
Abstract
Background:
Mesothelin is expressed at very low levels by normal mesothelial cells but is overexpressed in several human cancers. This makes mesothelin a promising target for immunotherapy. Limited data exist about mesothelin expression in esophageal carcinoma. In a current clinical trial, the highly potent anti-mesothelin antibody anetumab ravtansine is used in patients with mesothelin-positive tumors. Response rates are correlated with mesothelin expression (using the Ventana antibody) in tumor cells. No data are available on expression levels using the Ventana antibody. Most data have been generated using the Novocastra antibody. As patients are selected for clinical trials based on antibody staining of tumor samples, a comparison of these two available antibodies is crucial.
Methods:
We analyzed 481 esophageal carcinomas [373 esophageal adenocarcinomas (EACs), 108 esophageal squamous cell carcinomas (ESCCs)] using two different monoclonal antibodies (Novocastra and Ventana) for mesothelin expression (low–mid and high-level expression, as used in one clinical trial). We also checked for the correlation of these results with clinical and molecular data.
Results:
We revealed different staining results for both antibodies in EACs: Ventana: 53.6% (low expression: 25.3%; high expression: 28.3%) and Novocastra: 35.7% (low expression: 21.2%; high expression 14.5%). In ESCC we found comparable staining results: Ventana: 13.3% (low expression: 9.5%; high expression: 3.8%) and Novocastra: 13% (low expression: 11.1%; high expression: 1.9%). ARID1a-deficient EAC patients demonstrated significantly higher rates of mesothelin-positive tumors than ARID1a intact EAC patients. No correlations were found with other molecular alterations (TP53 mutation, ERBB2 amplification) or survival rates.
Conclusion:
To the best of our knowledge, this is the largest study analyzing the importance of mesothelin expression in esophageal carcinoma. This study revealed a significant number of mesothelin-positive esophageal carcinomas, especially adenocarcinomas. New therapeutic targets are urgently required to improve the outcome of patients with locally advanced or metastasized esophageal carcinoma. The inhibition of mesothelin can be a new attractive target.
Introduction
The incidence of esophageal adenocarcinoma has increased rapidly over the past few decades, mainly in the western world, both by period and birth cohort. 1 Despite improvements in perioperative treatments, the overall survival of patients with esophageal carcinoma remains low. The relative 5-year survival rate remains poor, with 21% in both sexes. 2
Mesothelin is a 40-kDa cell surface glycoprotein expressed at very low levels by normal mesothelial cells lining the pleura, peritoneum, and pericardium. 3 It was initially identified in 1992 by Chang et al. 4 The function of mesothelin is not yet completely clear, but in normal mesothelial cells, it seems to be involved in cell adhesion, cell differentiation, and signal transduction. 5 Normal esophageal mucosa does not express mesothelin.6,7 In cancer cells, mesothelin seems to be involved in the promotion of proliferation and cell migration, resistance to chemotherapy, and inhibition of apoptosis.8–10 Mesothelin overexpression has been described in several human cancers, including virtually all mesotheliomas and pancreatic adenocarcinoma, approximately 70% of ovarian and extra bile duct carcinomas, and 50% of lung and gastric adenocarcinomas.3,11–13
Limited data on mesothelin expression in esophageal carcinoma exist so far. Alvarez et al. analyzed 84 esophageal adenocarcinomas and found that approximately one third were positive for mesothelin using the Novocastra antibody. 14 In a study by Chang et al. 86% of 13 analyzed esophageal squamous cell carcinomas (ESCCs) showed mesothelin expression using another antibody that is not commercially available. 15 The very limited expression of mesothelin in normal tissue and the high expression in malignant tumors offers an opportunity for mesothelin-targeted therapy.
One aim of our study was to compare the level of mesothelin expression in a large number of esophageal carcinomas using two different commercially available monoclonal immunohistochemical antibodies: Novocastra (mesothelin mouse monoclonal antibody clone 5B2) and Ventana [MSLN (clone SP74), a ready-to-use monoclonal rabbit antibody currently being used in a clinical trial]. 16 Most previous data about mesothelin expression have been generated using antibodies like the Novocastra antibody, and there are no available data on mesothelin expression levels using the Ventana antibody. As patients for clinical trials and potential future treatment are selected by antibody staining of tumor samples, comparison of these two available antibodies is crucial.
