
Abstract
Immunotherapy through checkpoint inhibitors is now standard practice for a growing number of cancer types, supported by overall improvement of clinical outcomes and better tolerance. One anti-CTLA-4 antibody (ipilimumab), two anti-PD-1 antibodies (pembrolizumab and nivolumab) and three anti-PD-L1 antibodies (atezolizumab, avelumab and durvalumab) have been approved for clear benefits across diverse trials. Adverse events of an immune nature associated with these agents frequently affect the skin, colon, endocrine glands, lungs and liver. Most of these effects are mild and can be managed through transient immunosuppression with corticosteroids, but high-grade events often require hospitalization and specialized treatment. However, since immunotherapy is recent, physicians with clinical experience in the diagnosis and management of immune toxicities are frequently those who actively participated in trials, but many practicing oncologists are still not familiarized with the assessment of these events. This review focuses on the incidence, diagnostic assessment and recommended management of the most relevant immune-related adverse events.
Keywords
Introduction
Cancer cells evade recognition and immune destruction through overexpression of diverse immunosuppressive molecules in the tumor microenvironment. 1 Some of these molecules, such as cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4), programmed cell death protein 1 (PD-1) and its ligand PD-L1 have been used as targets of novel immunotherapy agents. These so-called immune checkpoint inhibitors (ICIs) allow the immune system to reactivate cytotoxic T-lymphocytes and destroy tumor cells, exhibiting notorious clinical benefit for diverse cancer types, as multiple recent studies have shown, establishing immunotherapy as a major advance in cancer treatment. 2
However, altering the immune system may subsequently result in the development of various autoimmune manifestations of a particular clinical spectrum, referred to as immune-related adverse events (irAEs). Since these effects are believed to derive from global immunity enhancement, they can potentially affect any system in the body, but predominantly involve the skin, colon, lungs, endocrine glands and liver. 3 Organ specificity, incidence and severity of grade of irAEs vary according to each particular agent and its dose, but they also differ across tumor types. 4
Management of such adverse events often involves transient immunosuppression with corticosteroids and other drugs, and is of essential importance for successful and safe implementation of these drugs in routine practice. 5 This review focuses on the overall incidence, diagnostic assessment and recommended treatment for the most frequent and clinically significant irAEs of currently approved ICIs.
Current status of indications for cancer immunotherapy
