
Abstract
Colorectal cancer (CRC) is one of the most common types of cancer worldwide, known as the second leading cause of cancer-related deaths annually. Currently, multimodal treatment strategies, including surgical resection, combined with chemotherapy and radiotherapy, have been used as conventional treatments in patients with CRC. However, clinical outcome of advanced stage disease remains relatively discouraging, due mainly to appearance of CRC chemoresistance, toxicity, and other detrimental side effects. New strategies to overcome these limitations are essential. During the last decades, melatonin (MLT) has been shown to be a potent antiproliferative, anti-metastatic agent with cytotoxic effects on different types of human malignancies, including CRC. Hence, this comprehensive review compiles the available experimental and clinical data analyzing the effects of MLT treatment in CRC patients and its underlying molecular mechanisms.
Introduction
Colorectal cancer (CRC) is one of the primarily responsible causes for cancer-related deaths worldwide.1–3 If diagnosed in the early stage, the 5-year survival rate after curative surgery reaches about 90%, dropping to only 14% with the appearance of distant metastasis. 4 Multimodal treatment regimens combine surgery with neoadjuvant/adjuvant chemotherapy (CTx) techniques as well as targeted therapies using antibodies and kinase inhibitors. 5 This results in decided improvement of survival for metastatic disease patients reaching a median of nearly 30 months. 6
CRC liver metastases (CRLM) occur in 20–70% of CRC patients, and represent the major cause of death in this group.7,8 Surgical resection is the standard treatment for patients with resectable CRLM (when it is possible to achieve R0 resection while maintaining at least a 30% functional liver tissue) resulting in a 5-year survival rate of up to 58% when combined with CTx.9,10 However, CRC cells are known to lose susceptibility to CTx by various mechanisms.11,12 To optimize treatment strategies, further evaluation of promising drug combinations and additives is necessary for improve patient survival.
Melatonin (MLT), a natural body hormone, previously demonstrated impressive protective properties against toxic effects of CTx and radiotherapy, in both experimental and clinical studies.13–15 This could pave the way for application of higher doses of CTx, resulting in improved efficacy. 16 Moreover, MLT itself exerts antiproliferative, antimetastatic, and cytotoxic effects on different types of human malignancies, including CRC.17–19 Taking into consideration that this endogenously generated molecule lacks any moderate–severe side effects at even relatively high dose,20–22 currently renders MLT a trending research topic, particularly in cancer treatment studies (Figure 1).

History of PubMed publications regarding MLT and cancer.
The objective of this comprehensive review is to summarize literature on the role of MLT in CRC and CRLM treatment, and discuss the mechanisms of its anti-cancer properties, based on experimental studies and clinical trials.
Melatonin
The endogenous hormone MLT, also known as N-acetyl-5-methoxytryptamine, was discovered by the North American dermatologist, Aaron Lerner in 1958 at Yale University. 23 For many years, MLT was considered to be synthesized exclusively in the pineal gland from the amino acid tryptophan in response to darkness (Figure 2).24–27 However, the presence of MLT-related enzymes was subsequently uncovered in a number of extrapineal tissues such as the gastrointestinal tract, thymus, spleen, heart, muscle, and others.18,24,28 Moreover, MLT was also identified in most living organisms, including bacteria, macroalgae, plants, invertebrates, and mammals.29–31

The biosynthesis process of MLT.
