
Abstract
Background:
We aim to assess the prognostic ability of three common lymph node–based staging algorithms, namely, the number of positive lymph nodes (pN), the lymph node ratio (LNR), and log odds of positive lymph nodes (LODDS) in patients with esophageal squamous cell carcinoma (ESCC).
Methods:
A total of 3902 ESCC patients treated at 10 Chinese institutions between 2003 and 2013 were included, along with 2465 patients from the Surveillance, Epidemiology, and End Results (SEER) database. The prognostic ability of the aforementioned algorithms was evaluated using time-dependent receiver operating characteristic (tdROC) curves, R2, Harrell’s concordance index (C-index), and the likelihood ratio chi-square score. The primary outcomes included cancer-specific survival (CSS), overall survival (OS), and CSS with a competing risk of death by non-ESCC causes.
Results:
LODDS had better prognostic performance than pN or LNR in both continuous and stratified patterns. In the multicenter cohort, the multivariate analysis showed that the model based on LODDS classification was superior to the others in predictive accuracy and discriminatory capacity. Two nomograms integrating LODDS classification and other clinicopathological risk factors associated with OS as well as cancer-specific mortality were constructed and validated in the SEER database. Finally, a novel TNLODDS classification which incorporates the LODDS classification was built and categorized patients in to three new stages.
Conclusion:
Among the three lymph node–based staging algorithms, LODDS demonstrated the highest discriminative capacity and prognostic accuracy for ESCC patients. The nomograms and novel TNLODDS classification based on LODDS classification could serve as precise evaluation tools to assist clinicians in estimating the survival time of individual patients and improving clinical outcomes postoperatively in the future.
Background
Esophageal cancer (EC) is the sixth most common cause of cancer-related deaths in the world, and the prognosis of this clinical entity is dismal. 1 At the histological level, EC is subdivided into esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma. ESCC is more common in Asia, while esophageal adenocarcinoma is prevalent in Western countries.2,3 After recognizing the differences in genomic alterations and survival outcomes between the two entities, the newest tumor–node–metastasis (TNM) staging system proposed by the American Joint Committee on Cancer (AJCC) introduced a separate stage grouping system for ESCC and esophageal adenocarcinoma. 4 Currently, although combined-modality therapy with curative intent has been recommended for ESCC patients, the 5-year survival outcome remains at 30–40% for patients with local disease. 5 The presence of regional lymph node (LN) metastases is occurs in at least 40% of ESCC patients at initial treatment and is an important prognostic factor.6,7
To avoid stage migration, it is important to examine a sufficient number of LNs and evaluate their malignant involvement. However, the largest data analysis evaluating esophagectomy patients found that nearly 40% of patients did not receive adequate LN examinations. 7 Given these circumstances, novel measures of LN status that can be integrated with the number of retrieved LNs are warranted. In addition to the traditional positive LN (pN)-stage classification, two other algorithms, namely, the lymph node ratio (LNR) and the log odds of positive lymph nodes (LODDS) have been developed. LNR, which is defined as the ratio of pN to the total number of LNs examined (TLN), has been suggested to have greater prognostic value than pN stage for EC patients. 8 LODDS is calculated as the log of the ratio of pN to the number of negative LNs. The effectiveness of the LODDS in predicting the survival outcomes of patients with several malignancies has been demonstrated.9 –11 However, the prognostic effectiveness of LODDS in ESCC patients is still unclear and has not been evaluated in a large, real-world data set. Moreover, the most feasible staging algorithm for predicting the prognosis of ESCC remains undetermined. 12
The primary aim of this study was to compare the prognostic ability of the three aforementioned LN algorithms for ESCC patients who underwent surgical resection using data from a Chinese multicenter cohort. We then validated our findings externally in the Surveillance, Epidemiology, and End Results (SEER) data set. Our secondary aim was to build the optimal LN algorithm-based nomograms, in which we further combined the T-stage with the optimal LN classification to propose a novel staging system for predicting survival in ESCC patients.
