
Abstract
Background:
There have been few studies on the efficacy of tyrosine kinase inhibitors in lung carcinomas. The purpose of this study was to evaluate the effect of gefitinib as a first-line therapy in patients with advanced non-small cell lung cancer (NSCLC) who were positive for epidermal growth factor receptor (EGFR) mutations.
Methods:
This prospective analysis included 120 patients with advanced NSCLC with EGFR mutations who were administered gefitinib as the first-line therapy. Patient follow-up and evaluation were performed every 3 months or when there were symptoms of progressive disease. The main criteria for the analysis of response were progression-free survival (PFS) and overall response rate (ORR). The secondary criteria were overall survival (OS) and disease control rate (DCR). In addition, the relationship of OS with sex, smoking history, and performance status (PS), as well as gefitinib toxicity were analyzed.
Results:
The ORR and DCR were 59.2% and 95.8%, respectively. The median PFS was 14.5 months and the median OS was 33 months. The longer OS was statistically significant in women and non-smokers, and the patients had a good PS. Adverse events occurred in 59.2% patients, but most of them were grade 1 and 2 events.
Conclusion:
This study conducted in Vietnam suggests the effectiveness of gefitinib as a first-line treatment option in patients with advanced NSCLC and positive EGFR mutations regardless of whether the patients have a good PS or not. In particular, targeted therapy with gefitinib improved the OS in women and non-smokers.
Background
Epidermal growth factor receptor (EGFR) mutation is a common mutation among Asian patients with non-small cell lung cancer (NSCLC), with an incidence rate of approximately 40–50%, while the incidence is only about 10–15% in non-Asian patients. 1 Phase III, multicenter clinical trials have shown that patients with advanced NSCLC with EGFR mutations respond well to tyrosine kinase inhibitors (TKIs). Moreover, the third-generation TKI osimertinib was observed to be more effective than the first-generation TKIs gefitinib and erlotinib.2–5 Second-generation TKIs including afatinib and dacomitinib are also reportedly more effective than chemotherapy in patients with NSCLC who are positive for EGFR mutations.6,7 In patients with advanced NSCLC with EGFR mutations, targeted therapy using TKIs is the preferred treatment option worldwide including in Vietnam. As the use of osimertinib is limited owing to its high cost and non-coverage by health insurance, the first- and second-generation TKIs are the preferred choice. Thus, studies evaluating the effectiveness of TKIs in Vietnamese patients are urgently required. There are currently some ongoing studies investigating the efficacy of erlotinib, gefitinib, and afatinib in patients with advanced NSCLC in some of the major medical centers in Vietnam; however, these studies are limited and have small sample sizes. In addition, there are some issues that have not been clarified yet; EGFR gene mutations are known to have higher incidence rates in women and non-smokers, and gefitinib can be administered to patients with a poor performance status (PS). The differences in the efficacy of gefitinib between men and women, between smokers and non-smokers, or between patients with a good PS versus those with a poor PS have rarely been mentioned in previous studies. Therefore, the aims of this study were to evaluate the effects of gefitinib treatment in patients with advanced NSCLC harboring EGFR mutations in our center as well as to analyze the above issues.
Methods
Patients
A total of 120 patients with advanced NSCLC with EGFR mutations were treated with gefitinib as the first-line therapy for a period of 4 years from January 2016 to January 2020.
Methods
Study design
This was a prospective real-world study.
Study protocol
The study protocol involved clinical examination, paraclinical testing, chest radiography, chest computed tomography, and tumor biopsy. Tissue samples were obtained after biopsy as well as post-surgery. The pathologist localized the malignant cells and then sent a specimen for genetic mutation testing. Following this, EGFR mutation tests were performed, and patients with NSCLC who were positive for EGFR mutations were administered gefitinib (IRESSA) as the first-line therapy.
The selection criteria for targeted therapy included: (1) patients with stage IIIB, IIIC, and IV NSCLC; (2) patients >18 years old; (3) had received no prior systemic treatment for advanced NSCLC; (4) duration of treatment was at least 3 months at the time of data analysis; (5) patients provided consent for treatment with gefitinib; and (6) sufficient information on treatment was available. The exclusion criteria were as follows: (1) patients with stage I, II, and IIIA NSCLC; (2) patients with small-cell lung cancer; and (3) patients did not provide consent for treatment with gefitinib.
