
Abstract
Background:
The effectiveness of atezolizumab plus nab-paclitaxel for advanced triple-negative breast cancer (TNBC) has been demonstrated. We aimed to evaluate its cost-effectiveness on advanced TNBC from the US payer perspective.
Methods:
A Markov model was adopted to project the disease course of newly diagnosed advanced TNBC. The clinical data were gathered from the IMpassion130 trial. Cost and health preference data were derived from the literature. The incremental cost-effectiveness ratio (ICER) was measured, and one-way sensitivity analysis and probabilistic sensitivity analysis were performed for exploring the model uncertainties.
Results:
Our results demonstrated that atezolizumab plus nab-paclitaxel augmented versus nab-paclitaxel therapy cost $104,278 and $149,465 and yielded an additional 0.371 and 0.762 of quality-adjusted life year (QALY) in in all patients with unknown PD-L1 status and subpopulation with PD-L1-positive, respectively, which led to an ICER of $281,448 and $196,073 per QALY gained. In all patients with unknown PD-L1 status, atezolizumab plus nab-paclitaxel treatment guiding by PD-L1 expression testing resulted in an ICER of $183,508 per QALY gained. Atezolizumab plus nab-paclitaxel could maintain a trend of positive incremental net health benefits and >50% probabilities of cost-effectiveness at the threshold of $200,000/QALY in more than half of subgroups with PD-L1-positive. One-way and probabilistic sensitivity analyses revealed the results were most sensitive to the hazard ratios (HRs) of overall survival (OS) of atezolizumab plus nab-paclitaxel versus nab-paclitaxel treatment.
Conclusion:
The atezolizumab plus nab-paclitaxel treatment is likely to be a cost-effective option compared with chemotherapy based on nab-paclitaxel for the patients with PD-L1-positive advanced TNBC.
Introduction
Breast cancer is by far the most common malignant tumor in women worldwide, and accounted for 7.56% of the disease burden from all neoplasms as reported by the Global Burden of Disease Study 2017. 1 Triple-negative [hormone-receptor-negative and human epidermal growth factor receptor 2 (HER2)-negative] breast cancer (TNBC) accounts for approximately 10–20% of breast cancer patients. 2 Over the past two decades, cytotoxic chemotherapy based taxanes and anthracyclines have prevailed as the primary established treatment option for patients with early-stage and advanced-stage TNBC. 3 However, fewer than 30% of women with advanced TNBC survive 5 years after diagnosis. 4 The design of the new modalities of novel regimens to breast cancer treatment needs to be undertaken.
In recent years, inhibition of the immune checkpoint regulator programmed cell death ligand-1 (PD-L1), and its receptor PD-1, has emerged as a new anticancer therapy. Due to increased PD-L1 expression in TNBC [odds ratio (OR) = 1.70, 95% confidence interval (CI): 1.24–2.33; p < 0.001], 5 inhibiting the PD-L1 pathway with a PD-L1-inhibitor, such as atezolizumab, provides a strong rationale for testing immunotherapies. The recent IMpassion130 trial reported the efficacy and safety of atezolizumab plus nab-paclitaxel compared with nab-paclitaxel for advanced TNBC. 6 The results revealed that atezolizumab plus nab-paclitaxel notably prolonged median progression-free survival (PFS) in comparison with the placebo group [7.2 months versus 5.5 months; hazard ratio (HR) for progression or death, 0.80; 95% CI, 0.69–0.92; p = 0.002], especially in the PD-L1-positive subgroup (7.5 months versus 5.0 months; HR for progression or death, 0.62; 95% CI, 0.49–0.78; p < 0.001). A notable trend of overall survival (OS) between the atezolizumab plus nab-paclitaxel and nab-paclitaxel arms was observed in the PD-L1-positive subgroup (median OS time: 25.0 months versus 15.5 months; HR for death, 0.62; 95% CI, 0.45–0.86). Treatment-related Grade 3–5 adverse events (AEs) were more frequently reported in the atezolizumab plus nab-paclitaxel group than the nab-paclitaxel group (40.3% versus 30.3%). Thus, the atezolizumab plus nab-paclitaxel regimen seems to be an attractive option for the treatment of advanced TNBC, especially for those with PD-L1-positive disease. However, taking cost-effectiveness into account in healthcare decisions is crucial for clinicians and decision-makers to optimally allocate limited healthcare resources. Herein, we investigated the cost-effectiveness of atezolizumab plus nab-paclitaxel for advanced TNBC from the US payer perspective.
