
Abstract
Over the past 20 years, management of patients with metastatic colorectal cancer (mCRC) has improved considerably, leading to increased overall survival and more patients eligible for third- or later-line therapy. Currently, two oral therapies are recommended in the third-line treatment of mCRC, regorafenib and trifluridine/tipiracil. Selecting the most appropriate treatment in the third-line setting poses different challenges compared with treatment selection at earlier stages. Therefore, it is important for physicians to understand and differentiate between available treatment options and to communicate the benefits and challenges of these to patients. In this narrative review, practical information on regorafenib is provided to aid physicians in their decision-making and patient communications in daily practice. We discuss the importance of appropriate patient selection and adverse events management through close patient monitoring and dose adjustments to ensure patients stay on treatment for longer and receive as much benefit as possible. We also highlight key physician–patient communication points to facilitate shared decision-making.
Introduction
The management of patients with metastatic colorectal cancer (mCRC) has improved considerably over the past 20 years, and the median overall survival (OS) from the start of systemic therapy is now approximately 30 months.1,2 Choosing the optimal first-line treatment, tailored to the clinical characteristics of the patient and molecular features of the tumors, is an essential step in achieving disease control and facilitating subsequent treatment. 3 First-line treatment typically consists of chemotherapy with oxaliplatin-containing or irinotecan-containing regimens in combination with an anti-epidermal growth factor receptor (anti-EGFR) antibody (only in patients with RAS wild-type tumors) or an angiogenesis inhibitor. 1 Other key factors contributing to improvements in survival are availability and access to subsequent lines of therapy. To increase the likelihood of survival, it is important that patients are given the opportunity to receive all available treatment options as part of the ‘continuum of care’. 1
In addition to appropriate and effective systemic treatment, local treatment of metastases is increasingly important, especially in the oligometastatic setting, emphasizing the need for a multidisciplinary approach. Local treatment can include metastasectomy, thermal ablation, radioembolization, or stereotactic radiotherapy for some metastases (e.g. liver, lung, and spine metastases, and peritoneal carcinomatosis).4,5
As OS increases, more patients become eligible for third- or later-line therapy [classically after progression or intolerance to standard therapies: fluoropyrimidine, oxaliplatin, irinotecan, bevacizumab, and an anti-EGFR antibody (in case of RAS wild-type tumors)].1,6 Therefore, it is important for physicians to understand and differentiate between available treatment options and to communicate the benefits and challenges of these to patients. The issues faced by physicians and patients when selecting treatment in third line differ from those at earlier stages: the expectations of treatment shift from objective response to disease control (tumor response or stabilization), while patient preference, tolerability, and quality of life (QoL) become more important. 6 Two options recommended in current guidelines for third-line treatment are regorafenib and trifluridine/tipiracil (TAS-102), which are both oral therapies 1 ; therefore, patients can continue active treatment without the disadvantages associated with intravenous chemotherapy. Nevertheless, the transition from intravenous to oral therapies creates other challenges, including patient responsibility for medication adherence and monitoring, and the need for frequent communication with healthcare professionals to pre-empt and manage toxicity.
This narrative review provides expert opinion on treatment with regorafenib and patient management to aid physicians in their decision-making and communications with patients in daily clinical practice.