The patients were followed up every 3 months or when the patients had symptoms of progressive disease. Tumor response was evaluated using the Response Evaluation Criteria in Solid Tumors 1.1. Toxicity was evaluated using the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.03. 2010. The main criteria for the analysis were the progression-free survival (PFS) and overall response rate (ORR). The secondary criteria were the disease control rate (DCR), toxicity, overall survival (OS), and OS rate at 12, 24, 36, 48, and 60 months. The treatment was discontinued if the disease progressed, if severe adverse events occurred, if combined treatment still did not relieve the symptoms, or when the patients disagreed on treatment. The endpoint for data analysis was May 2020.
Ethics approval and consent to participate
The study was approved by the ethics committee of the 108 Military Central Hospital, Vietnam at 2524/HĐĐĐ, 28 May 2019. All patients who participated in this study voluntarily provided their informed consent.
Statistical analysis
The Statistical Package for the Social Sciences software version 22.0 was used for all statistical computations. Differences were considered statistically significant when p < 0.05. Survival was calculated using Kaplan–Meier analysis.
Results
Clinical and paraclinical characteristics of the patients treated with gefitinib
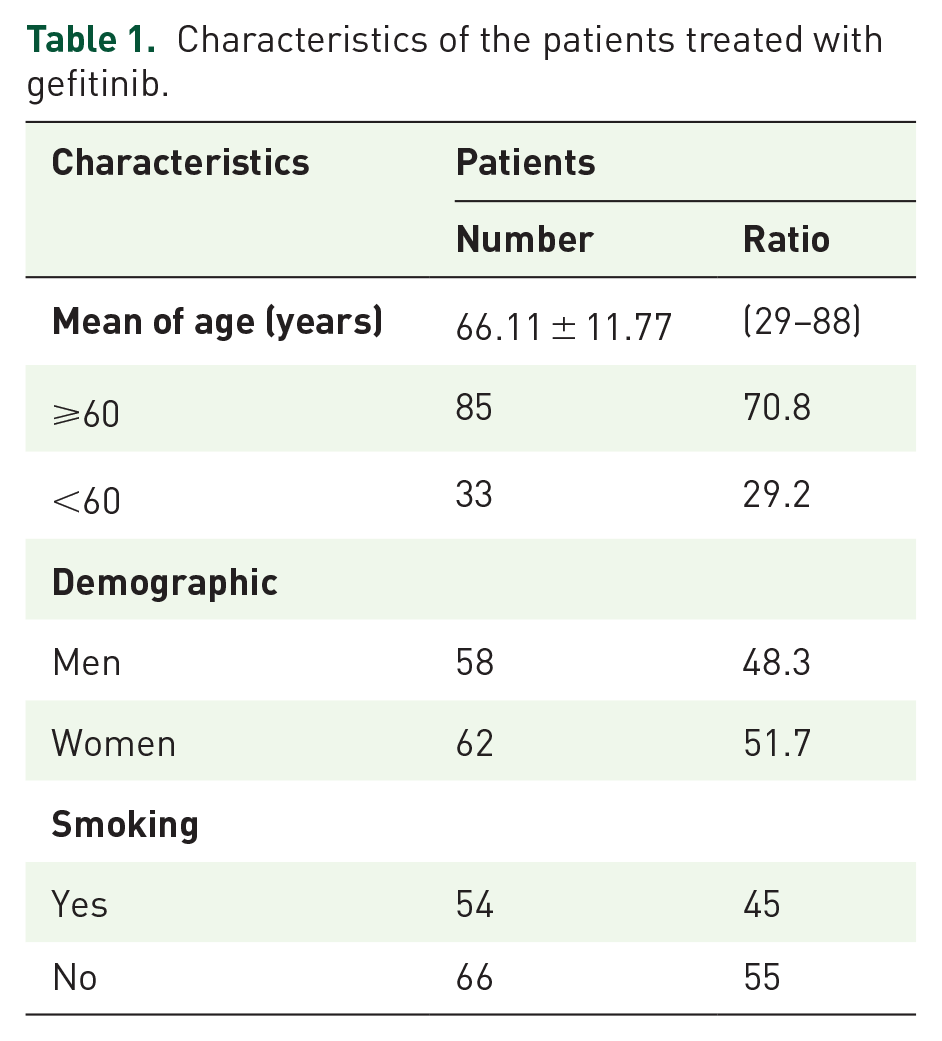
The median age of the patients treated with gefitinib in this study was 67.5 years and 11.7 months, with a maximum age of 88 and a minimum of 29 years. The men/women ratio was nearly 1/1. Most patients did not have a smoking history. The characteristics of the patients treated with gefitinib are detailed in Table 1.
