
Abstract
Hereditary diffuse gastric cancer (HDGC) is a rare malignancy characterized by autosomal dominant inheritance of pathological variants of the CDH1 gene encoding E-cadherin, which is involved in cell–cell adhesion, maintenance of epithelial architecture, tumor suppression, and regulation of intracellular signaling pathways. Late-stage recognition of HDGC is typically associated with a poor clinical outcome due to its metastatic potential and risk of lobular breast cancer (LBC) development. The American College of Gastroenterology issued guidelines to evaluate HDGC, test for CDH1 genetic variants, and recommend prophylactic gastrectomy for carriers of CDH1 mutations. If surgery is not pursued, endoscopy is a surveillance alternative, although it carries a limited ability to detect malignant foci. As part of clinical research efforts, novel endoscopy advances are currently studied, and a center of excellence for HDGC was created for a comprehensive multidisciplinary team approach. Within this review, we cover current conventional treatment modalities such as gastrectomy and chemotherapy, as the mainstay treatments, in addition to Pembrolizumab, an immune checkpoint inhibitor, as the last therapeutic resort. We also shed light on novel and promising approaches with emphasis on immunotherapy to treat HDGC. We further break down the therapeutic paradigms to utilize molecular tools, antibodies against checkpoint inhibitors, TGF-β and tyrosine kinase inhibitors, cell-based adoptive therapies, and oncolytic viral therapies. We aim to expand the understanding on how to modulate the tumor microenvironment to tip the balance towards an anti-tumor phenotype, prevent metastasis of the primary disease, and potentially alter the therapeutic landscape for HDGC.
Overview of HDGC
Gastric malignancy is the third leading cause of cancer mortality worldwide and ranks as the fifth most frequently diagnosed cancer since it accounted for 1 million new cancer cases in 2018. 1 Gastric cancer is a heterogeneous entity attributed to multiple environmental and genetic factors and is divided into either sporadic (90% of cases) or familial (10%), 1 as well as intestinal (well-differentiated) or diffuse (undifferentiated). 2 Hereditary diffuse gastric cancer (HDGC) – a form of diffuse familial aggressive gastric cancer – constitutes 1–3% of gastric cancer cases and is inherited in an autosomal dominant fashion. 3
On a molecular basis, HDGC is linked to pathogenic variants of the CDH1 gene encoding E-cadherin, located on chromosome 16q22. E-cadherin is a pleiotropic protein involved in cell–cell adhesion, maintenance of epithelial architecture, tumor suppression, cell polarity, and regulation of intracellular signaling pathways. 4 CDH1 mutations that are manifested in a decrease of E-cadherin expression were first described in 1998 in New Zealand in three Maori families. 5 Since then, research findings have reported more than 120 different pathogenic variants of CDH1 associated with HDGC, which is characterized by signet ring cells. 6 Furthermore, multiple genes such as CTNNA1, BRCA2, and MAP3K6 are currently under intense research focus to explore their roles and implications in the pathogenesis of HDGC.7,8 STK11 and PALB2 have also been detected in families meeting HDGC criteria. 7 Investigating the association of these new candidate genes with HDGC will enhance our understanding of the underlying genetic causes of this disease.
In carriers of CDH1 mutations, the lifetime risk of HDGC in both men and women by the age of 80 years is 80%, while that of lobular cancer is 60%. 9 The combined risk of lobular breast cancer (LBC) and HDGC is higher, and estimated at 90% by the age of 80 years. 10 Taking into account the high penetrance of CDH1 mutations, genetic counseling and surveillance are imperative.
Clinical management of HDGC
The American College of Gastroenterology (ACG) has issued guidelines and criteria to evaluate and manage HDGC and test for CDH1 carriers (Table 1). 11
Indications for genetic evaluation for HDGC in affected families according to ACG clinical guidelines.

ACG, American College of Gastroenterology; GC, gastric cancer; HDGC, hereditary diffuse gastric cancer; LBC, lobular breast cancer.