Regorafenib activity
Regorafenib is an oral tyrosine kinase inhibitor targeting angiogenesis, the tumor microenvironment, and tumor immunity,7,8 and is approved for the treatment of mCRC after progression on standard therapies.9,10 Regorafenib is also approved for third-line use in locally advanced, unresectable, or metastatic gastrointestinal stromal tumors and for second-line use in hepatocellular carcinoma.9,10 Regorafenib has also shown activity in phase II trials in chemotherapy-refractory biliary tract adenocarcinoma, 11 advanced non-adipocytic soft-tissue sarcomas, 12 progressive metastatic osteosarcoma,13,14 and relapsed glioblastoma. 15
Approval in mCRC was based on results of the pivotal phase III CORRECT trial, which demonstrated significantly longer OS with regorafenib compared with placebo in patients who had progressed after all approved standard therapies 16 ; these results were confirmed in the phase III CONCUR trial in Asian patients. 17 Meta-analysis of the data from these two studies showed a significantly longer OS and progression-free survival (PFS) with regorafenib compared with placebo and best supportive care [hazard ratios (HRs) 0.67 and 0.40, respectively]. 18 Regorafenib is recommended as third-line therapy in the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology guidelines1,19; NCCN guidelines also recommend that either regorafenib or trifluridine/tipiracil can be used as second-line therapy after FOLFOXIRI chemotherapy (5-fluorouracil, leucovorin, oxaliplatin, irinotecan). 19 Data from single-arm phase IIIb and real-world observational studies of regorafenib in over 3500 patients support the results observed in the randomized phase III trials (Table 1; REBECCA, 20 CONSIGN, 21 CORRELATE, 22 RECORA, 23 Japanese post-marketing surveillance study, 24 and the CORECT Czech Registry 25 ).
Efficacy of regorafenib across phase III clinical trials and real-world studies.
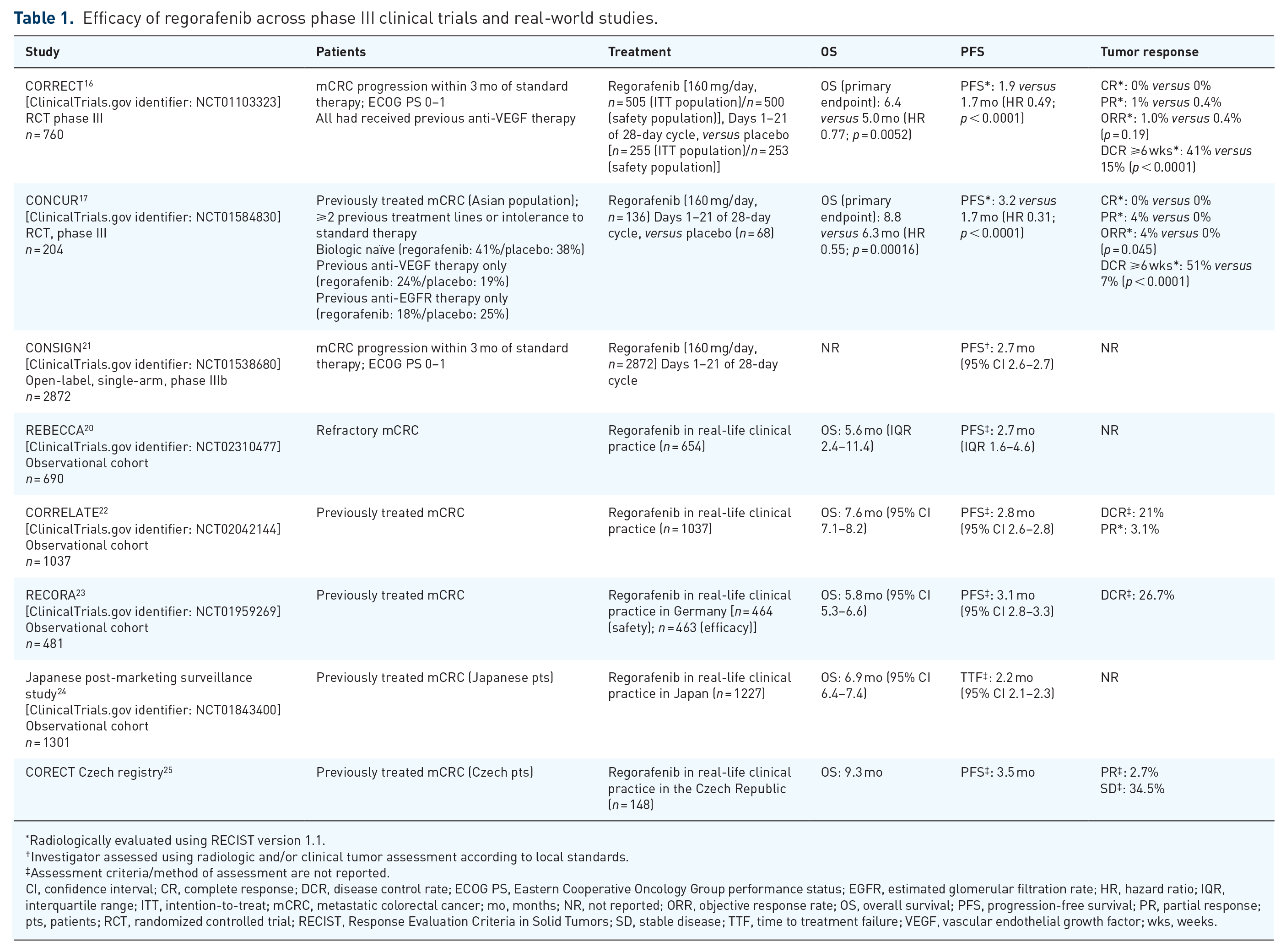
Radiologically evaluated using RECIST version 1.1.
