
Abstract
Background:
The association between the survival or efficacy of chemotherapy and the Lauren subtype of gastric cancer (GC) remains unclear. We aimed to clarify whether patients with different Lauren subtypes have different survival after treatment with systemic chemotherapy: intestinal gastric cancer (IGC) patients survived better than patients with mixed type gastric cancer (MGC) or diffuse gastric cancer (DGC) after treatment with systemic chemotherapy.
Patients & methods:
Relevant studies for the meta-analysis were identified through searching Pubmed, Embase, Cochrane and Ovid up to March 2020. We also included our own prospectively collected cohort of patients that were followed over a 10-year period. Sub-group and sensitivity analyses were also performed.
Results:
In our prospective cohort, the overall survival (OS) of IGC patients receiving systemic chemotherapy (chemoIGC) [median OS 5.01 years, interquartile range (IQR) 2.63–6.71] was significantly higher than that of DGC patients receiving the same chemotherapy (chemoDGC) (median OS 1.33 years, IQR 0.78–3.33, p = 0.0001). After adjusting for age, gender and cancer stage, there was a significant difference in OS in patients treated with chemotherapy based on the Lauren classification of GC {hazard ratio (HR) for OS of the IGC versus DGC 0.33, [95% confidence interval (CI), 0.17–0.65; p < 0.001]}. In the IGC patients, the adjusted HR associated with chemotherapy was 0.26 (95% CI, 0.12–0.56; p = 0.001), whereas the association was 0.64 (95% CI, 0.30–1.33; p = 0.23) in the DGC patient group.
In our meta-analysis, 33 studies comprising 10,246 patients treated with systemic chemotherapy (chemoIGC n = 4888, chemoDGC n = 5358) met all the selection criteria. While we accounted for much of the heterogeneity in these studies, we found that chemoIGC patients showed significantly improved OS [HR, 0.76 (95% CI, 0.71–0.82); p < 0.00001] when compared with similarly treated chemoDGC patients.
Conclusion:
Our results support the consideration of Lauren subtype when prescribing systemic chemotherapy for GC, particularly for MGC or DGC, which may not benefit from chemotherapy. Lauren classification should be considered to stratify chemotherapy regimens to GC patients in future clinical trials, with particular relevance to MGC or DGC, which is more difficult to treat with current regimens.
Summary of the article’s main point
Our analysis using primary data and 33 studies consisting of 10,246 patients showed that diffuse gastric cancer (DGC) patients do not benefit from systemic chemotherapy as much as intestinal gastric cancer (IGC) patients. This suggests decisions on administration of chemotherapy for gastric cancer (GC) patients should incorporate Lauren subtype.
Introduction
Gastric cancer (GC) is the fifth most common cancer and the third leading cause of cancer-related mortality worldwide. 1 It is most frequently identified at advanced stages and occurs with highest incidence in Eastern Asia, Central and Eastern Europe, and South America. 2 It has lowest prevalence in Northern America and parts of Africa. The prognosis of patients with GC continues to be poor, despite improved surgical and adjuvant treatment approaches, with a 5-year OS of less than 25%. 3
Surgery is considered to be the only potentially curative therapy for GC; however, even after curative gastrectomy, relapse rates remain in the range of 40–60%.4,5 There are some global differences in how local-regional GC is managed and treated. 6 In the United States (US) and some parts of Europe, perioperative chemotherapy is a preferred management approach. Adjuvant chemoradiation is considered if the surgical resection is performed upfront. However, in Asia, postoperative chemotherapy alone after D2 surgical resection is considered standard-of-care treatment. The prognosis of resectable as well as locally advanced GC is improved significantly by perioperative chemotherapy.4,7–9 Moreover, systemic chemotherapy has resulted in improvement of survival in patients with inoperable, recurrent or metastatic tumors. 10
Currently, the clinical or pathological stage of the tumor is the primary variable used in the decision to prescribe chemotherapy. However, it must be pointed out that the individual prognosis of GC patients varies significantly within the same stage, and OS is dependent on additional prognostic factors, 11 including Lauren classification. 12
The intestinal and diffuse subtypes of GC describe two histological entities identified by both World Health Organisation (WHO) and Lauren’s classification systems that differ with regard to epidemiology, pathogenesis, molecular characteristics, biological features, clinical behaviour and prognosis.12–15 Despite these apparent differences, different Lauren subtypes are currently treated in equivalent ways with no difference in the choice of chemotherapy.16,17
A previous study performed in our laboratory examined relapse patterns after curative surgery in IGC, MGC and DGC patients and found that Lauren subtypes may be predictive of response to fluoropyrimidine-based chemotherapeutics, with lower response rates to chemotherapy seen in DGC. 18 This suggested that different Lauren subtypes should be treated as separate entities when given systemic chemotherapy.
To date there have been no meta-analyses being performed to evaluate the association between the survival or efficacy of systemic chemotherapy and the Lauren subtypes of gastric cancer, although there are some meta-analyses generally mentioning the survival benefit of chemotherapy after surgery irrespective of Lauren subgroup. 19 or clarifying the prognostic value of Lauren’s classification in GC patients. 12 These do not go far enough in determining whether chemotherapeutic response may be different in Lauren subtypes.
Therefore, we performed a systematic review and meta-analysis to elucidate the association between survival after systemic chemotherapy and the Lauren subtypes of GC with a specific focus on systemic adjuvant chemotherapy (ACT) and palliative chemotherapy (PCT). We compared the overall survival (OS) of intestinal GC (IGC) with diffuse GC (DGC) or mixed type GC (MGC) with DGC after chemotherapy.