Materials and methods
Patients and tumor samples
We analyzed formalin-fixed and paraffin-embedded material from 481 patients with esophageal carcinomas (including 373 adenocarcinomas and 108 squamous cell carcinomas) who underwent primary surgical resection or resection after neoadjuvant therapy between 1999 and 2012 at the Department of General, Visceral and Cancer Surgery, University of Cologne, Germany. The standard surgical procedure was laparotomic or laparoscopic gastrolysis and right transthoracic en-bloc esophagectomy, including two-field lymphadenectomy of mediastinal and abdominal lymph nodes. Reconstruction was performed by intrathoracic esophagogastrostomy, as described previously. 17
Patients with advanced esophageal cancer (cT3, cNx, M0) received preoperative chemoradiation (5-FU, cisplatin, 40 Gy according to the CROSS protocol) or chemotherapy alone (according to the FLOT protocol). Follow-up data were available for all patients. Patient characteristics are shown in Tables 1–4. Depending on the effect of neoadjuvant chemotherapy or chemoradiotherapy, there is a preponderance of minor responders, defined as histopathological residual tumor of ⩾10%. 18
Univariate analysis of clinical parameters – Esophageal adenocarcinoma – Mesothelin Ventana.

Sum of patients does not add to 371 patients due to missing clinical data or missing tumor spots on the TMA.
pN, pathological classification of the degree of spread to regional lymph nodes; pT, pathological classification of the size or direct extent of the primary tumor; TMA, tissue microarray; UICC, Union internationale contre le cancer stage.
Univariate analysis of clinical parameters – Esophageal adenocarcinoma – Mesothelin Novocastra.
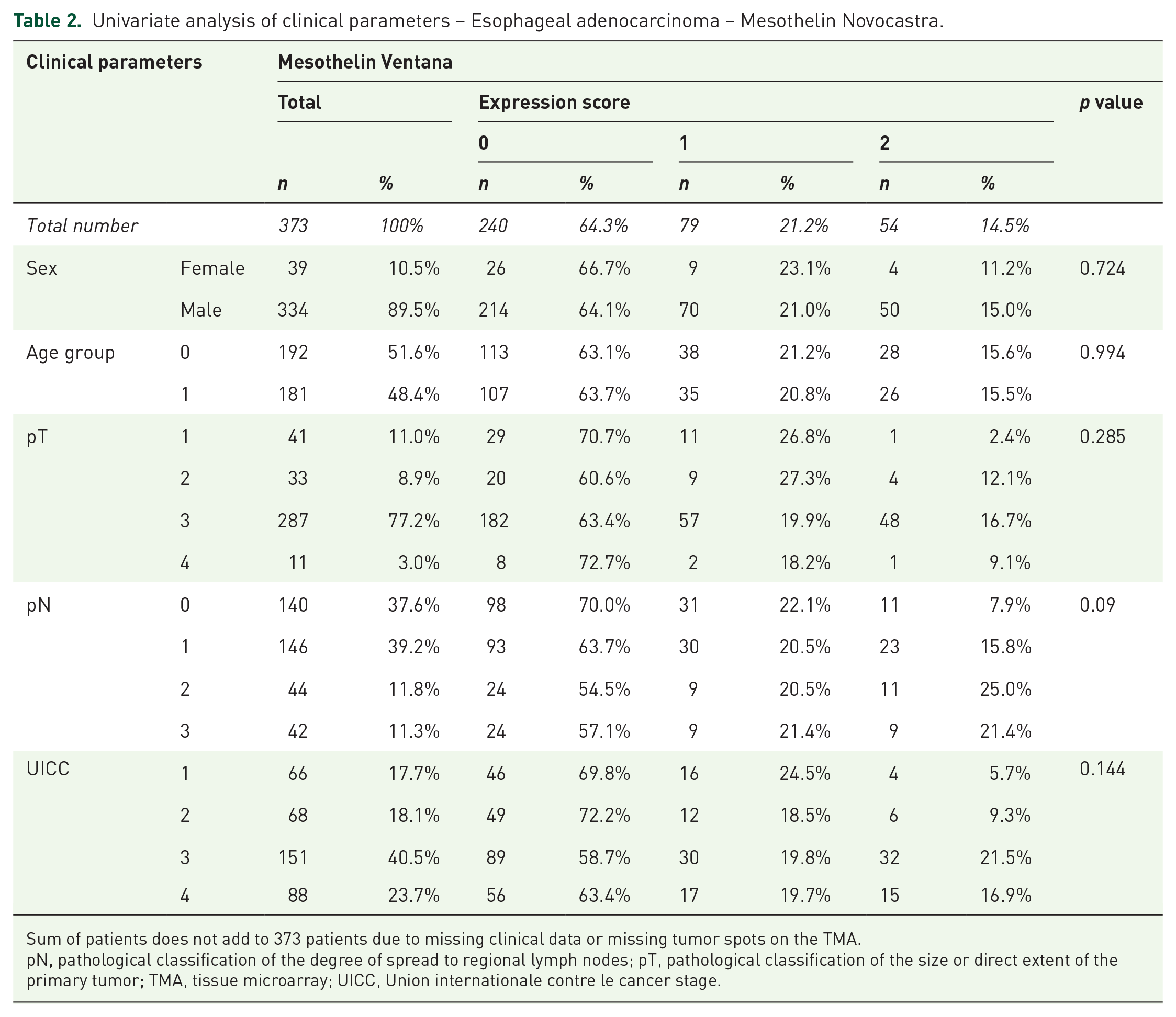
Sum of patients does not add to 373 patients due to missing clinical data or missing tumor spots on the TMA.
pN, pathological classification of the degree of spread to regional lymph nodes; pT, pathological classification of the size or direct extent of the primary tumor; TMA, tissue microarray; UICC, Union internationale contre le cancer stage.
Univariate analysis of clinical parameters – Esophageal squamous cell carcinoma – Mesothelin Ventana.