In the light of the close association between LBC and HDGC, some have proposed a nomenclature change for HDGC into a broad designation of the syndrome of hereditary gastric and LBC. 12 ACG clinical guidelines also recommends breast cancer screening for women with HDGC through annual mammography and semiannual breast MRI and breast examination starting at age of 35 years. 11 Colonoscopy in families with colon cancer is also recommended starting at the age of 40 years. In complementation to the ACG guidelines, the International Gastric Cancer Linkage Consortium (IGCLC) has recently devised updated guidelines for HDGC as well. 13
Prophylactic gastrectomy is recommended for carriers of CDH1 mutation secondary to the aforementioned elevated lifetime risk of HDGC.11,14 Since the mean age of diagnosis is between 38 and 40 years, the timing of surgery is optimal either at the age range of 20–30 years or at the age of 5 years younger than the youngest affected family member.11,14,15 The importance of this prophylactic approach is manifested in that 87% of patients with CDH1 mutations who underwent prophylactic gastrectomy had histology findings of malignancy, including 65% of specimens showing the characteristic signet rings. 16 Prior to operative intervention, upper endoscopy is recommended for the purpose of surgical planning. 14
Some patients elect to delay or not pursue the surgical intervention due to personal and psychological preferences. In that case, endoscopy can be used for surveillance at semiannual or annual intervals starting at the cut off of 5 years prior to the family’s earliest cancer diagnosis. 11 But the endoscopic approach is suboptimal because malignant foci are not visible on endoscopic evaluation due to the foci’s subepithelial and heterogeneous locations in the stomach.17,18 Thus, endoscopy findings can remain normal until late stages of the disease leading to a delay in the diagnosis and a very poor prognosis. In an attempt to improve the detection of malignant lesions, multiple alterations to endoscopy have been suggested, such as enhanced imaging as well as chromoendoscopy through the use of Congo red dye and pentagastrin.19,20 In addition, a detailed endoscopic evaluation spanning at least 30 min has been recommended, along with the use of high definition white light to obtain biopsies of visible lesions followed by multiple random biopsies.14,21 It remains prudent to counsel patients about the importance of prophylactic gastrectomy and emphasize the deficiencies and limited utility of the endoscopic approach.