Characteristics of the patients treated with gefitinib.
Effects of targeted therapy using gefitinib
The median follow-up time was 15.5 months, with a minimum of 3 months and a maximum of 63 months. In the third month, the ORR was 59.2% (complication rate and partial response rate were 2.5% and 56.7%, respectively), and the DCR was 95.8%.
The median PFS was 14.5 ± 0.86 months [confidence interval (CI) 95%:12.8–16.1] (Figure 1).
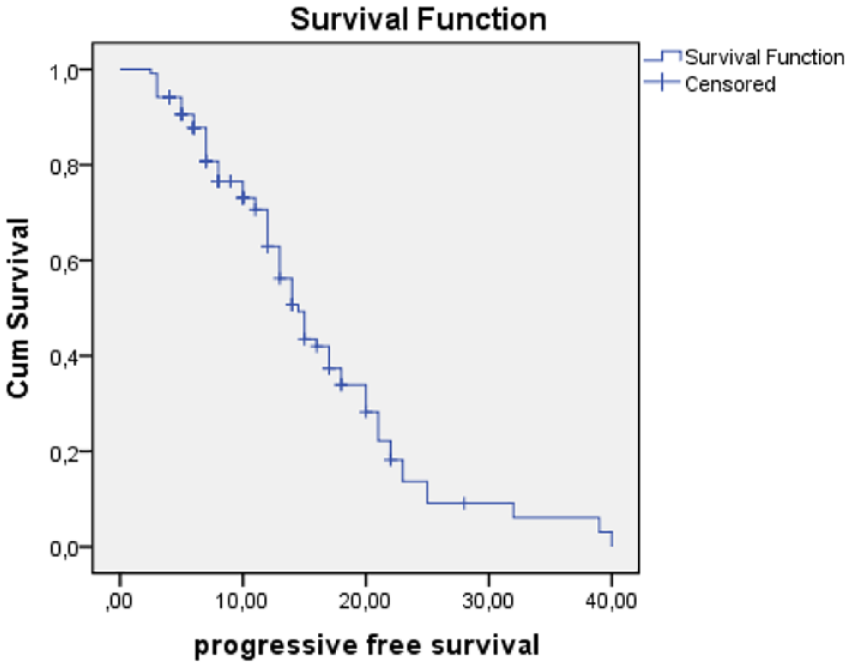
Progression-free survival.
The number of events was 26. The median OS was 33 months (95% confidence intervals [CI]: NR–NR).The OS rates at 12, 24, 36, 48, and 60 months were 63.3%, 25%, 5.8%, 2.5%, and 1.7%, respectively (Figure 2, Table 2).

Overall survival.
Overall survival rates.

OS, overall survival.
The median OS in women was longer than that in men, and the difference was statistically significant (p = 0.049). The median OS in non-smokers was longer than that in smokers, with a statistically significant difference (p = 0.025). However, there were no statistically significant differences in the PFS between patients with a good PS [Eastern Cooperative Oncology Group (ECOG) 0–2] and patients with a poor PS (ECOG 3–4) (p > 0.05). The OS of patients with a good PS was longer than that of patients with a poor PS, and the difference was statistically significant with p = 0.02 (Table 3, Figure 3).
Relationship of PFS and OS with some characteristics.

OS, overall survival; PFS, progression-free survival; PS, performance status.