Sum of patients does not add to 105 patients due to missing clinical data or missing tumor spots on the TMA.
pN, pathological classification of the degree of spread to regional lymph nodes; pT, pathological classification of the size or direct extent of the primary tumor; TMA, tissue microarray; UICC, Union internationale contre le cancer stage.
Univariate analysis of clinical parameters – Esophageal squamous cell carcinoma – Mesothelin Novocastra.

Sum of patients does not add to 108 patients due to missing clinical data or missing tumor spots on the TMA.
pN, pathological classification of the degree of spread to regional lymph nodes; pT, pathological classification of the size or direct extent of the primary tumor; TMA, tissue microarray; UICC, Union internationale contre le cancer stage.
For tissue microarrays (TMAs), one tissue core from each tumor was punched out and transferred into a TMA recipient block. TMA construction was performed as previously described.19,20 In brief, tissue cylinders with a diameter of 1.2 mm each were punched from selected tumor tissue blocks using a self-constructed semi-automated precision instrument and embedded in empty recipient paraffin blocks. Four-micrometer sections of the resulting TMA blocks were transferred to an adhesive-coated slide system (Instrumedics Inc., Hackensack, NJ, USA) for immunohistochemistry.
Immunohistochemistry
Immunohistochemistry (IHC) was performed on single-spot TMAs. In order to answer the question of the heterogeneous distribution of mesothelin expression within the tumor, we additionally examined 38 tumors using a multi-spot TMA considering 12 tumor spots from different tumor areas (for details, refer to a previous study) 21 as well as ten large-scale whole tumor slides using two antibodies. These ten cases are considered in the multi-spot TMA and the 38 tumors of the multi-spot TMA are considered in the single spot TMA. The structure of our multi-Spot TMA is able to reflect the expression situation of mesothelin on the large tumor surface.
Ventana antibody: MSLN, clone SP74, rabbit monoclonal antibody, ready to use (Ethylenediamine tetraacetic acid (EDTA) buffer) on Ventana Benchmark stainer.