Subjects and methods
Molecular analysis of upper gastrointestinal cancer cohort
Ethics statement
Ethical approval for the study was obtained from the Institutional Review Boards of individual hospitals involved (Peter MacCallum Cancer Centre, St Vincent’s Hospital, Royal Melbourne Hospital and Western Health, Box Hill Hospital, Cabrini Hospital). Written informed consent was obtained from study participants, who were identified prior to surgery by study investigators. Overarching approval for the tissue banking cohort and this study is from the Peter MacCallum Cancer Centre Ethics Committee.
All intestinal and diffuse patients in our Molecular Analysis of Upper Gastrointestinal Cancer (MAUGIC) cohort who would routinely be treated with curative intent and prescribed adjuvant therapy and had complete follow-up information were included in this analysis (IGC subgroup = 64, DGC subgroup = 49). The description of patients and clinical information has been described previously. 18 We compared the OS between chemoIGC and chemoDGC patients using Kaplan–Meier survival curves. The OS between patients who received or did not receive chemotherapy for each subgroup was also compared. Pathological assessment of all cases was conducted by central review, and each case was reported by at least two pathologists. Multivariable Cox regression was performed to adjust for confounders (cancer stage, patient age and gender). The Kaplan–Meier survival curves were generated using GraphPad Prism 5 and comparisons made by log-rank test. Cox regression analyses were performed using SPSS 16·0.
Systematic review and meta-analysis
Protocol and registration
The preplanned protocol of our network meta-analysis was documented online on 19 February 2018 [PROSPERO registration number: CRD42018088979]. Detailed registration information can be found on the website of http://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018088979.
Data sources
A systematic review and meta-analysis was performed in accordance with PRISMA guidelines. A comprehensive search of all relevant studies in Pubmed, Embase, Cochrane and Ovid database up to March 2020 was performed using the following keywords in combination: gastric, stomach, adenocarcinoma, cancer, tumour, neoplasm, Lauren, classification, type, intestinal, diffuse, mixed, survival or survive or prognosis or prognostic or outcome. A total of 10,649 studies were identified. After removal of duplicates and studies that did not fulfil the inclusion criteria, 33 studies remained and the data were extracted.18,20–51 Two reviewers (KNW and AB) performed the search and data extraction independently and any discrepancy in the inclusion of a study or in data extraction was reviewed independently by JAS.
Study selection
A concise search was performed based on specific keywords and the combinations of steps performed to derive the list of abstracts and titles for review before full text review. Abstracts, figures and tables of 2968 records were screened by two reviewers (KNW and AB), and 463 studies were selected for full-text review. Records were included with survival probabilities (⩾5 years survival) or hazard ratio (HR) for IGC or MGC or DGC after systemic chemotherapy. The inclusion and exclusion criteria can be found below. The flowchart is shown in Figure 1.

PRISMA flowchart of overview of records search and selection.
Inclusion criteria
Records with survival (⩾5 years survival) or HR and Lauren in the abstracts, figures or tables;
Records with ‘chemo’ in the abstracts, figures or tables;
Records with full text.
Exclusion criteria
No survival, no HR, no Lauren in the abstracts, figures or tables;
Records with less than 5 years survival, for example, 2 years survival, 1 year survival, etc.;
No full text;
Records without survival or HR information related to ‘chemo’ or ‘adjuvant’ or ‘postoperative’ or ‘palliative’ or ‘perioperative’ or ‘neoadjuvant’ for IGC and DGC in the abstract or tables or figures;
Records only with intraperitoneal chemo;
Records without detailed chemotherapy information for IGC or DGC (including case number of chemotherapy, survival after chemotherapy for IGC and DGC, or HR after chemotherapy for IGC and DGC);
Records without OS.
Data extraction and meta-analysis
Agreed electronic dataset criteria were developed to ensure that all data pertinent to this study were collected. These include author, publication year, country of recruitment, number of centres, study design, number of total patients, intestinal cases and diffuse cases, gender, age, length of follow up, primary tumour site, American Joint Committee on Cancer (AJCC) stage, type of chemotherapy, chemotherapy regimen, survival probability or HR in terms of OS. Two reviewers (KNW and AB) performed the search and data extraction independently and any discrepancy in the inclusion of a study or in data extraction was independently reviewed by JAS. In each study, OS was extracted directly or indirectly as HR with corresponding 95% CI. OS was defined as the time from surgery to death from any cause.
The study-specific HRs were pooled using a random-effects model. Between-study heterogeneity was assessed using the I2 statistic and interpreted as: 0–30%, minimal; 30–60%, moderate; 60–90%, substantial; and 90–100%, considerable heterogeneity. The Newcastle-Ottawa scale (NOS) was used for assessing the quality of non-randomised studies in this meta-analysis, where a score of ⩾6 represents good quality. Quality of randomised studies in this meta-analysis was assessed according to the Cochrane reviewers’ handbook 5·3. The quality of the 33 included studies was assessed.18,20–51
The differences in survival of MGC comparing with DGC were explored in five eligible included studies with detailed chemotherapy information for not only IGC and DGC, but also for MGC (including mixed subtype case number of chemotherapy, survival after chemotherapy for mixed subtype, or HR after chemotherapy for mixed subtype).18,25,29,38,49
Subgroup meta-analyses and sensitivity analyses were also performed to account for the existing heterogeneity. To evaluate the publication bias risk for the 33 included studies,18,20–51 funnel plots were evaluated and Trim-and-Fill-adjusted analysis was calculated. All meta-analyses were performed using Revman version 5.3.