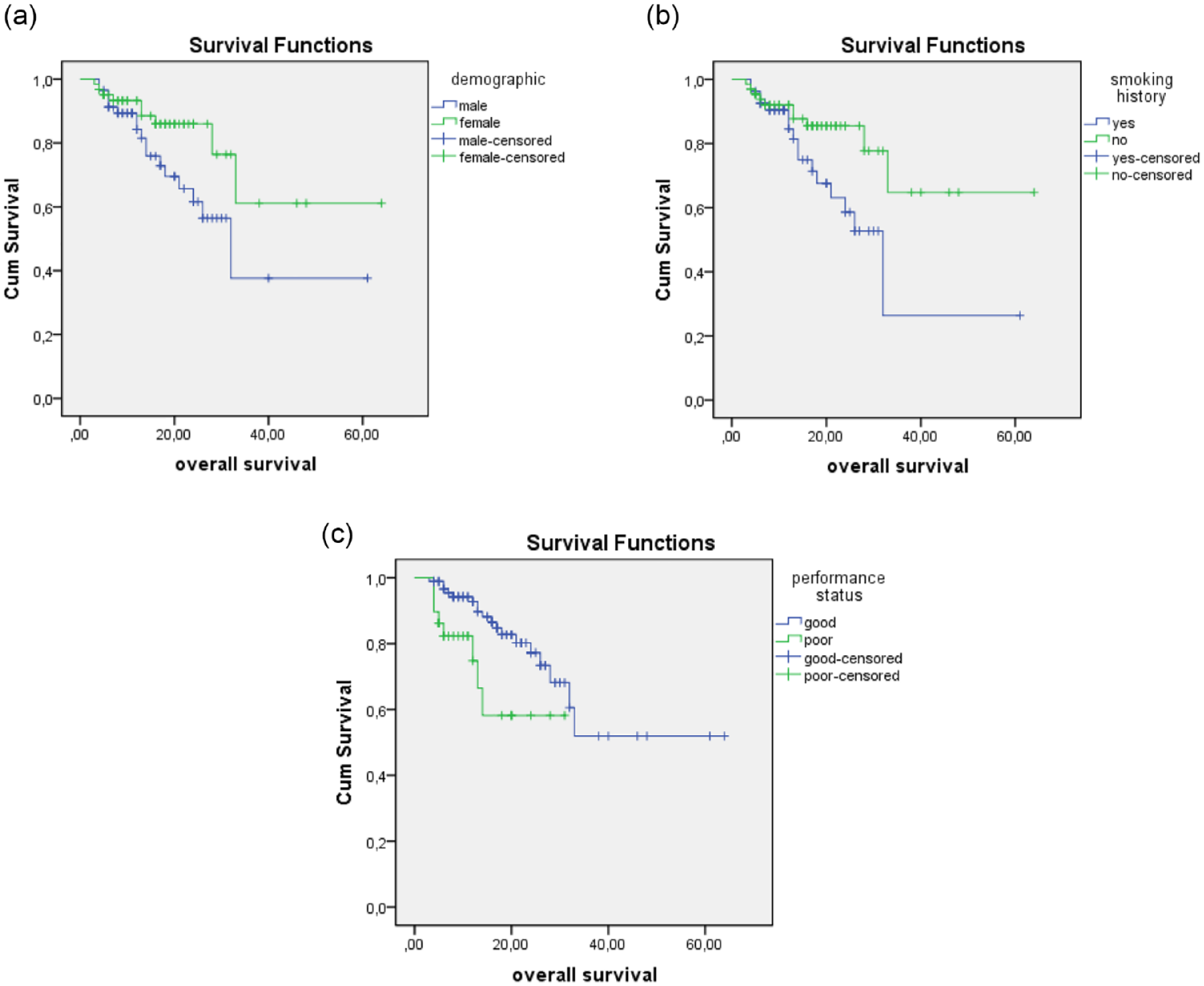
Relationship of overall survival (OS) with some patient characteristics. (a) OS and sex, (b) OS and smoking history, (c) OS and performance status (PS) of patients.