In humans and mammals, two classes of plasma membrane associated MLT receptors are known. They are named MT1 (encoded by MTNR1A gene) and MT2 (encoded by the MTNR1B gene), respectively,32–34 and are expressed in various parts of the central nervous system and the peripheral organs.35,36 Another binding site for MLT, MT3, has been recently characterized as a MLT-sensitive form of the quinone reductase 2. 37 It is related to the cell’s xenobiotic metabolism (detoxification enzyme) expressed in various tissues.24,38 However, MT3 is an entirely different type of protein, not fully satisfying the criteria for MLT receptors. 24 MLT also binds to cytoplasmic proteins, like the calcium-binding proteins calmodulin or tubulin, as well as nuclear receptors like RORα/RZR, and acts through non-receptor-mediated mechanisms.17,35
Soon after MLT was discovered to have a direct free radical scavenger effect, it was proposed as an anti-cancer agent. 20 In 2004, MLT was shown to be associated with mechanisms influencing cancer initiation and cell growth for the first time. 39 Since then, numerous studies have supported these findings.17–19
Modes of action in anti-cancer treatment
Proliferation inhibition
MLT exerts a wide range of antiproliferative properties by inhibition/blocking of the cancer cell cycle under in vitro and in vivo conditions.40–42 Activation of MT1 and MT2 receptors inhibits adenyl cyclase and cyclic adenosine monophosphate, leading to a reduction in uptake of linoleic acid, which serves as an energy source for tumor growth and tumor growth-signalling molecules. 17 MLT-induced inhibition of linoleic acid uptake is considered as antiproliferative mechanism, and was described by Blask et al. in a rat hepatoma model. 43 Furthermore, antiestrogenic effects, 20 and the ability to inhibit tumor growth by reducing glucose uptake and modifying the expression of the GLUT1 transporter have been shown in vitro and in vivo. 44 In a study on a murine colon carcinoma-derived cell line, MLT inhibited tumor growth in a dose-dependent manner; DNA synthesis was inversely associated with MLT dose. 45 Moreover, Lee et al. demonstrated that physiological levels of MLT are able to modulate the expression of microRNAs in a non-metastatic breast cancer cell line, promoting antiproliferative properties. 46 Recent studies found that these transcripts are dysregulated in many cancer entities, including CRC, and play an essential role in cancer-related signalling pathways.47–49
Apoptosis activation
Resistance to apoptosis is one of the fundamental hallmarks of cancer. There is strong evidence that MLT enhances and promotes apoptosis in various tumor cells.19,50–59 Jia-Yi Wei et al. demonstrated that histone deacetylase 4 plays a crucial role in MLT-induced apoptosis in LoVo (a human colon adenocarcinoma cell line) cells, most likely through the inactivation of calcium/calmodulin-dependent protein kinase (CaMK) IIα. 19 More recently, Lee et al. showed that MLT influences apoptosis and autophagy in human colon cancer stem cells by regulating the cellular prion protein (PrPC)-octamer-binding transcription factor (Oct) 4 axis. 53 Additionally, MLT acts via B-cell lymphoma 2 (Bcl-2) expression, the c-Jun N-terminal kinase, p38 and nuclear factor (NF)-κB-p65 signalling pathways, thereby promoting apoptosis in different types of cancer.51,54–59
Angiogenesis inhibition
As neovascularization is essential for tumor growth and metastasis, controlling angiogenesis is a promising treatment option for limiting cancer progression. Angiogenesis is regulated by factors like vascular endothelial growth factor or hypoxia induced factor (HIF), 60 and MLT has the ability to regulate the oncogenic potential by controlling the expression of such factors.40,61 In vitro and in vivo (rodent models) studies demonstrated that MLT affects HIF-1α, the most important and primary transcriptional mediator in hypoxic response, in a receptor-independent manner. 61 Previous findings suggest that upregulation of microRNAs mediates MLT induced anti-angiogenic effects in breast and hypoxic prostate cancer cells in vitro.62,63 These findings have been approved in a xenograft model. 63
Modulation of the immune system
The immune system presents the greatest potential for the specific destruction of malignant cells not harming normal tissue, and with the long-term memory offering a potent opportunity to prevent cancer recurrence. 64 The immuno-enhancing action of MLT was evident in recent animal and clinical studies.17,65 MLT has been shown to contribute to effective anti-cancer immune responses via mechanisms such as stimulation of interleukins (IL-2, IL-6, IL-12) production, the inhibition of macrophage-mediated suppressive events, and inflammatory status modulation.66,67
Antioxidative and pro-oxidative effects
MLT and its metabolites exert antioxidative effects. Besides direct scavenging of reactive oxygen and nitrogen species (ROS/RNS), MLT stimulates antioxidant enzymes, suppresses pro-oxidant enzymes, and improves mitochondrial function, thereby reducing radical formation in physiological and pharmacological concentrations.68–70 In vitro studies demonstrated a role of MLT in the maintenance of levels of the intracellular antioxidant glutathione, which has been related to cancer cell growth. 71 Elevated levels of ROS/RNS have been detected in almost all cancer entities, where they promote aspects of tumor development and progression. 72 For example, the steady-state levels of superoxide are significantly higher (5- to 20-fold) in colon cancer cell lines compared with normal colon epithelial cells and fibroblasts. 73 Interestingly, a few in vivo studies found that MLT induces the generation of ROS at pharmacological concentrations (μM to mM range) in tumor cells, leading to the assumption that MLT could be a conditional pro-oxidant. 68 This property of MLT may promote an inflammatory response leading to apoptosis in tumor cells, but further in vivo studies are needed to concretize this scenario.