Clinical advances are improving the diagnostic outcome of HDGC. A clinical trial examining the use of confocal endoscopic microscopy with the aim of improving the sensitivity of early SRC detection in HDGC is underway and is currently in phase II of a clinical trial [ClinicalTrials.gov identifier: NCT03648879] (Table 2). Moreover, as part of the increased efforts focused on improving the quality of medical care and research on HDGC, a center of excellence for HDGC was established. 22 In this model of an integrated multidisciplinary team, the center aims at a comprehensive approach for HDGC through the evaluation and input of multiple specialists including surgeons, gastroenterologists, oncologists, pathologists, pharmacists, genetic counselors, and dietitians. Such diverse team is of paramount importance for the effective and focused treatment and planning of such a rare disease and genetic counseling for affected families.
Completed and ongoing clinical trials focusing on HDGC for the past 4 years.
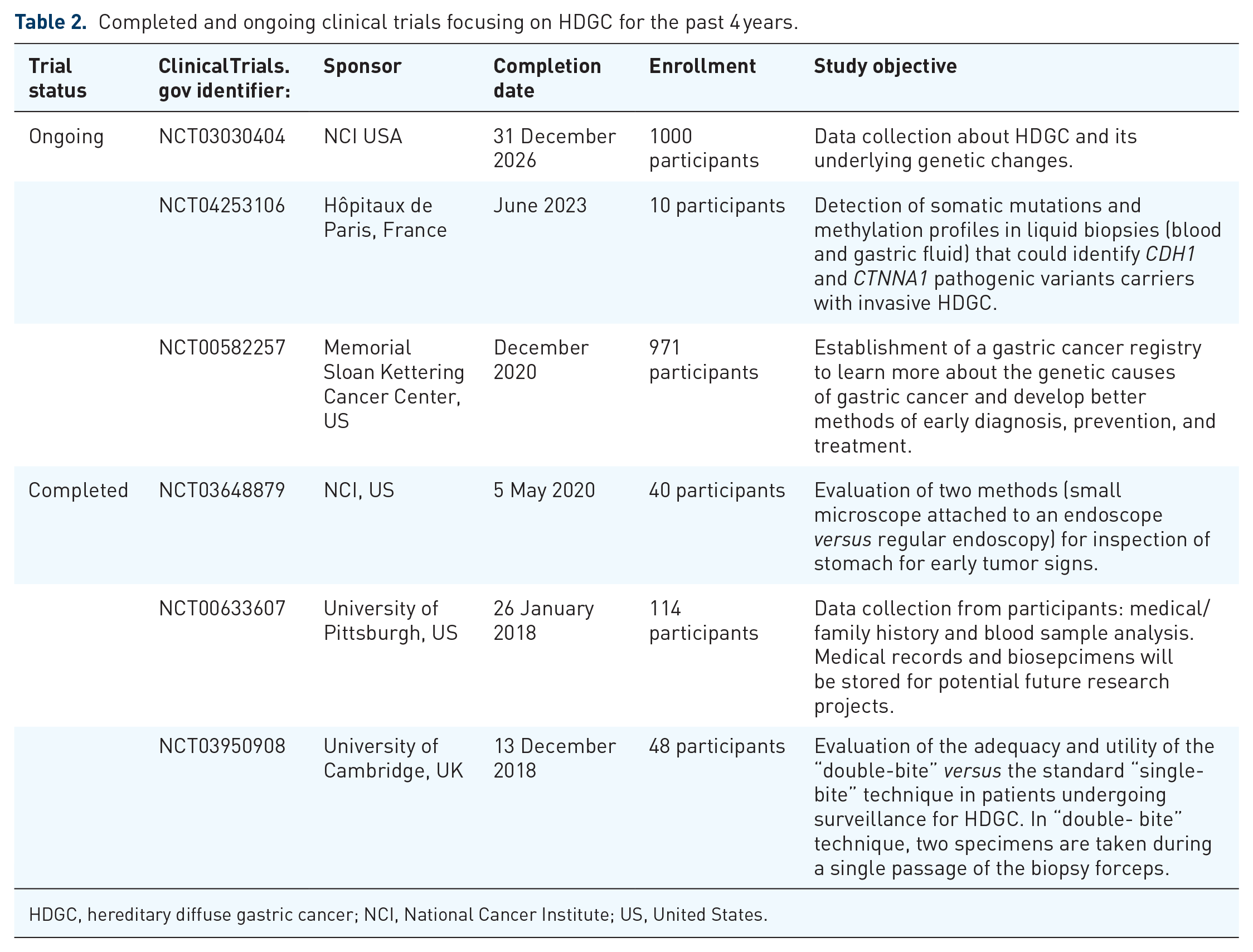
HDGC, hereditary diffuse gastric cancer; NCI, National Cancer Institute; US, United States.
Current therapeutic approaches
Surgery
In addition to the prophylactic gastrectomy approach mentioned earlier, gastrectomy is the mainstay treatment to reduce tumor development and metastasis (Figure 1). Minimally invasive gastrectomy is associated with a faster recovery and reduction in post-operative pain and hospital length of stay. Laparoscopic-assisted gastrectomy was first described in 1994, and, since then, it has become the established treatment for early and advanced HDGC. 23 Robotic-assisted gastrectomy was first reported in 2002, and gained traction in Asia due to its enhanced operative precision and improved clinical outcomes. 24 Although no clinical trials have compared robotic gastrectomy with either laparoscopic or any equivalent, the premise is that robotic-assisted gastrectomy is expected to deliver the same benefits due to three-dimensional (3D) vision, reduction in intra-operative blood loss, high magnification, stable optical platform, and tremor reduction technology, which is potentially superior to established minimally invasive methods.