Methods
Patients
A multi-institutional Chinese cohort consisting of 3902 ESCC patients who received treatment between January 2003 and December 2013 at 10 institutions in People’s Republic of China (The Second Affiliated Hospital of Soochow University, Suzhou; The First Affiliated Hospital of Soochow University, Suzhou; Zhongda Hospital Southeast University, Nanjing; Fudan University Shanghai Cancer Center, Shanghai; Shanghai Chest Hospital of Shanghai Jiaotong University School of Medicine, Shanghai; Shanghai Pulmonary Hospital, Shanghai; Suzhou Kowloon Hospital of Shanghai Jiaotong University School of Medicine, Suzhou; Taicang Affiliated Hospital of Soochow University, the First People’s Hospital of Taicang, Taicang; Zhangjiagang Hospital Affiliated to Suzhou University, Zhangjiagang First People ‘s Hospital, Zhangjiagang; and the Affiliated Hai’an Hospital of Nantong University, Hai’an) was established. Prior to surgery, all patients received computed tomography (CT) of the chest and abdomen and EUS (endoscopic ultrasound) as part of their routine staging workup. Patients received whole body fluorodeoxyglucose-positron emission tomography (FDG-PET) to eliminate the possibility of distant metastases if the attending physician considered it was necessary. All patients received a surgical R0 resection, and those who received an R1 or R2 resection were excluded. Notably, there has been nothing approaching a consensus on the extent of LN dissection for ESCC patients. As previous studies focused on the LN schemes,6,13,14 patients who received neoadjuvant therapy were excluded due to the influence of neoadjuvant therapy on LN status and pathologic T-stage. All resected tumors and LNs were carefully reviewed by pathologists specializing in gastrointestinal histology. Eligible ESCC patients were then restaged according to the 8th edition of the AJCC TNM staging system. Data regarding age, gender, tumor location, histological grade, type of resection, T-stage, N-stage, total number of retrieved LNs, number of positive LNs, status of vascular invasion, and perineural involvement were extracted. The primary endpoints were overall survival (OS), which was defined as the time between date of surgery and death from any cause, and cancer-specific survival (CSS), defined as the time from date of surgery to death caused by ESCC. CSS with a competing risk of death from non-CSS causes was defined as the secondary endpoint. After receiving esophagectomy, patients were followed up by clinical examination every 3 months for the first year, every 3–6 months for the second year, and every 6–12 months from then on. A cutoff date of December 30, 2018, was selected to ensure a 5-year postoperative follow-up time. ESCC patients with a survival time shorter than 3 months were excluded to rule out a contribution of postoperative complications to mortality.
In order to validate the findings derived from the multicenter cohort, an independent cohort composed of 2465 ESCC patients was obtained from the SEER database using the software SEER*Stat, version 3.5. 15 The eligibility criteria including (1) primary tumor located in the esophagus and diagnosed between 1988 and 2013; (2) age older than 18 years; (3) primary tumor surgery and no neoadjuvant radiotherapy; (4) histologically confirmed ESCC (see Supplementary Information); (5) at least one LN examined; (6) survival time of at least 3 months. All patients were required to have sufficient information for restaging according to the 8th edition of the TNM staging system.
Definitions of LN-based staging algorithms
