
Abstract
Background:
Although immune checkpoint inhibitors (ICIs) have improved survival for advanced wild-type non-small cell lung cancer (NSCLC), a lack of direct comparisons of various first-line treatments is clouding clinical decision-making. A network meta-analysis was conducted to compare current first-line treatments and identify the optimal regimen for patients with specific characteristics.
Methods:
PubMed, Embase, the Cochrane Central Register of Controlled Trials, Clinical Trials databases were searched from inception to 31 July 2020. Phase II/III randomized controlled trials (RCTs) comparing first-line treatments including chemotherapy, anti-angiogenesis, ICIs, and their combinations for previously untreated stage IIIB/IV or recurrent driver-gene wild-type NSCLC patients were included.
Results:
Twenty-six RCTs were identified and included, involving 16,977 patients and a total of 18 regimens. ICI-containing treatments led to significantly prolonged overall survival (OS) compared with ICI-free treatments (0.82, 0.72–0.93). ICI plus chemotherapy had significantly longer progression-free survival (PFS; 0.70, 0.58–0.86) and marginally longer OS (0.90, 0.79–1.05) compared with ICIs alone. Ranking highest in the Bayesian network meta-analysis, pembrolizumab plus chemotherapy, nivolumab plus ipilimumab and chemotherapy, had significantly superior OS than standard chemotherapy with or without bevacizumab treatments. Pembrolizumab-chemotherapy ranked first for OS, 1-year OS rate, and subgroups of non-squamous, PD-L1 ⩾1%, non-smoking, and liver metastasis; while nivolumab–ipilimumab–chemotherapy for squamous, PD-L1 <1%, brain metastasis NSCLC. Furthermore, the ICI-containing bevacizumab-free treatments, such as pembrolizumab plus chemotherapy, nivolumab and ipilimumab with or without chemotherapy, were not significantly different from atezolizumab plus chemotherapy and bevacizumab in OS.
Conclusions:
A combination of ICIs with chemotherapy, rather than double ICIs, is the best first-line treatment for advanced wild-type NSCLC, with synergy that leads to better long-term survival. The panoramic view of the relative efficacy of any two regimens with different rankings provides strong evidence for selecting optimal first-line ICIs according to patients’ clinical characteristics.
Keywords
Background
In first-line treatment of advanced non-small cell lung cancer (NSCLC), the third-generation platinum-based doublet chemotherapy (CT) has brought limited survival advantage,1,2 while maintenance therapy (MT) with CT 3 and/or anti-angiogenesis agents bevacizumab (BEV) 4 has moderately prolonged the survival of non-squamous NSCLC. Discovery of driver genes and their tyrosine kinase inhibitors (TKIs) advanced oncology into the era of targeted therapy and has significantly improved patient survival. 5 In 2014, development of immune checkpoints inhibitors (ICIs) against programmed-death 1 (PD-1) or its ligand (PD-L1), and cytotoxic T-lymphocyte-associated antigen 4 (CTLA4), have prolonged survival more than any previous treatments,6–8 and are novel therapeutic strategies for advanced driver-gene wild-type NSCLC.
Some ICIs alone significantly prolonged overall survival (OS) of advanced NSCLC patients with high PD-L1 expression, such as pembrolizumab (PEM) in KEYNOTE 024, 9 or atezolizumab (ATE) in IMpower 110. 10 Since mono-ICI is only suitable for to patients with high PD-L1 expression, more phase III randomized clinical trials (RCTs) with ICI-combination treatments have been completed rapidly and achieved positive outcomes.11,12 ICI-combination therapy includes ICIs plus CT, such as PEM plus pemetrexed and platinum in non-squamous NSCLC in KEYNOTE 021G 12 and KEYNOTE 189, 11 or PEM plus paclitaxel and platinum in squamous NSCLC in KEYNOTE 407 13 or further addition of BEV in non-squamous NSCLC in IMpower 150, 14 and dual ICIs targeting both PD-1/L1 and CTLA-4 in CheckMate 227,15,16 or dual ICIs plus CT in CheckMate 9LA. 17 However, without a direct comparison of these effective ICI-based treatments, it is a huge challenge for clinicians to select the most appropriate first-line treatment. Among ICI-based strategies, such as ICI combined with CT, doublet ICIs, doublet ICIs plus CT,18–20 which one is the best as the first-line treatment for advanced wild-type NSCLC? Are ICI-combination treatments besides ATE/CT/BEV 14 also superior to the conventional CT/BEV regimen? Can CT be avoided, as suggested in CheckMate 227? 16 Furthermore, is there a suitable individualized treatment regimen?
To address these complex questions reasonably, we conducted a network meta-analysis (NMA) directly and indirectly comparing all large RCTs of first-line treatments for advanced wild-type NSCLC. We reveal differences in efficacy and safety among all types of first-line regimens and their ranking probabilities in the overall and subgroup network, to provide strong evidence for the optimal treatment option for patients with specific characteristics.
Methods
This NMA was performed in accordance with the PRISMA extension statement for NMA 21 (Supplemental Table S1). Research was registered with PROSPERO (CRD42020184534).
Data sources and searches
PubMed, Embase, the Cochrane Central Register of Controlled Trials, and ClinicalTrials.gov databases were searched to find relevant articles up to 31 July 2020. Abstracts on NSCLC from several important international conferences (American Society of Clinical Oncology, European Society of Medical Oncology, and World Conference on Lung Cancer) from 2015 to 2020 were inspected to identify potentially relevant studies. For an outcome in the same trial, only the most recent data were kept. The detailed search strategy is shown in Supplemental Table S2.