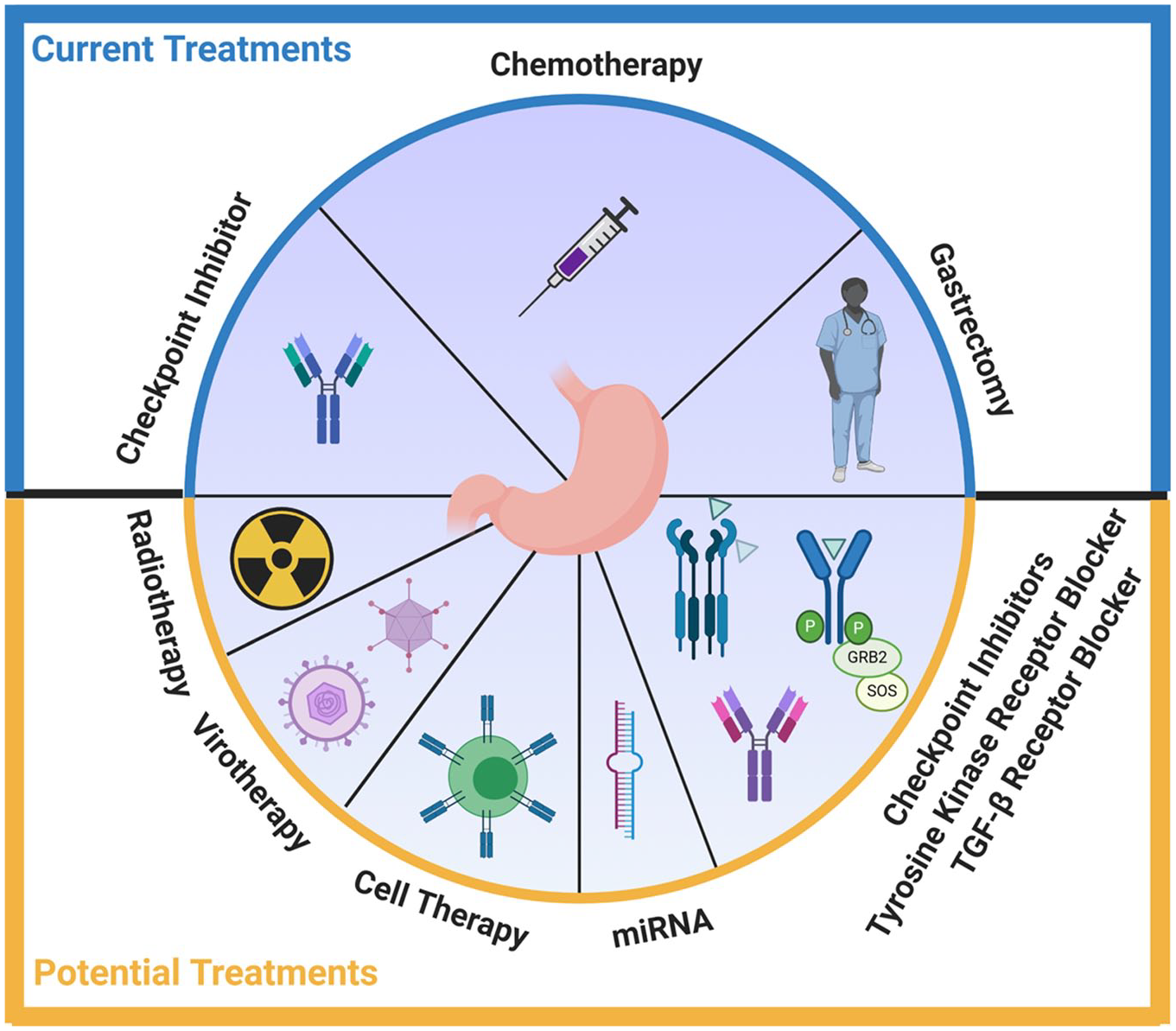
Current (highlighted in blue) and potential (highlighted in yellow) treatments for HDGC.
Chemotherapy
When HDGC metastasizes, a systemic treatment is recommended after mandatory testing for the expression of human epidermal growth factor receptor-2 (HER-2). Patients overexpressing HER-2 have trastuzumab (monoclonal antibody directed against HER-2) added to chemotherapeutic agent(s). 25 Although there is no single standard chemotherapeutic protocol that is followed worldwide, a commonly used first-line treatment combines platinum and fluoropyrimidine doublet, such as FOLFOX, CAPOX, cisplatin/5-fluorouracil (5-FU), or cisplatin/capecitabine (Figure 1).26,27
Chemotherapy has been shown to enhance survival by around 7 months as compared with palliative care. 28 Moreover, first-line combination chemotherapy improves survival by 1 month in comparison with 5-FU alone. 28 Selecting any drug combination for chemotherapy is challenging and requires close attention to the toxicity profile of drug(s), tumor burden, and patient response. 29
Immunotherapy
Anti-programmed cell death 1 (PD1) antibodies are immune checkpoint inhibitors that block the inhibitory axis between the checkpoint ligands [programmed cell death ligand 1 (PD-L1)] on tumor cells and their cognate receptors (PD-1) on the effector cells, unleashing a potent anti-tumor response. Currently Pembrolizumab is the only approved anti-PD1 antibody for the treatment of patients with advanced, recurrent, or metastatic gastric cancers that have either microsatellite instability-high (MSI-H), DNA mismatch repair deficient (dMMR), or at least 1% expression of PD-L1 after failing at least two lines of systemic therapy (Figure 1).30,31 No genetically engineered cell-based immunotherapeutic approach is currently approved for treatment of HDGC.
