
Abstract
Background and Aims:
The standard treatment of non-metastatic anal squamous cell carcinoma (ASCC) consists of chemotherapy with mitomycin (MMC) plus 5-fluorouracil (5FU) for 1–2 cycles concomitant with pelvic radiotherapy. Subsequent studies introduced cisplatin (CDDP) combined with 5FU, with unclear results. We evaluated the doublet capecitabine (C) and CDDP as a possible alternative to MMC-5FU regimen concomitant with intensity-modulated radiation therapy (IMRT).
Patients and Methods:
We carried out a retrospective study on 67 patients affected by stage I–III ASCC, treated with CDDP (60–70 mg/m2 every 21 days for two courses) plus C (825 mg/m2 twice daily for 5 days/week) chemotherapy concomitant with IMRT for curative intent.
Results:
At a median follow up of 41 months, the clinical complete response calculated at the 6-month time-point (6-moCR), the 6-month objective response rate and the 6-month disease control rate were 93%, 94%, and 99%, respectively.
Disease-free survival rates at 1, 2, and 3 years were 89%, 87%, and 85%, while the overall survival rates at 1 and 2 years were 100% and 95%. The colostomy-free survival rates were 90% at 1 year and 88% at 2 years. Grade 3–4 acute adverse events were reported in 61% of patients; predominantly skin toxicity (46%) and limited hematological toxicity (12%).
Conclusion:
In this retrospective study, chemotherapy with C plus CDDP concomitant with IMRT proved safe and effective, and may represent a possible alternative option to standard MMC-containing regimen for curative intent.
Keywords
Introduction
Anal cancer is a rare malignancy (2.7% of gastrointestinal tumors). 1 Risk factors include female gender, tobacco consumption, human papillomavirus (HPV) or human immunodeficiency virus (HIV) infection, previous vulvar or cervical cancer and chronic immunosuppression. Poor prognostic features at tumor diagnosis are tumor size >5 cm and regional nodal involvement.2–4
Based on results of the phase II trial by Nigro, confirmed by phase III trials that established the clear advantage of chemo-radiotherapy (C-RT) over radiotherapy (RT) alone, systemic chemotherapy with mitomycin (MMC) plus 5-fluorouracil (5FU) for 1–2 cycles concomitant with pelvic RT represents the standard treatment for non-metastatic anal squamous cell carcinoma (ASCC).5–8 Surgery is reserved as salvage therapy for progressive/recurrent local disease only. 9
The well-known radiosensitizing properties of platinum-salt agents in different squamous cell tumors have stimulated a growing interest in the combination of cisplatin (CDDP) with 5FU in studies. However, even though efficacy data are comparable, there is no clear advantage in terms of toxicity and so no consensus for replacing the standard MMC in ASCC treatment. 10
Developments in RT have allowed dynamic variations in dose intensity to be delivered more precisely to the tumor tissue with reduced damage to surrounding normal tissue and consequent reduced genitourinary and bowel toxicity. Currently intensity-modulated radiation therapy (IMRT) represents the standard of care in the United States (US), even if it is not adopted worldwide for ASCC; its better management in terms of efficacy and toxicity could allow the concomitant role of CDDP to be reassessed. 11
Since 2010, IMRT has been proposed in our institute, concomitantly with CDDP plus oral fluoropyrimidine capecitabine (C) as a possible alternative to the MMC-5FU regimen in patients who preferred to avoid central vein catheter and/or when an increased hematological toxicity related to clinical history was expected.
Here, we report the largest case series treated with this combination to date.
Patients and methods
Patient selection
We carried out a retrospective study on consecutive patients with ASCC treated between June 2010 and December 2017 at the Gastrointestinal Division of the European Institute of Oncology, Milan, Italy.
Inclusion criteria were: histologically proven diagnosis of ASCC, absence of distant metastases (stage I–III), measurable disease according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, 12 age >18 years, Eastern Cooperative Oncology Group (ECOG) performance status (PS) ⩽2, treatment with CDDP plus C chemotherapy concomitant to IMRT for curative intent. All patients had life expectancy of at least 3 months, adequate bone marrow (hemoglobin ⩾9 g/dl, neutrophil count ⩾1500/mm3, platelet count ⩾100,000/mm3), liver (serum total bilirubin ⩽1.5× upper limit normal, transaminases ⩽3× upper limit normal) and renal function (serum creatinine within normal ranges and calculated creatinine clearance ⩾50 ml/min).