Novocastra antibody: mesothelin, clone 5B2, mouse monoclonal using a dilution of 1:50 with EDTA buffer on BOND stainer.
The mesothelin staining intensity was scored manually by two pathologists (AQ and HL) according to a two-tier scoring system (low–mid level and high level) used in a phase Ib study by Bayer [A phase Ib multi-indication study of anetumab ravtansine (BAY 94-9343) in patients with mesothelin-expressing advanced or recurrent malignancies]. In this study protocol, Score 2 (high expression) means ⩾30% positive tumor cells with 2+ or 3+ membrane staining intensity and Score 1 (low–mid expression) means ⩾5% all intensities and <30% positive tumor cells with 2+ or 3+ membrane staining intensity. 16
In addition, we used a well-known analysis algorithm of IHC (H-Score) and applied two established interpretation pathways [two-tier expression behavior in low and high (H-Score 2) and three-tier in low, intermediate, and high (H-Score 1)]. The H-Score is obtained using the following formula: 3 × percentage of strongly stained cells + 2 × percentage of moderately stained cells and percentage of weakly stained tumor cells. The H-Score ranges from 0 to 300. We analyzed both scoring systems (study-related scoring protocol versus H-Scores) in a blinded manner and from clinical and molecular data. Discrepant results were resolved by a consensus review.
Procedures were followed as outlined in accordance with ethical standards formulated in the Helsinki Declaration 1995 (and revised in 2000). Patients provided their written consent with respect to the use of their tumor specimens; an approval was obtained from the University of Cologne Ethics Committee (reference number: 13-091).
Statistical analyses
Clinical data were collected prospectively according to a standardized protocol. For statistical analysis, SPSS Statistics for Mac (IBM Corp. Released 2012. IBM SPSS Statistics for Macintosh, Version 21.0. Armonk, NY: IBM Corp.) was used. Interdependence between staining and clinical data was calculated using the chi-squared and Fisher’s exact tests and displayed by cross-tables. The interdependence of mesothelin expression by Ventana and Novocastra antibodies was additionally tested by kappa and Goodman–Kruskal tau test. Survival curves were plotted using the Kaplan–Meier method and analyzed using the log-rank test.
Results
In cross-table analysis (chi-square test), a strong correlation was observed between Ventana and Novocastra (p < 0.001). The kappa value for the correlation was 0.447 (p < 0.001), and the Goodman–Kruskal tau correlation was 0.372 (p < 0.001).
Esophageal adenocarcinoma
Ventana antibody
A total of 371 esophageal adenocarcinomas were analyzable; 53.6% showed a mesothelin expression. Of these, 25.3% showed a low mesothelin expression (Score 1) and 28.3% a high expression (Score 2; Table 1 and Figures 1, 3, and 5). Only tumor cells showed mesothelin expression (Figures 7 and 8).

The same esophageal adenocarcinoma completely negative for mesothelin using both antibodies.

The same esophageal adenocarcinoma with low staining intensity (Score 1). Ventana antibody detects few more tumor cells. Both antibodies show a more pronounced cytoplasmatic staining pattern.

The same esophageal adenocarcinoma with high staining intensity (Score 2). Ventana antibody detects few more tumor cells and shows a combined drop-like and cytoplasmatic staining pattern. Novocastra antibody shows a drop-like pattern.

Different positive staining pattern for mesothelin in esophageal adenocarcinoma.
Novocastra antibody
A total of 373 esophageal adenocarcinomas were analyzable. The detection rate of mesothelin-positive tumors was lower with the Novocastra antibody; 35.7% demonstrated mesothelin expression. Of these, 21.2% showed a low mesothelin expression (Score 1) and 14.5% a high expression (Score 2; Table 2 and Figures 2, 4, and 6). Only tumor cells showed mesothelin expression.
Esophageal squamous cell carcinoma
Mesothelin expression in ESCC is lower compared with that in adenocarcinoma.
Ventana antibody
A total of 105 ESCCs were analyzable; 13.3% of these in our cohort were mesothelin positive. Of these, 9.5% showed a low expression (Score 1) and 3.8% a high mesothelin expression (Score 2; Table 3 and Figures 9 and 10). Only tumor cells showed mesothelin expression.