Investigator assessed using radiologic and/or clinical tumor assessment according to local standards.
Assessment criteria/method of assessment are not reported.
CI, confidence interval; CR, complete response; DCR, disease control rate; ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, estimated glomerular filtration rate; HR, hazard ratio; IQR, interquartile range; ITT, intention-to-treat; mCRC, metastatic colorectal cancer; mo, months; NR, not reported; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; PR, partial response; pts, patients; RCT, randomized controlled trial; RECIST, Response Evaluation Criteria in Solid Tumors; SD, stable disease; TTF, time to treatment failure; VEGF, vascular endothelial growth factor; wks, weeks.
In most cases, patients treated with regorafenib achieved a survival benefit with disease stabilization rather than tumor shrinkage (CORRECT: no complete responses, 1% partial responses; CONCUR: no complete responses, 4% partial responses).16,17 In routine clinical practice, response to treatment is usually assessed with regular computed tomography (CT) scans using Response Evaluation Criteria in Solid Tumors (RECIST). 26 However, because patients may benefit from anti-angiogenic therapy without experiencing a response based on a reduction in tumor size, a number of studies are evaluating alternative techniques that assess changes in tumor metabolism or morphology rather than shrinkage of target lesions. 26 Cavitation of lung metastases in response to regorafenib treatment has been observed using CT scans, potentially caused by anti-angiogenic therapy-induced necrosis or arterial thrombosis, and may be a novel radiologic marker of favorable outcome. 27 The observation of non-size-based morphologic changes in liver metastases using contrast-enhanced CT have also been identified as potential markers for early response to regorafenib.28,29 Collectively, these studies suggest that Week 8 CT assessment can provide useful information that may help predict outcome.27–29 In addition, positron emission tomography (PET), dynamic contrast enhanced-magnetic resonance imaging, and diffusion-weighted imaging are being evaluated in translational studies; these studies include the phase II TEXCAN study [ClinicalTrials.gov identifier: NCT02699073], 30 which evaluated CT texture analysis as a marker for response to regorafenib, and RegARd-C, a multicenter prospective study that used serial fluorodeoxyglucose PET-CT imaging to identify patients who are unlikely to respond to regorafenib [ClinicalTrials.gov identifier: NCT01929616]. 31
Clinical outcomes with regorafenib
Treatment with regorafenib has resulted in long-term response or disease stabilization in patients with mCRC in several phase III trials. In CORRECT, 19% of patients with mCRC receiving regorafenib experienced PFS >4 months, 32 and the proportion of patients with PFS in CONSIGN was similar (23%). 21 A higher proportion of patients (34%) achieved PFS >4 months in CONCUR, and an extended tail is visible on the Kaplan–Meier survival curve (PFS HR = 0.31), possibly because fewer patients in this trial had received prior biological therapy. 33 While this information regarding long-term responders is of value, communicating these data to patients can be challenging because there is currently no standardized method of identifying patients with mCRC most likely to benefit from regorafenib for an extended period. Although an extended tail on the survival curve has generally not been seen with regorafenib (unlike immunotherapy in microsatellite unstable mCRC in a minority of patients), 34 it is an important option for heavily pretreated patients, particularly for the majority of patients with mCRC who have microsatellite stable tumors, and who are therefore not eligible for immunotherapy. For most patients, it could be helpful to explain, in advance of treatment initiation, that achieving disease stabilization is a reasonable and positive treatment outcome. In other words, treatment could result in a halting of tumor progression and that the 2-month re-evaluation landmark is an appropriate time for taking further decisions.