Exclusion criteria were: previous pelvic RT, different chemotherapy schedules, medical or psychological impairments associated with restricted ability to give consent or difficulty in adhering to the regular treatment plan. Patients with past or current malignancies, other than ASCC, were allowed if treated with curative intent.
Study procedures
The present study was part of the research project “Image guided radiotherapy in gastrointestinal malignancies”, approved by the European Institute of Oncology Ethical Committee, Milan, Italy (registration number: IEO N87/11). Clinical and technical analyses for this project, carried out both retrospectively and prospectively, were conducted according to the Declaration of Helsinki and in line with the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals. All patients gave written informed consent for the research and educational purposes, and their data were extrapolated anonymously.
Treatment
Radiotherapy
All patients, with a full urinary bladder and empty rectum, underwent planning computed tomography (CT) scan in the supine position. The gross tumor volume, including primary tumor and involved lymph nodes, was delineated on the CT scan. Magnetic resonance imaging (MRI) and/or positron emission computed tomography with 18fluorodeoxyglucose (18FDG-PET/CT) were used to better define the anatomical structures during contouring procedures. The clinical target volume and the planning target volume (PTV) were contoured according to Radiation Therapy Oncology Group (RTOG) 0529 and Australasian Gastrointestinal Trials Group (AGITG) guidelines.13,14 For all patients, RT to the bilateral inguinal nodes was planned as prophylactic or curative. Patients with early stage disease were evaluated for a boost with brachytherapy (BRT) depending on clinical factors (age, PS, clinical tumor stage). The low-risk (bilateral external and internal iliac, presacral, and inguinal nodes), the high-risk (strictly adjacent tumor tissues) and the tumor PTVs were scheduled to receive at least 32 Gy, 40 Gy, and 50 Gy, respectively. Dosimetric parameters followed the International Commission on Radiation Units and Measurements (ICRU) recommendations (report No. 83). 15 The dose volume constraints for the organs at risk, delineated by the CT scan, were adopted from RTOG 0529 and RTOG 0921 trials.13,16,17 IMRT was performed using either RapidArc® or Tomotherapy® image-guided RT.
Chemotherapy
The chemotherapy scheme consisted of CDDP 70 mg/m2 (60 mg/m2 for patients >70 years) every 21 days for two courses plus C 825 mg/m2 twice daily for 5 days/week concomitant with IMRT until the evening of the last dose of RT.
At baseline, complete medical history, including age, gender, ethnicity, ECOG PS, Charlson comorbidity index (CCI, a score based on the patient comorbidities weights able to predict outcomes, such as mortality or higher resource use), 18 histological type, HPV genotype, tumor-node-metastasis stage 7th edition, was recorded. Clinical and instrumental evaluation were performed by digital anorectal examination (DRE), anorectal endoscopy with tumor biopsy for histology and HPV status, anorectal ultrasound and/or pelvic MRI with contrast and chest-abdominal-pelvic CT scan with contrast. In case of suspected extra regional disease (44 patients), 18FDG-PET/CT was carried out. Female patients underwent a gynecological examination at the beginning of the treatment and they were followed up regularly at the discretion of the gynecologist.
ECOG PS, vital signs, weight and body mass index, physical examination, blood samples for bone marrow, renal and liver function were performed at baseline, at weekly intervals during therapy (including before each CDDP administration) and at the end of treatment. Subsequent analyses were carried out at 8 weeks and 6 months after treatment start, and then every 4 months during the first 2 years and every 6 months during the subsequent 3-year follow-up period.
During treatment, and at the same time points as previously mentioned, all toxicities were recorded according to Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. 19 Patients with abnormal values after the termination of C-RT were monitored for toxicity weekly and, if necessary, every 4 weeks until normalization of the values.
Assessment of tumor response was planned at 6 months from the start of C-RT by DRE, anorectal endoscopy, and pelvic MRI, and repeated every 4 months during the first 2 years and every 6 months for the subsequent 3 years if a CR was obtained. Distant disease monitoring was conducted by chest-abdominal-pelvic CT scan every 6 months for 2 years and annually thereafter.