Materials and methods
Analytic overview
A mathematical model combining a decision tree and Markov approach was established to measure the clinical and economic outcomes of adding atezolizumab treatment for treatment-naïve patients with advanced TNBC, and was similar to the IMpassion130 trial. 6 The decision trees included two scenarios: all patients with unknown PD-L1 status TNBC (scenario 1) and patients with known PD-L1-positive TNBC (scenario 2). In scenario 1 (Figure 1A), all patients receive one of three interventions: nab-paclitaxel (chemotherapy strategy), atezolizumab plus nab-paclitaxel (atezolizumab strategy), or the PD-L1-guided strategy (nab-paclitaxel for PD-L1-negative and atezolizumab plus nab-paclitaxel PD-L1-positive after the PD-L1 tissue testing). In scenario 2 (Figure 1B), patients with known PD-L1-positive receive one of two interventions: nab-paclitaxel (chemotherapy strategy) or atezolizumab plus nab-paclitaxel (atezolizumab strategy). A three-health-state Markov model was established to reflect the disease course of advanced TNBC, which included the following health states: progression-free disease (PFD), progressed disease (PD), and death. The Markov cycle length was 28 days in keeping with the treatment schedule reported by the IMpassion130 trial, 6 and the time horizon was 10 years. During each Markov cycle, the model redistributes the hypothetical patients among the three health states according to transition probabilities, which were based on results of the IMpassion130 trial. 6 The initial state was assumed to be PFD, with death as the terminal state.

Model structure for advanced triple-negative breast cancer.
Clinical data inputs
Table 1 summarizes the key clinical inputs. PFS and OS for atezolizumab plus nab-paclitaxel and nab-paclitaxel treatment were informed by the results of the IMpassion130 trial (at least trial follow-up), 6 and extrapolated over the model time horizon using standard statistical analyses described by Guyot et al. 7 The Digitize R package (https://github.com/tpoisot/digitize/) was used to gather the data points from the PFS and OS curves, and these data points were then used to fit the following parametric survival functions: Weibull, log-normal, log-logistic, exponential, generalized gamma, Gompertz, and Royston/Parmar spline model. The goodness of fit was based on a visual inspection and Akaike information criterion. In all patients with unknown PD-L1 status TNBC, we determined that log-logistic and Weibull distributions were the most rational function to extrapolate PFS and OS of nab-paclitaxel treatment, and log-normal and Weibull distributions were used for atezolizumab plus nab-paclitaxel treatment, respectively. In the patients with known PD-L1-positive TNBC, log-logistic and generalized gamma distributions were used to extrapolate PFS and OS of nab-paclitaxel arms, and log-normal and log-logistic distributions were adopted for atezolizumab plus nab-paclitaxel treatment, respectively. Virtual patient-level data comprised event and censor times and were equal in number to the initial number at risk, which was closely reproduced by the digitized Kaplan–Meier (KM) curves of the IMpassion130 trial. 6 The PFS and OS plots created by using the virtual patient-level data and the predicted curves by using parametric survival models are shown in Appendix Figures 1.
Model parameters: baseline values, ranges, and distributions for sensitivity analysis.