All eligible ESCC patients were classified according to their AJCC 8th edition N stages (8th pN stages), LNR stages and LODDS stages. According to the 8th edition of AJCC TNM staging, pN0 was defined as no regional LN metastasis, pN1 was defined as metastasis in one to two regional LNs, pN2 was defined as metastasis in three to six regional LNs and pN3 was defined as metastasis in seven or more regional LNs. LNR was defined as the ratio of the number of positive LNs (pLN) to the total number of LNs examined (TLN). Using recursive partitioning analysis,16,17 LNR was divided into four categories: LNR0 (LNR = 0), LNR1 (0 < LNR ⩽ 0.11), LNR2 (0.11 < LNR ⩽ 0.19), and LNR3 (0.19 < LNR ⩽ 1). LODDS was calculated as
Proposal of novel TNLODDS classification
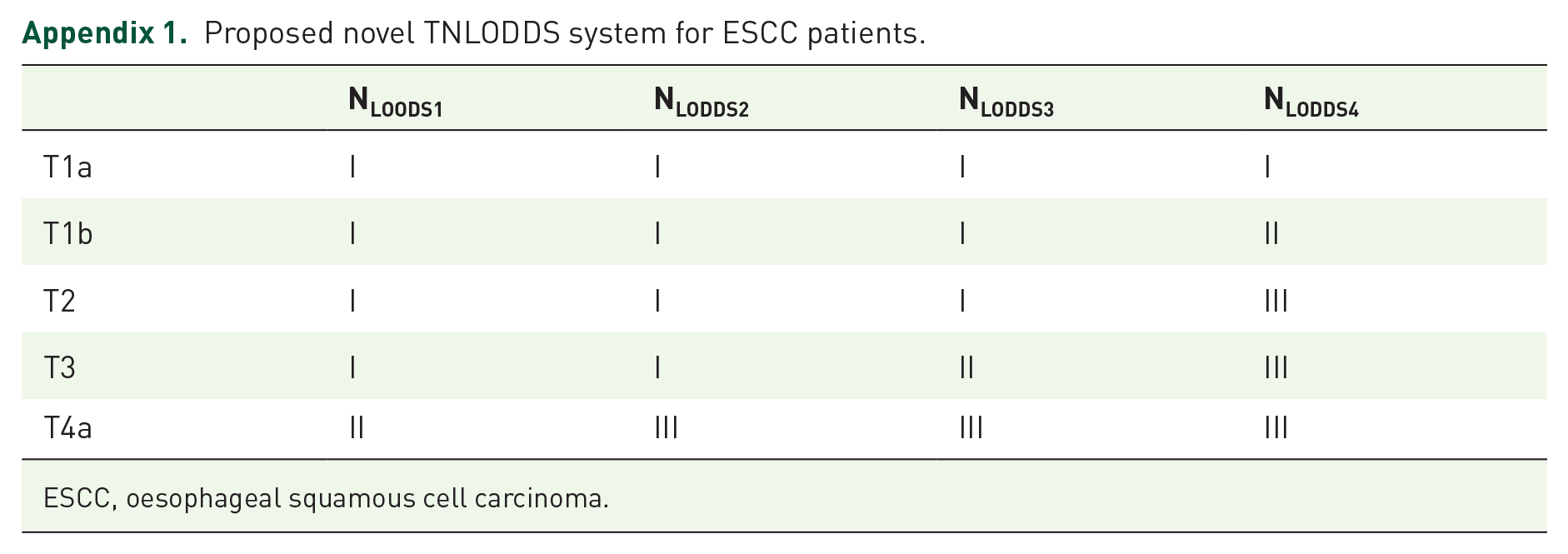
According to the depth of tumor invasion/LN status by combing 5 T categories (1a/1b/2/3/4a) and 4 NLODDS categories (1/2/3/4), ESCC patients were initially divided into 20 groups, from T1aNLODDS1, T1aNLODDS2 ... to T4aNLODDS4. By combining with T and NLODDS after adjusting for significant clinicopathological factors in the multivariable Cox analysis, adjusted HRs (AHRs) were calculated and integrated into three groups using the k-means clustering analysis.
Statistical analysis
Spearman coefficients were used to evaluate the correlation of three LN algorithms. The log-rank test and Kaplan–Meier survival curves were employed to compare OS and CSS between different subgroups. For the competing-risk model, death from ESCC and death from other causes were two competing events. The cumulative incidence function (CIF) was used to describe the probability of death. 18 To evaluate the relationship between three LN staging algorithms and ESCC survival, the univariate Cox regression model with a restricted cubic spline function was used. We investigated the prognostic performance of the LN staging algorithms using time-dependent receiver operating characteristic (tdROC) curve analyses. For OS analysis, multivariable Cox regression analyses were applied to assess the prognostic ability of the LN staging algorithms as well as other prognostic factors. For the competing-risk model analysis, the proportional subdistribution hazards regression method was used. To assess the performance of the OS model, we calculated R2, Harrell’s concordance index (C-index), and the likelihood ratio chi-square score. A higher R2 indicated a better prognostic model; 19 a higher likelihood ratio chi-square score indicated better homogeneity; a high C-index indicated better discriminatory ability. 20 The prognostic variables identified by the multivariate analyses were used to develop nomograms to predict OS and cancer-specific mortality. 21 A calibration plot described the fitting degree between the actual survival and the nomogram predicting survival. The clinical utility of the nomograms was assessed by decision curve analysis (DCA). A two-sided p value < 0.05 was considered statistically significant. Statistical analyses were conducted with R software version 3.5.2 (Institute for Statistics and Mathematics, Vienna, Austria; https://www.r-project.org/).
Results
Clinicopathological characteristics
As shown in Table 1, this study included a total of 3902 ESCC patients from the Chinese multicenter cohort as well as another 2465 patients from the SEER database. ESCC patients tended to be male, to have tumor located in the middle third of the esophagus and to be diagnosed with high histological grades. In the multicenter cohort, a median of 23 TLN was identified, while the number was 10 TLN in the SEER database. More than half of ESCC patients were in pN0 stage (multicenter cohort vs SEER data set: 56.8% and 57.1%).