Subgroup meta-analyses were performed according to type of chemotherapy (ACT versus PCT versus NAC), type of study [retrospective versus prospective versus randomised controlled trial (RCT)], ethnic groups (Asian versus non-Asian), length of follow up (>5 years versus ⩽5years), primary tumour site: percent of proximal tumour (>40% versus ⩽40%), AJCC stage (AJCC staging 7th Edition): ratio of I–III to IV (⩾1:1 versus <1:1) and treatment regimens [Capecitabine versus S-1 versus Taxanes-based or fluoropyrimidine (5-FU) only versus platinum and fluoropyrimidine (PF) only].
Moreover, sensitivity analyses was performed. We extracted 23 studies of good quality (NOS above score 7 or quality level A) and performed meta-analysis to determine whether the quality of the studies were influencing our results.20,22–26,28–35,37,40–42,45,46,49–51 Additionally, Trim-and-Fill-adjusted analysis was calculated to investigate publication bias for the 33 studies.18,20–51
Results
Study design and quality
A total of 33 studies,18,20–51 including data from our MAUGIC cohort, 18 met the inclusion and exclusion criteria, with an overall patient number of 10,246, of which 4888 were included in the IGC group treated with systemic chemotherapy (chemoIGC) and 5358 were DGC patients treated with systemic chemotherapy (chemoDGC). Patients in 13 studies18,23,24,29,31,32,34,37,40,41,46,49,50 received adjuvant chemotherapy (for curative intent), patients in another 13 studies20–22,25–27,33,35,38,44,45,48,51 received PCT (for inoperable or metastatic disease) and patients in 7 studies28,30,36,39,42,43,47 received perioperative chemotherapy – neoadjuvant chemotherapy (NAC). Since we did not find any perioperative chemotherapy (three cycles preoperatively and three cycles postoperatively) study that met all the inclusion criteria, we included seven NAC studies that met all the inclusion criteria. The major characteristics of all the included studies with HRs for OS are shown in Table 1.
Characteristics of all the included studies (HR for OS).

Type of study: # Retrospective analysis from prospectively collected data. Primary tumor site: The primary tumour site was categorized as proximal if the bulk of the tumor (more than 80%) was located in the gastric cardia with possible extension up to the gastroesophageal junction and a small portion of the distal oesophagus (including Fundus); Distal means the primary tumor site was in the mid body of the stomach or down to the pylorus. Proximal cases%: percentage of proximal cases. Ratio of I–III to IV: number of cases of AJCC stage I and II to number of cases of AJCC stage III and IV; AJCC staging 7th Edition. Type of chemotherapy.
ACT, adjuvant chemotherapy; AJCC, American Joint Committee on Cancer; DGC, number of diffuse gastric cancer cases; 5-FU based, fluoropyrimidine based chemotherapy regimens; HR, hazard ratio; HR for OS (IGC/DGC) or HR for OS (MGC/DGC), hazard ratio in terms of overall survival, DGC was reference; IGC, number of intestinal gastric cancer cases; LCI, lower 95% confidence intervals; MAUGIC, Molecular Analysis of Upper Gastrointestinal Cancer; MGC, number of mixed type gastric cancer cases; NAC, neoadjuvant chemotherapy; OS, overall survival; PCT, palliative chemotherapy; PF-based, platinum and fluoropyrimidine based chemotherapy regimens; UCI, upper 95% confidence intervals.
In seven publications,18,20,22,32,38,41,48 findings from a prospective database were presented. There were 16 retrospective studies,21,24,26,27,29,31,33–35,37,40,45,46,49–51 1 prospective observational study, 23 1 pooled analysis of 2 phase III trials, 44 and 1 RCT. 25 All non-randomized studies, when assessed for quality, were assigned NOS >6 and the randomized study, assessed according to the Cochrane reviewers’ handbook 5.3, scored A (low risk of bias); thereby, all studies were deemed good quality (online supplemental appendix pp. 2).
OS of Lauren subtypes after chemotherapy in the MAUGIC cohort
We compared OS between the Lauren subtypes treated with systemic chemotherapy (chemoIGC and chemoDGC) in the MAUGIC cohort. As shown in Figure 2A, the OS of chemoIGC [median OS 5.01 years, interquartile range (IQR) 2.63–6.71] was significantly higher than that of chemoDGC (median OS 1.33 years, IQR 0.78–3.33; p = 0.0001). The HR for OS of the chemoIGC versus chemoDGC was 0.26 (95% CI, 0.13–0.52; p = 0.0001). The OS between the GC treated with chemotherapy (chemoIGC or chemoDGC) and GC cases not treated with chemotherapy (nochemoIGC or nochemoDGC) was also compared. There was a significant difference in the OS between chemoIGC (median OS 5.01 years, IQR 2.63–6.71) and nochemoIGC (median OS 3.44 years, IQR 1.06–5.25; p = 0.0012) with HR 0.32 (95% CI, 0.16–0.64; p = 0.0012), whereas there was no difference in OS between chemoDGC (median OS 1.33 years, IQR 0.78–3.33) and nochemoDGC (median OS 1.68 years, IQR 1.20–5.09; p = 0.46) with HR 1.26 (95% CI, 0.69–2.29; p = 0.46), as shown in Figure 2B and C, indicating that IGC patients benefit more than DGC patients from chemotherapy, and that DGC may not achieve benefit from the same chemotherapy used.

OS of Lauren subtypes after chemotherapy in the MAUGIC cohort.