The role of ICIs in the global treatment of cancer is continuously endorsed by substantial clinical impact, as shown in many recently published trials and contemporary use in routine oncology practice. To date, six ICIs have been approved by the United States Food and Drug Administration (US FDA) for the treatment of various tumors at diverse stages. 6 Most of the indications have been subsequently approved by the European Medicines Agency (EMA). 7 Of note, pembrolizumab was the first drug to obtain US FDA approval agnostic of cancer site or histology, but depending on a biomarker (microsatellite-instability-high or mismatch-repair-deficiency) in May 2017. 8 Table 1 summarizes the indications for which all different ICIs have been approved until January 2018 and their dates of approval by the US FDA and the EMA.
Indications and dates of approval of ICIs by US FDA and EMA updated to January 2018.
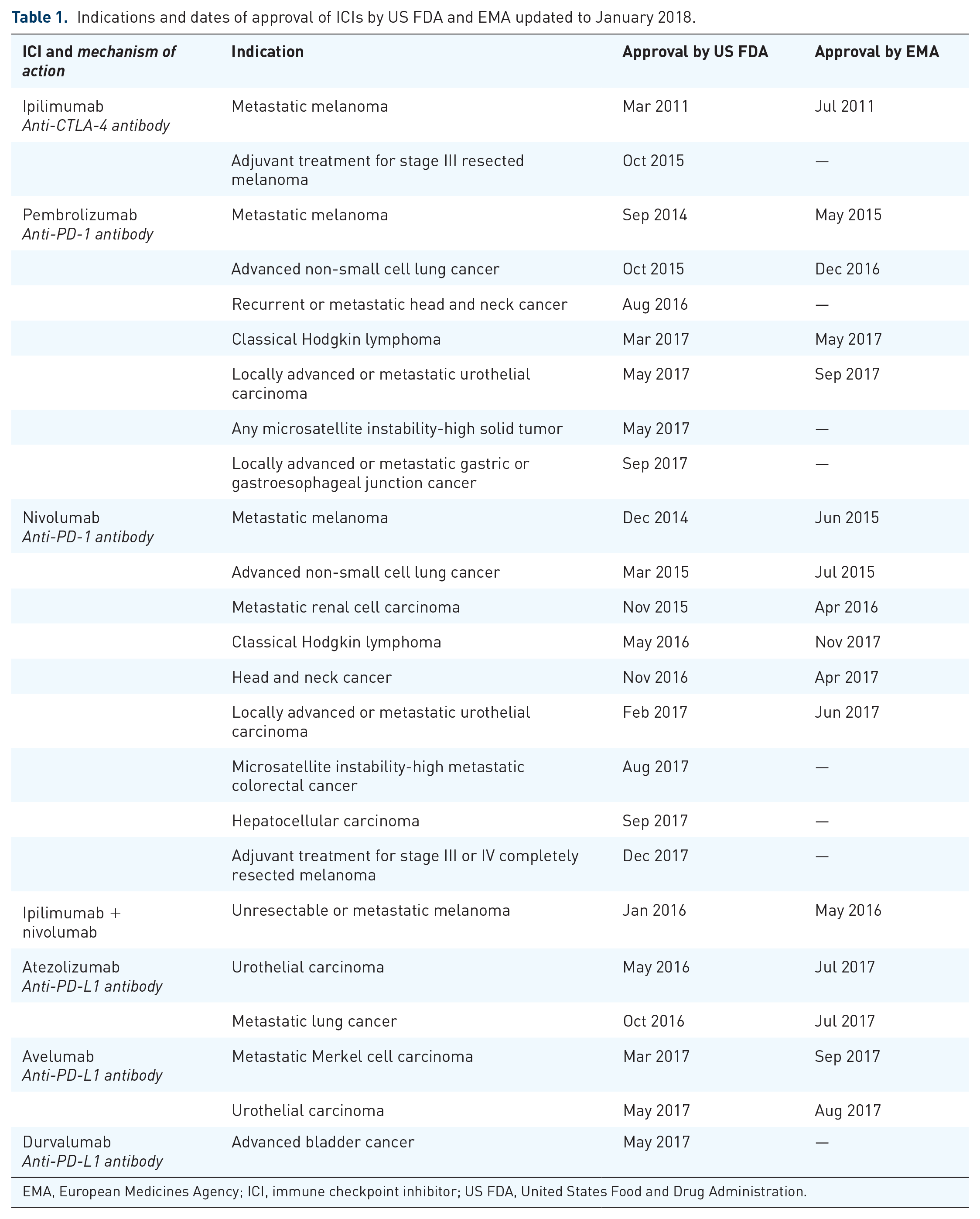
EMA, European Medicines Agency; ICI, immune checkpoint inhibitor; US FDA, United States Food and Drug Administration.
As data from clinical trials mature, more approvals and newer drugs are expected in years to come. This will considerably increase the number of patients exposed to these agents. Consequently, the need to understand and treat their associated events, in particular irAEs, becomes of upmost importance in daily clinical practice.
Incidence and chronological pattern of irAEs
IrAEs are very common for all ICIs and across different tumor types: events of any grade happen in about 90% of patients treated with anti-CTLA-4 ipilimumab and approximately 70% of those treated with any anti-PD-1 or anti-PD-L1 antibody.3,9
Since immune microenvironments vary substantially among tumors, the pattern of incidence, type and grade of irAEs is also diverse across trials for different cancers and stages treated with checkpoint inhibitors. 10
An overview of the frequency of organ-specific irAEs in melanoma, non-small cell lung cancer and urothelial carcinoma can be found from Davies and colleagues. 11 Severe irAEs, those of grade 3–4 that might require hospital admission, happen in 10–42% of patients treated with ipilimumab,12–15 and are fairly less frequent for anti-PD-1 (about 11–20%)11,16,17 or anti-PD-L1 agents (1–9%).18–23 A meta-analysis of 46 studies that represented 12,808 cancer patients treated with nivolumab, pembrolizumab, atezolizumab, durvalumab and avelumab reported global incidence of any grade irAEs of 26.8% and of severe grade of 6.1%; with lower incidence of severe irAEs for pembrolizumab (5.1%) and atezolizumab (5.3%) than for nivolumab (8.2%). 24
For combined ICI treatment, the rates of grades 3–4 irAEs are significantly higher: the CheckMate-067 trial reported 59% of grade 3–4 adverse events for the combination of ipilimumab 3 mg/kg plus nivolumab 1 mg/kg every 3 weeks for four doses followed by nivolumab 3 mg/kg every 2 weeks for untreated melanoma. 25 On the same lines, for patients with progressive small-cell lung cancer, the CheckMate-032 accounted 19% of serious irAEs in the ipilimumab 1 mg/kg plus nivolumab 3 mg/kg every 3 weeks for four doses cohort and 30% in the ipilimumab 3 mg/kg plus nivolumab 1 mg/kg every 3 weeks for four doses cohort (both cohorts were followed by nivolumab 3 mg/kg every 2 weeks). 26
Severity of irAEs also shows a trend according to the organ or body system affected: most grade 1–2 events present in the skin and gastrointestinal tract, while grade 3–4 events are usually restricted to the colon and endocrine glands. 3