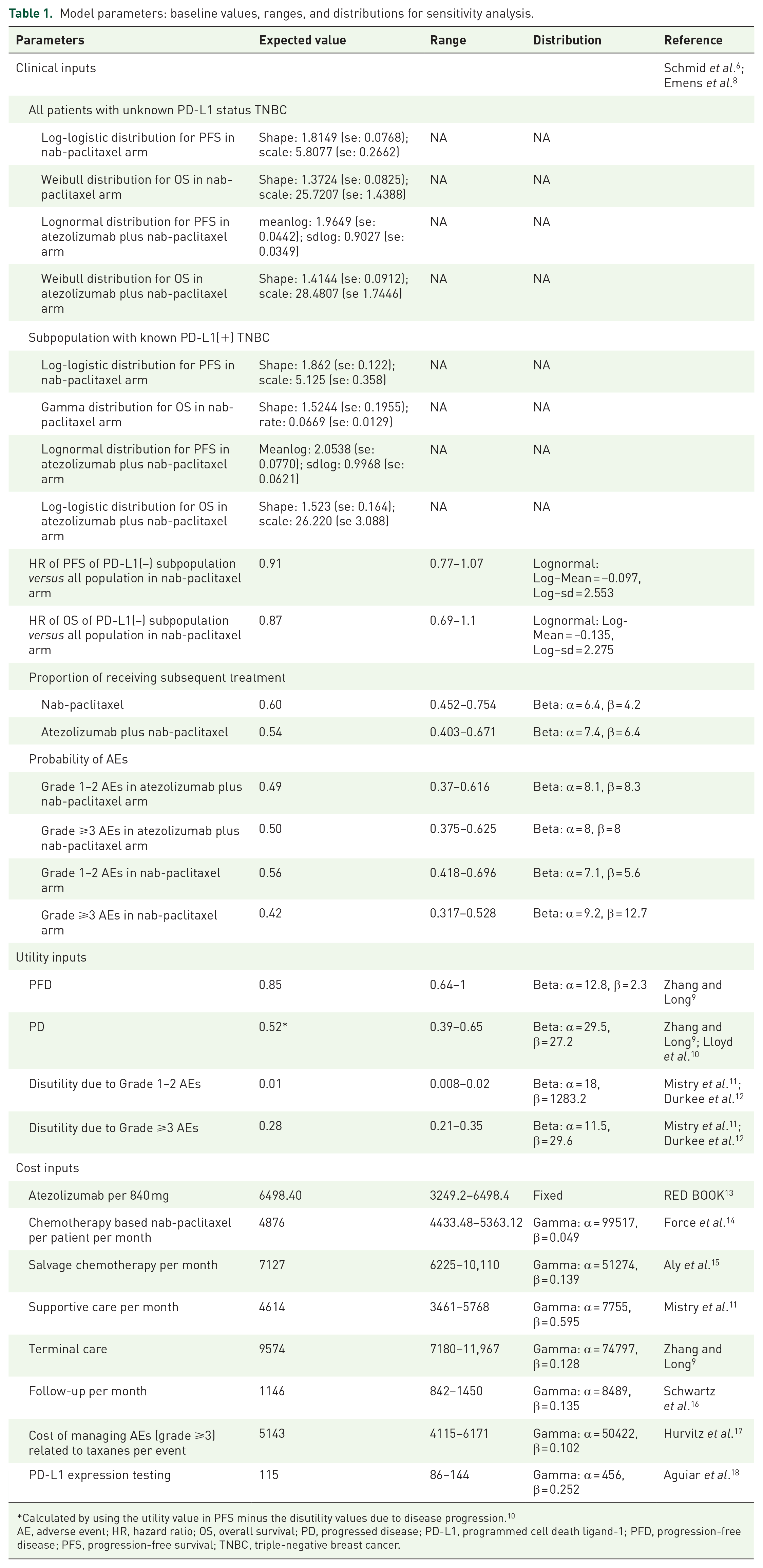
Calculated by using the utility value in PFS minus the disutility values due to disease progression. 10
AE, adverse event; HR, hazard ratio; OS, overall survival; PD, progressed disease; PD-L1, programmed cell death ligand-1; PFD, progression-free disease; PFS, progression-free survival; TNBC, triple-negative breast cancer.