Toxicity was observed in 59.2% of the patients, the majority of which comprised rash and acne, accounting for 41.7%. However, these toxicities were commonly grade 1 and grade 2 toxicities. These adverse events were followed by other toxicities, such as paronychia, anorexia, and diarrhea. Two patients exhibited an increase in the transaminase level of grade 3 by 1.7%. No patients showed a reduction in the red blood cells, white blood cells, or platelets in the bone marrow. There were no data available on interstitial lung disease (ILD) due to gefitinib (Figure 4).

Adverse events.
Discussion
Researchers from around the world including from Vietnam have demonstrated that older age is one of the risk factors for lung cancer.8–10 In our study, the mean age of the patients was 66.11 years, with a maximum of 88 and a minimum of 29 years, and most patients were >60 years old (70.8%). Although the mean age in this study was similar to that in other studies, this study also shows the age rejuvenation of lung cancer patients. This rejuvenation has been explained by an increase in the smoking habit among young people. According to statistics, up to 85–90% of lung cancer patients have a history of smoking. Environmental pollution is also one of the factors that increases the risk of lung cancer. 8 In our study, there were more women (51.7%) than men, and the proportion of non-smokers (55%) was also higher than that of smokers (45%). Studies have shown that men and smokers have a higher incidence of lung cancer compared with women and non-smokers. However, in this study, we evaluated the effect of EGFR-TKI treatment on advanced NSCLC with EGFR mutations. Therefore, our results were consistent with those of previous studies, in which EGFR mutations were more common in women and non-smokers.1,8
The efficacy of EGFR-TKIs in patients with NSCLC harboring EGFR mutations has been confirmed through multicenter clinical trials and included in the practical guidelines for the treatment of NSCLC.2–7 In Vietnam, first-generation, second-generation, and third-generation EGFR-TKIs are all used for the treatment of patients with advanced NSCLC; however, the first-generation TKIs (gefitinib and erlotinib) are most commonly used. In this study, we evaluated the efficacy of gefitinib as a first-line therapy in 120 patients with advanced NSCLC, with a median follow-up time of 15.5 months. In the third month, the DCR and ORR of patients were 95.8% and 59.2%, respectively. The IPASS study is a well-known, multicenter, phase III trial on the treatment of advanced NSCLC with gefitinib as the first-line therapy compared with standard chemotherapy. The trial results showed a significantly higher ORR of 71.2% in the targeted therapy group than in the control group. 2 Another trial was the NEJ002, a multicenter phase III study conducted in Japan from March 2006 to May 2009. 3 The results revealed that the ORR in the targeted therapy group was significantly higher (73.7%). These ORR results were higher than those observed in our study.
In terms of monitoring and evaluating the response of patients who were treated with TKIs, clinical trials of gefitinib have been conducted at intervals of 6 to 8 weeks, and have demonstrated that the PFS in patients using targeted therapy were 9.8 months and 10.8 months in the IPASS and NEJ002 trials, respectively.2,3 In the FLAURA study, which compared the efficacy of osimertinib with first-generation TKIs in patients with advanced NSCLC harboring EGFR mutations, the authors conducted a separate analysis of Japanese patients to examine the effectiveness of gefitinib compared with osimertinib. 11 The median PFS in the gefitinib group was 13.8 months, which was higher than that in previous clinical trials. In our study, the median PFS was 14.5 months, and the median OS was 33 months. The OS rates at 12, 24, 36, 48, and 60 months were 63.3%, 25%, 5.8%, 2.5%, and 1.7%, respectively. The PFS rate that indicated the effectiveness of gefitinib in our study was higher than those of other studies; however, similar OS and 5-year survival rates were observed.2,3,8 Moreover, our results were significant compared with the results of a study by Douillard et al., in which the use of gefitinib as a first-line therapy in Caucasians resulted in a median OS of 19.2 months. 12 In real-world data from Taiwan, the median PFS and OS were 11.9 months and 26.9 months, respectively. 13 The differences in PFS can be explained by the fact that the time interval for treatment evaluation in this study was usually 3 months or less, depending on whether the patients had symptoms of progressive disease. Thus, there may be a time difference between the actual PFS interval and the evidence of progressive disease upon diagnosis. However, Kaplan–Meier curve analysis revealed that up to 40% patients had a PFS of 15 months, which may also be responsible for our median PFS being longer than that in other studies.