The occurrence of irAEs from ICIs typically follows a chronological pattern according to the drug used. Most of the toxicities associated with ipilimumab start within the first 8–12 weeks from beginning treatment, with dermatologic toxicity onset at 2–3 weeks, followed by gastrointestinal and liver toxicity after 6–7 weeks, while endocrine gland affection usually appears later at around 9 weeks.27,28 Most irAEs from ipilimumab happen within the induction period, in the first 3 months of treatment.5,29
The timeline of occurrence of irAEs from anti-PD-1 antibodies is less well established, but it shows a trend to present slightly later than anti-CTLA-4 toxicity. In a pooled analysis of patients treated with nivolumab, the onset of dermatologic irAEs was at about 5 weeks, gastrointestinal at 7 weeks, hepatic at 8 weeks, pulmonary at 9 weeks, endocrine at 10 weeks and renal toxicity at 15 weeks.17,30 However, incidence of anti-PD1 irAEs does not show a consistent timeline across multiple trials and is not clear at the moment. Pembrolizumab has a median onset of grade 3–4 irAEs at about 9 weeks. 31
Since anti-PD-L1 are the newest agents with immune mechanism of action, their irAEs and pattern of onset are less clear, but seem to be milder and less frequent than for anti-CTLA-4 or anti-PD-1 antibodies.18–24
Of note, due to the fact that responses can occur late after withdrawing treatment, late-onset irAEs may also happen several weeks or even months after completing or suspending ICI therapy, which demands for watchful follow up of these patients.32,33
Dose-dependence relationship
According to several trials, ipilimumab exhibits a clear dose-dependent relationship with regards to incidence and severity of irAEs. All-grade events varied from 61% at a dose of 3 mg/kg to 79% when administered at 10 mg/kg. 34 The incidence of serious irAEs from ipilimumab doubles when used at a dose of 10 mg/kg (38%) versus 3 mg/kg (18%). 15 On the other hand, the incidence of irAEs for anti-PD-1/PD-L1 agents does not seem to be dose related.4,35,36 According to an exposure-response analysis of efficacy and safety, nivolumab exposure (dose rank 1 to 10 mg/kg) is not associated with overall survival or higher risk of adverse events in patients with non-small cell lung cancer. 37 A meta-analysis that included 6350 cancer patients from 16 phase II/III clinical trials of PD-1 inhibitors did not find significant differences in the incidences of pneumonitis between high-dose and low-dose groups of PD-1 inhibitors, concluding the risk was dose independent. 38
Biomarkers of irAEs
Attempting to identify patients more likely to develop irAEs has also been an objective of clinical trials, thus leading to the approval of various ICIs. Gene expression profiling, circulating autoantibodies and interleukin-17 levels, among other assays, have been tested as potential predictive biomarkers for the development of irAEs, but their sensitivity was low.39,40 Intestinal microbiome analysis was shown to help identify melanoma patients at higher or lower risk for ipilimumab associated colitis: Those with microbiomes enriched with members of the Bacteroidetes phylum were less prone to develop colitis. 41 To date, there are no available predictive biomarkers for immune toxicity from immune checkpoint blockade.