Clinicopathological characteristics of patients with esophageal squamous cell carcinoma in the multicenter cohort and SEER database.

CHSDA, Contract Health Service Delivery Areas; IQR, interquartile range; LN, lymph node; LNR, lymph node ratio; LODDS, log odds of positive lymph nodes; NR, not recorded; PORT, postoperative radiotherapy; SD, standard deviation; SEER, Surveillance, Epidemiology, and End Results.
Characteristics of three LN staging algorithms
Supplementary Figure S1 demonstrates the relationships between LNR and LODDS, between pN and LODDS and between pN and LNR. The Spearman rank test showed a stronger correlation between LNR and LODDS than between LODDS and pN (r: 0.876 vs 0.768). The restricted cubic spline analyses suggested the risk of mortality increased as scores from the three LN staging algorithms rose, and the associations were nonlinear (Supplementary Figure S2A–C). Interestingly, for ESCC patients with pN0 stage, the mortality risk also increased as LODDS increased (Supplementary Figure S2D).
Prognostic abilities of three LN staging algorithms
According to the results of the tdROC analyses, LODDS showed better discriminatory capacity than pN or LNR, not only for OS but also for CSS (see Supplementary Figure S3A–F and Supplementary Table S1). When we compared the AUC (area under curve) values of the three LN staging algorithms in the competing-risk model considering a competing risk of death due to non-ESCC cause, LODDS had higher 1-, 3- and 5-year AUCs than either of the other algorithms (5-year AUC: LODDS vs pN vs LNR, 69.92%, 67.39%, and 63.43%, respectively) (Supplementary Figure S3G-I and Supplementary Table S1). Kaplan–Meier analyses showed that patients stratified by LODDS (p < 0.001), LNR classifications (p < 0.001), and pN classification (p < 0.001) could discriminate OS rates effectively (Supplementary Figure S4A–C and Supplementary Table S2). Similar results were noted when CSS was used as the outcome (Supplementary Figure S4D–F and Supplementary Table S2). Moreover, the CIF for cancer-specific mortality suggested that patients with advanced LNR and LODDS stages had an increased risk of death (Figure 1).
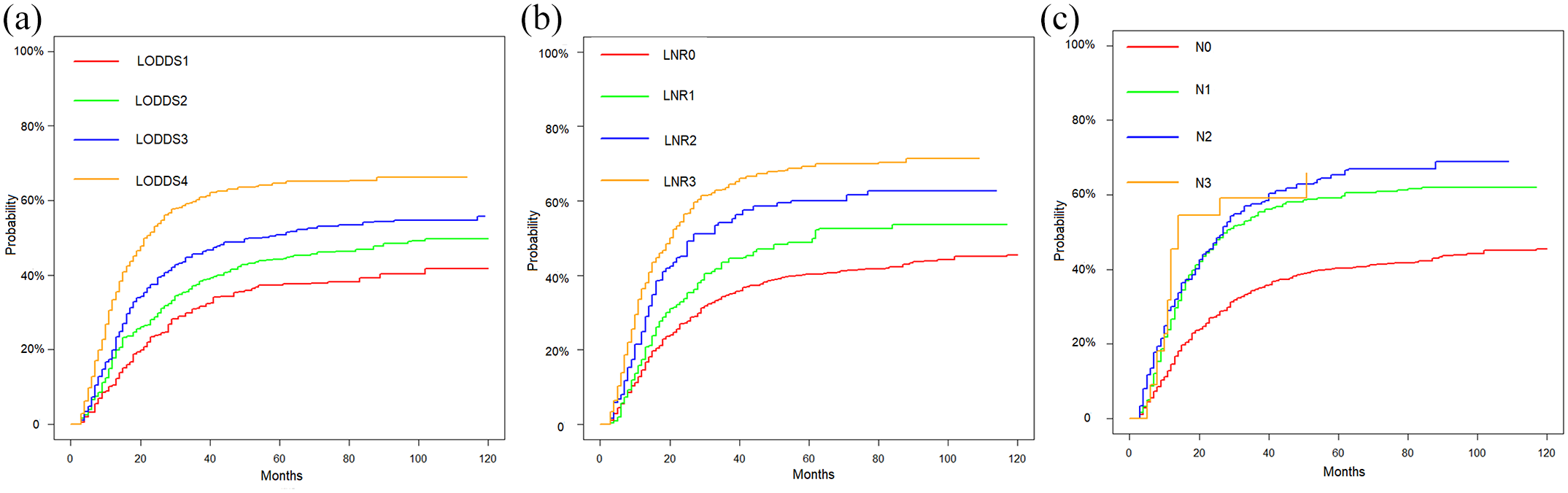
Cumulative probability of death owing to ESCC according to LODDS classification (a), LNR classification (b), and 8th pN classification (c) in the multicenter cohort, respectively.