Proposed treatment targets and future directions
Molecular approach
The mature E-cadherin protein contains a single transmembrane domain, a cytoplasmic domain, and an extracellular domain (EC1–EC5) that contains N-glycosylation sites. 32 The intracellular portion of E-cadherin orchestrates with catenin subunits to bind to cytoplasmic actin and enforce intra-cellular adhesion. When E-cadherin cDNA was introduced into fibroblasts lacking this protein, the cells started aggregating and forming tightly connected colonies. 33 Hence viral and non-viral methods for efficient delivery of full E-cadherin gene to cells with mutated gene versions can be explored.34,35 Another gene candidate to screen for and modulate as a therapeutic target candidate is CTNNA1 in a sub-population of HDGC patients. CTNNA1 codes for α-catenin that clusters with β-catenin in the cytoplasm and bridges E-cadherin to the actin cytoskeleton of cancer cells.8,36 It is important to note that aberrations in E-cadherin expression do not depend solely on gene mutations and epigenetic alterations. Successful post-translational glycosylation is necessary for transporting E-cadherin to the cell surface. 32 For example, N-acetylglucosaminyltransferase III (GnT-III) is an enzyme needed to add bisecting GlcNAc structure in N-glycans of E-cadherin, which helps suppress metastasis. On the other hand, GnT-V is a competing enzyme that mediates the addition of β1,6 GlcNAc branching of N-glycans, which, in turn has been shown to increase metastasis. 37 Other molecular approaches that may control E-cadherin-related metastasis include the use of microRNA (miR-200) family members to suppress ZEB1 and ZEB2 transcription factors. The latter factors are markers of the epithelial to mesenchymal transition (EMT) induced by TGF-β, and act as repressors to E-cadherin transcription.38,39 However, further investigation is warranted to study the safety, stability, and dosing of such miRNAs for clinical use.
Another rare occurrence in HDGC families is nonsense-mutated CDH1 (around 20% of cases), that leads to premature and short E-cadherin protein production. One way to fix this aberration, at least in vitro, is by using suppressor-tRNA. These sup-tRNAs are capable of introducing a specific amino acid in premature stop codons to allow for a complete translation and generation of full-length E-cadherin protein. 40
Antibody approach targeting tyrosine kinase receptors
Early attempts to develop specific antibodies that target HDGC were mostly unsuccessful due to the lack of an identified tumor-specific antigen(s). Others have found that certain self-molecules are overexpressed in this type of cancer such as EGFRvIII and could be targeted by tyrosine kinase (TK) inhibitors.41,42 The epidermal growth factor receptor (EGFR) is a member of the ERBB transmembrane growth factor receptor family, and humanized monoclonal antibodies such as cetuximab, panitumumab, and matuzumab have been studied as potential inhibitors. 43 In addition, gastric cancer tumors, including HDGC, recruit vascular endothelial growth factor (VEGF) for angiogenesis and promoting metastasis. The anti-VEGF antibody, bevacizumab was used in combination with chemotherapy agents (capecitabine and cisplatin) in the phase III AVAGAST clinical trial [ClinicalTrials.gov identifier: NCT00548548]. Improved median survival and a significant progression-free survival was observed with bevacizumab versus placebo (6.7 versus 5.3 months, p = 0.0037). 44 Another member of TK family is MET that binds to hepatocyte growth factor (HGF) and initiates a cascade of signaling involving Ras, PI3K, mTOR, STAT3, and NF-κB in tumor cells. 43 Rilotumumab is a human monoclonal antibody developed to target HGF and limit metastasis; however, this drug showed efficacy only in patients with high MET profile. 45
Antibody approach targeting checkpoints