System and organ-specific irAEs
Global incidence and general recommendations for diagnosis and treatment for the most frequent and clinically relevant irAEs are described in the following section. 42
Dermatologic toxicity
Rash and pruritus rank among the most frequent irAEs for any ICI, occurring in about 50% of patients treated with ipilimumab, 40% of patients with anti-PD1 treatment33,43 and 1–7% for anti-PD-L1 agents.18–23 Other common dermatologic effects afflicting patients undergoing immunotherapy include vitiligo (almost exclusively in melanoma patients, and particularly associated with survival benefit), 44 photosensitivity reactions and xerosis cutis. Lichenoid dermatitis and psoriasis have been reported as a characteristic dermatologic irAE in melanoma patients treated with anti-PD-1/PD-L1 antibodies. 45 Alopecia areata and universalis can be a rare effect of ICIs, including anti-PD-L1 agents. 46 Rare cases of Stevens–Johnson syndrome and toxic epidermal necrolysis have been reported. 47 As an interesting effect, as opposed to the vitiligo reactions seen with melanoma treatment, hair re-pigmentation can occur during anti-PD-1/PD-L1 treatment, as reported in a series of 14 patients. 48
Skin irAEs are typically low grade and in general improve with symptomatic treatment that includes topical corticosteroids and oral antihistamines. 49 Discontinuing the ICI is rarely necessary for these events, but can be considered in case of persistence or severity of the lesions. 42
Gastrointestinal toxicity
Incidence of gastrointestinal (GI) irAEs is more frequent for anti-CTLA-4 ipilimumab than for the other types of checkpoint inhibitors.
When assessing GI events, diarrhea should be ideally distinguished from colitis: diarrhea only implies an increase in the frequency of stools, while colitis might include abdominal pain, vomiting, fever, hematochezia and/or endoscopic evidence of colon inflammation. In common clinical grounds, however, they often are parts of the same spectrum of disease.
In pivotal trials using ipilimumab at a 3 mg/kg dose, any grade diarrhea presented in 23–35% of patients, while it happened in about 41% of those treated at a 10 mg/kg.
Colitis was less frequent, reported in about 8–22% of ipilimumab treated patients, but it is considered its most severe toxicity, and the main cause for discontinuation of treatment. 50
When combined treatment of ipilimumab plus nivolumab was assayed, the frequency of GI irAEs was highest: 45% of patients presented diarrhea and colitis. 51
The incidence of diarrhea or colitis for anti-PD1/anti-PD-L1 agents is considerably lower: 8–9% for nivolumab, 7–16% for pembrolizumab, 2–15% for atezolizumab, 1–9% for avelumab and 2% for durvalumab.18–23 However, anti-CTLA-4 and anti-PD-1-induced colitis develops through different immunopathological mechanisms, as assessed by tumor necrosis factor (TNF)-a’ concentrations in biopsy specimens. 52
Warning the patient about initial assessment of diarrhea/colitis is crucial when starting ICI treatment, since early management might prevent progression to more severe toxicity. Maintaining oral hydration is a first step, but if diarrhea persists or worsens in the first 3 days despite symptomatic treatment, oral or intravenous corticosteroids might be required once concomitant infection with Clostridium difficile has been ruled out. Colonoscopy or sigmoidoscopy is indicated for persistent grade 2 or higher diarrhea to confirm colitis. High mucosal TNF-a’ concentrations in biopsy supernatants can predict steroid resistance after CTLA-4 blockade. 52 For severe (grade 3–4) GI toxicity, hospitalization is required and infliximab 53 or other immunosuppressive agents might be used if no improvement is seen with intravenous corticosteroids. Permanent discontinuation of the immune checkpoint inhibitor is suggested in these cases. 42
Endocrine toxicity
Damage to the thyroid, hypophysis or adrenal glands occurs in about 5–10% of patients who receive any ICI for cancer treatment,54,55 but their symptoms are often nonspecific and can be difficult to diagnose. The most frequent endocrinopathies reported are hypophysitis (1.8% of patients treated with ipilimumab, 0.5% of those treated with pembrolizumab) and hypothyroidism (2% in patients treated with ipilimumab and 8% of those treated with anti-PD-1 agents). 42 Very few cases of hyperthyroidism have been reported in relationship to immune checkpoint blockade, although it might often precede hypothyroidism.
Symptoms such as fatigue, headaches and visual field changes are suggestive of hypophysitis. Although the pathogenic mechanism for hypophysitis from ipilimumab is unknown, it has been demonstrated that pituitary cells express CTLA-4, being able to trigger an inflammatory response.56,57 Diagnosis can be confirmed through measurement of pituitary hormones [adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH), follicle-stimulating hormone, luteinizing hormone, growth hormone and prolactin] and aided by imaging such as magnetic resonance imaging. High ACTH would suggest adrenal insufficiency and high TSH plus low free T4 (FT4) would be indicative of hypothyroidism. It is common practice to monitor thyroid function monthly or every two cycles while on treatment with ICIs.