Effects of MLT on CRC
Epidemiological studies demonstrated that night-shift workers might have an increased risk for cancer development, including CRC. This finding may support the hypothesis that environmental light inhibits MLT production, resulting in cancer promotion.74,75 In fact, many in vitro and in vivo studies have shown that MLT exerts anti-cancer effects on CRC. Those studies are compiled in Tables 1 and 2, respectively.
Summary of in vitro studies investigating the effects and mechanisms of MLT on CRC.
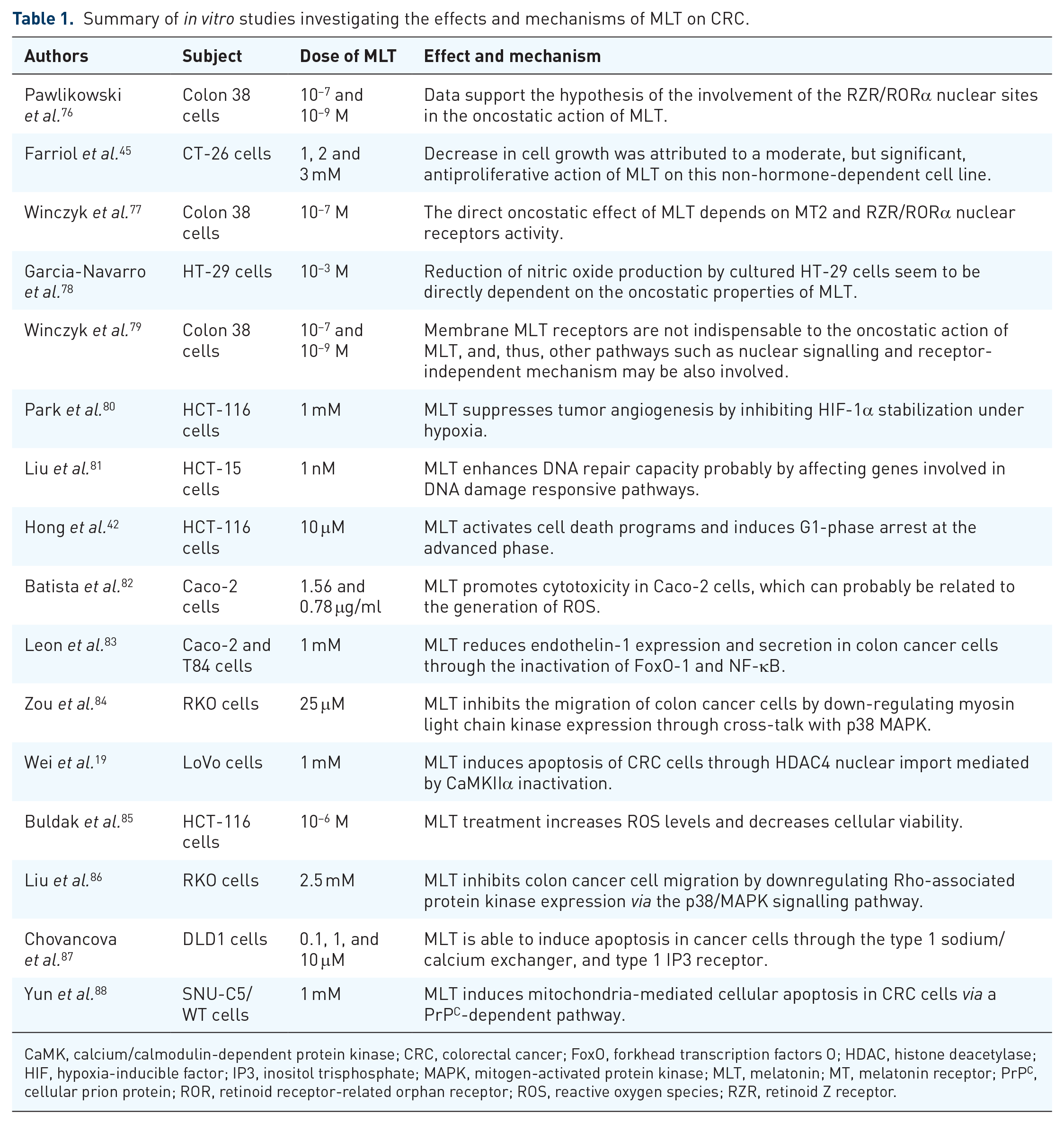
CaMK, calcium/calmodulin-dependent protein kinase; CRC, colorectal cancer; FoxO, forkhead transcription factors O; HDAC, histone deacetylase; HIF, hypoxia-inducible factor; IP3, inositol trisphosphate; MAPK, mitogen-activated protein kinase; MLT, melatonin; MT, melatonin receptor; PrPC, cellular prion protein; ROR, retinoid receptor-related orphan receptor; ROS, reactive oxygen species; RZR, retinoid Z receptor.
Summary of in vivo studies investigating the effects and mechanisms of MLT on CRC.

These studies used synthetic pineal peptide Epitalon.
CRC, colorectal cancer; DMH, dimethylhydrazine; LC, light chain; MLT, melatonin; MT, melatonin receptor; PO, per oral administration; ROR, retinoid receptor-related orphan receptor; RZR, retinoid Z receptor; SC, subcutaneous administration.
The synergistic effect of MLT and anti-cancer drugs in CRC treatment