Eligibility criteria
We included published phase II/III RCTs reported in English that met the following inclusion criteria: First, trials that enrolled previously untreated patients with histologically confirmed advanced (stage III/IV or recurrent) driver-gene wild-type NSCLC and compared two or more different arms of first-line treatments. Second, the hazard ratio (HR) or odds ratio (OR) and their 95% confidence interval (CI) of outcomes, such as OS, progression-free survival (PFS), overall response rate (ORR), and adverse event (AE) are available.
We excluded trials with methods other than CT, anti-angiogenesis or ICIs, such as targeted therapy (both TKI and mono-antibody) toward driver-gene, radiotherapy, immune cells or cytokines, cancer vaccines, oncolytic virus, and so on. We also excluded trials that studied specific populations, such as old patients, with poor ECOG scores or limited regions or lack of necessary outcomes. Further, we excluded trials using unavailable drugs. 22 In non-squamous NSCLC, trials without MT, or trials with MT that only provided outcomes of maintenance stage, were also excluded.
Given that MT with pemetrexed significantly improved OS of advanced non-squamous NSCLC,3,23 and is often included as control group in most ICI/CT RCTs,11,14,24 we included first-line CT plus maintenance CT (CT/Mpem) as an independent intervention from CT alone. Regarding use of either BEV or ICI therapy, MT has been indispensable for first-line treatment of advanced NSCLC for its confirmed function in prolonging survival. Therefore, we take the first-line treatment followed by MT (including CT, anti-angiogenesis, or ICI) as a sequential but integral approach for comparison and evaluation. Study selection diagram is shown in Figure 1.

Study selection.
Data extraction
Main data of qualified trials such as study ID, first author, publication year, number of patients, and pathological characteristics, treatments and outcomes were extracted into a spreadsheet for further analysis. All investigators independently extracted data parameters using a unified data extraction form.
The primary outcome was OS. Secondary outcomes were PFS, ORR and higher than grade 3 AEs (⩾3 AEs). All available direct and indirect evidence was synthesized to compare different treatments in terms of efficacy and safety, reported as HR/OR and corresponding 95% credible intervals (CrI) for OS, PFS, ORR and ⩾3 AEs.
Risk of bias assessment
Two investigators (QX and JG) independently assessed risk of bias of individual studies. Any disagreement was discussed and resolved by LL and LS to reach a consensus. The bias risk of included trials was assessed using the Cochrane Risk of Bias Tool, consisting of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and other sources of bias.
Data synthesis and analysis
Network plots were generated using Stata 15.0, choosing which treatments were compared directly or indirectly for different outcomes. NMAs were performed in a Bayesian framework using a Markov Chain Monte Carlo simulation technique within the GEMTC package in the R-Statistics and the J.A.G.S. program. Fixed and random-effect models were considered and compared using deviance information criteria. 25 We used non-informative uniform and normal prior distributions to fit the model, with four different sets of initial values. For each outcome, 150,000 sample iterations were generated with 100,000 burn-ins and a thinning interval of 1 except for ORR and ⩾3 AEs, for which we increased the thinning interval to 10 to minimize auto-correlation. We tested the adequacy of convergence (reaching a stable equilibrium distribution) using visual inspection methods of trace plots and estimating the values of the Brooks–Gelman–Rubin statistic. 26 Once convergence was established, the posterior distributions for the model parameters were obtained. To determine whether there were issues of inconsistency, an unrelated mean effects model was used to assess inconsistency by comparing the model fit and between-study variance (heterogeneity) estimate of the pair-wise comparisons against the results of the consistency model. 25 Network consistency was also evaluated by comparing the direct estimates with the indirect estimates for each comparison, with a node-splitting technique. 27 p < 0.05 indicated significant inconsistency. To measure the consistency of the effect size, pair-wise meta-analyses were further performed with the frequentist method for head-to-head trials based on two or more comparisons, using the model consistent with NMA. Heterogeneity was assessed between studies using the Q test and I 2 statistic. The estimated I 2 values under 25%, between 25% and 50%, or over 50% indicated low, moderate, or high heterogeneity, respectively.
The probability of being at each rank was estimated for all treatments. A treatment hierarchy was determined using the probability of being the best treatment by using the surface under the cumulative ranking curve (SUCRA; score of 0–1 and 1 is the best).
Sensitivity analysis
In addition to the principal analyses, two sensitivity analyses were conducted to test the robustness and reliability of results by excluding phase II RCTs or trials with highly selective subgroup populations.
Results
Studies characteristics
Twenty-six trials3,4,9–19,24,28–38 were included involving 16,977 patients and a total of 18 treatment regimens (Table 1). They are (a) ICI-free treatments, including platinum-based doublet CT, CT/Mpem, CT/BEV, or CT/BEV with maintenance of pemetrexed (CT/BEV/Mpem); (b) ICI-containing treatments, including mono-ICI, namely PEM, nivolumab (NIV), ATE, durvalumab (DUR); (c) ICI-combination treatments, including ICIs plus CT (PEM/CT, NIV/CT, ATE/CT, camrelizumab (CAM)/CT, ipilimumab (IPI)/CT), ATE plus CT and BEV (ATE/CT/BEV); (d) doublet ICIs including NIV/IPI, DUR plus tremelimumab (DUR/TRE); and (e) dual ICIs plus CT (NIV/IPI/CT or DUR/TRE/CT). CheckMate 227 was divided into three trials including cohort 1 with PD-L1 ⩾1% (Part 1a, containing 3 arms); cohort 2 with PD-L1 <1% (Part 1b, 3 arms); and cohort 3, all-comers (Part 2, 2 arms), each cohort with different populations. The networks are shown in Figure 2a. The detailed risk of bias assessment is summarized in Supplemental Figure S1.
