despite the observed low correlation (p = 0.003 for 28.8 assay), both ORR and DCR were significantly increased in patients with histological high PD-L1 expression (cutoff ⩾ 25% of membranous tumor cell staining).
Strikingly, waterfall plots of percentage change in tumor size from baseline at 12 weeks clearly confirmed a major activity in three and 10 patients exhibiting tumor shrinking of more than 60%, in the nivolumab and combination groups, respectively, irrespective of the histological subset. 40 Conversely, 12 and five patients, respectively, exhibited more than 60% of tumor size increase, with major and rapid tumor burden progression exceeding 80% observed in a few patients (six and two, respectively). This suggested some patients could have experienced ‘hyper-progression’ an aggressive pattern of progression, while MPM is a rather indolent disease, in line with observations by other authors in NSCLC settings.41–43
After a median 32.5-month follow-up, median response duration was 7.4 months in the nivolumab group vs 8.3 months in the combination group. More strikingly, median OS was 11·9 months (95% CI: 6.7–17.4) and 15·9 months (95% CI: 10.7–22.2), in the nivolumab and nivo + ipi groups, respectively, with a 2-year OS of 25.4%, (95% CI: 15.5–36.6) and of 31.7% (95% CI: 20.5–43.4) for nivolumab and nivo + ipi groups, respectively. No imbalance in post-discontinuation treatments received by patients was detected between both arms.
Another smaller, yet non-randomized trial (‘INITIATE’, NCT03048474) using the same design than the NIVOMES trial, carried-out by P. Baas et al., showed similar trends of treatment benefits. This trial involving 35 patients assessed the usefulness of administrating nivolumab (1 mg/kg/3 weeks vs /2 weeks as in MAPS-2) plus ipi (1 mg/kg/6 weeks) as second- or third-line treatment in MPM (85%) patients. 37 ORR and DCR at 12 weeks were 30% and 75%, respectively, with a 4.8-month PFS, yet still immature OS data.
A third single-arm Phase-II trial (‘NIBIT-MESO-1’; NCT02588131) evaluated combined 1 mg/kg tremelimumab and 20 mg/kg durvalumab given in four intravenous doses every 4 weeks, which was followed by durvalumab maintenance at the same dose and schedule for nine doses, as first- or second-line treatment for unresectable malignant mesothelioma patients. 38 This trial met its primary endpoint, with 11/40 (27·5%) patients exhibiting immune-related (ir)-partial response (median DOS: 16.1 months) and 25/40 (65%) ir-disease control, resulting in a median ir-PFS of 8 months (median PFS = 5.7 months) and median OS of 16.6 months (95% CI: 13·1–20·1). In this specific trial, baseline tumor PD-L1 expression displayed no predictive or prognostic value.
Finally, immunotherapy-based combinations were recently completed by the BMS-sponsored large randomized Phase-III CheckMate CA209-743 trial. This trial assessed the benefit of nivolumab + ipi combination versus standard frontline chemotherapy (platinum + pemetrexed for maximally six cycles) with OS as primary endpoint. 39 This recently published trial, which randomized 605 pleural mesothelioma patients, PS 0–1, actually met its primary endpoint in revealing a longer OS for nivolumab + ipi-treated patients (median OS = 18.1 months (95% CI: 16·8–21·4)) compared with those receiving standard first-line combination of pemetrexed plus platinum (median OS = 14.1 months, (95% CI: 12.4–16.2), HR = 0.74, (96.6% CI: 0.60–0.91), p = 0.002). There was no imbalance in terms of treatments administered at progression (45% and 48% in the chemotherapy and i.o. arms, respectively), and such OS results were obtained while 20% of chemotherapy patients received immunotherapy as subsequent therapeutic line, mainly using off-label anti-PD-1 drugs. There was no safety signal reported, with around 30% of treatment-related Grade 3–4 AEs in both arms, despite longer treatment median duration in the immunotherapy arm. Long-term survival was appealing, with a 50% improvement in 2-year OS, consisting of 41% in the double immunotherapy arm versus 27% in the chemotherapy arm, with an almost median 30-month follow-up. Given this background, it must be stressed that benefits with the double immunotherapy