Factors such as appropriate patient selection and management [including optimal management of adverse events (AEs)] can maximize the treatment benefit. Firstly, in CORRECT, patients who achieved PFS >4 months tended to have a better baseline Eastern Cooperative Oncology Group performance status (ECOG PS) than patients with shorter PFS (⩽4 months), 32 highlighting the importance of using regorafenib early during third line before deterioration of ECOG PS. While the CORRECT trial only included patients with an ECOG PS of 0 and 1, real-world studies have confirmed that patients with ECOG PS 0–1 achieved better outcomes than those with ECOG PS 2.20,24 Secondly, it is important to consider the optimal treatment sequence. As mentioned earlier, the longer OS observed in CONCUR compared with CORRECT may be related to the fact that patients in CONCUR had received fewer prior treatments, including targeted agents.16,17 In CORRECT, all patients had received prior bevacizumab, and 52% had received prior anti-EGFR therapy versus 41% and 35%, respectively, in CONCUR.16,17,35 The results of a small phase II Japanese study, REVERCE, in patients with KRAS wild-type tumors also support regorafenib use earlier in the treatment sequence, although these results need to be confirmed in additional studies. OS after relapse on chemotherapy was longer with the sequence of regorafenib followed by cetuximab +/– irinotecan compared with cetuximab +/– irinotecan followed by regorafenib. 36 In line with these results, and due to lack of available high-quality evidence, we believe that any rechallenge or recycling of a treatment given previously should be reserved for later lines of treatment. This is consistent with the conclusions from a recent systematic review stating that regorafenib or trifluridine/tipiracil are appropriate choices for third-line treatment and that rechallenge should be reserved for later use in patients with good ECOG PS who are willing to receive further lines of treatment. 6 Finally, appropriate dose modifications and proactive management of AEs (discussed later) are essential to ensure that patients are able to maintain a good QoL and remain on therapy long enough to receive benefit.
AE profile of regorafenib
Regorafenib has a consistent and predictable AE profile, typical of tyrosine kinase inhibitors, characterized by hand–foot skin reaction (HFSR), hypertension, diarrhea, and fatigue (Table 2).18,37 The AEs reported during regorafenib treatment differ from those of conventional chemotherapy (e.g., unlike chemotherapy agents, including trifluridine/tipiracil, regorafenib does not cause bone marrow suppression, and skin toxicity is different from that seen with capecitabine and other chemotherapy agents). This distinctive pattern of AEs, which also differs from other targeted agents, may present challenges to clinicians who are unfamiliar with their management.
Most frequent regorafenib-related grade ⩾3 AEs.

AE, adverse event; HFSR, hand–foot skin reaction; NR, not reported.
AEs typically occur early in treatment, reaching the maximum grade and highest incidence during the first two cycles, and subsequently declining to a stable incidence.21,24,38 Many AEs are low grade, and regorafenib toxicity is not cumulative. 39 In the CORRECT trial, the incidence of grade ⩾3 HFSR, fatigue, hypertension, and rash/desquamation typically peaked in Cycle 1 and reached a relatively stable lower incidence over later cycles, while the incidence of diarrhea remained relatively constant throughout the study. 38 HFSR first occurred at a median of 15 days, with the worst grade at a median of 22 days. 38 Therefore, it is important to monitor patients closely while on treatment, with proactive and frequent monitoring particularly in the first 1–2 cycles, with appropriate dose adjustment, treatment breaks, and intervention to avoid permanent discontinuation of treatment.
We recommend that patients are evaluated at least weekly for the first 4 weeks (first cycle) and then every 2 weeks during Cycle 2. Evaluation can be through face-to-face consultations or telephone calls from a trained healthcare professional. 37 Specialist nurses can play an important role in the management of AEs, by educating patients about what to expect and providing support in the first few weeks of therapy. Close monitoring during the first cycle ensures that the dose can be optimized in the second cycle. Experience from clinical trials has shown that after initial dose adjustments, patients can usually tolerate long-term treatment.