Key study features.

Data are expressed as intervention/control unless indicated otherwise.
⩾3 AEs, grade ⩾3 adverse events; ATE, atelizumab; BEV, bevacizumab; BSC, best supportive care; CAB, carboplatin; CAM, camrelizumab; CIS, cisplatin; CT, chemotherapy; DCR, disease control rate; DOR, duration of overall response; DUR, durvalumab; GEM, gemcitabine; IPI, ipilimumab; irORR, immune-related ORR; irPFS, immune-related progression-free survival; ITT, intent-to-treat; M, maintenance therapy; Meta, metastasis; mITT, modified intent-to-treat; mut, mutation; NG, not given; NIV, nivolumab; non-squ, non-squamous; ORR, objective response rate; OS, overall survival; Pb-CT, platinum-based doublet CT; PEM, pembrolizumab; pem, pemetrexed; PFS, progression-free survival; PTX, paclitaxel; Squ, squamous; TOR, time to response; TRE, tremelimumab.
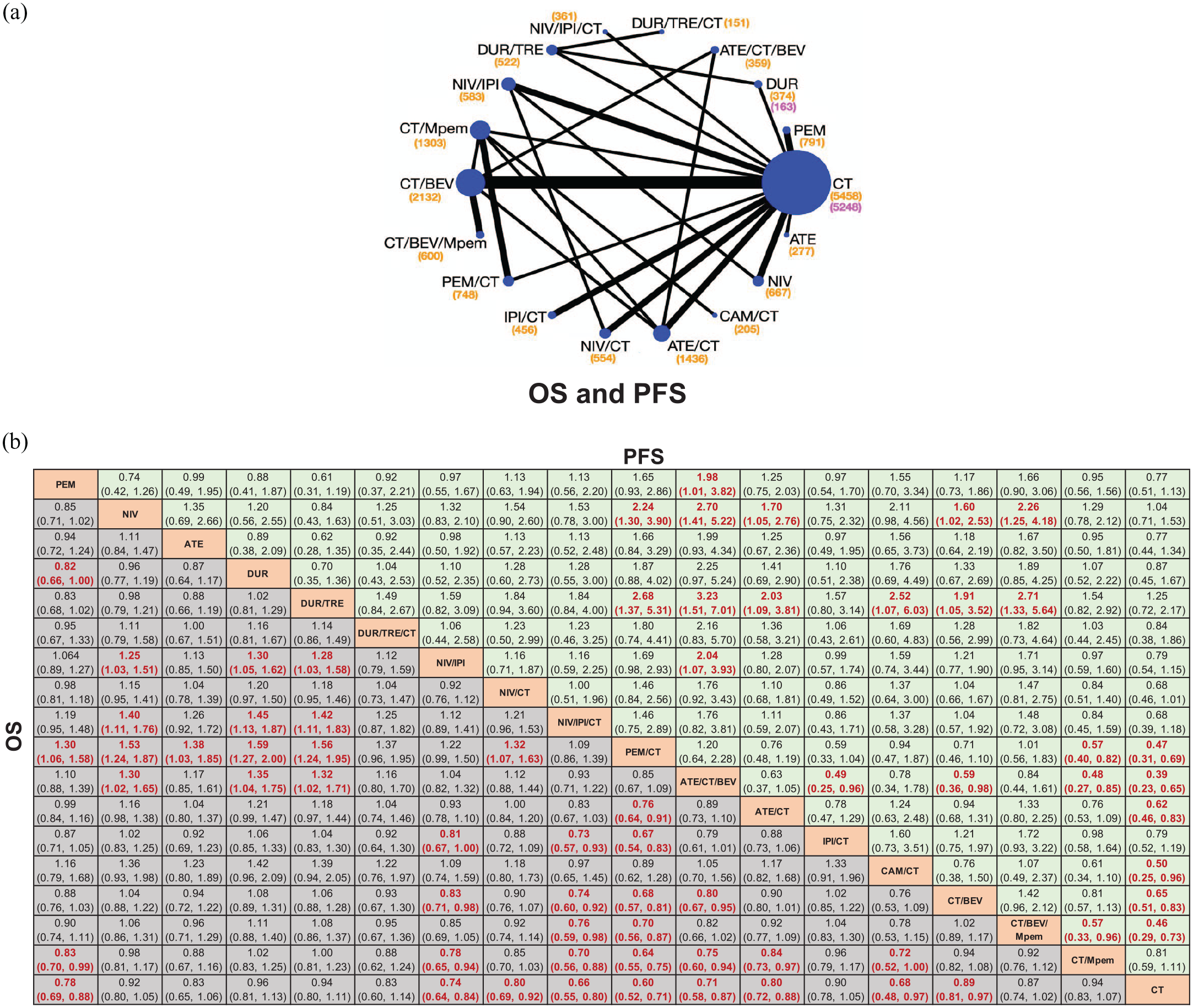
Network meta-analysis of comparisons of overall survival and progression-free survival in patients with advanced wild-type NSCLC. (a) Network diagrams of comparisons on overall survival (OS) and progression-free survival (PFS). Each circular node represents a type of treatment. Each line represents a type of head-to-head comparison. Node size and line thickness are weighted according to the number of studies evaluating each treatment and direct comparison, respectively. The total number of patients receiving a treatment is shown in brackets. The total number in each node for OS is the same as that for PFS except for durvalumab (DUR) and chemotherapy (CT) (marked in red for PFS). (b) Pooled estimates of the network meta-analysis of OS and PFS. Data in each cell are HR (95% CrIs) for the comparison of row-defining treatment versus column-defining treatment.