These findings remained significant after controlling for stage of cancer, Lauren subtype, patient age and sex (Table 2). The adjusted HR for OS of the chemoIGC versus chemoDGC was 0.33 (95% CI, 0.17–0.65; p < 0.001). In the IGC patients, the adjusted HR associated with chemotherapy was statistically significant at 0.26 (95% CI, 0.12–0.56; p = 0.001), whereas the association was not significant at 0.63 (95% CI, 0.30–1.33; p = 0.23) in the DGC patient group.
Multivariable Cox regression analyses of potential poor prognostic factors in GC in the MAUGIC cohort.

AJCC, American Joint Committee on Cancer; CI, confidence interval; chemoDGC, DGC patients receiving adjuvant chemotherapy; chemoIGC, IGC patients receiving adjuvant chemotherapy; DGC, diffuse gastric cancer patients; HR, hazard ratio; IGC, intestinal gastric cancer patients; MAUGIC, Molecular Analysis of Upper Gastrointestinal Cancer; N/A, not available; nochemoDGC, diffuse gastric cancer patients receiving no chemotherapy; nochemoIGC, IGC patients receiving no chemotherapy.
Meta-analysis of OS
The differences in survival after chemotherapy by IGC and DGC were evaluated by comparison of OS between chemoIGC and chemoDGC in all 33 studies, comprising a total of 10,246 patients analysed (chemoIGC n = 4888, chemoDGC n = 5358). The pooled HR was 0.76 (95% CI, 0.71–0.82; p < 0.00001; I2 71%), indicating that IGC patients survive longer after chemotherapy compared with DGC patients (Figure 3).

Meta-analysis of OS (all 33 studies).
The differences in survival of MGC comparing with DGC were explored in five eligible included studies, 18,25,29,38,49 with detailed chemotherapy information for not only IGC and DGC, but also for MGC (including mixed subtype case number of chemotherapy, survival after chemotherapy for mixed subtype or HR after chemotherapy for mixed subtype). The pooled HR of MGC versus DGC was 0.94 (95% CI, 0.73–1.21; p = 0.63; I2 49%); meanwhile, the pooled HR of IGC versus DGC was 0.74 (95% CI, 0.55–0.98; p = 0.04; I2 71%). The results showed that IGC patients had best improved OS, MGC better and DGC worst after systematic chemotherapy. However, there is no significant difference in OS between MGC and DGC patients after systematic chemotherapy (Figure 4).
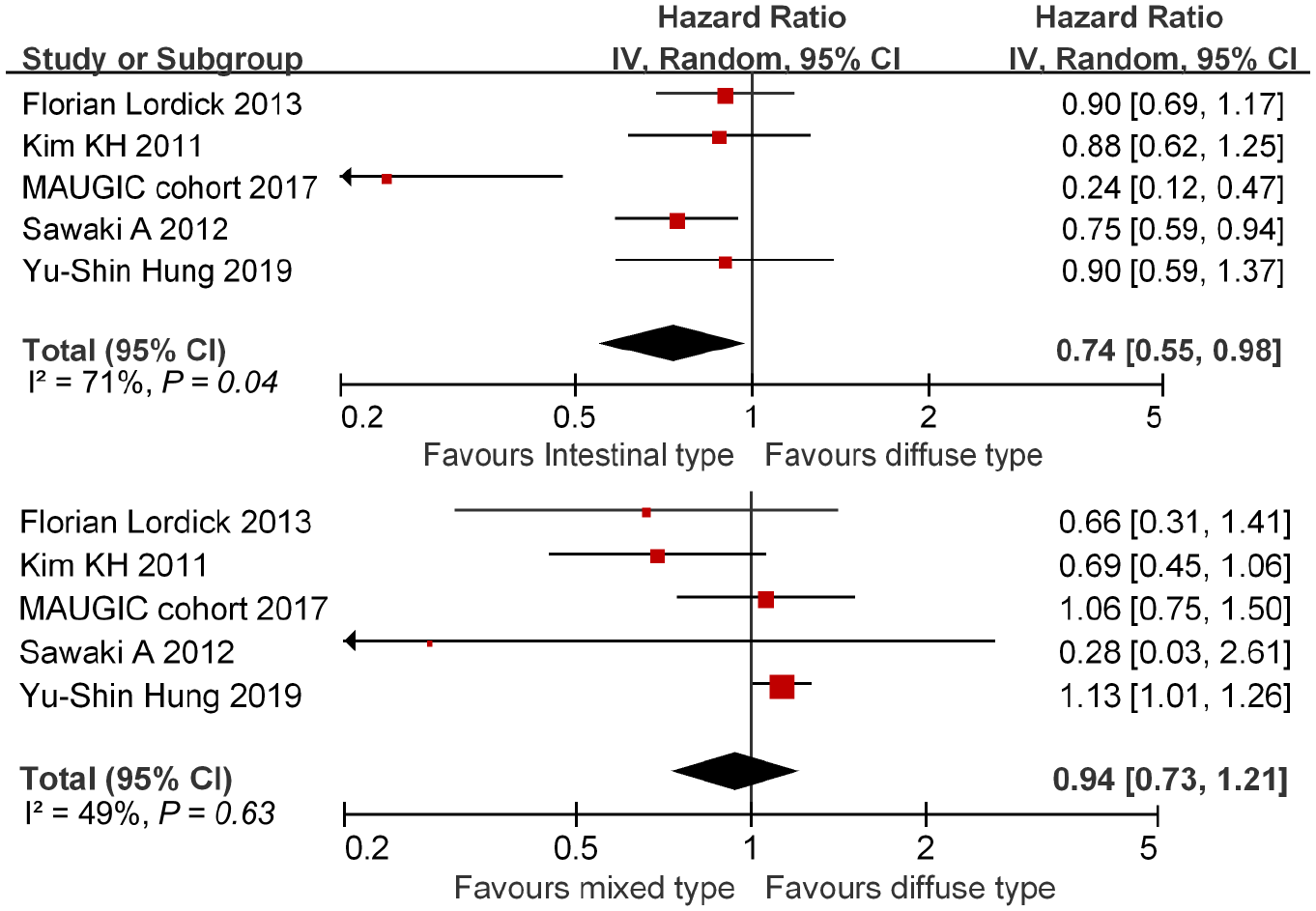
Differences in survival of IGC versus DGC and MGC versus DGC after systematic chemotherapy.