Given the insidious nature of these autoimmune events, their consequences tend to be persistent, or even permanent and require prolonged hormone replacement therapy, but the ICI may be continued. 42
Hepatotoxicity
Hepatic function is routinely monitored before every cycle of ICI treatment. Thereby, hepatotoxicity as an irAE usually presents as asymptomatic increase of alanine aminotransferase (ALT), aspartate aminotransferase (AST) or total bilirubin, and occurs in 5–10% of patients under treatment with ICIs in monotherapy and as many as 25–30% of those in combined treatment of ipilimumab plus nivolumab.47,58 When assessing hepatotoxicity, noninflammatory etiologies (progressive disease, viral hepatitis, other concomitant medications) must be ruled out first through imaging and other ancillary studies. 59
The grade of toxicity guides management. For grade 2 events the ICI should be withheld and transaminases and bilirubin measured twice weekly. If liver function tests (LFTs) remain elevated after 1–2 weeks and other causes have been ruled out, then oral corticosteroids should be started, re-starting the ICI once LFTs have improved and steroid has been tapered. For more severe or persistent reactions, the ICI should be permanently discontinued and higher doses of steroids or other immunosuppressive drugs such as mycophenolate might be necessary, as well as consultation with a Hepatologist, further imaging or even liver biopsy. Immune-mediated hepatitis often resolves in 4–6 weeks. 42
Pulmonary toxicity
Highly variable in onset and severity, immune-related pneumonitis is uncommon, although a potentially severe or even fatal complication. It is rare for ipilimumab in monotherapy (<1%),60,61 more frequent for anti-PD-1/anti-PD-L1 treatment (1–2% for melanoma patients, 3–6% for lung cancer patients),18–23,36,62–64 and presents in up to 10% of patients with combined ICI treatment.14,58 Its reported range of clinical presentation varies from 9 days to 19 months, usually as a dry cough, progressive dyspnea and fine inspiratory crackles. 61 Once cardiac failure is ruled out, a computed tomography scan often confirms diagnosis and systemic steroid treatment must promptly ensue in a hospital setting. If symptoms do not improve, infectious causes (such as Pneumocystis jirovecii, mycoplasma) must be ruled out through bronchoscopy, ideally before increasing corticosteroid dose. For grade 2 events, withholding ICI treatment is recommended until the steroid has been tapered, usually over 6 weeks; but in grade 3–4 pneumonitis, immune checkpoint blockade is permanently suspended. 42
Interstitial lung disease (ILD) has also been identified in up to 3.5% of patients treated with ICIs; typically males and former smokers, occurring early and with suggestive radiological characteristics. Most patients have low grade ILD and require only corticosteroids and antibiotics, but definitive suspension of ICIs can be necessary in up to 75% of them. 65
Less common irAEs
Although less frequent, other irAEs must be taken into account when treating patients with ICIs.
Nephrotoxicity
Immune-mediated acute kidney injury happens in less than 1% of patients treated with ICIs, although it borders 5% of incidence for combined or sequential ICI therapy. 66 It is often detected as asymptomatic elevation of creatinine through routine laboratory testing before a cycle of treatment. Initial management or immune-related nephritis includes stopping any concomitant nephrotoxic drugs and evaluating other possible prerenal, intrarenal or postrenal etiologies for acute renal failure.