Explaining the current therapies for gastric cancer as a whole, will pave the therapeutic road for HDGC, while keeping in mind each disease’s unique characteristics. Multiple immune checkpoint inhibitors are currently investigated in clinical trials against gastric cancers (Figure 1): Atezolizumab [ClinicalTrials.gov identifier: NCT03421288], Avelumab (JAVELIN Solid Tumor study), Camrelizumab [ClinicalTrials.gov identifier: NCT03472365], and Durvalumab (MEDI4736) [ClinicalTrials.gov identifier: NCT02340975] are antibodies against PD-L1 expressed on gastric tumor cells; Nivolumab (ATTRACTION-2 [ClinicalTrials.gov identifier: NCT02267343] and CheckMate-032 [ClinicalTrials.gov identifier: NCT01928394], MOONLIGHT, CA224-060, CheckMate-577, CheckMate-648, and CheckMate-649), and Tislelizumab (BGB A317) [ClinicalTrials.gov identifier: NCT03469557] are antibodies directed against PD-1 expressed on immune effector cells; Tremelimumab [ClinicalTrials.gov identifiers: NCT03751761, NCT03959293, NCT02658214] is a CTLA-4 inhibitor; INCAGN02390 [ClinicalTrials.gov identifier: NCT03652077] is an anti-TIM-3 antibody; Relatlimab (Anti-LAG-3) is involved in two clinical trials [ClinicalTrials.gov identifiers: NCT03044613, NCT03704077] against gastric cancer, while INCAGN02385 is another anti-LAG-3 antibody involved in a clinical trial: [ClinicalTrials.gov identifier: NCT03538028]. Of special significance are bi-specific antibodies directed against dual antigens and clinically tested against cancer tumors: XmAb22841 targets immune checkpoint receptors CTLA-4 and LAG-3 [ClinicalTrials.gov identifier: NCT03849469]; MGD013 is an anti-PD-1, anti-LAG-3 dual checkpoint inhibitor [ClinicalTrials.gov identifier: NCT04082364]; MGD013 binds PD-1 and LAG-3 [ClinicalTrials.gov identifier: NCT03219268]. Finally, M7824 was developed as a fusion protein, combining human anti-PD-L1 antibody with two extracellular domains of transforming growth factor-beta (TGF-β receptor II [ClinicalTrials.gov identifier: NCT02699515]). Further details are provided in detailed reviews.46,47
Antibody approach targeting tumor-promoting cytokines
TGF-β has been involved in tumor cell proliferation, angiogenesis, EMT, gastric tumor migration and invasion.48,49 Combining antibodies directed against TGF-β and PD-L1 induced T cell infiltration into tumors, which resulted in tumor regression in a preclinical model of mammary carcinoma. 50 Several TGF-β [ClinicalTrials.gov identifiers: NCT03451773, NCT03954704] and TGF-β-receptor antagonists [ClinicalTrials.gov identifier: NCT02452008] are in clinical trials against solid tumors and can be potentially tested against HDGC. The IL-6 cytokine is another soluble factor secreted chronically in the tumor milieu that contributes to tumor progression. 51 Therefore, agents designed to block this cytokine may potentially be utilized for the treatment of HDGC. Such agents include tocilizumab against IL-6 receptor and siltuximab directed against IL-6 itself. 52
Cellular approach
To date, the United States Food and Drug Administration (FDA) approved multiple cell therapies for liquid tumors against CD19/CD20. Numerous studies are under investigation for cell-therapy applications in solid tumors. However, little attention is given to rare cancers such as HDGC. In the light of the current discussion, scientists were recently able to identify an antigen called Claudin 18.2 as a target for antibody therapy in gastric cancer (Zolbetuximab Claudin 18.2 inhibition: FAST TRIAL). 53 Another membrane protein involved in cell adhesion, CD24, was shown to bolster progression of gastric cancer through increasing tumor cell proliferation and regulating EGFR internalization and signaling.54,55 CD24 is an attractive prognostic factor for HDGC. 56 These extracellular targets could be utilized to design chimeric antigen receptor T (CAR-T) cells, or T-cells with engineered TCR, and CAR-NK cell-based therapies. Other potential gastric cancer antigen targets include survivin and MG7.57,58 Next generation CAR-T cells now incorporate costimulatory molecules such as 4-1BB and OX40 to prolong persistence and effector functions. Some CAR-T strategies also use CRISPR technology to delete unwanted exhaustion markers such as PD-1.59,60 Others have incorporated safety switches within their construct design that can be activated with molecules such as rapamycin to induce the suicide of CAR-T and prevent graft-versus-host-disease (GVHD) toxicity. 61 Addition of the IL-12 inflammatory cytokine has also proven efficacious in reversing the tumor microenvironment (TME) to Th1 anti-tumor phenotype. 62 Autologous or off-the-shelf CAR-NK therapy on the other hand resulted in a lower toxicity profile and generated potent killer activity, especially with the addition of IL-15 and/or IL-2 cytokines. 63