Statistical analysis
The primary endpoint was the proportion of patients with observed CR at 6-months after the start of C-RT (6-moCR). Secondary end-points were: the 6-month objective response rate (6-moORR), that is the percentage of patients who achieved CR and partial response at the 6-month time-point; the 6-month disease control rate (6-moDCR), that is the percentage of patients with CR, partial response, and stable disease at the 6-month time-point; the disease-free survival (DFS), calculated only in patients achieving CR from 6-months after the start of therapy to the date of the first documented tumor recurrence, other primary tumor, or death due to any cause; the overall survival (OS), calculated in all patients from the start of the study treatment until death from any cause; the tumor-related and treatment-related colostomy-free survival (CFS), calculated in all patients from the baseline to the day of surgery for colostomy or death, whichever occurred first; the incidence of acute (within 3 months of treatment) severe toxicity [grade (G)3–G4, according to CTCAE version 4.03]. The maximum toxic effect grade was used for each patient and each event type. Exact confidence intervals (CIs) for binomial proportion were calculated. The DFS, OS, and CFS were estimated using the Kaplan–Meier method. All analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA). A p value less than 0.05 was considered statistically significant.
Results
The main patient characteristics are reported in Table 1.
Baseline patient characteristics (N = 67).

BMI, body mass index; CCI, Charlson comorbidity index; ECOG, Eastern Cooperative Oncology Group; HIV, human immunodeficiency virus; HPV, human papillomavirus; PS, performance status; SCC, squamous cell carcinoma.
Out of 96 screened consecutive patients, 67 [60 females (F) and 7 males (M)], all Caucasian, were eligible for treatment evaluation in terms of toxicity and efficacy. A total of 29 patients were excluded due to metastatic disease (4 cases), treatment choice different from the CDDP-C doublet schedule (24 cases) or to C monotherapy (1 patient with kidney failure).
HIV positivity was identified in 1/21 evaluated patients. Of the cases with HPV, 52 were HPV16+, 6 had multiple HPV genotypes in combination with HPV16+, and 3 were HPV33+.
Tumor location in all patients was the anal canal. Basaloid histology was described in 5 patients (4 F HPV16+ and 1 M HPV16+/18+). Based on medical history, 17 patients (25%) reported cancer diagnoses: 7 cervical intraepithelial neoplasia type 3; 1 cervical cancer; 1 cervical cancer plus lymphoma; 5 breast cancer; 1 melanoma; 1 squamous penile cancer (HPV16+18+, HIV+), and 1 concomitant diagnosis of papillary thyroid carcinoma treated with surgery after completing C-RT for ASCC.
The elective low-risk PTV received a median dose of 41.4 Gy (range 32.4–48.6 Gy), high-risk PTV received a median dose of 46 Gy (range 40–56 Gy), while tumor and positive nodes received a total median dose of 56 Gy (range 36–60 Gy). The boost on macroscopic disease was given using either a sequential boost technique or a simultaneous integrated boost strategy. Some patients received boost with BRT after 36–50 Gy of external RT. Both high dose rate (HDR) and pulsed dose rate (PDR) BRT were used. In case of PDR treatment, the dose administered was 10 Gy with dose rate of 0.4 Gy/h and 20 Gy with dose rate of 0.4 or 0.5 Gy/h; in case of HDR treatment, a mean dose of 16 Gy (range 8–25 Gy in 3–5 fractions) prescribed to 5 mm depth was given. Median time gap between EBRT and BRT was 21 days (range 12–53 days). Only two patients received the BRT boost after a time gap of longer than 1 month. One of them received the boost after 39 days because of skin and gastrointestinal toxicity; the second patient underwent a restaging MRI to evaluate the response and to optimize boost parameters. Objectives for target volume were set so that, for PTV, 95% of the prescribed volume should receive at least 95% of the prescribed dose. The prescribed dose was delivered in a median of 28 fractions (range 18–29), with daily fractions of 1.7–2 Gy, 5 days per week. The minimum and maximum dose, as the accepted variation in the dose distribution, was 93% <0.03 cm3 of the PTV <110%.
Due to G2–4 systemic or local adverse events (AEs), a median break in C-RT of 7 days (range 1–21) was necessary in 56 patients (84%), though all patients completed the planned RT. RT details are shown in Table 2.
Radiotherapy details.