Esophageal squamous cell carcinoma using the Novocastra antibody (identical staining pattern using the Ventana antibody).
Novocastra antibody
A total of 108 ESCCs were analyzable; 13% of these in our cohort were mesothelin- positive using the Novocastra antibody. Of these, 11.1% showed a low expression (Score 1) and 1.9% a high mesothelin expression (Score 2; Table 4 and Figures 9 and 10). Only tumor cells showed mesothelin expression.
Mesothelin expression and correlation to clinical parameters
Esophageal adenocarcinoma
We could not find any positive correlations between mesothelin expression and tumor stages [Union internationale contre le cancer (UICC) stages (Ventana: p = 0.279; Novocastra: p = 0.144), sex (Ventana: p = 0.333; Novocastra: p = 0.724) or survival data (Tables 1 and 2)].
Esophageal squamous cell carcinoma
In ESCCs, there are contradictory results for the UICC stages when using different antibodies. The Ventana antibody-related staining results revealed statistically significant correlations of mesothelin expression and advanced tumor stages (Ventana: <0.001), whereas the staining results found by Novocastra showed no such correlations: p = 0.815. Furthermore, no correlations were found when considering the sex (Ventana: p = 0.427; Novocastra: p = 0.501; Tables 3 and 4).
Mesothelin expression and correlation to molecular tumor parameters
A correlation between molecular data and mesothelin expression was observed for EAC alone. However, a correlation between mesothelin expression and TP53 mutations (Ventana: p = 0.619, Novocastra: p = 0.592) and Her-2 amplification (Ventana: p = 0.905, Novocastra: p = 0.102) was not found, respectively. Mesothelin expression was correlated with loss of the chromatin remodeling protein ARID1A (Ventana: p < 0.001, Novocastra: p = 0.003).
Mesothelin expression and correlation to overall survival
We could not find any positive correlation between mesothelin expression and overall survival (Ventana: p = 0.327; Novocastra: p = 0.323) (see Supplemental material).
H-Score
The additionally applied H-Score showed a high concordance of the evaluation results with the study protocol used in parallel (Table 5).
The additionally applied H-Score showed a high concordance of the evaluation results with the study protocol used in parallel.
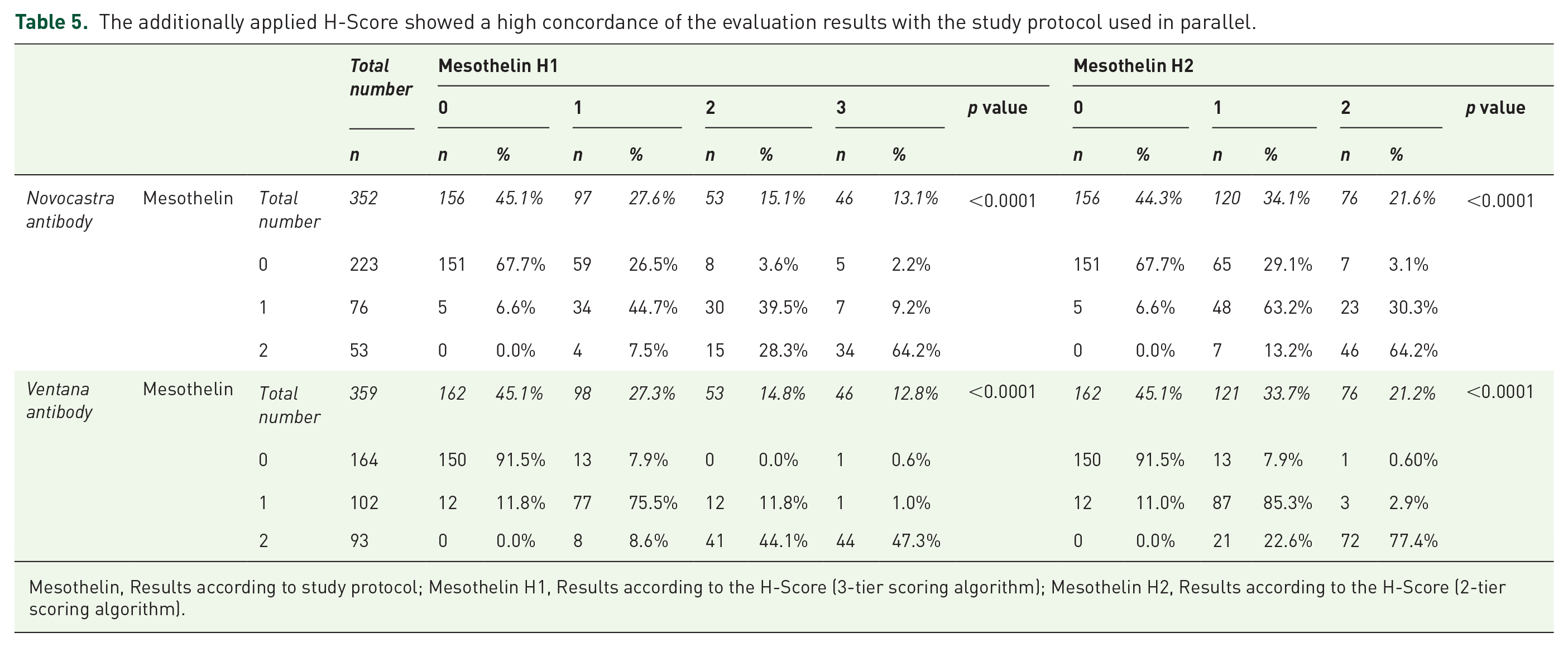
Mesothelin, Results according to study protocol; Mesothelin H1, Results according to the H-Score (3-tier scoring algorithm); Mesothelin H2, Results according to the H-Score (2-tier scoring algorithm).
Heterogeneity of mesothelin expression