Position evaluation of ICIs versus chemotherapy
As first-line treatments, ICI-containing treatments had significantly prolonged OS (HR 0.82, 95% CrI 0.72–0.93) and marginally improved PFS (0.85, 0.66–1.07) compared with ICI-free treatments (Supplemental Figure S2a). Interestingly, CT-free treatments had better OS than CT alone (0.86, 0.81–0.91), but were significantly inferior to CT-combination treatments in both OS (0.87, 0.79–0.95) and PFS (0.66, 0.57–0.78; Supplemental Figure S2b).
Furthermore, ICI/CT had prolonged OS (0.75, 0.67–0.83) and PFS (0.63, 0.55–0.72) over CT. ICI/CT also had significantly longer PFS (0.70, 0.58–0.86) but not OS (0.90, 0.79–1.05) compared with ICI alone. ICIs had equal PFS (0.89, 0.76–1.04) but longer OS (0.83, 0.74–0.92) over CT. When comparing doublet ICIs with ICI/CT, the results were similar to the trend of the whole ICIs versus ICI/CT (Supplemental Figure S2).
Overall outcomes
In terms of OS of specific treatments, PEM/CT showed significant benefits over most other treatments, including both ICI-free treatments, such as CT ± Mpem ± BEV; or many ICI-containing treatments, such as ATE/CT, DUR/TRE and all mono-ICI. NIV/IPI/CT was superior to all ICI-free treatments. ATE/CT/BEV was equal to most ICI-containing treatments, such as PEM/CT, ATE/CT, NIV/IPI ± CT, or DUR/TRE/CT, but was better than all ICI-free treatments except for CT/BEV/Mpem. CT alone had nearly the shortest OS, while CT/Mpem reached an OS not significantly different from CT/BEV and CT/BEV/Mpem. In terms of PFS, ATE/CT/BEV, PEM/CT, and CT/BEV/Mpem showed significant advantages compared with CT ± Mpem, while CAM/CT, ATE/CT, and CT/BEV were better than CT only (Figure 2b).
When analyzing ORR of first-line therapy, ATE/CT/BEV, PEM/CT, CAM/CT, NIV/CT, CT/BEV, and ATE/CT each showed a similar superior efficacy compared with CT. In general, the ORRs of CT-free treatments were lower than that of CT-containing ones. Addition of anti-angiogenesis or/and ICI to CT could improve ORR. Conversely, CT-free treatments showed markedly lower than the CT-containing ones with ⩾3 AEs. AEs ⩾3 in most ICI/CT and CT/BEV were significantly higher than pure ICIs. In combination treatments, DUR/TRE ± CT, NIV/IPI, PEM/CT showed the fewest ⩾3 AEs, equally with CT ± Mpem (Supplemental Figure S3). Considering ICI-related AEs, higher incidences of rash, hyper/hypothyroidism were observed in DUR/TRE/CT and ATE/CT/BEV separately (Supplemental Figures S4 and S5).
Subgroups of various clinicopathological characteristics
Pathology
In the squamous NSCLC subgroup, NIV/IPI/CT, NIV/IPI, NIV/CT, PEM/CT and PEM showed improved OS. PEM, NIV/CT, PEM/CT achieved best PFS outcomes (Figure 3a). In non-squamous NSCLC, the most significantly prolonged OS were from PEM/CT, CAM/CT, and ATE/CT/BEV, while PEM/CT and ATE/CT/BEV achieved better PFS (Figure 3b). Furthermore, there was no significant difference in OS/PFS between pemetrexed-based and paclitaxel-based regimens in non-squamous NSCLC. When combined with ICIs, pemetrexed/platinum plus PEM (KEYNOTE 189 mode) was the most effective solution, with significantly longer OS than that of pemetrexed/platinum plus ATE (IMpower 132 mode) or paclitaxel/platinum plus ATE (IMpower 130 mode), or all other ICI-free regimens. But the pemetrexed/platinum plus PEM regimen was equal to ATE/paclitaxel/platinum plus BEV (IMpower 150 mode) (Supplemental Figure S6).