For several years, scientists searched for strategies to reduce the toxic side effects of CTx on the one hand, and to increase tumor-specific response on the other. Data on the synergistic effects of CTx agents and MLT on CRC suggest that MLT should be used in therapeutic concentrations rather than its physiological concentrations, which lack sufficient protection of cells from the toxic effects of CTx. 99 So far, most of these studies were performed in vitro, lacking confirmation in vivo.
In vitro studies
In vitro studies evaluating MLT synergistic effects with anti-cancer drugs in CRC treatment are compiled in Table 3. It seems that addition of MLT increased the specific cytotoxicity of anti-cancer drugs, including doxorubicin, irinotecan, cisplatin, oxaliplatin, and 5-fluoruracil (5-FU), on different CRC cell lines, including drug resistant cells.52,53,99–107 However, MLT was not effective in inducing DNA damage in healthy human cells. The main mechanisms suppressing tumor growth, proliferation, and tumor-mediated angiogenesis include (a) apoptosis activation through simultaneous modulation of cytochrome c/caspase, matrix metallopeptidase 9 (MMP9)/cyclooxygenase 2 (COX-2), and p300/NF-κB signalling pathways 107 ; (b) suppression of phosphatidylinositol 3-kinase (PI3K)/protein kinase B (AKT) and nuclear factor kappa B (NF-κB)/inducible nitric oxide synthase (iNOS) signalling pathways 101 ; and (c) and downregulation of PrPC.52,53
Summary of in vitro studies investigating the synergistic effect of MLT combined with anti-cancer drugs in CRC treatment.