A correlation has been observed between HFSR during regorafenib treatment and OS regardless of when it occurs or at what grade. This important finding should be communicated to patients experiencing HFSR to encourage them to remain on treatment. In a post hoc exploratory analysis of the CORRECT study, the median OS of patients with HFSR at any time in the study was 9.5 months versus 4.7 months for patients without HFSR (HR 0.41). 40 Median OS was also numerically longer in those who experienced HFSR in Cycle 1 (7.2 versus 5.7 months in patients without HFSR in Cycle 1; HR 0.66). 40 Similarly, the REBECCA and Japanese studies showed that OS was longer in patients experiencing HFSR early.20,24 A correlation has also been reported between OS and skin rash or hypothyroidism in a small retrospective analysis of 144 patients 41 ; however, there are no prospective data documenting a link between incidence of AEs and longer survival. Therefore, it is important to educate patients before starting treatment on the potential AEs and how to promptly recognize and manage them; this, in turn, may motivate them to adhere to treatment.
Management of AEs
As aforementioned, appropriate AE management includes both preventive measures and symptom management, as well as dose adjustments and temporary interruption.37,42,43 Management of clinically relevant AEs (HFSR, hypertension, and fatigue) is summarized in Table 3, and Figure 1 provides detailed guidance for HFSR.
Management of selected AEs.

ACE, angiotensin-converting enzyme; AE, adverse event; HFSR, hand–foot skin reaction.

Management of HFSR. Adapted from McLellan et al. 44
HFSR can be particularly problematic for patients because it can affect their ability to undertake day-to-day activities, and should be pre-empted if possible and actively managed to allow patients to remain on active therapy for longer. Preventive strategies include skin examinations, manicures/pedicures, exfoliation of pressure points, creams, and avoidance of stress and friction on the skin.37,42,44 If HFSR occurs, management should be proactive and include reinforcement of preventive measures, topical creams, pain relief as necessary, and dose interruption/reduction (see Figure 1 and Table 3 for details).37,42,44
Hypertension occurs relatively frequently during regorafenib treatment, but it is not cumulative, and provided it is treated appropriately, it has negligible impact on patients’ QoL. 43 Pre-existing hypertension should be well controlled before the start of regorafenib treatment and blood pressure should be measured frequently during treatment, at least weekly in the first two cycles and then at the start of subsequent cycles. Patients should be advised to monitor their blood pressure at home and to report specified increases.42,43 If hypertension occurs, it should be treated with appropriate antihypertensive therapy in line with usual guidelines, together with regorafenib dose interruption/reduction.
Fatigue can have a serious impact on QoL and may be difficult to manage. 43 Patients should be encouraged to take gentle exercise. 42 If thyroid function is impaired, appropriate replacement therapy may be needed. 45 It has been reported that prophylactic oral dexamethasone lessens fatigue during regorafenib treatment. 46 Dose interruption or reduction should be considered for persistent fatigue.
Diarrhea can be managed with standard anti-diarrhea medication such as loperamide. Patients should be given advice on diet modifications and be encouraged to keep a food record to help identify the cause.37,43 Dose interruption or reduction may be needed for persistent grade 3 diarrhea.