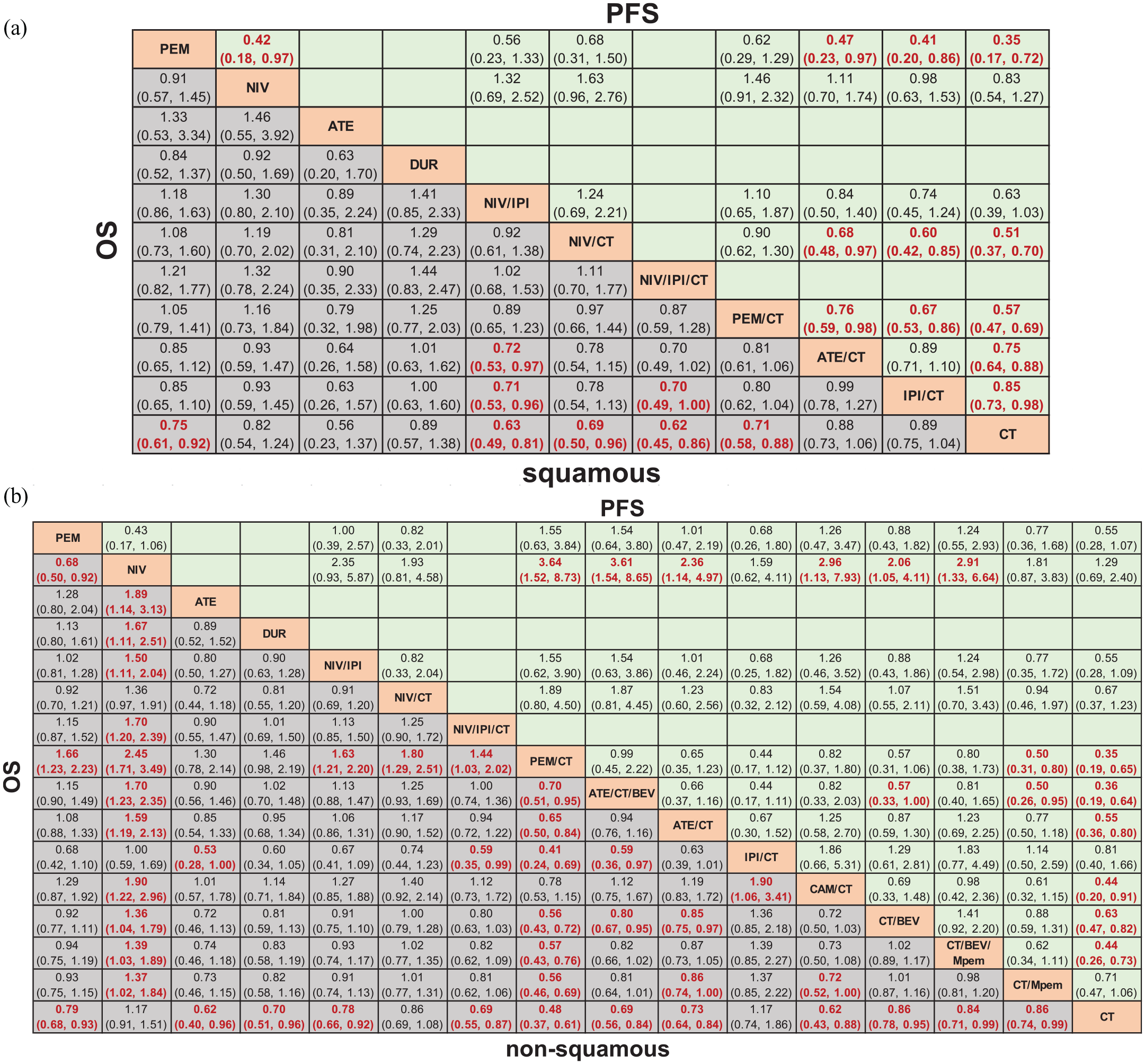
Pooled estimates of subgroup analyses according to pathology. (a) Pooled hazard ratio (HR, 95% CrIs) for overall survival (OS) and progression-free survival (PFS) of squamous subgroup. (b) Pooled HR (95% CrIs) for OS and PFS of non-squamous subgroup.
PD-L1 expression
In both PD-L1 <1% (or TC/IC = 0) and PD-L1 ⩾1% (or TC1-3/IC1-3) subgroups, NIV/IPI/CT, PEM/CT, NIV/IPI could prolong OS to a similar extent compared with CT. In general, OS of BEV/CT had no statistical difference with ICI-based treatments in PD-L1 <1% subgroup, but was significantly shorter than most ICI combination treatments in PD-L1 ⩾1% subgroup (Figure 4a and Supplemental Figure S7a). In the PD-L1 1–49% or TC1-2/IC1-2 groups, NIV/IPI/CT and PEM/CT had better OS than CT ± BEV and NIV/IPI. As PD-L1 expression increased to ⩾50%, all the differences on OS among the ICI-based therapies disappeared, and most of them showed significant OS benefits over CT (Figure 4b and Supplemental Figure S7b).

Pooled estimates of subgroup analyses according to PD-L1 expression. (a) Pooled HR (95% CrIs) for overall survival (OS) in patients with programmed-death ligand 1 (PD-L1) ⩾1% (or TC/IC = 1/2/3) and PD-L1 <1% (or TC/IC = 0) subgroups. (b) Pooled HR (95% CrIs) for OS of PD-L1 ⩾50% (or TC/IC = 3) and PD-L1 1–49% (or TC/IC = 1/2) subgroups. (c) Pooled results of head-to-head comparisons on OS according to PD-L1 expression using frequentist pair-wise meta-analyses. (d) Pooled results of head-to-head comparisons on OS according to PD-L1 expression using Bayesian pair-wise () and network () meta-analyses. Data in each cell are HR (95% CrIs) for the comparison of row-defining treatment versus column-defining treatment.
Tumor mutation burden (TMB)
In the subgroup with high TMB (including tTMB and bTMB), DUR/TRE, NIV/IPI, PEM/CT showed significantly prolonged OS and PFS compared with CT. In low TMB populations, OS of PEM/CT was statistically superior to CT, and similar to NIV/IPI. PEM/CT also showed better PFS than any other treatments in the low TMB group (Supplemental Figure S8).
Smoking or gender
ATE offered the best OS advantage for smokers but ranked last in non-smokers. PEM/CT showed a significant OS benefit in both smokers and non-smokers, and dramatically reduced the risk of death by 70–80% in non-smokers. NIV/IPI/CT and NIV/IPI led to a similar outcome as PEM/CT in smokers but were inferior to PEM/CT and had no significant advantage over other treatments in non-smokers. CT/BEV/Mpem regimen showed leading OS among non-smokers but lagged behind the ICI-based regimens among smokers (Supplemental Figure S9). In females, PEM/CT showed an overwhelming OS advantage compared with other treatments. In males, NIV/IPI ± CT yielded superior OS than PEM/CT (Supplemental Figure S10).