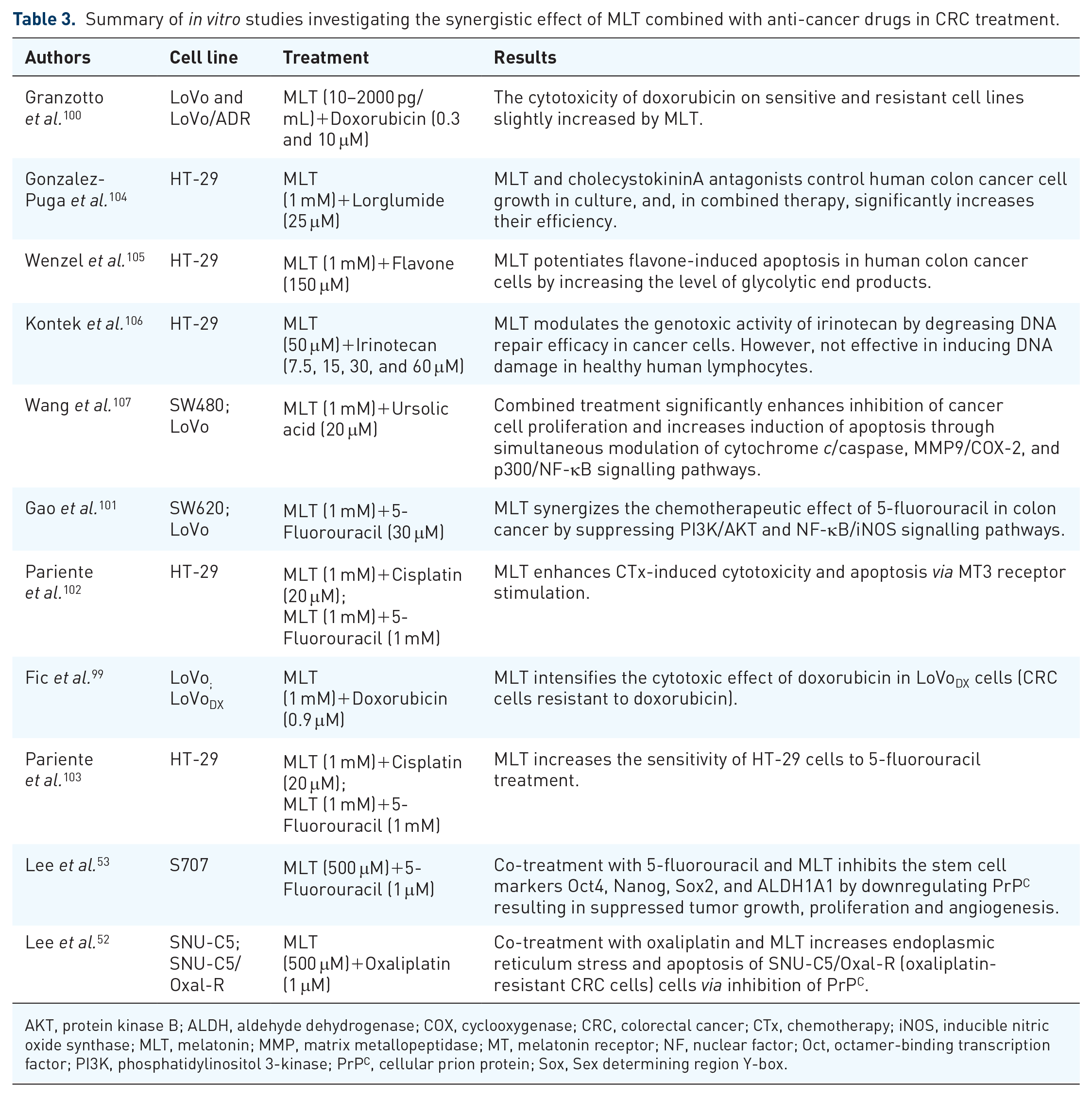
AKT, protein kinase B; ALDH, aldehyde dehydrogenase; COX, cyclooxygenase; CRC, colorectal cancer; CTx, chemotherapy; iNOS, inducible nitric oxide synthase; MLT, melatonin; MMP, matrix metallopeptidase; MT, melatonin receptor; NF, nuclear factor; Oct, octamer-binding transcription factor; PI3K, phosphatidylinositol 3-kinase; PrPC, cellular prion protein; Sox, Sex determining region Y-box.
In vivo studies
There are a limited number of in vivo studies evaluating the synergistic effects of MLT combined with anti-cancer drugs in CRC treatment (Table 4). Authors found that octreotide and MLT administered separately exert antiproliferative and proapoptotic effects on CRC in a murine model; however, combination of substances did not show additive effects. 108 Recently, Bakalova et al. investigated the anticancer effect of MLT in combination with active irinotecan metabolites in a murine model of CRC. 73 This combined treatment reduced tumor volume by decreasing oncogenic and increasing onco-suppressive ROS in tumor tissue. However, the small sample size of the study limits its explanatory power.