Since AEs may be an early indicator of anti-tumor activity, appropriate management to control symptoms is extremely important to minimize treatment interruption. 41
Dosing and dose modifications
The standard dose of regorafenib is 160 mg (4 × 40 mg tablets) once daily for 3 weeks on followed by 1 week off therapy (3/1 schedule), which is one cycle.9,10 The dose can be adjusted in 40 mg (one tablet) weekly steps, but should not be lower than 80 mg/day; the maximum daily dose is 160 mg. Treatment modifications (dose reduction or delay) can be used in conjunction with appropriate symptomatic treatment to manage AEs. Re-escalation is an option once the toxicity has resolved, and this should be at the physician’s discretion, taking into account patient preference, as well as relevant clinical factors such as performance status and duration and severity of prior adverse reactions. The prescribing information provides guidance on treatment interruption and dose reduction for the management of AEs.9,10 Details of the dose modifications for HFSR management are given in Figure 1. 44 The prescribing information also gives guidance on dose interruptions and modifications in case of liver toxicity. Dose interruptions and/or reductions may be required for other AEs based on individual safety and tolerability. In the pivotal trials (CORRECT and CONCUR), most patients were titrated to a tolerable regorafenib dose and some patients were able to return to the full dose once the toxicity had resolved.16,17 Dose and schedule modifications play a key role in managing AEs and allow patients to remain on therapy for as long as possible, thus optimizing benefit. 37
Alternative starting doses
Many clinicians start regorafenib at a lower dose (80 or 120 mg/day) and escalate according to patient tolerance.1,19,37,47–49 A lower starting dose (80 or 120 mg/day) may be appropriate for certain patients, with subsequent dose escalation to reach the recommended dose of 160 mg/day subject to tolerability at the highest dose given. 37 Real-life experience suggests that in patients who do not meet the entry criteria for CORRECT, regorafenib can be started at 120 mg/day and then escalated to 160 mg/day on Day 14 if tolerated. 42 A randomized, phase II trial (ReDOS) evaluated the strategy of starting treatment at 80 mg/day for the first week, with weekly escalation to 120 mg/day and then to 160 mg/day if no significant drug-related toxicities or disease progression occurred; dose escalation is thus based on clinical judgement. 50 This approach was superior to the standard starting dose of 160 mg/day, with more patients completing two cycles and starting the third cycle compared with those starting at the standard dose (43% versus 26%, p = 0.043) [ClinicalTrials.gov identifier: NCT02368886]. 50 There was a non-significant trend toward longer OS with the dose-escalation schedule, as well as improved QoL after the second week. A key challenge in a real-world clinical setting is to try and ensure patients reach their first tumor evaluation (8-week scan) and receive regorafenib long enough to potentially observe at least disease stabilization because continued durable benefit may be expected in some cases. The ReDOS study results indicate that a reduced starting dose (and thus a reduced need to actively handle AEs), followed by flexible dose escalation where tolerability allows, may be a way of achieving this in many patients who may not otherwise have been able to benefit from regorafenib treatment. The regorafenib dose-escalation schedule evaluated in ReDOS has been incorporated in the latest NCCN guidelines and may represent an important option for selected patients. 19
Other trials have evaluated flexible first cycle dosing strategies. REGOCC-12 was a single-arm Japanese study in which regorafenib was administered at 120 mg/day with an option to increase to 160 mg/day from Cycle 2 onwards in the absence of significant toxicity. 51 The disease control rate (primary endpoint) was 37%, and 7% of patients had stable disease lasting for ⩾6 months. It was concluded that the 120 mg starting dose appeared to have similar efficacy to the 160 mg dose. 51 Another study (RESET) also evaluated a 120 mg/day starting dose of regorafenib in Japanese patients. In this study, dose escalation to 160 mg on Day 15 was achieved in only 6/70 patients and the disease control rate was lower than expected (32.4%), suggesting that efficacy may be compromised if dose escalation is not implemented. 52 However, PFS was not reported, and this was a small study, which should therefore be interpreted with caution. The randomized, phase II REARRANGE study investigated different dosing approaches of induction (first cycle) treatment with regorafenib in patients with mCRC, including an assessment of safety, efficacy, and dose-related outcomes. 53 While REARRANGE did not meet its primary endpoint of improved tolerability in patients who received regorafenib at a reduced or intermittent dose (120 mg/day for 3 weeks on/1 week off, or 160 mg/day for 1 week on/1 week off, respectively) compared with the standard dose, flexible dosing showed numerical improvement in relevant AEs such as fatigue, HFSR and hypertension, while maintaining efficacy, thereby supporting the results from ReDOS.50,53
Communicating with patients
Patient preference is a very important consideration, particularly in later lines of therapy, and it is essential to explain the options to the patient and involve them in treatment decisions. For example, trifluridine/tipiracil (TAS-102) is an alternative efficacious salvage option in patients who are refractory to standard therapies. Crossover treatment with both drugs improves survival, and, in one study, median OS was longer in patients who crossed over from regorafenib to TAS-102 (11.5 months) compared with those who crossed over from TAS-102 to regorafenib (7.6 months); nonetheless, decisions on their sequencing will depend on individual patient characteristics and preferences.54–56 Key points to communicate to patients are summarized in Box 1. The SHARE Communication Framework provides a basis for shared decision-making in third-line treatment of patients with mCRC. It provides a five-step structure to facilitate physician–patient interaction that covers the advantages and disadvantages of each treatment option, potential side effects, and treatment expectations. 57
Checklist of points to cover with patients.