In the SEER database, stratification by LODDS classification showed good discriminatory ability in predicting OS (Supplementary Figure S5A–C), and the results were similar for CSS (Supplementary Figure S5D–F) and cumulative ESCC death probability (Supplementary Figure S6). The 5-year OS and CSS rates for ESCC patients in the SEER database when stratified by the three LN staging schemes are displayed in Supplementary Table S2.
Selecting potential variables
In the multivariate analysis of OS in the multicenter cohort, after adjustment for clinicopathological variables including age, gender, tumor location, histological grade and T stage, we identified LODDS, LNR, and pN classification as independent factors (Table 2). Next, we performed the likelihood ratio test and calculated the C-index and R2 of three LN classifications. The results suggested that among three classifications, the LODDS classification had the greatest R2 (0.136), likelihood ratio (569.8), and C-index (0.636, 95% CI: 0.624–0.648). Thus, we found that the LODDS classification offered the most accurate prognostic stratification (as measured by R2 and by the C-index) and the best homogeneity (as measured by the likelihood ratio test). The results of multivariate analysis for the competing risk model are provided in Table 2, which also shows that the LODDS, LNR, and pN classifications were significantly associated with cancer-specific mortality in patients with ESCC. Relative to those with lower stages, patients with higher stages had a substantially increased risk of cancer-specific mortality (Table 2). The discrimination performance of the three cancer-specific mortality models also suggested that the LODDS classification-based model (C-index: 0.622, 95% CI: 0.569–0.680) had the best discriminatory ability.
Multivariable Cox model with different node classification of prognosis for overall survival and proportional subdistribution hazard models with different node classification of probabilities of death resulting from esophageal squamous cell carcinoma in the multicenter cohort.

CI, confidence interval; C-index, Harrell’s concordance index; HR, hazard ratio; LNR, lymph node ratio; LODDS, log odds ratio; pN, pathological positive lymph node; sHR, subdistribution hazard ratios.
Represent the LODDS classifications, LNR classifications, and 8th pN for corresponding multivariable models.
Development and validation of the prognostic nomograms
Since the LODDS classification outperformed the other two classifications for both OS and cumulative ESCC death probability, we constructed two nomograms integrating the LODDS classification and other clinicopathological risk factors associated with OS as well as cancer-specific mortality (Figure 2). The calibration curves also showed good consistency in between the observed and nomogram-predicted 1-, 3-, and 5-year OS in both the multicenter cohort (Figure 3(a)–(c)) and the SEER database (Supplementary Figure S7A–C). In addition, the DCA demonstrated that the nomogram had great positive net benefits across almost all of the threshold probabilities at different time points, indicating the favorable potential clinical effect of the nomogram (Figure 3(d)–(f), Supplementary Figure S7D–F). In the nomogram for predicting cancer-specific mortality, calibration plots also showed good concordance between predicted and actual outcomes in the two cohorts (Supplementary Figure S8A–C and Supplementary Figure S9A–C). In the multicenter cohort, the results of the DCA revealed the great potential for clinical application of the nomogram, as the nomogram ensured greater net benefits than the treat-all or the treat-none option throughout the range of threshold probabilities for 1-, 3- and 5-year cancer-specific mortality (Supplementary Figure S8D–F). Similar results were obtained in the SEER cohort (Supplementary Figure S9D–F).

Nomograms for predicting overall survival (a) and cancer-specific mortality (b) for ESCC postoperatively.

(a–c) Calibration curves showing the probability of 1-, 3-, and 5-year OS between the nomogram prediction and the actual observation in the multicenter cohort. Nomogram predicted survival is plotted on the x-axis; actual survival is plotted on the y-axis. A plot along the 45° line indicated a perfect calibration model in which the predicted probabilities were consisted with the actual outcomes. (d–f) Decision curves of the nomogram predicting OS in the multicenter cohort. The x-axis represents the threshold probabilities, and the y-axis measures the net benefit. The dashed line represents the nomogram for OS.