In this study, we also analyzed the relationship between PFS and OS with respect to clinical and paraclinical factors such as sex, smoking history, and PS of patients, which has rarely been mentioned in previous studies, especially the PS of patients. The results demonstrated that compared with men and smokers, the OS was significantly longer in women and non-smoking patients (p < 0.05). These results indicate that women and non-smoking patients may have a higher EGFR mutation rate, and they are both good prognostic factors for OS if treated with TKIs. Comparing the PFS and OS between patients with a good PS (ECOG 0–2) and poor PS (ECOG 3–4) revealed that gefitinib therapy in patients with advanced NSCLC with a poor PS was not different from that in patients with a good PS with respect to the median PFS. Meanwhile, in patients with a good PS, the OS was significantly longer than that in patients with a poor PS (p < 0.05). Therefore, targeted therapy with gefitinib is an appropriate option for patients with advanced NSCLC with EGFR mutations, even in patients with a poor PS. In a retrospective study of 1,660 Japanese patients with advanced NSCLC with EGFR mutations who responded to EGFR-TKIs, Inoue et al. showed that sex, age, histology, EGFR mutation type, clinical stage, and PS affected the OS. 10
Another concern about targeted therapy in patients with NSCLC who are positive for EGFR mutations is the occurrence of adverse events. The common side effects in patients treated with EGFR-TKIs are rash and acne, paronychia, anorexia, diarrhea, increasing transaminase levels, interstitial pneumonia, and leukopenia. Depending on the generation of TKIs, studies have shown a different incidence of each type of adverse event.2–7 In total, 59.2% patients exhibited adverse events in our study, majority of which were rash and acne (41.7%), and were mostly grade 1 and grade 2 events. This was followed by the occurrence of paronychia (21.7%) and anorexia (15.0%). The percentages of patients with diarrhea and increase in transaminase levels were 9.2% and 3.3%, respectively. Two patients had grade 3 transaminase levels; therefore, they discontinued gefitinib and switched to treatment with other TKIs. All these adverse events resolved on their own or after medical treatment. Reduction in the red blood cells, white blood cells, and platelets in the bone marrow was not observed in any patient. We also do not have data on ILD related to gefitinib. Overall, our results are similar to the observations of other studies on toxicity and grade after treatment with gefitinib.2–7,10
This is the first study on the use of gefitinib as a first-line treatment in Vietnamese patients with advanced NSCLC harboring EGFR mutations, and showed the benefits both in terms of PFS and OS in this patient population. In particular, our research has revealed that there is no difference in the PFS benefit between patients with a poor PS and good PS when treated with gefitinib.
The limitations of this study are that it had a limited number of patients and it was conducted in a single center. We plan to continue treatment and follow-up, as well as an analysis of a larger number of patients, including patients with brain metastases.
Conclusions
Gefitinib is an effective first-line treatment in Vietnamese patients with advanced NSCLC who are positive for EGFR mutations regardless of whether the patients have a good PS or not. In particular, targeted therapy with gefitinib provides the benefit of OS in women and non-smokers. However, the number of patients in this study is still limited, and further research is required for an in-depth analysis of patients with brain metastases.
Footnotes
Authors’ contributions
-PVL, Medical Doctor in the Department of Respiratory Medicine, 108 Military Central Hospital, Vietnam: formal analysis, principal investigation, methodology, resources, writing original draft, review, and editing.
-NDT, Associate Professor, Head of Department of Respiratory Medicine, 108 Military Central Hospital, Vietnam: Research member, formal analysis, and methodology.
-NMH, PhD, Vice Head of Department of Respiratory Medicine, 108 Military Central Hospital, Vietnam: Research member and provided resources.
-NDaoT, PhD, Vice Head of Department of Respiratory Medicine, 108 Military Central Hospital, Vietnam: Research member and provided resources.
-TTD, Medical Doctor in the Department of Respiratory Medicine, 108 Military Central Hospital, Vietnam: Research member and provided resources.
All authors have read and approved the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The study was approved by the ethics committee of the 108 Military Central Hospital, Vietnam. All patients who participated in this study voluntarily provided their consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.