In order to answer the question of the heterogeneous distribution of mesothelin expression within the tumor, we additionally examined 38 tumors. We analyzed multi-spot TMAs (12 tumor biopsies) and large tumor areas.
Two cases showed a significant heterogeneity in the expression behavior of mesothelin. One primary tumor was negative for mesothelin but positive in lymph node metastasis, and one additional tumor showed mesothelin expression of its tumor cells only in the invasion zone, while the near-surface tumor portions were negative. The remaining 36 tumors showed a homogeneous expression distribution within the tumor even when using the H-Score with only minor variations.
Discussion
This is the largest and, to the best of our knowledge, the first comparative description of mesothelin protein expression in esophageal carcinomas considering different immunohistochemical antibodies.
Currently, very little data exist about mesothelin expression in esophageal carcinomas. The expression data of mesothelin in gastric cancers cannot be transferred to esophageal carcinomas22,23 since comparative molecular analyses of gastric adenocarcinomas revealed important differences between gastric and esophageal adenocarcinomas (e.g. absence of Epstein–Barr virus and near absence of microsatellite instability subtypes in esophageal adenocarcinoma). 24 This further emphasizes the importance of our study that places large-scale focus on esophageal carcinoma.
Most data about mesothelin expression were generated using monoclonal antibodies like the Novocastra antibody.7,14,25 There are presently no data available on the expression levels of the Ventana antibody. As patients for clinical trials and potential future use are selected by antibody staining of tumor samples, the comparison of these two antibodies is crucial. Our study revealed significant differences in the staining results of the two antibodies used, indicating a more sensitive detection rate of mesothelin expression for the Ventana kit, at least in esophageal adenocarcinomas, but comparable results for ESCC.
The results of our study are consistent with those obtained by Alvarez et al. who showed that approximately one-third of esophageal adenocarcinomas express mesothelin using the Novocastra antibody (in our study the Novocastra antibody showed mesothelin expression in 35.7% of esophageal adenocarcinomas) even though they used a lower number of tumor samples (n = 84). 14
Furthermore, we could demonstrate that mesothelin expression is much lower in ESCCs with 13.3% using the Ventana antibody versus 13% using the Novocastra antibody.