Summary of in vivo studies investigating the synergistic effect of MLT combined with anti-cancer drugs in CRC treatment.
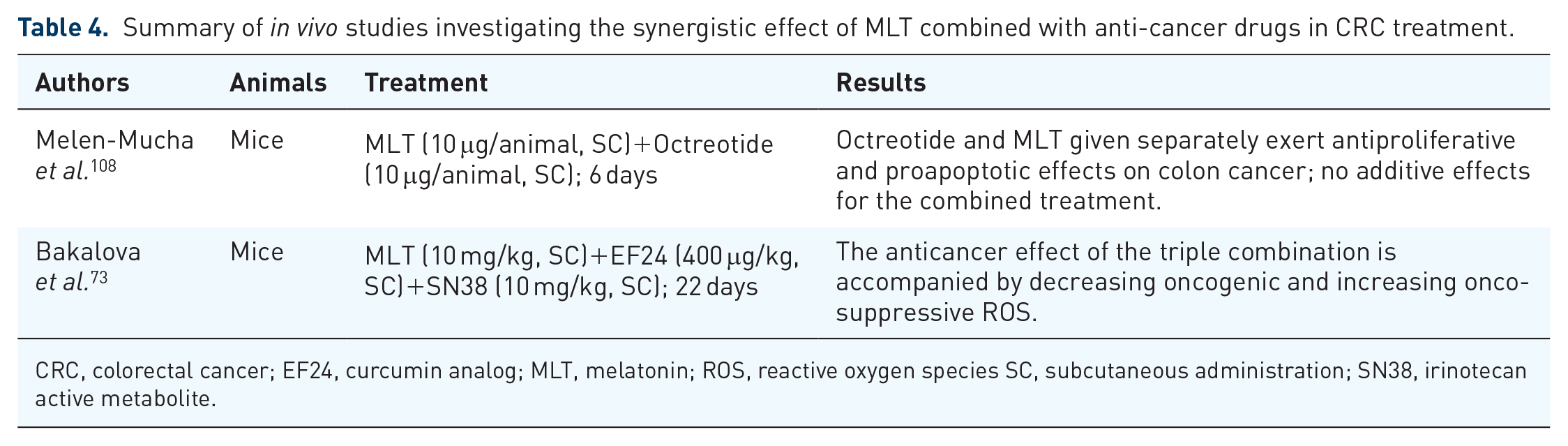
CRC, colorectal cancer; EF24, curcumin analog; MLT, melatonin; ROS, reactive oxygen species SC, subcutaneous administration; SN38, irinotecan active metabolite.
Clinical studies
The first controlled clinical trial to evaluate the effects of MLT on cancer was published in 1987 by Lissoni et al. 109 A total of 19 patients suffering from advanced solid tumors, including CRC, not responding to standard therapies, were included in the study. MLT was administered intramuscularly at a daily dose of 20 mg, followed by a maintenance period with lower MLT doses in patients with remission, a stabilization of disease or an improvement in performance status. MLT induced an amelioration of the performance status score and the quality of life in 60% patients. This preliminary study suggested a promising effect of MLT in treatment of cancer patients not responding to standard anti-cancer therapies. 109
In 1990, Barni et al. evaluated the therapeutic activity of the pineal hormone MLT in patients with metastatic CRC who did not respond to 5-FU treatment. 110 MLT was administered intramuscularly at a daily dose of 20 mg for 2 months, followed by daily oral administration of 10 mg. An evident improvement in performance status was seen only in 5 out of 14 (36%) patients. The results indicated a lack of antitumor activity for MLT in metastatic CRC patients resistant to 5-FU treatment.
Promising synergistic anti-cancer effects of MLT and IL-2 have been demonstrated in a study including 35 patients with various tumors, that is, CRC, gastric cancer, hepatocellular carcinoma, or pancreas adenocarcinoma. 111 Oral administration of 50 mg MLT daily started 7 days prior to IL-2 administration, resulting in an overall response rate of 23%. Another study suggested that preoperative neuro-immunotherapeutic treatment with low-dose IL-2 and MLT (40 mg/day) is a well-tolerated therapy, able to prevent surgery induced lymphocytopenia in cancer patients. 112 A decline in lymphocyte number greater than 30% occurred in 8/10 control patients, but only in 1/10 treated with IL-2 and MLT.