Corticosteroid treatment and withholding immunotherapy is recommended until complete resolution of the event. Nephrology consultation and renal biopsy might be necessary for higher grade events.42,67
Neurological toxicity
Although rare (about 1% of all patients treated with ICIs), a wide range of neurologic syndromes have been described in association with immune checkpoint blockade: polyneuropathy, facial paralysis, optic neuritis, Guillian–Barre syndrome (GBS), myasthenia gravis, transverse myelitis, encephalitis and aseptic meningitis.68–70 Neurology consultation is ensued and image studies to rule out progression are necessary. Steroid treatment often alleviates minor symptoms, but higher doses or other procedures (e.g. intravenous immunoglobulin for GBS) might be required for more severe toxicity. 42
Cardiotoxicity
A variety of cardiac manifestations such as heart failure, cardiomyopathy, heart block, myocardial fibrosis and myocarditis can subside treatment with ICIs. 71 Myocarditis is very rare, documented in 0.27% of patients treated with ipilimumab plus nivolumab versus 0.06% for nivolumab alone. Other cardiac issues related to ICI treatment include pericarditis, cardiomyopathy, arrhythmias and heart failure.72,73 In these cases, consultation with cardiologists is guaranteed and treatment with steroids is critical. 71
Pancreatic toxicity
Although routine monitoring of amylase and lipase is not recommended for ICI treatment, asymptomatic mild elevations of these enzymes should not be treated. However, isolated reports of immune-mediated pancreatitis are described and should be treated as such. 74
Ocular toxicity
Extremely rare irAEs from ICIs, although of particular importance 75 include keratitis, uveitis, conjunctivitis and episcleritis. Most of these are successfully treated with topical or systemic corticoids. 42
Musculoskeletal and rheumatologic toxicity
Mild or moderate myalgias are frequently described in association to ICIs (2–12%), 28 but rare syndromes such as vasculitis, inflammatory arthritis and inflammatory myositis have been reported. 76 In most cases symptomatic or low-dose steroids are effective for these events. 42
Impact of immune-mediated toxicity and its treatment in response
Although it was initially hypothesized that the use of corticoids would alter the established immune enhancement from ICIs, and through such affect tumor response, preliminary data appear to demonstrate that systemic immunosuppression does not have a negative impact on efficacy.77,78 Among patients who had at least grade 2 irAEs following treatment with ipilimumab, a nonstatistically significant trend of higher disease control rate was described in a series of cases and then reported in a pooled analysis of phase II studies.78,79 Another pooled analysis of 576 patients treated with nivolumab found no difference between objective response rate of those who required immunosuppressive treatment and those who did not (30% versus 32%). 80 A retrospective analysis of patients treated with nivolumab even showed improved overall survival in patients with grade 3 or higher irAEs, 81 while a prospective cohort study of 43 patients with advanced non-small cell lung cancer treated with nivolumab demonstrated a higher objective response rate in patients with irAEs (37%) than those without irAEs (17%), as well as longer median progression-free survival (6.4 months versus 1.5 months). 82
Another prospective study of 58 patients with non-small cell lung cancer treated with PD-1 blockade concluded that thyroid dysfunction was an independent predictive factor for a favorable outcome, since overall survival and progression-free survival were significantly improved in the thyroid disfunction group. 83
Even patients treated with infliximab for severe ipilimumab-derived colitis did not exhibit worse survival than those only treated with steroids in a retrospective study, arguing in favor of early administration of infliximab to reduce steroid toxicity. 84
As a cause–effect relationship between irAEs and efficacy outcomes (response rate, overall survival) has not been consistently demonstrated in prospective studies, it is reasonable to consider that the incidence and treatment of irAEs does not seem to alter the disease-dependent prognosis of patients treated with ICIs.
Safety of re-challenging the immune system after an irAE
Although retreatment with ipilimumab seems to be well tolerated according to a trial, 85 the use of a different ICI when immune toxicity has occurred with a first one remains a controversy in the clinical practice of oncology. Limited available data come from retrospective studies. A trial demonstrated higher frequency of high-grade irAEs, particularly pneumonitis (7%), in a small group of patients with advanced melanoma treated with ipilimumab after first-line nivolumab or pembrolizumab. 86 Another trial, however, demonstrated safety of pembrolizumab in ipilimumab-refractory melanoma patients. 87 A recent retrospective study on advanced melanoma patients suggested anti-PD-1 treatment frequently induced mild immune toxicities but these were easily managed and a significant proportion of patients achieved clinical responses. 88 In the retrospective analysis of 64 patients that developed ILD after immunotherapy, 7 out of 10 patients re-challenged with ICIs did not develop irAEs. 65
From these diverse experiences it can be inferred that toxicity might be treatment-specific rather than attributable to immune checkpoint blockade as a single entity. 89
Many immunotherapy trials have excluded patients who had been previously exposed to ICIs. True contraindications to re-exposing the patient to immunotherapy after an irAE have not been established, but clinical common sense should prevail, considering long half-lives of most antibodies. Support of any decision by a multidisciplinary committee is always encouraged.
Conclusion
Considering significant outcome benefit and overall better tolerance, immunotherapy with ICIs has shifted the paradigm of treatment on diverse cancer types. These novel therapies entail a wide spectrum of immune-related adverse events, commonly affecting the skin, colon, liver, endocrine glands or lungs. Most of these effects are reversible and manageable with transient corticosteroid treatment, but some of them can be potentially fatal and require special attention. Education of patients, nurses and other collaborative staff is mandatory when considering these drugs for the treatment of cancer.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.