To utilize the HR information of PFS and OS between atezolizumab plus nab-paclitaxel and nab-paclitaxel treatment, the model used the estimated PFS and OS data in atezolizumab plus nab-paclitaxel strategy by multiplying the HRs of atezolizumab plus nab-paclitaxel versus nab-paclitaxel and the PFS and OS data in the nab-paclitaxel treatment. The HRs of PFS and OS between atezolizumab plus nab-paclitaxel and nab-paclitaxel treatment in all patients with unknown PD-L1 status TNBC and the subpopulation with known PD-L1-positive TNBC were collected from the IMpassion130 trial. 6 In patients with known PD-L1-negative TNBC receiving nab-paclitaxel treatment, the PFS and OS data were estimated by multiplying the PFS and OS data in the entire population receiving nab-paclitaxel treatment and the HRs between the PD-L1-negative subpopulation and entire population, which were estimated according to the reported survival data of nab-paclitaxel treatment in PD-L1-negative subpopulation and entire population (Appendix Figure 2).6,8 The influence of HR was checked in sensitivity and subgroup analyses. On the basis of the fitted PFS and OS model, denoted as P(t) and S(t), we computed the disease progression probability Prob (PFS→PD) and cause-specific mortality Prob (PD→Death) at cycle t as follows: Prob (PFS→PD) = (P[t]−P[t + 1])/P(t) and Prob (PD→Death) = (S[t]−S[t + 1])/(S[t]–P[t]), respectively. Due to the poor prognosis of advanced TNBC, we assumed that all deaths were incurred from disease progression. After the disease progressed, the data of patients who received second-line active treatment were collected from the IMpassion130 trial. 6
Cost and utility inputs
Only direct medical costs were considered and reported in 2018 US dollars, including drug acquisition costs, costs attributed to the patient’s health state, costs for the management of AEs, and costs of end-of-life care (Table 1). The costs associated with healthcare services were inflated to 2018 values according to the US consumer price index. 19
Based on the IMpassion130 trial, 6 atezolizumab at a dose of 840 mg was administered on days 1 and 15, while nab-paclitaxel was administered at a dose of 100 mg per square meter of body-surface area on days 1, 8, and 15 of every 28-day cycle until disease progression. The prices of atezolizumab and nab-paclitaxel in the US (average wholesale price) were collected from public databases and the literature. 13 In the US, the price of atezolizumab plus nab-paclitaxel would be discounted at 17% to account for contract pricing. 20 By including 2245 study participants with metastatic breast cancer from paid medical insurance claims, 14 the overall total cost of nab-paclitaxel per patient per month was $4876 (95% CI: 4433–5363), which included other direct medical costs, such as office visits, hospitalizations, and laboratory tests. After the disease progressed, 54% of patients in the atezolizumab plus nab-paclitaxel arm and 60% of patients in the chemotherapy arm received subsequent active therapy, while 15% of patients in the chemotherapy arm received PD-L1 inhibitor treatment in subsequent therapy. 6 Because over 95% patients received chemotherapy as the subsequent treatment in the IMpassion130 trial, we assumed that subsequent active treatment is chemotherapy. The cost of salvage chemotherapy was $7127 per patient per month, 15 which was derived from a retrospective study including 625 US patients with TNBC from the SEER-Medicare database. The cost of supportive care was $4614 per month. 11 The costs of follow up, PD-L1 expression testing, and terminal care were collected from other economic studies.9,16,18
We included only the cost of managing AEs of at least grade 3; grade 1/2 events were considered manageable within standard patient monitoring. The analysis included the overall costs related to AEs of at least grade 3, which were derived from a real-world study by including 1551 metastatic breast cancer patients who had at least one episode of treatment with single or multiple agents for at least 30 days. 17
Each Markov health state was assigned a health utility preference on a scale of 0 (death) to 1 (perfect health). Owing to the absence of utility values associated with TNBC, we assumed the utility values in non-TNBC and TNBC were comparable because quality of life was mainly affected by cancer stage regardless of HER-2 and hormone status as in one recent study. 21 Therefore, the PFD and PD states related to MBC were 0.85 and 0.578, respectively, which were estimated based on established values in non-TNBC.9,10 Disutility values due to grade 1/2 and 3/4 AEs were included in this analysis. All AEs were assumed to have been incurred in the first cycle.11,12 The duration-adjusted disutility was subtracted from the baseline PFS utility.