AE, adverse event; HFSR, hand–foot skin reaction; OS, overall survival.
The shift to an oral, targeted agent places greater responsibility on the patient to adhere to treatment; education about the importance of adherence and its potential impact on clinical outcomes has an important role. The drug’s mechanism of action, potential AEs, and the strategy for preventing and managing these AEs should be explained to the patient before starting treatment. The importance of close and regular communication between the patient and the oncology team, especially within the first few weeks of therapy, was described earlier. Patients should be informed about the importance of reporting any possible AEs promptly so that they can be managed appropriately, increasing the likelihood of remaining on treatment for a longer period.
Conclusion
Key take-home messages to consider when treating patients with regorafenib in the third-line setting are listed in Box 2. Appropriate patient selection and good management of AEs can allow patients to achieve maximum benefit from regorafenib, maintain good QoL, and potentially increase survival time, allowing patients to receive subsequent lines of therapy. Fourth-line therapy can include trifluridine/tipiracil, which is effective after regorafenib. 58
Take-home messages.

AE, adverse event; HFSR, hand–foot skin reaction; OS, overall survival; QoL, quality of life.
To optimize outcomes, consideration should be given to offering eligible patients all active agents, as later-line therapies are associated with significant OS benefit. It is expected that the treatment of patients with mCRC will continue to improve with increasing individualization of treatment as more biomarkers are identified and allow a greater understanding about which patient subgroups will or will not benefit from specific agents.
Footnotes
Acknowledgements
Editorial assistance in the preparation of this article was provided by Christine Drewienkiewicz of Open Health Medical Communications (Choice) with financial support from Bayer.
Conflicts of interest statement
FL has held consulting/advisory roles with Amgen, Bayer, and Sanofi; is a speakers bureau member for Amgen, Bayer, Roche, and Sanofi; has received research funding from Amgen, Bayer, Merck Serono, and Roche; and has received personal fees from Amgen, Merck Serono, and Roche. J-BB has received honoraria from Amgen, AstraZeneca, Bayer, Celgene, Merck Serono, Pierre Fabre, Roche, Sanofi, Servier, and Shire; has held consulting/advisory roles with Amgen, Bayer, Merck Serono, and Servier; and has received personal fees from Amgen, Merck Serono, and Roche. FP has held consulting/advisory roles with Amgen, Bayer, Lilly, Merck Serono, Roche, Sanofi and Servier. HT has received honoraria from Bayer, Chugai Pharma, Lilly Japan, Merck Serono, Taiho Pharmaceutical, Takeda, and Yakult Honsha, and has received research funding from Boehringer Ingelheim, MSD Oncology, Otsuka, and Takeda; SY has received honoraria from Bayer Yakuhin, Bristol-Myers Squibb Japan, Chugai Pharma, Lilly Japan, Merck Serono, Ono Pharmaceutical, Sanofi, Taiho Pharmaceutical, Takeda, and Yakult Honsha. TB-S has held consulting/advisory roles with Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Genentech/Roche, Glenmark, Ipsen, Lilly, Merrimack, National Comprehensive Cancer Network, and Regeneron and Research to Practice (a Multi-tumor Regional Symposia series); has received research funding from National Comprehensive Cancer Network, National Cancer Institute, and Oncolytics; has provided expert testimony for Helsinn Therapeutics; and holds other relationships with ARMO BioSciences, Exelixis, Merck, Polaris, and SillaJen. LA, F-CK, TM, R-HX, TW and SZ have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Bayer.