were observed in all patient subgroups, excepting patients aged at least 75 years old. Patients with epithelioid and non-epithelioid histological subtypes exhibited upon double immunotherapy a similar median OS of 18.7 and 18.1 months, respectively, whereas the latter subgroup experienced a poor survival with chemotherapy, consisting of a median OS of only 8.5 months versus 16.5 months for patients with epithelioid MPM. This difference accounted for the striking HR of 0.46 (95% CI: 0.31–0.68), though the OS difference did not reach statistical significance in the epithelioid subgroup. Notably, benefit of immunotherapy doublet was higher in PD-L1 > 1% tumor patients (HR = 0.69, 95% CI: 0.55–0.87) than in PD-L1 < 1% tumor patients (HR = 0.94, 95% CI: 0.62–1.40), whereas median OS data upon immunotherapy doublet were similar at 18.0 months and 17.3 months, respectively. PD-L1 positive patients derived less benefit from chemotherapy than from i.o., which further supports an adverse prognosis effect of tumor PD-L1 expression. Median PFS did not statistically differ between both arms, as often described in mesothelioma trials. This observation namely emphasizes both namely how difficult response assessment in MPM patients proves to be, as well as the long-term effect assessment of immuno-oncology drugs. Indeed, these latter drugs were associated with the same response rate than chemotherapy (40% and 43% respectively), while 32% of patients were still responding at 2 years with i.o. versus only 8% with chemotherapy. Of note, the 2-year PFS was 16% versus 7%, respectively. However, it should be mentioned that 19% of patients progressed within 2 months in the immunotherapy arm, suggesting that some patients could have experienced what is called ‘hyper-progression’, 43 by some authors, This supports the need for an early tumor evaluation upon immunotherapy as soon as 6 weeks. Based on such results, the combination of nivolumab plus ipi was registered in 2020 by the United States Food and Drug Administration (FDA), while European registration is expected to occur in 2021. An exploratory analysis, since PDL1 was not a stratification factor, showed that patients with positive tumor PD-L1 expression who received the combination immunotherapy displayed a 18.0 median OS versus 13.3 months for patients with positive PD-L1 tumor, when treated by chemotherapy (HR = 0.69 (0.55–0.87)). Conversely, patients with negative PD-L1 tumor exhibited a 17.3 months OS with immunotherapy versus 16.6 months with chemotherapy (HR = 0.94 (0.62–1.40)). However, the interaction test was not significant, possibly limited by small samples sizes. PD-L1 tumor staining either positive or negative, thus did not significantly impact OS of patients treated by the combination immunotherapy with 17.3 and 18.0 median OS respectively, supporting the findings of MAPS2 trial, in which PD-L1 tumor positive staining associated with longer OS of MAPS2 patients treated by single-agent nivolumab as compared to patients with negative tumor PD-L1 staining (HR = 0.59), although statistical significance was not reached again because small sample sizes. Conversely another exploratory analysis identified a predictive expression signature of four genes (PD-L1, LAG-3, CD8A, and STAT1), which predicted longer survival in patients treated with immunotherapy, when these genes exhibited high expression (21.8 vs 16.8 months, HR = 0.57, 95% CI (0.40–0.82)), with one third of high-expressing patients alive at 3 years, while such signature did not influence the survival of patients who received chemotherapy (13% of 3-years survivors whatever was the level of expression). Such signature should therefore deserve a prospective evaluation in another set of MPM patients treated by this immunotherapy combination.
Trials using combination therapy with anti-PD-1 or PD-L1 monoclonal antibodies and pemetrexed-platinum-based chemotherapy
The well-documented activity of immunotherapy in MPM patients in second-line and now even first-line settings led some investigators to assess the chemo-immunotherapy strategy, being inspired by the results of such combination in stage-IV non-small-cell cancer patients (Table 5).