Subgroup analyses
A number of clinical and etiological factors may contribute to patient survival after chemotherapy and were explored in subgroup analyses. Importantly, subgroup meta-analysis was performed according to type of chemotherapy (adjuvant versus palliative versus perioperative). Since we did not find any perioperative chemotherapy (three cycles preoperatively and three cycles postoperatively) study that met all the inclusion criteria, we included seven NAC studies that met all the inclusion criteria. Patients in seven studies received perioperative chemotherapy–NAC. 28,30,36,39,42,43,47 Patients with IGC consistently survive longer after treatment with ACT [HR, 0.72 (95% CI, 0.61–0.86; p = 0.0002)], PCT [HR, 0.82 (95% CI, 0.77–0.88; p < 0.00001)] and NAC [HR, 0.50 (95% CI, 0.32–0.77; p = 0.002)] compared with DGC patients, as shown in Figure 5.

Subgroup meta-analysis forest plot according to type of chemotherapy, with 13 studies assessing OS of IGC versus DGC after ACT (I2 = 69%, p = 0.0002); 13 studies assessing OS of IGC versus DGC after PCT (I2 = 26%, p < 0.00001); and 7 studies assessing overall survival of IGC versus DGC after NAC (I2 = 76%, p = 0.002). The closed circles and horizontal lines correspond to study-specific HR and 95% CI. The diamond marker represents the pooled HR and 95% CI, derived using random-effects model.
Subgroup meta-analysis was also performed according to type of study (retrospective versus prospective versus RCT). Patients with IGC consistently survive longer after chemotherapy in retrospective studies [HR, 0.92 (95% CI, 0.90–0.94; p < 0.00001)], studies of prospective data [HR, 0.86 (95% CI, 0.75–0.98; p = 0.02)] and studies of RCT [HR, 0.87 (95% CI, 0.75–1.00; p = 0.05)] compared with DGC patients, as shown in Figure 6.

Subgroup meta-analysis forest plot according to type of study.
Importantly, chemotherapy drugs were stratified and subgroup meta-analysis was analysed according to treatment regimens used (Capecitabine versus S-1 versus Taxanes-based or 5-FU only versus PF only). Chemotherapy regimens of each included study are shown in Table 1. Since some studies used several chemotherapy regimens, it may be difficult to stratify the drugs accurately. As shown in Figure 7, the results indicated that IGC patients consistently had improved survival comparing with DGC patients using Capecitabine [HR, 0.83 (95% CI, 0.70–0.99; p = 0.03)] or S-1 [HR, 0.77 (95% CI, 0.60–0.98; p = 0.03)] or Taxanes-based [HR, 0.84 (95% CI, 0.80–0.88; p < 0.00001)] or 5-FU only [HR, 0.65 (95% CI, 0.44–0.94; p = 0.02)] or PF only regimens [HR, 0.80 (95% CI, 0.68–0.93; p = 0.004)].

Subgroup meta-analysis forest plot according to regimens (Capecitabine or S-1 or Taxanes-based or 5-FU only or PF only).
We also conducted analyses of other clinical relevant subgroups and the forest plots of these subgroup analyses are shown in online supplemental appendix (pp. 4–7). In all the subgroup analyses, patients with DGC have consistently less benefit from existing chemotherapy regimens irrespective of ethnicity, time of follow up, primary tumour site, AJCC stage, type of chemotherapy, type of study or type of chemotherapy regimens used (Capecitabine or S-1 or Taxanes-based or 5-FU only or PF only) as shown in Table 3.
Comparison of OC in GC of different Lauren types after chemotherapy.

Studies were excluded if they did not contain information for each subgroup. In studies selected for Ethnic groups (Asian versus Non-Asian countries), only one study (Lordick et al.) not included for mixed origins. 25 Primary tumor site: The primary tumor site was categorized as proximal if the bulk of the tumor (more than 80%) was located in the gastric cardia with possible extension up to the gastroesophageal junction and a small portion of the distal oesophagus (including Fundus); Distal means the primary tumor site was in the mid body of the stomach or down to the pylorus. Ratio of I-III to IV: number of cases of AJCC stage I, II and III to number of cases of AJCC stage IV; AJCC staging 7th Edition.
ACT, adjuvant chemotherapy; AJCC, American Joint Committee on Cancer; CI, confidence interval; 5-FU, fluoropyrimidine; HR, hazard ratio; HR for OS, hazard ratio in terms of OS, DGC was reference; PF, platinum and fluoropyrimidine. NAC, neoadjuvant chemotherapy; OS, overall survival; PCT, palliative chemotherapy; RCT, randomised controlled trial.