Proposal and validation of novel TNLODDS staging system
Using the AHRs based on the multivariable Cox model, a novel staging system incorporating LODDS classification was proposed, and ESCC patients were categorized into three new groups (Appendix 1). The survival curves showed that the novel TNLODDS classification had great ability to allow prognostic stratification for OS (5-year OS: stage I vs II vs III, 32.39%, 16.73% and 6.20%, p < 0.001), CSS (5-year CSS: stage I vs II vs III, 52.20%, 32.20%, and 14.7%, p < 0.001) and cancer-specific mortality in the multicenter cohort (5-year: stage I vs II vs III, 40.43%, 55.40%, and 66.97%; Figure 4). The novel classification also has the ability to predict prognosis in the SEER data set (Supplementary Figure S10). For patients in the multicenter cohort, as measured by C-index, the TNLODDS staging system (OS: 0.652, 95% CI: 0.596–0.713; CSS: 0.650, 95% CI: 0.608–0.695) showed better discriminability capacity than the AJCC TNM (OS: 0.615, 95% CI: 0.565–0.670; CSS: 0.621, 95% CI: 0.578–0.667) and the TNLNR staging systems (OS: 0.638, 95% CI: 0.623–0.653; CSS: 0.639, 95% CI: 0.602–0.678). Meanwhile, the TNLODDS staging system had higher R 2 (OS: 0.180; CSS: 0.176) than the AJCC TNM (OS: 0.134; CSS: 0.127) and the TNLNR staging systems (OS: 0.158; CSS: 0.153). Regarding the results of tdROC analyses, the TNLODDS staging system had 5-year AUC value of 0.695 (95% CI: 0.642–0.752) for OS and 0.691 (95% CI: 0.652–0.732) for CSS, which were higher than other two staging systems. In the SEER cohort, the TNLODDS staging system also had higher R2, AUC, and C-index value than those of other staging systems (Supplementary Table S3 and Supplementary Figure S11).

(a) OS, (b) CSS, and (a) CIF of cancer-specific mortality for ESCC patients grouped by the novel TNLODDS classification in the multicenter cohort.
Discussion
Not until the 7th edition of the AJCC TNM staging system were the N criteria for esophageal carcinoma subclassified according to the number of regional LNs containing metastases. 22 Moreover, many studies have reported LNR, is of prognostic value for EC patients.23,24 However, neither TLN nor LNR is included as a prognostic factor in the revised TNM staging system for ESCC patients. 4 Based on a large multicenter cohort, our study compared the predictive ability of three LN staging algorithms for the outcomes of ESCC patients. Our analysis suggested that LODDS outperformed the 8th pN and LNR as a classification method, whether the patterns were continuous or stratified. Furthermore, we developed and validated the first two nomograms to predict OS and cancer-specific mortality for ESCC patients using the LODDS classification postoperatively.
Only a few previous studies have compared the three LN staging algorithms for EC. Cao et al. 25 suggested that LODDS was more accurate than either number of pLN or LNR in patients undergoing resection for EC, which was consistent with our results. However, the findings of Cao’s study were mainly derived from the SEER database, which lacks details regarding the choice of surgical approach and the resection margins. In addition, that study contained far fewer patients with ESCC than with adenocarcinoma. The small sample size of the validation cohort also limited the credibility. Moreover, no existing study has accounted for competing risks; this methodological weakness could lead to a substantial bias in risk estimation. In this study, OS, CSS, and CSS with a competing risk of non-ESCC death were all selected as survival endpoints; those who underwent radical surgery and treatment at the real-world institutions were recruited, which makes our results statistically convincing.