Trials using combination therapy with anti-PD-1 or PD-L1 monoclonal antibodies and pemetrexed–platinum based chemotherapy.

DCR, disease control rate; IHC, immunohistochemistry; OS, overall survival; PD-1, programmed cell death-1; PDL1, programmed cell death-ligand 1; PFS, progression-free survival.
Two single-arm Phase-II trials assessed durvalumab, an anti-PD-L1 monoclonal antibody form Astra-Zeneca, combined with the cisplatin-pemetrexed doublet, in the US (PrE0505; NCT 02899195; n1 = 55, results still awaited) and Australia (‘DREAM’ trial; n = 54). This latest trial’s final results were recently published. 44 First-line MPM patients, PS = 0–1, received cisplatin-pemetrexed at standard dosing, along with durvalumab 1125mg q3 weeks, for six cycles as induction therapy; in case of disease control, they were treated up to 17 cycles of maintenance durvalumab 1125mg q3 weeks, until progression or toxicity. The primary endpoint was PFS at 6 months, using mRECIST and a Simon-2 stage design. Again, accrual run very fast with 54 patients enrolled by 10 sites within 10 months, demonstrating the unmet need for efficient systemic treatment in MPM patients. Median age was 68 years, 60% of patients were PS = 0, and 83% presented with epithelioid histological-type. Dose-intensity of both chemotherapy and durvalumab was excellent, as 97% of patients received six doses of platinum with only 13 patients (24%) for whom cisplatin was converted to carboplatin, and with a median number of 11.5 durvalumab doses (94% dose-intensity). Confirmed ORR was 48%, along with 37% stable disease patients, when using mRECIST for evaluation, with two patients experiencing a pseudo-progression (58% iRECIST ORR). Overall, a remarkable 85% DCR was thus obtained, with six patients experiencing major tumor shrinkage of ⩾80%. With a median 28-month follow-up, median PFS was 6.9 months (95% CI: 5·5–9·0), and 6-month PFS was 57%. The median OS was 18.4 months (95% CI: 13.1–24.8); 24-month OS was 37% (95% CI: 26–52). Overall, 15% of patients experienced Grade 3–4 IRAEs, 13% experienced Grade 3–4 neutropenia, 7% Grade 3–4 anemia, with 66% of patients experiencing Grade 3–5 adverse events, including five deaths (9%) during study treatment including one tumor progression, without any death adjudicated to durvalumab.
These results supported the launching of a Phase-3 trial titled ‘DREAM3R’’ (NCT04334759) in the first-line setting, with OS as primary endpoint, sponsored by PrECOG and the ALTG Australian group. This trial is designed to recruit 480 patients until 2024.
In the meantime, the results of the IND227-IFCT1901 (NCT02784171) Phase 2–3 trial, which was initiated by the Canadian Cancer Trials Group along with the French Intergroup (IFCT) will be made available. This trial seeks to explore the efficacy of a frontline therapy combining pemetrexed-cisplatin with pembrolizumab versus cisplatin and pemetrexed alone. Patient accrual was completed in November, 2020, with 520 MPM patients recruited.
Therefore, we should know very soon whether chemo-immunotherapy combination is as efficacious as double immunotherapy for MPM treatment. Should this be the case, this would represent a major advance in the care of this previously orphan disease, for which sensitivity to checkpoint inhibitors was put in the forefront.
Conclusion
MPM is a low mutational burden tumor, with only moderate PD-L1 expression levels in MPM tissue samples. Nevertheless, data are accumulating supporting the use of modern immunotherapy in MPM patients, using anti-PD-1 or anti-PD-L1 antibodies, in combination with (first-line setting) or without (second-/third-line settings) an anti-CTLA-4 antibody (yet not anti-CTLA-4 antibody single-therapy).