Sensitivity analyses
To determine whether the quality of the studies was influencing our results, we extracted 23 studies objectively assessed as higher quality (NOS above score 7 or quality level A) and performed meta-analysis.20,22–26,28–35,37,40–42,45,46,49–51 These studies were analysed for OS (online supplemental appendix pp. 8) and the result was compared with the results of all 33 studies in Figure 3. The result indicated IGC benefits more from chemotherapy compared with DGC, with a HR of 0.92 (95% CI, 0.90–0.94; P < 0.00001). This was consistent with the results of analysis including all 33 studies [HR, 0.76 (95% CI, 0.71–0.82; p < 0.00001)], suggesting that the quality of the studies did not influence the primary outcomes.
When we performed sensitivity analyses using the Trim-and-Fill-adjusted method, six studies were found with larger bias.18,36,39,43,47,49 After removing them, the heterogeneity reduced, with I2 6%, but the overall result remained unaltered [HR, 0.83 (95% CI, 0.80–0.86; p < 0.00001)] (online supplemental appendix pp. 9).
Given the potential publication bias observed by Begg’s funnel plot (online supplemental appendix pp. 10), we calculated the Trim-and-Fill-adjusted analysis. We removed three studies with largest publication bias and performed the analysis again.18,36,49 The Begg’s funnel plot became more symmetrical (online supplemental appendix pp. 10); however, the overall result remained unchanged [HR, 0.78 (95% CI, 0.73–0.3; p < 0.00001)] with decreased heterogeneity as indicated by I2 decreasing from 71% to 34% (online supplemental appendix pp. 11).
Discussion
GC is most frequently discovered in advanced stages, 2 and systemic chemotherapy remains an important component of therapy for GC patients. Currently, decisions on the chemotherapy management of patients with GC is dependent mostly on prognostic assessment based on clinical and pathological stage, with little differentiation based on histological subgroups such as Lauren subtypes. Increasingly, with molecular profiling and the advent of targeted therapies including immune related therapies, there will be refinement to the management of this disease. Our study suggests this should incorporate Lauren classification to help tailor future therapies in GC.
The Lauren subtypes of GC differ with regard to epidemiology, pathogenesis, biological features, clinical behaviour, molecular characteristics and prognosis.13,15 DGC accounts for 32–40% of GC in our community and appears to be increasing in prevalence. 10 Intestinal-type cancers show recognizable gland formation similar in microscopic appearance to colonic mucosa, whereas diffuse-type cancers have non-cohesive tumor cells infiltrating the stroma of the stomach diffusely and often exhibiting deep infiltration of the stomach wall with little or no gland formation. 10 Despite these obvious differences, there is no difference in the choice of systemic chemotherapy for different Lauren subtype GC in clinical practice.16,17 Analysis of the MAUGIC cohort, 18 which is a unique cohort of GC patients of predominantly European ethnicity in Australia, found that the OS of patients with IGC treated with chemotherapy was significantly improved compared with those patients with DGC. This outcome could be due to innate poor prognosis of DGC rather than poor response to chemotherapy. We therefore analysed the benefit of chemotherapy within Lauren subgroups. IGC patients treated with chemotherapy had improved survival compared with IGC patients not treated with chemotherapy and matched for other clinical variables. However, there was no benefit of chemotherapy observed in DGC patients treated with chemotherapy compared with DGC patients that were not treated. This result suggests that the longer survival of chemotherapy-treated IGC compared with chemotherapy-treated DGC is not just because of the prognostic impact of Lauren classification, but due to differential response to chemotherapy by IGC and DGC.
To investigate whether this observation in a single cohort was generalizable to larger populations, we used a systematic review and meta-analysis approach to identify 33 studies. Meta-analysis of these studies found that IGC has greater benefit from systemic chemotherapy compared with DGC, with DGC patients having a 24% reduction in OS compared with IGC, suggesting that primary or secondary chemoresistance may be responsible for this difference in survival.
The differences in survival of MGC comparing with DGC were also explored in five eligible included studies with detailed chemotherapy information for not only IGC and DGC, but also for MGC (including mixed subtype case number of chemotherapy, survival after chemotherapy for mixed subtype, or HR after chemotherapy for mixed subtype).18,25,29,38,49 The results showed that IGC patients had best improved OS, MGC better and DGC worst after systematic chemotherapy. However, there is no significant difference of OS between MGC and DGC patients after systematic chemotherapy (Figure 4).
Sub-group analyses indicated that IGC, not MGC and DGC, would benefit from systemic chemotherapy and this was not influenced by ethnicity, duration of follow up, primary tumour site, AJCC stage, type of chemotherapy, type of study or type of chemotherapy regimens. Importantly, IGC, but not MGC and DGC, showed benefit from ACT, PCT and NAC.
Some studies suggest that histological heterogeneity correlates to sensitivity to different drugs.52,53 One study identified an acquired-resistance signature comprising genes related to cell survival, DNA repair, and embryonic stem cell biology in GC. 54 DGC, by its nature, is more mesenchymal-like and has features of stem cell attributes. DGC may be more inclined to chemoresistance and result in a worse survival than IGC after chemotherapy.