Age or ECOG
PEM/CT, ATE, and NIV/IPI/CT showed the best OS benefit in both ECOG 0 and 1 populations (Supplemental Figure S11). In patients less than 65 years old, the OS of PEM/CT was significantly longer than most other treatments except NIV/IPI/CT. NIV/IPI/CT was only superior to CT ± Mpem or CT/BEV. In patients ⩾65, PEM/CT, NIV/IPI/CT, NIV/IPI and ATE/CT obtained significantly longer OS than CT ± Mpem (Supplemental Figure S12).
Liver or brain metastasis
In patients with a liver metastasis, PEM/CT offered both OS (0.62, 0.39–0.98) and PFS (0.52, 0.34–0.80) advantages over CT/Mpem. ATE/CT/BEV had significant OS (0.54, 0.33–0.88)/PFS (0.41, 0.27–0.63) superiority compared with CT/BEV (Supplemental Figure S13). In patients with a brain metastasis, NIV/IPI/CT and PEM/CT lowered the death risks by nearly 60% compared with CT/BEV-based treatments. PEM/CT significantly improved PFS for patients with/without brain metastasis (Supplemental Figure S14).
Rank probabilities
The Bayesian ranking probabilities and corresponding SUCRA of comparable treatments in different populations are shown in Figure 5, Supplemental Figures S15 and S16. In overall, PEM/CT was most likely to be ranked first for OS, 1-year OS rate; ATE/CT/BEV for PFS, ORR and ⩾3 AEs; and DUR/TRE/CT for 2-year OS rate. Considering certain pathological characteristics, treatments with the probability of being ranked first in OS were as follows: PEM/CT (non-squamous NSCLC, PD-L1 ⩾1%, non-smoking, female, ECOG 0 or 1, <65, liver metastasis); NIV/IPI/CT (squamous NSCLC, PD-L1 <1%, PD-L1: 1~49%, brain metastasis); DUR/TRE/CT (PD-L1 ⩾50%, ⩾65); DUR/TRE (high TMB); NIV/IPI (low TMB); ATE (smoking, male).
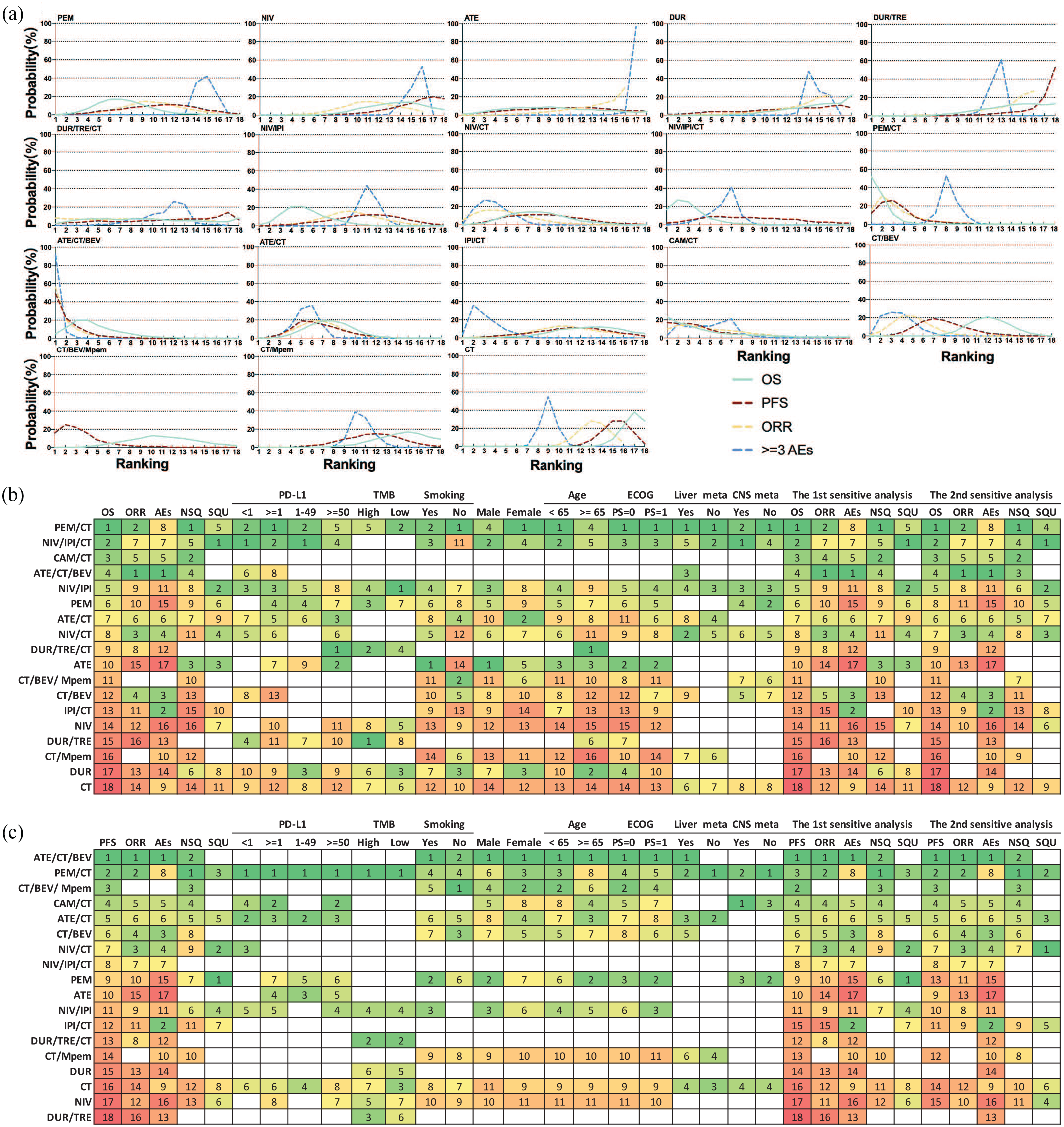
Bayesian ranking profiles of comparable treatments on efficacy and safety for patients with advanced wild-type non-small cell lung cancer (NSCLC). (a) Profiles indicate the probability of each comparable treatment being ranked from first to last on overall survival (OS), progression-free survival (PFS), objective response rate (ORR), grade ⩾3 adverse events (⩾3 AEs), 1-year OS rate and 2-year OS rate. (b) Number in each cell indicates the probability of each treatment being ranked from first to last on overall OS, OS for subgroups, ORR and ⩾3 AEs according to the surface under the cumulative ranking curve (SUCRA) presented in Supplemental Figure S16. (c) Number in each cell indicates the probability of each treatment being ranked from first to last on overall PFS, PFS for subgroups, ORR and ⩾3 AEs according to the SUCRA value presented in Supplemental Figure S16.