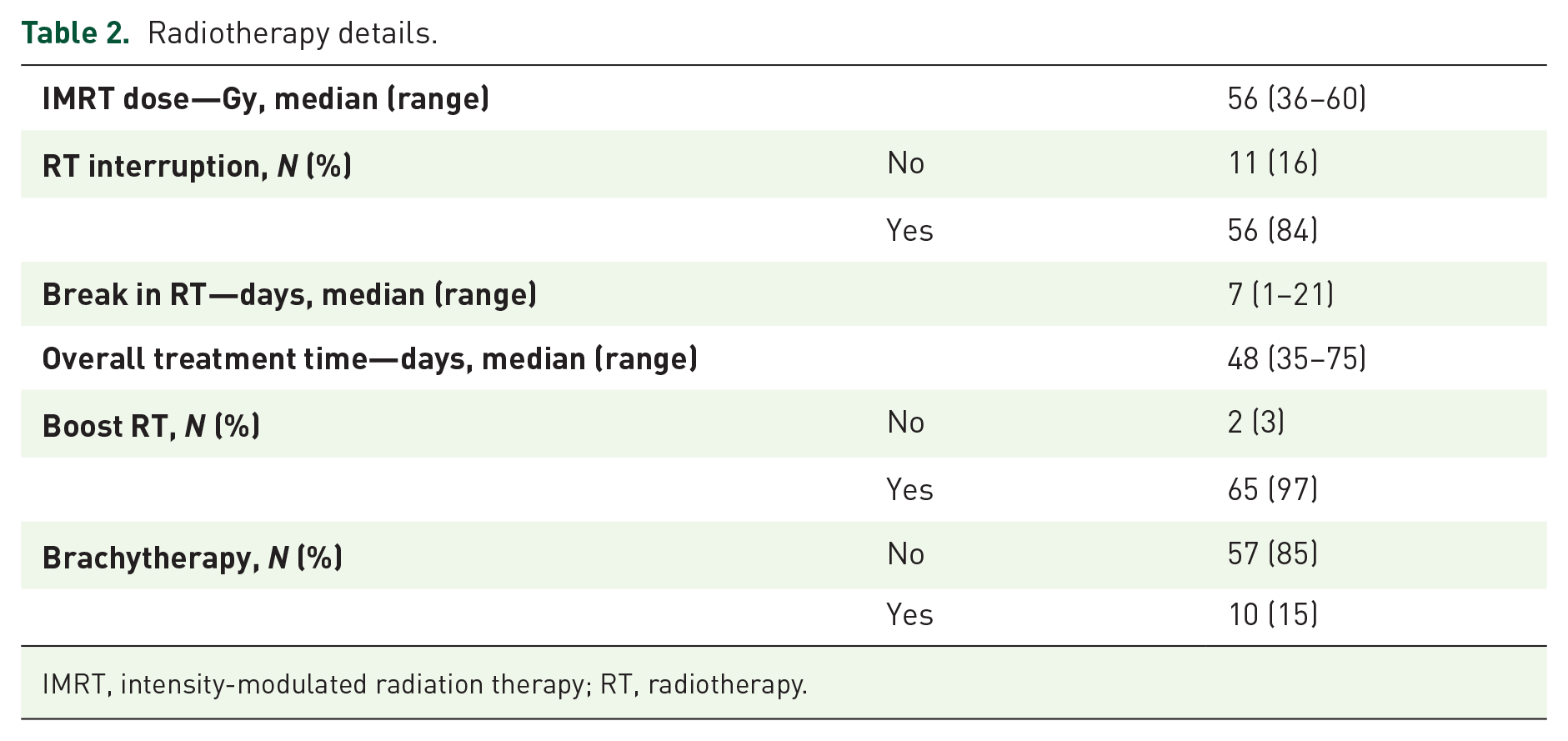
IMRT, intensity-modulated radiation therapy; RT, radiotherapy.
A total of 62 patients (93%) were able to complete both the two cycles of chemotherapy, while 5 patients underwent only one cycle.
All patients experienced some acute toxicity, of which 61% had G3–4: 39 (58%) patients reported G3 AEs, mainly skin toxicity (46%), with one case of anal-cutaneous fistula that developed during EBRT; G4 AEs occurred in only two cases (one gastrointestinal and one hematological, with leuco-neutropenia and thrombocytopenia). Toxicity details are shown in Table 3.
Acute toxicity (N = 67). The maximum toxic effect grade was considered for each patient and each event type.

Only the maximum grade observed for each patient is reported.
The 6-moCR, the 6-moORR and the 6-moDCR were 93% (62/67 patients), 94% (63/67), and 99% (66/67), respectively.