These findings contradict the results of Chang et al., who described expression of mesothelin in 86% of ESCCs, 15 and emphasize the importance of our study further. The significantly higher expression rate might be explained by the very small number of tumor samples they analyzed (n = 13) and the self-constructed, and not commercially available antibody used in the study (MAb K1). 26
However, some limitations of our study should be noted. As previously described, there are no available data describing expression levels of mesothelin using the Ventana antibody. Our results indicate that the Ventana antibody is more sensitive in terms of mesothelin detection in esophageal adenocarcinoma. We do not have an explanation for this fact. Therefore, this should be addressed in future studies on this topic.
The fact that only two previous studies with a small number of cases on mesothelin expression in esophageal carcinoma exist so far and the limited tumor sampling are other limitations that should be mentioned. Both should be addressed in future studies with a higher number of tumor samples to detect the expression of mesothelin in esophageal carcinoma.
Regarding mesothelin as a potential target for immunotherapy, these findings may have an impact on screening procedures and possible future therapeutic strategies. The fact that it is only expressed at very low levels by normal mesothelial cells lining the pleura, peritoneum, and pericardium, 3 and its overexpression in several human cancers, including virtually all mesothelioma and pancreatic adenocarcinomas as well as approximately 70% of ovarian and extrahepatic bile duct carcinomas and 50% of lung and gastric adenocarcinomas,3,11–13 make it such an appealing target. We did not observe any staining in the endothelia or nerves.
Different novel antibody-based therapeutics targeting mesothelin for solid tumors are in various stages of preclinical and clinical development and have shown anti-tumor activity.16,27–31 In a current phase Ib study anetumab ravtansine is being investigated in different mesothelin-expressing advanced or recurrent malignancies [non-small cell lung cancer (NSCLC), TNBC (triple-negative breast cancer), gastric adenocarcinoma including gastro-esophageal-junction (GEJ) cancer, thymic carcinoma, cholangiocarcinoma, pancreatic adenocarcinoma] to evaluate safety and efficacy in the respective indications in patients with either of two mesothelin expression levels (the same expression levels we used in our study). 16 The results are not available yet, but might predict a response rate according to the level of mesothelin expression. 16
How homogeneously a protein relevant for therapy is distributed within the tumor is important from both a therapeutic and a diagnostic point of view. The probability of the efficacy of a therapy increases with the homogeneity of protein distribution. Tumor segments close to the surface, usually achieved with endoscopically obtained tumor biopsies, showing a different expression behavior compared with tumor segments from the invasion zone are also important from a diagnostic point of view, since the entire tumor situation can no longer be deduced from the endoscopically obtained material. We have devoted ourselves to this question and found a relevant homogeneity of mesothelin expression in different tumor areas. It can be assumed that endoscopic biopsy material is likely to provide representative results for the residual tumor.
Due to the extremely aggressive nature and poor survival rates of locally advanced or metastasized esophageal carcinoma, new targets to improve the outcome of patients suffering from these diseases are crucial. The inhibition of mesothelin could be such a novel attractive target. This study revealed a significant number of mesothelin-positive esophageal carcinomas, especially adenocarcinomas.
Supplemental Material
Supplementary_material_2 – Supplemental material for Mesothelin expression in esophageal adenocarcinoma and squamous cell carcinoma and its possible impact on future treatment strategies
Supplemental material, Supplementary_material_2 for Mesothelin expression in esophageal adenocarcinoma and squamous cell carcinoma and its possible impact on future treatment strategies by Valeska Moentenich, Erdem Comut, Florian Gebauer, Armin Tuchscherer, Christiane Bruns, Wolfgang Schroeder, Reinhard Buettner, Hakan Alakus, Heike Loeser, Thomas Zander and Alexander Quaas in Therapeutic Advances in Medical Oncology
Footnotes
Availability of data and materials
The datasets generated and/or analyzed in the current study are available from the corresponding author on reasonable request.
Conflict of interest
The authors declare that there is no conflict of interest.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Research ethics and patient consent
Procedures were followed as outlined in accordance with ethical standards formulated in the Helsinki Declaration 1995 (and revised in 2000). Patients gave their written consent for usage of their tumor specimens, and approval was obtained from the University of Cologne Ethics Committee (reference number: 13-091).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.