Previous studies have shown that DGC is associated with peritoneal translocation of malignant cells, which leads to malignant ascites. 13 Thus, intraperitoneal injection of chemotherapy represents a promising treatment option due to the enhancement of anti-tumor activity via gradual absorption through the lymphatic system. 55
The Lauren subtype of DGC was significantly enriched in the genomically stable subgroup of The Cancer Genome Atlas (TCGA) molecular characterization of GC, whereas tumors with chromosomal instability corresponded mostly with IGC. The RhoA pathway was a feature of the genomically stable subgroup, which was enriched with DGC. Notably, it was already shown that FGFR2 amplification is typical of DGC and RhoA activation mediated chemotherapy resistance in DGC,56,57 indicating that inhibition of FGFR2 or RhoA may play an effective role in DGC treatment. Moreover, drugs targeting the phosphatidylinositol 3-kinase-AKT-mTOR (PI3K-AKT-mTOR) pathway may be particularly effective against DGC, which is associated strongly with mesenchymal-subtype cancer. 58 Therapeutic strategies, targeting specific Lauren subtypes (particularly DGC) based upon their somatic genetic driver alterations or tumor microenvironment (e.g. stromal cells and tumor-infiltrating immune cells), remain to be developed. 59 There may be a role for immune checkpoint inhibitors for subgroups of DGC, where there is an active T cell immunity. Our overall impression is that more specific targeted therapies would be more efficacious in DGC and require more extensive clinical evaluation in prospective studies.
As this study was a meta-analysis, some limitations must be noted. The selection criteria limited article selection to those published in English and therefore non-English records were not included. Another limitation is the lack of prospective studies examining Lauren subgroup, hence the presence of heterogeneity that arose from: studies using adjuvant chemotherapy; studies using palliative chemotherapy; studies using perioperative chemotherapy; retrospective registry studies and; only one randomized controlled study. There is a paucity of prospective controlled data that incorporates Lauren classification in de novo design of studies rather than post hoc analysis. We analysed all studies including ACT, PCT and perioperative chemotherapy together as shown in Figure 3, but, importantly, performed separate subset analysis according to type of chemotherapy (adjuvant or palliative or perioperative) as shown in Figure 5. These issues led to the observed heterogeneity of studies, which we incorporated in our analysis. The I2 of the analyses in our study with three studies with largest publication bias removed was 34%,18,36,49 and the I2 was 6% after six studies with larger bias removed,18,36,39,43,47,49 suggesting minor influence of heterogeneity in our findings. What is more, we performed subgroup analyses, sensitivity analyses, Trim-and-Fill-adjusted analysis, etc., to reduce the heterogeneity in our study.
While our own cohort (MAUGIC cohort) was collected prospectively and included individual data, a limitation of the meta-analysis is that individual patient data was not available for the other studies. Histological assessment of the Lauren subtype has been described for over 50 years based on Lauren’s criteria, which were introduced in 1965 and remain currently widely accepted and employed, since they constitute a simple and robust classification. 13 The lack of individual patient data in a meta-analysis makes control of histological assessment in each study difficult. We cannot exclude the possibility of biased reporting of subtype due to lack of a standard approach to pathological reporting (e.g. where assessment was based on whole tissue sections or tissue microarrays). 60 Our prospective cohort had central pathology reporting and consensus for any ambiguity but we cannot attest to this in the studies included in the meta-analysis other than where stipulated by the authors. Given the experience of gastrointestinal pathologists in histological assessment of GC, this would be an unexpected confounder.
Our study did not specifically address the role of radiation therapy. Patients of three studies also received radiotherapy in the adjuvant setting,18,31,34 which may be a confounder for the survival of different Lauren subtypes after chemotherapy. The role of radiation therapy in this disease remains to be determined, and there are ongoing clinical trials to address this issue.
The major strengths of this study are: the inclusion of a prospective cohort study; comprehensive search strategy – selection and incorporation of all available records strictly refined to our inclusion and exclusion criteria; careful quality assessment of the included studies; subgroup analyses to assess if the observed association was maintained across different patient groups; and the use of OS as the outcome, which is recognized widely as the best efficacy endpoint in cancer. Furthermore, a sensitivity analysis adjusting for quality assessment score (keeping 23 studies of higher quality level) did not alter the conclusion of the study.20,22–26,28–35,37,40–42,45,46,49–51 Moreover, the trim-and-fill procedure found that, after removal of three studies with potential publication bias,18,36,49 or six studies with larger bias,18,36,39,43,47,49 the heterogeneity reduced sharply (with I2 6%), but the conclusion that IGC has better outcomes than DGC after systemic chemotherapy remains unchanged.
There are another two important strengths of this study. There are geographical differences in the standard adjuvant treatment strategies for GC, such as postoperative chemoradiotherapy in North America, postoperative chemotherapy in Asia and perioperative chemotherapy in Europe. So the meta-analysis of our study included all eligible systematic chemotherapy studies including adjuvant, palliative and perioperative chemotherapy. Survival of different Lauren subtypes patients were compared in different chemotherapy setting to elucidate the response of Lauren subtypes toward chemotherapy to the full extent. Importantly, chemotherapy drugs were stratified and subgroup meta-analysis was analysed according to treatment regimens used (Capecitabine versus S-1 versus Taxanes-based or 5-FU only versus PF only) although it may be difficult to stratify the drugs accurately because some studies used several chemotherapy regimens.
It is notable to discuss results from analysis of the MAGIC trial, 61 which did not find any difference between the survival of IGC and DGC. One difference between our analysis and the MAGIC study was that the MAGIC investigators studied neoadjuvant chemotherapy whereas all the studies included in this meta-analysis examined postoperative adjuvant chemotherapy or palliative chemotherapy as shown in Figure 1. Moreover, the proportion of DGC (surgery group 20.0%, NAC plus surgery group 15.1%) patients in the MAGIC study was much lower than IGC (surgery group 72.5%, NAC plus surgery group 81.7%), 61 which is unusually different from the reported prevalence of DGC cases (32–40%) in the reported literature.18,62 The lower proportion of DGC in the MAGIC study may be because this study focussed on patients with resectable esophagogastric cancer not primarily non-cardia GC. 61 Therefore, comparison of our current study, which examines predominant non-cardia GC and the MAGIC cohort, 61 may not be appropriate to answer the question of chemotherapy outcomes between DGC and IGC.