At a median follow up of 41 months, the median DFS was not reached in 62 patients with CR at the 6-month time-point (Figure 1A), with a DFS rate of 89% (95% CI 77–95%], 87% (95% CI 75–94%), and 85% (95% CI 72–92%) at 1, 2, and 3 years, respectively. The median OS of all 67 patients was not reached (Figure 1B), with an OS rate of 100% and 95% (95% CI 85–98%) at 1 and 2 years, respectively.

(A) DFS in patients with CR at 6 months from the start of treatment (N = 62). (B) OS in all patients (N = 67).
Using an exact Fisher’s text, we compared the 6-moCR for all 67 patients between different levels of possible predictors. We included the 62 patients with 6-moCR in a survival analysis, modelling the DFS with a Cox univariate model for each predictor. No statistically significant difference was observed. A better trend in response was seen for patients who developed G3 cutaneous toxicity, but the small sample size does not allow its predictive value to be estimated (Table 4).
The 6-moCR (N = 67) and the DFS (N = 62) according to different possible predictors.

DFS, disease-free survival; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; 6-moCR, complete response at the 6-month time-point; PS, performance status; RT, radiotherapy; SCC, squamous cell carcinoma.
When stratified for other cancer diagnoses, patients did not show differences in DFS (p = 0.058; Figure 2A) and in OS (p = 0.345; Figure 2B), although the DFS curve suggests a slightly better prognosis at 3 years in terms of recurrence of disease for the subgroup without any history of cancer.

DFS (A) and OS (B) in patients with (dashed line) and without (continuous line) history of cancer.
Eight (13%) patients with 6-moCR presented recurrence within 2 years: four local relapses treated with abdominoperineal resection and four distant relapses treated with systemic chemotherapy.
The CFS rates were 90% (95% CI 79–95%) and 88% (95% CI 77–94%) at 1 and 2 years, respectively: three patients underwent colostomy before C-RT and never reversed, three patients underwent colostomy due to local progressive disease within 1 year after C-RT, and one patient due to the onset of an anal-cutaneous fistula.
Discussion
The primary aim of the treatment of non-metastatic ASCC is to achieve complete local control at 6 months from the start of treatment. This is the optimum time-point for minimizing loco-regional and systemic early and late toxicities.20,21
The doublet MMC-5FU concomitant with RT is considered the gold standard treatment, based on the results from phase III trials indicating its statistical improvement over RT alone/combined to 5FU.6–8,22
In the ACT I trial, the benefit of C-RT was confirmed beyond a median of 13 years, with an expected 25.3% fewer patients with locoregional relapse and 12.5% fewer anal cancer deaths compared with RT alone. 6
The contribution of CDDP as a curative therapy for ASCC is still unclear mainly because the available studies were addressed specifically to investigating its role as induction or maintenance therapy before or after C-RT.
Intergroup study RTOG 98-11 compared 5FU (1000 mg/m2 days 1–4 and 29–32) plus MMC (10 mg/m2 on days 1 and 29) and RT (45–59 Gy) with 5FU (1000 mg/m2 days 1–4, 29–32, 57–60 and 85–88) plus CDDP (75 mg/m2 on days 1, 29, 57 and 85) and RT (45–59 Gy; start day: 57). In the last 2012 update of 649/682 evaluable patients, DFS and OS resulted statistically better for the MMC arm versus the CDDP arm (5-year DFS: 67.8% versus 57.8%, p = 0.006; 5-year OS: 78.3% versus 70.7%, p = 0.026), with a trend toward statistical significance for CFS (p = 0.05). Conversely, increased hematological toxicity was described in the MMC group (61.8% versus 42%, p < 0.001). 23
In the ACT II trial, patients were randomly assigned to one of four groups: MMC (12 mg/m2 on day 1) or CDDP (60 mg/m2 on days 1 and 29), with 5FU (1000 mg/m2 days 1–4 and 29–32) and RT (50.4 Gy), with or without two courses of maintenance chemotherapy (5FU and CDDP weeks 11 and 14). At a median follow up of 5 years, no difference in terms of ORR, progression-free survival (PFS) and OS was found between MMC for one cycle plus RT and CDDP-5FU for two cycles plus RT ± two additional CDDP-5FU courses, confirming higher hematological toxicity in the MMC arm (G3–G4 26% versus 16%). 24
Furthermore, the role of CDDP was excluded both as an induction and maintenance treatment: this failure could be due to the delay in the start of the RT and the longer duration of the treatment, with a consequently greater probability of radio-resistance to platinum through the process of ‘cell repopulation’ (persistence of tumor cell clones that proliferate during treatment intervals), or could be determined by the increased radiosensitizing effect of MMC under hypoxic conditions.25–28
Limited data are available regarding the role of oral fluoropyrimidines, such as C, that represents a cost-effective alternative to infusional 5FU widely used in several malignancies, also concurrently with RT.29–31
The administration of C on a continuous daily basis can be assumed to increase the radiosensitizer effect compared with 5FU administration during the first and the last 4 days of RT, and to improve patient compliance also by avoiding venous central catheter.