The 8th AJCC staging system divides ESCC patients into different pN subsets based on the absolute number of pLN, which is significantly affected by TLN. However, neither pN nor LNR is capable of distinguishing among cases where none or all of the LNs are involved. For example, suppose that patient A has a pLN number of 7 out of a TLN number of 7, patient B has 30 of 30, patient C has 0 of 7, and patient D has 0 of 30. Patients A and B have the same pN stage (pN3) and LNR stage (LNR3), as do patients C and D (pN0 and LNR0). However, their LODDS values are different (LODDS = 1.176 for patient A, 1.785 for patient B, –1.176 for patient C, –1.785 for patient D, respectively). The LODDS classifications of patients C and D are different (LODDS2 for patient C and LODDS1 for patient D). As shown in Supplementary Table S2, OS, CSS, and cancer-specific mortality were differed significantly between them, which mean that patients with the same pN and LNR have different prognoses. Besides the aforementioned example, there is another one which also highlights the prognostic value of LODDS for ESCC patients with inadequate LN examined. For patients with one PLN out of six TLNs, the N stage could move from pN1 stage (pLN = 1) to LNR2 stage (LNR = 0.167) and to LODDS4 stage (LODDS = –0.564). According to our results, the 5-year CSS and cancer-specific mortality rates were estimated to be significantly different for this patient (5-year CSS and cancer-specific mortality: pN1 stage, 29.3% and 59.2%; LNR2 stage, 26.6% and 60.0%; LODDS4 stage, 18.8% and 64.6%, respectively). Given that the estimated prognoses can vary by different classifications has been observed, this example illustrated that computation of the LODDS was able to change the prognosis for individual patients (especially those with small number of LN examined) in a meaningful way. Furthermore, theoretically, patients who had insufficient TLN retrieved were at an increased risk of stage migration or the probability of false negatives.26,27 Thus, it is important to identify a minimum number of LNs for harvesting by lymphadenectomy for ESCC patients to optimize survival and tumor staging. Regrettably, the value of extended lymphadenectomy remains controversial. Some researchers have even suggested that extensive lymphadenectomy can increase mortality among patients in certain tumor stages.8,13,28 Since there is no consensus about the minimal number of LNs that should be retrieved in ESCC patients, when the TLN is different, the ability of LODDS classification to separate N0 patients into different prognostic categories for different TLN is of great value for clinicians in decision-making.
Moreover, we conducted subgroup analysis to compare the prognostic discriminability between the LODDS and pN classifications according to the retrieved TLN. Similar with previous literature, ESCC patients were subdivided into insufficient and sufficient retrieved TLN groups by using 15 TLN as the threshold number.29,30 For patients with less than 15 TLN, the LODDS classification showed better prognostic discriminatory capacities than the pN classification (Supplementary Figure S12 and S13). In addition, this difference decreased in the sufficient retrieved TLN subgroups (Supplementary Figure S14 and S15). Our findings demonstrated that the small number of retrieved LNs might influence the prognostic discriminability of the staging systems.
In our final nomograms based on the results of the multivariate analyses, we included the LODDS classification, age, and gender in addition to pathological T-stage and the prognostic factors used in the AJCC system. In the external validation cohort, both calibration plots and DCAs showed optimal agreement between the prediction and actual observation, which guarantees the repeatability and reliability of the established nomogram. Our nomograms provide clinicians and patients the opportunity to assess the probabilities of OS and cancer-specific mortality.
This study should be considered in the context of its limitations. First, due to the complicated calculation method of the index, LODDS might not easily be obtained in clinical setting. We regarded our study as a preliminary exploration of the novel LODDS-based staging proposal for ESCC patients and hope to have the nomogram as a digital/online calculator in the future, which would allow clinicians to enter clinical information, and the calculator could calculate the LODDS or TNLODDS and provide prognosis prediction. Second, although our findings have been verified in both the Eastern and the Western cohorts, the optimal threshold for LODDS worldwide warrants further validation due to the heterogeneous backgrounds of tumor, patient and therapeutic approaches. Furthermore, we acknowledged that the new staging system embodied limited discriminatory advantages for prognosis for patients with early stage disease (especially those diagnosed with pT1N0M0). Moreover, in our study, patients received neoadjuvant therapy and patients with early stage who received endoscopic submucosal dissection (ESD) treatment were excluded, which decreased the generalizability of our findings. The surgical procedures, assessments, and enumeration of LNs varied among regions, surgeons, laboratories, and pathologists because our study was based on real-world patient information. However, the large sample size of this study partly compensates for this weakness. Last but not the least, it is warranted to have a clinical algorithm based on our findings to inform surveillance and adjuvant treatment for ESCC patients.
In conclusion, our study compared the prognostic ability of three staging algorithms for ESCC. We found that LODDS classification was superior in predicting the outcomes of ESCC in both a Chinese multicenter cohort and the SEER database. We then established and validated two nomograms as well as a novel staging system for predicting the survival of patients with resected ESCC; these could serve as precise tools to assist clinicians in estimating the postoperative survival of individual patients and improving clinical outcomes.