The FLOT4 study is a very good new study related to perioperative chemotherapy, and we tried to include this study to our meta-analysis. 8 However, unfortunately, this study did not meet the inclusion criteria because the Lauren subtypes in this study were divided into Missing, Diffuse, and Non-diffuse (Non-diffuse type includes the intestinal type, mixed types, and types not evaluable according to Lauren) without intestinal subtype, and there is no specific OS or HR data in relate to each subtype. Since perioperative chemotherapy plays an important role in GC treatment in Europe, we also tried to include studies of perioperative chemotherapy.
It is a pity that there is no Lauren subtype and no perioperative chemotherapy survival or HR data related to each Lauren subtype, not only in the FLOT4 study but also in other perioperative studies.4,5,7,8,63–78 As a result, we could not extract the data and perform meta-analysis for perioperative studies. However, it is worth mentioning that some papers, which are related to perioperative chemotherapy in different Lauren subtype of GC, indicated that IGC patients may benefit more from perioperative chemotherapy. A study 79 reported that preoperative chemotherapy patients with intestinal histology have a longer OS than patients with a diffuse histology. A multicenter phase II study of perioperative chemotherapy in GC mentioned a very good response predominantly in patients with intestinal type tumours comparing with diffuse and mixed type tumors, and intestinal type tumour showed a significantly longer OS and an improved PFS compared with non-intestinal type tumour after perioperative chemotherapy. 80 Nils Homann et al. found that the pathological complete remission rate was highest in tumours of intestinal type histology (30.8%) and lowest in patients with diffuse/mixed type tumours (0%). 81 Al-Batran et al. found that the tumour regression grade was much better in IGC than in DGC after neoadjuvant chemotherapy with FLOT (fluorouracil, leucovorin, oxaliplatin, and docetaxel) or ECF (epirubicin, cisplatin, and fluorouracil). 67
Although we did not find any perioperative chemotherapy (three cycles preoperatively and three cycles postoperatively) study that met all the inclusion criteria, we included seven neoadjuvant chemotherapy studies that met all the inclusion criteria,28,30,36,39,42,43,47 and the results showed that patients with IGC also survive longer after treatment with NAC compared with DGC patients, as shown in Figure 5. This indicated that, no matter what kind of chemotherapy (ACT, PCT or NAC) is given, IGC patients consistently had improved survival comparing with DGC patients.
We focussed our approach using a systematic review and meta-analysis approach to validate our observation in our smaller prospectively collected cohort, 18 and found that patients with IGC have greater benefit from systematic chemotherapy (adjuvant, palliative or perioperative chemotherapy) compared with patients with DGC.
Conclusion
The principal finding of this study is that DGC patients do not benefit from systematic chemotherapy as much as IGC patients. To our knowledge, this is the first systematic review and meta-analysis to address this issue. Our finding supports the use of Lauren subtype as a simple, cost effective additional stratification factor in triaging GC patients for chemotherapy. We believe this finding supports consideration of Lauren subtype when prescribing systemic chemotherapy for DGC patients, given the apparent futility of treating DGC with current chemotherapy regimens. However, it is recognised this observation requires further prospective validation and should include specific molecular-targeted therapies, which are currently being investigated for DGC. We hope the evidence presented will help clinicians and patients make more informed decisions about the treatment of DGC, and provide further justification for future research.
Supplemental Material
Supplementary_Information_for_TAM – Supplemental material for A cohort study and meta-analysis of the evidence for consideration of Lauren subtype when prescribing adjuvant or palliative chemotherapy for gastric cancer
Supplemental material, Supplementary_Information_for_TAM for A cohort study and meta-analysis of the evidence for consideration of Lauren subtype when prescribing adjuvant or palliative chemotherapy for gastric cancer by Kunning Wang, Enxiao Li, Rita A. Busuttil, Joseph C. Kong, Sharon Pattison, Joseph J. Y. Sung, Jun Yu, Emad M. El-Omar, Julie A. Simpson and Alex Boussioutas in Therapeutic Advances in Medical Oncology
Footnotes
Author contributions
Conceptualization: Kunning Wang, Alex Boussioutas.
Data curation: Kunning Wang, Julie A Simpson, Alex Boussioutas.
Formal analysis: Kunning Wang, Enxiao Li, Joseph C. Kong, Julie A Simpson.
Investigation: Kunning Wang.
Project administration: Kunning Wang, Alex Boussioutas.
Resources: Kunning Wang, Sharon Pattison, Rita A. Busuttil, Alex Boussioutas.
Supervision: Alex Boussioutas.
Visualization: Kunning Wang.
Writing ± original draft: Kunning Wang.
Writing ± review & editing: Kunning Wang, Rita A. Busuttil, Sharon Pattison, Joseph J Y Sung, Jun Yu, Emad M El-Omar, Enxiao Li, Alex Boussioutas.
Comment on the study: Joseph J Y Sung, Jun Yu, Emad M El-Omar, Enxiao Li, Alex Boussioutas.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grant 81702421 from the National Natural Science Foundation of China (to Kunning Wang) and by China Scholarship Council (CSC) 201606285152.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.