A large clinical study in 2002 included 1440 patients with untreatable advanced solid tumors (279 patients with CRC), receiving supportive care alone or supportive care in combination with MLT to investigate the effect of MLT on cancer. 113 The second part of this study, evaluated the influence of MLT on the efficacy and toxicity of CTx in 200 metastatic patients with CTx-resistant tumors (51 patients with CRC). CTx regimen consisted of 5-FU with folinic acid (FA) or raltitrexed. Additionally, MLT (20 mg/day) was administered orally during the night. The results led to the assumption that MLT may be effective in the prevention of cancer progression-related symptoms, such as cachexia, asthenia, and lymphocytopenia, and CTx-induced toxicity, such as thrombocytopenia, asthenia, and neurocardiotoxicity. Moreover, the study revealed synergistic effects of MLT in combination with anti-cancer drugs.
Cerea et al. evaluated the influence of a concomitant administration of MLT on irinotecan therapeutic activity in metastatic CRC. 114 The study included 30 metastatic CRC patients progressing after at least one previous chemotherapeutic line containing 5-FU. After randomization, MLT was administered orally at 20 mg/day during the night. The percent of disease-control achieved in patients concomitantly treated with MLT was significantly higher than that observed in those treated with CTx alone, at 85.7% and 43.8%, respectively.
More recently, a study randomized 370 cancer patients to receive CTx treatment alone or CTx combined with orally administered MLT (20 mg/day). 14 CRC patients accounted for one-third of the study population (122 patients) treated by oxaliplatin plus 5-FU and FA, or 5-FU and FA or weekly irinotecan. The overall tumor regression rate was significantly higher, and 2-year survival was significantly improved in patients receiving CTx and MLT.
Clinical pharmacokinetics of MLT
Several administration regimens for MLT have been investigated, but it is not yet clear which regimen results in the optimal pharmacologic effect. A systematic review by Harpsoe et al., including 22 studies with 359 volunteers/patients, provided important insights concerning the pharmacokinetics of exogenously administered MLT. 115 This review documented a time to maximal plasma/serum concentration (Tmax) of approximately 50 min following oral immediate-release formulations of MLT. The half-life time of oral and intravenous MLT was about 45 min (ranging from 28 to 126 min). Bioavailability after oral administration was generally low (ranging between 9 and 33%) with significant intra-individual variability. It is proposed that the low bioavailability is caused by a considerable first-pass metabolism in the liver. 116 Another systematic review of experimental or clinical studies investigated the pharmacokinetics of alternative administration regimen for MLT. 117 In that review, intranasal administration demonstrated a higher bioavailability and Tmax compared with oral MLT, 55–94% and ranging from 2.5 to 7.8 min, respectively. Whereas the oral transmucosal regimen resulted in higher maximal plasma/serum concentrations with similar Tmax compared with oral MLT, transdermal administration of MLT yielded slow absorption and deposition of MLT in the skin. Since no side effects have been reported, MLT appears to be safe for daily doses up to 100 mg/kg.69,118 However, most of the studies included primarily young healthy volunteers, whereas previous studies indicated that the pharmacokinetics of MLT is affected by age, health status, and external factors, such as caffeine intake, cigarette smoking, and the use of oral contraceptives.22,119,120
Conclusion
The effects of MLT alone and in combination with anti-cancer regimen have been studied in vitro and in vivo including animal models and clinical trials. Clinical trials focus mainly on advanced cancer patients, but the best MLT administration regimen for CRC treatment is still unknown and needs further research. To deepen the knowledge about the effects of MLT in CRC treatment, animal experiments to evaluate clinically important application regimen of MLT for treatment of complex CRC and CRLM are mandatory. This will pave the way for further clinical studies probably answering the question about the optimal application regimen for MLT.
In summary, there is sufficient evidence that MLT is involved in carcinogenesis, development, and progression of CRC cells by different mechanisms. Thus, further clinical trials are warranted to include MLT as a new promising therapeutic agent for CRC treatment.