While available data actually support the adverse prognostic effect of PD-L1 expression in MPM, more and more data are accumulating, suggesting a favorable predictive effect of such PD-L1 tumor expression in MPM patients treated with anti-PD-1 or PD-L1 single-drug antibodies. However, this predictive effect is often obscured in MPM, as compared with NSCLC, by the lower and overall heterogeneous expression of PD-L1 by mesothelial tumor cells.
Phase-2 results with pembrolizumab or nivolumab-based therapy appear to be concordant when considering fit, not-refractory, and pre-treated MPM patients, given than more than 300 patients have now been treated in clinical trials, with remarkable PFS and long-term OS data. In the literature, similar data had never been reported with previously available cytotoxic drugs, which rarely resulted in more than 25% ORR and significant PFS data exceeding 3 months. In particular, MAPS2 Phase-2 randomized trial, though not comparative, could be considered as having generated sufficient data on the drugs’ tolerability and efficacy to justify nivolumab single-therapy, or nivolumab plus ipilimumab doublet, in second- or third-line settings in MPM patient, PS 0–1. With this reasoning in mind, which appears particularly sound in an orphan disease like MPM, NCCN guidelines have actually integrated this second-line therapeutic option, without waiting for putative Phase-3 results.
In first-line setting, positive results of the anti-PD-1 and anti-CTLA-4 antibody combination in the CheckMate-743 Phase-3 trial supported the superiority of i.o. combination over standard pemetrexed-platinum-based doublet, yet with lower impact of PD-L1 tumor expression. However, the control arm of this trial could be a matter of debate, and the triplet bevacizumab-pemetrexed-cisplatin should certainly have been chosen as control arm in patients eligible for bevacizumab or, alternatively, the nivolumab plus ipilimumab combination. Whether PD-L1 expression remains important for patient selection remains debatable, and clearly of less importance in double i.o combination, as also observed in NSCLC. More complex immune signature should be further explored as suggested in CheckMate-743 trial to better select patients deriving the most important effect from immunotherapy combinations.
Thus, a future challenge would be to assess a 4-drug combination with bevacizumab, anti-PD-1/PDL1 antibody, pemetrexed, and platinum, as such a combination has recently been proven efficient in NSCLC patients, and given that there is a biological rationale supporting the synergy anti-VEGF therapy and immuno-therapeutics. The BEAT-meso Phase-3 trial, sponsored by ETOP, has actually chosen such a design. This study is designed to compare atezolizumab plus bevacizumab and standard chemotherapy versus bevacizumab and standard chemotherapy as first-line treatment for 320 advanced MPM patients. The trial’s results are awaited by 2024.
Further clinical trial results are also eagerly awaited (Table 6), such as those assessing frontline chemo-immunotherapy regimens, and future years will clearly see a major improvement in the care of MPM patients, after years of stagnation and therapeutic failures.
On-going immunotherapy-based trials in pleural mesothelioma with pending results.

EPP, extrapleural pleuro-pneumonectomy; IFN, interferon; OS, overall survival; VEGF, vascular endothelial growth factor.
Footnotes
Author contributions
Valerie Gounant and Gérard Zalcman conceived the review of Literature, draw the first draft. All authors revuewed the final version
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: GZ participated in advisory boards for Roche, Bristol-Myers-Squibb (BMS), Merck & Co, Boehringer Ingelheim, and Astra-Zeneca, and received reimbursements for attendance at 2016 and 2017 ASCO annual meetings from Roche;2018 ASCO annual meeting from Abbvie, 2017 ESMO annual meeting from Astra-Zeneca; 2016 WCLC meeting from BMS. He is the co-principal investigator of the MAPS2 trial with nivolumab and ipilimumab, sponsored by the French IntergReviewroup (IFCT), with the support of BMS. His research group received a research grant from Roche for funding a PhD student. VG received reimbursements for attendance at 2016 ASCO annual meeting from Roche. She is the co-principal investigator of the SAVIMMUNE Phase 2 trial with durvalumab, sponsored by the French Intergroup (IFCT), with the support of Astra-Zeneca. SB has no potential conflict of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.