In order for cell therapies to work efficiently and infiltrate tumors, combinatorial strategies are needed to modulate the TME and overcome the inhibitory stroma. The latter is a matrix imbedding inhibitory cells such as Tregs, myeloid derived suppressor cells (MDSCs), M2 macrophages, and cancer-associated fibroblasts. Gastric cancers in particular have been shown to harbor high levels of Th17 T-cells and Tregs. Th17 cells produce IL-17 and contribute to chronic inflammation, while Tregs produce excessive TGF-β and promote tumor progression. 64 Therefore, a combination treatment of IL-17 or anti-CTLA-4 blockade along with optimized cell therapy may boost systemic anti-tumor responses and improve clinical outcomes. Other studies also aimed at suppressing MDSCs by using Indoleamine 2,3-dioxygenase 1 (IDO-1) inhibitors. 65
Another future direction could be to implement radiotherapy (RT) prior to gastrectomy to release neoantigens and prime T-cells (Figure 1). The addition of RT after surgery and palliative chemo did not result in significant survival benefit for HDGC patients. 43 However, optimal sequencing of RT prior to surgical resection may confer an immune-mediated systemic protection. The nucleic acid released upon RT damage of tumors activates the cGAS/STING pathway that ultimately leads to the production of type I interferons and upregulation of MHC-I molecules.66,67 To maximize the availability of cytoplasmic DNA fragments, researchers are currently developing poly ADP ribose polymerase (PARP) inhibitors to block tumor DNA repair mechanisms and enhance immune priming. PARP inhibitors such as Olaparib, Fluzoparib, and Pamiparib are currently under clinical investigation [ClinicalTrials.gov identifiers: NCT01924533; NCT03026881; NCT03427814]. In conclusion, given the novel therapeutic approaches mentioned above, immunotherapy plus RT holds a promising potential for treating rare cancer types including HDGC, especially in metastatic cases.
Oncolytic virotherapy
Oncolytic viruses have emerged as effective therapeutic agents for cancer treatment. They are genetically engineered to selectively target and kill cancerous cells. In the process, they augment anti-tumor responses and hence they have been administered with immune checkpoint inhibitors to switch immunologically cold tumors into hot ones with proinflammatory microenvironments. 68 Multiple ongoing clinical trials are testing different viral vectors along with pembrolizumab [ClinicalTrials.gov identifiers: NCT03069378, NCT04068181, NCT02965716, NCT03842943, NCT02509507, NCT02798406, NCT03003676], the only approved immune checkpoint inhibitor against gastric cancers. Interestingly, some virotherapeutic approaches, in combination with pembrolizumab, are investigating intravenous and intramuscular delivery routes of oncolytic viruses [ClinicalTrials.gov identifier: NCT03773744, NCT02879760] to solid tumors. If these trials are proven successful, systemic delivery of oncolytic viruses may be tested against immunologically cold and metastatic tumor models such as HDGC (Figure 1).
Conclusions and perspectives
Multiple pathogenic variants of CDH1 germline mutations have been associated with HDGC and further research is uncovering a panel of susceptibility genes contributing to HDGC. On the clinical side, endoscopic surveillance and prophylactic/therapeutic gastrectomy are the mainstay approach to curb the development of HDGC. Unfortunately, late diagnosis of HDGC unfolds a pessimistic clinical outcome. Chemotherapy and Pembrolizumab are currently the only FDA-approved treatments. Ongoing clinical trials and research encompassing molecular, immune-cell, and antibody-based approaches have the potential to deliver safer and more efficacious treatment modalities for HDGC patients in the foreseeable future.
Footnotes
Acknowledgements
The authors would like to thank Rachael El Rami and Chen KueiHua Liu for critically reading and commenting on the manuscript.
Author contributions
FEE, HBB, and GWK conceived, wrote, and reviewed the figures, tables, and the manuscript. All authors approved the final draft of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.