Consistency and inconsistency assessment
The fit of the consistency model in most comparisons was similar or better than the fit of the inconsistency model, except for PFS (overall, non-squamous, male, and age <65 subgroups) and ORR, for which a random model was used (Supplemental Table S3). Inconsistency in the NMA estimates using the node-splitting approach did not show significant differences in comparisons of OS except for PEM/CT versus CT, CT/Mpem versus CT, CT/Mpem versus PEM/CT (Supplemental Table S4). Convergence of four chains was verified visually by inspecting the trace plots and the Brooks–Gelman–Rubin diagnostic statistic with values around 1 (Supplemental Figure S17). No inconsistency was found between direct and indirect comparisons by pair-wise Bayesian or frequentist meta-analyses and NMAs (Figure 4c, d and Supplemental Figures S18 and S19).
Sensitivity analyses
To ensure the reliability and robustness of the results, we conducted two sensitivity analyses by excluding phase II studies, or studies with highly selected patients (Supplemental Table S5). The results obtained are the same as the original in the overall trend, for most statistical changes occurred in PFS or ORR, instead of OS (Supplemental Figures S20 and S21).
Discussion
The main findings of this NMA are as follows: (1) In comprehensive terms of OS, ICI combination therapy (including ICI plus CT, doublet ICIs, doublet ICIs plus CT) is more effective than ICI-free therapy (including CT or following MT with pemetrexed or BEV) for survival of advanced wild-type NSCLC. Of these, the combination of ICI with CT is the best first-line treatment. (2) In general, PEM/CT has the best outcome, and NIV/IPI/CT ranks second. (3) ATE/CT/BEV has the highest ORR and PFS, but its AE also ranks first.
The position of ICI as the key first-line treatment in advanced driver-gene wild-type NSCLC was confirmed by the NMA. Indirect comparison implied that ICI-containing treatments were significantly superior to ICI-free treatments in OS, partly consistent with conclusions of previous meta-analyses.40,41 Among the 18 comparable treatments, the top 10 OS were all from ICI-based treatments, and all ICI-free treatments ranked in the bottom eight. In contrast to ICI, the current status of CT seems to be crumbling. Interestingly, although CT-free strategies showed better OS than CT alone, CT-combination treatments surpassed CT-free treatments completely in terms of OS/PFS/ORR. So far, NVI/IPI obtained a positive survival result in CheckMate 227 16 and was approved by the FDA in the population with high PD-L1 expression. Another anti-PD-L1/CTLA4 combination, DUR/TRE failed to achieve the success of NVI/IPI regimen even in the population with PD-L1 ⩾25% in MYSTIC trial. 38 Specifically, our NMA found that ICI/CT combination is superior to ICI alone and is the most reliable combination mode. However, NVI/IPI ranks 11th in PFS, fifth in OS, and ninth in 2-year OS rate in the NMA, lagging behind most ICI/CT combinations.
Among the ICI/CT combinations, PEM/CT showed the highest efficacy and widest applicability, with better efficacy than most other combinations of ICI/CT. The NIV/IPI/CT regimen from CheckMate 9LA 17 ranked first in subgroups of squamous NSCLC, PD-L1 <49%, and brain metastasis. NMA found that CT also had a significant synergistic effect on the doublet ICIs NIV/IPI and DUR/TRE, with greatly improved efficacy and a limited increase in side effects.
The combination of ICI and CT expanded the advantages of either of them. Besides killing tumor cells fast to release tumor antigens, and activate the immune responses of CD8+ T cells,42,43 CT can help avoid the hyper-progression possibly caused by ICI, and protect patients from early disease deterioration before ICI takes effect. ICI functions slowly but persistently to make up for the shortcomings of CT. Synergy leads to long-term patient survival. As CT is indispensable but has inevitable toxicities, it is especially important to pinpoint the precise position of CT. As designed in CheckMate 9LA, 17 by reducing the CT cycles and performing CT at the beginning of the treatment course, 37 short-term CT may avoid possible early progressions with simultaneous decreasing toxicity, finally obtaining the maximum clinical benefit combined with immunotherapy. Therefore, in the era of immunotherapy, it is worth exploring how to reasonably apply CT in combination to maximize efficacy and synergy.
To date, only the IMpower150 trial reported that the addition of ATE to CT/BEV brought extra OS advantage, and no difference existed between ATE/CT and CT/BEV in non-selected populations of non-squamous NSCLC. 44 As most phase III ICI-combination RCTs chose CT alone instead of CT/BEV as a control group, it remains uncertain whether they are definitely better than CT/BEV. So we included large RCTs related to CT/BEV such as ECOG4599, 4 BEYOND 18 and AVAiL 34 into the research network as ICI-free treatments. In addition to ATE/CT/BEV, several ICI-combination regimens, such as PEM/CT, NIV/IPI/CT, and NIV/IPI, had significantly superior OS compared with CT/BEV-based treatments. Although CT/BEV/Mpem had significantly longer PFS than many ICI-based treatments, it failed to translate into OS benefit. On the other hand, ATE/CT/BEV yielded significant PFS but not OS benefit compared with ATE/CT and most other ICI/CT regimens or NIV/IPI.