Supplemental Material
sj-docx-1-tam-10.1177_17588359211054895 – Supplemental material for Comprehensive analysis of prognostic value of lymph node classifications in esophageal squamous cell carcinoma: a large real-world multicenter study
Supplemental material, sj-docx-1-tam-10.1177_17588359211054895 for Comprehensive analysis of prognostic value of lymph node classifications in esophageal squamous cell carcinoma: a large real-world multicenter study by Junmiao Wen, Jiayan Chen, Donglai Chen, Salma K. Jabbour, Tao Xue, Xufeng Guo, Haitao Ma, Fei Ye, Yiming Mao, Jian Shu, Yangyang Liu, Xueguan Lu, Zhen Zhang, Yongbing Chen and Min Fan in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359211054895 – Supplemental material for Comprehensive analysis of prognostic value of lymph node classifications in esophageal squamous cell carcinoma: a large real-world multicenter study
Supplemental material, sj-docx-2-tam-10.1177_17588359211054895 for Comprehensive analysis of prognostic value of lymph node classifications in esophageal squamous cell carcinoma: a large real-world multicenter study by Junmiao Wen, Jiayan Chen, Donglai Chen, Salma K. Jabbour, Tao Xue, Xufeng Guo, Haitao Ma, Fei Ye, Yiming Mao, Jian Shu, Yangyang Liu, Xueguan Lu, Zhen Zhang, Yongbing Chen and Min Fan in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359211054895 – Supplemental material for Comprehensive analysis of prognostic value of lymph node classifications in esophageal squamous cell carcinoma: a large real-world multicenter study
Supplemental material, sj-docx-3-tam-10.1177_17588359211054895 for Comprehensive analysis of prognostic value of lymph node classifications in esophageal squamous cell carcinoma: a large real-world multicenter study by Junmiao Wen, Jiayan Chen, Donglai Chen, Salma K. Jabbour, Tao Xue, Xufeng Guo, Haitao Ma, Fei Ye, Yiming Mao, Jian Shu, Yangyang Liu, Xueguan Lu, Zhen Zhang, Yongbing Chen and Min Fan in Therapeutic Advances in Medical Oncology
Footnotes
Appendix
Proposed novel TNLODDS system for ESCC patients.
| NLOODS1 | NLODDS2 | NLODDS3 | NLODDS4 | |
|---|---|---|---|---|
| T1a | I | I | I | I |
| T1b | I | I | I | II |
| T2 | I | I | I | III |
| T3 | I | I | II | III |
| T4a | II | III | III | III |
ESCC, oesophageal squamous cell carcinoma.
Author contributions
Junmiao Wen, Jiayan Chen, Yongbing Chen, Salma K. Jabbour and Min Fan contributed to study design. Junmiao Wen, Jiayan Chen, Donglai Chen, Tao Xue, Xufeng Guo, Haitao Ma, Fei Ye, Yiming Mao, Jian Shu and Yangyang Liu collected the study data. Junmiao Wen, Jiayan Chen and Donglai Chen contributed to data analysis and interpretation. All the authors contributed to manuscript writing. Min Fan and Yongbing Chen reviewed the manuscript and contributed to quality control. All authors have reviewed the study and approved the final version. We appreciate the support from Jueren Wang (the École supérieure des sciences économiques et commerciales, France). The authors wish to thank Dr. Shaonan Fan (Fudan University, China) for helping editing this manuscript.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by the Clinical Research Plan of SHDC (No. SHDC2020CR3025B), the National Natural Science Foundation of China (grant number 82102724 and 82172076), Jiangsu Key Research and Development Plan (Social Development) Project (BE2020653), Suzhou Key Discipline for Medicine (SZXK201803), Suzhou Key Laboratory of Thoracic Oncology (SZS201907), Municipal Program of People’s Livelihood Science and Technology in Suzhou (SS2019061), Discipline construction project of the Second Affiliated Hospital of Soochow University (XKTJ-XK202004) and Scientific Program of Suzhou Municipal Health and Health Committee (LCZX202004).
Ethical approval
This study was approved by the Institutional Review Board of FUSCC (IRB number: 050432-4-1911D) and registered with ClinicalTrials.gov, number NCT04764240 (![]() ). Meanwhile, the institutional review boards of the other nine participating sites have waived the requirement of the ethics ID application, given the role of sub-investigators in the study. The permission to access the SEER database was received from the National Cancer Institute (the private SEER ID 10425-Nov2018). This study was performed in accordance with the Declaration of Helsinki.
). Meanwhile, the institutional review boards of the other nine participating sites have waived the requirement of the ethics ID application, given the role of sub-investigators in the study. The permission to access the SEER database was received from the National Cancer Institute (the private SEER ID 10425-Nov2018). This study was performed in accordance with the Declaration of Helsinki.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.