The evidence of efficacy and manageable toxicity of the doublet MMC-C derived from retrospective studies (similar activity, but better tolerability of MMC-C versus MMC-5FU concomitant to IMRT, with lower hematologic toxicity and fewer treatment interruptions) and from phase II trials, with CR and locoregional control ranged from 77% to 89.1% and 79% to 94%, respectively, and high treatment completion rates despite the appearance of radiation dermatitis as the main toxicity (ranged from 23% to 63%).32–40 The data regarding the combination of C with CDDP or oxaliplatin are more limited.41–43 The main studies including C are reported in Table 5.
Main studies including capecitabine.

Bid, bi-daily; C, capecitabine; CDDP, cisplatin; CFS, colostomy-free survival; CR, complete response; D, day; DCR, disease control rate; DFS, disease-free survival; IMRT, intensity-modulated radiation therapy; MMC, mitomycin; ORR, objective response rate; OS, overall survival; RT, radiotherapy.
Definitive conclusions regarding CT treatment choices from the past studies are difficult to draw, because primary outcome measures were different in terms of DFS, PFS, local failure or CFS and the definitions of primary and secondary endpoints were not consistent across trials, as observed in a recent review of six randomized controlled trials, describing endpoints in curative ASCC treatment on 2877 patients. 44 Now the main goal is to find the best parameters to evaluate outcome in this setting.
Our mono-institutional retrospective study investigated well-defined endpoints and represents the largest trial conducted with the CDDP-C doublet concomitant with IMRT with curative intent in Stage I–III ASCC.
At a median follow up of 41 months, we showed substantial local control, with rates of 93%, 94%, and 99% for 6-moCR, ORR, DCR, respectively, and a satisfactory 3-year DFS rate of 85%, in agreement with the previous literature with the MMC-5FU regimen (26 weeks-CR: 89.6% in the CDDP group versus 90.5% in the MMC group, 3-year PFS: 74% for maintenance versus 73% for no maintenance in the ACT II trial). 24
In this study the CDDP-C schedule did not appear to affect adversely CFS. In fact, the cumulative rate of colostomies was 10% (7/67 patients), with three colostomies performed before treatment, due to locally extended disease, and only four colostomies within 1 year after the C-RT. The number of colostomies is smaller compared with ⩾20% historical results of CDDP-5FU plus RT.23,24,45
In our study, toxicity results were manageable and comparable with previous studies: 61% had G3–4 AEs, related mainly to local skin toxicity (46%). This apparent increased toxicity could potentially be related to the possible cutaneous effects of C, which could be reinforced by its daily radiosensitizing activity, and this could potentially be predictive for clinical outcome. 46
G3–4 hematologic AEs were less (12%) than with the MMC regimens (61.8% in the RTOG 98-11 trial; 26% in the ACT II trial).23,24 No treatment-related deaths occurred.
The patients included in our study had several comorbidities and often a high CCI. Previous malignancies, mostly HPV-related, were pre-treated with local and or systemic treatments in some cases. These adverse clinical features are often exclusion criteria preventing patient inclusion in clinical trials. However, in our study these comorbidities do not represent a problem as patients have already been treated with chemotherapeutical agents and so the proposed scheme is manageable in the context of real-life care.
Considering our favorable results in terms of efficacy, toxicity and CFS, C plus CDDP concurrent with IMRT should be considered an interesting alternative curative approach for patients with ASCC.
The main limitation is that this is a retrospective study and so does not allow definitive conclusions.
Conclusion
C plus CDDP chemotherapy concomitant with IMRT proves to be effective and well manageable in non-metastatic ASCC and it could represent a valid option to standard MMC-containing regimen, also for patients with unfavorable clinical characteristics. Prospective trials are needed to confirm these results.
Footnotes
Acknowledgements
The authors thank the patients, their families and all care givers; Cristina Mazzon and Darina Tamayo for data management; and Linda A. Cairns for English language editing.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.