In the comprehensive subgroup analysis based on main clinicopathological features in the NMA, rank probability analyses showed that PEM/CT and NIV/IPI/CT regimens led the treatments in most subgroups. As PD-L1 expression increases, the survival benefits of immune-related treatments for patients gradually expand with HR gradually decreasing, and its gap between ICI-free therapy, such as CT ± BEV, increasing, while the gap among ICIs is getting smaller. When PD-L1 expression increased to ⩾50%, all differences in OS among ICI-based therapies disappeared. This suggests that ⩾50% PD-L1 expression is a good marker to screen ICI-dominant group to benefit completely from immunotherapy, no matter what it is or what combination it is. In patients with liver metastases in NSCLC, ATE/CT/BEV and PEM/CT significantly prolong OS. In patients with brain metastases, NIV/IPI/CT and PEM/CT can reduce the risk of death by about 60%. Consistent with relevant reports, 45 ICI has shown excellent efficacy in brain metastases. Perhaps this is related to the suppression state of the local immune microenvironment in brain metastatic lesions. 46 ICI can reach the brain parenchyma through the lymphatic circulation, or lymphocytes activated by ICI outside the brain can enter brain to function. 47 For these clinically refractory patients, ICI shows significant and unique survival advantages over conventional therapy.
Among all regimens, ATE/CT/BEV ranked first in both PFS and ORR, but its AEs were also first-ranking. Considering the severity of side effects, single ICIs had the least AEs, doublet ICIs had slightly increased AEs; ICI/CT showed moderate AEs, and ICI plus CT combined with anti-angiogenesis had the highest AEs. However, we must pay attention to the unique side effects and their effective control, to ensure the safety of ICI-related treatment.
To our knowledge, this is the first NMA covering all first-line treatment and MT strategies in advanced wild-type NSCLC. Through integrated comparison and analysis, this study provides a panoramic view of the relative efficacy of any two first-line treatments and their ranking in the network intuitively for the overall population and for subgroups with specific pathological characteristics. Most former similar studies compared only some of the treatment measures we included, such as comparison of ICI/CT with CT or ICI,39,48 or only for limited involvement of subgroups (pathological types, or different PD-L1 expressions).39,49,50 Therefore, conclusions drawn may be of limited representation or effectiveness and may not meet the complicated needs of clinical decision.
The findings of this study suggest treatments with clear and feasible ranking probability in comprehensive overall populations and subgroups according to the clinicopathological characteristics including pathology, PD-L1 expression, tissue or blood TMB, gender, smoking, ECOG, age, and liver or brain metastasis. These outcomes help clinicians to choose the optimal first-line option for each individual patient.
Our study has some limitations. First, we included all studies covering various strategies for first-line treatments of advanced NSCLC with a long time-span, so large differences may exist in the types of population characteristics reported. For instance, previous trials of CT or anti-angiogenesis seldom reported gene mutation or PD-L1/TMB expression. Second, the different characteristics and criteria for enrollment in various studies may lead to biased results. Third, the direct comparison of some treatments was involved in just one study, which may lead to the cascade amplification of the treatment outcome in the network. Finally, because we are committed to pursuing the most up-to-date data for each result, some data in this study were extracted or calculated from a meeting summary or Figures, with possibly limited accuracy and authority.
Conclusion
Among the main treatment strategies of first-line treatments of driver-gene wild-type advanced NSCLC, ICI has been indispensable, while CT is still important. Based on both direct evidence and indirect comparison with the NMA, combination of ICI and CT is currently the most effective treatment. Ranking highest in the Bayesian NMA, pembrolizumab plus chemotherapy, nivolumab plus ipilimumab and chemotherapy, had significantly superior OS than standard chemotherapy with or without bevacizumab treatments. Pembrolizumab-chemotherapy ranked first for OS, 1-year OS rate, and subgroups of non-squamous, PD-L1 ⩾1%, non-smoking, and liver metastasis; nivolumab–ipilimumab–chemotherapy for squamous, PD-L1 <1%, brain metastasis NSCLC. Furthermore, pembrolizumab plus chemotherapy, nivolumab and ipilimumab with or without chemotherapy, were equal to atezolizumab plus chemotherapy and bevacizumab in OS. These results support selection of the most appropriate treatment regimens according to the clinical characteristics of patients for long-term survival and manageable adverse effects.
Supplemental Material
sj-pdf-1-tam-10.1177_17588359211018537 – Supplemental material for Selection of optimal first-line immuno-related therapy based on specific pathological characteristics for patients with advanced driver-gene wild-type non-small cell lung cancer: a systematic review and network meta-analysis
Supplemental material, sj-pdf-1-tam-10.1177_17588359211018537 for Selection of optimal first-line immuno-related therapy based on specific pathological characteristics for patients with advanced driver-gene wild-type non-small cell lung cancer: a systematic review and network meta-analysis by Lei Sheng, Jing Gao, Qian Xu, Xue Zhang, Miao Huang, Xin Dai, Song Li and Lian Liu in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We thank Alexandra Marshall (Marshall Medical Communications) for editing the manuscript.
Author contributions
LL, SL and LS designed the study. LS, JG, QX, XZ, JH and DX ran the systematic search, collected the data and performed the analyses. LL and LS discussed the results and wrote the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.