Analysis
In the base-case analysis, incremental cost-effectiveness ratio (ICER) was calculated as incremental cost per additional quality-adjusted life-year (QALY) gained between atezolizumab plus nab-paclitaxel and placebo. Cost and QALYs were discounted at an annual rate of 3%. 22 The threshold is in line with findings that, in the oncology setting in the US, a broad range of thresholds between $150,000 and $300,000 per QALY has been applied.23,24 The current analysis adopted $200,000 per QALY as the willingness-to-pay (WTP) threshold. We also estimated the incremental net-health benefit (INHB) based on the following formula: INHB(λ) = (μE1–μE0)–(μC1–μC0)/λ = ΔE–ΔC/λ, where μCi and μEi are cost and effectiveness of atezolizumab plus nab-paclitaxel (i = 1) or placebo (i = 0), respectively, and λ is the WTP threshold ($200,000/QALY).25,26 Subgroup analyses were performed in the prespecified subgroup as reported in the IMpassion130 trial by varying the HRs of PFS. 6 The Markov model and statistical analyses were implemented in R software (http://www.r-project.org). The data used in this analysis is anonymous and therefore no informed consent was needed.
To evaluate the robustness of the base-case result, one-way and probabilistic sensitivity analyses (PSA) were conducted. One-way sensitivity analyses were conducted for all parameters, and the estimated range of each parameter was either based on the reported or estimated 95% confidence intervals in the referenced studies or determined by assuming a 25% change from the base-case value (Table 1). In the PSA, a Monte Carlo simulation of 1000 iterations was generated by simultaneously sampling the key model parameters from the pre-specified distributions. Gamma distribution was selected for the cost parameters, log-normal distribution for hazard ratios, and beta distribution for probability, proportion, and preference value parameters. Based on the data from 1000 iterations, a cost-effectiveness acceptability curve (CEAC) was created to represent the likelihood that atezolizumab plus nab-paclitaxel would be considered cost-effective at various WTP levels for health gains (QALYs).
Results
Base-case analysis and subgroup analyses
When PD-L1 status was unknown (scenario 1), adding atezolizumab to nab-paclitaxel (atezolizumab strategy) for all patients provided an additional 0.371 QALYs and 0.632 overall life years with an incremental cost of $104,278, which resulted in an ICER of $281,448/QALY and a INHB of –0.151 QALY at the threshold of $200,000/QALY comparison with nab-paclitaxel (chemotherapy strategy). When atezolizumab plus nab-paclitaxel was administered for the subpopulation with PD-L1(+) after PD-L1 expression was tested, the ICERs and INHB of the PD-L1-guided strategy were $183,508/QALY and 0.030 QALY respectively, in comparison with nab-paclitaxel. When PD-L1 status was confirmed (scenario 2), the ICERs and INHB of atezolizumab plus nab-paclitaxel over nab-paclitaxel were $196,073/QALY and zero QALY respectively. The results are summarized in Table 2.
Summary of cost ($) and outcome results in the base-case analysis.

Compared with chemotherapy strategy.
INHB, incremental net-health benefit; LY, life years; NA, not applicable; PD-L1, programmed cell death ligand-1; QALY, quality-adjusted life years.
Compared with nab-paclitaxel (chemotherapy strategy), adding atezolizumab to nab-paclitaxel for the PD-L1(+) subpopulation in scenario 2 settings showed the trend of gaining additional health benefits in more than half of the subgroups (Figure 2). The INHBs of PD-L1-guided strategy versus chemotherapy strategy in the subgroups with respect to the health benefit varied from –0.05 (range: –0.13–0.04, probabilities of cost-effectiveness: 8.4%) in patients with brain metastases to 0.06 (range: 0.02–0.06, probabilities of cost-effectiveness: 100%) in patients with no previous anthracycline treatment (Figure 2).

Subgroup analysis of INHB and probabilities of cost-effectiveness by varying the HRs of the PFS of the PD-L1-guided strategy versus the chemotherapy strategy in the scenario 1 setting. The vertical line indicates the point of no effect (INHB = 0), the red circle indicates the median INHB, and the green bar indicates the ranges of INHB adjusted by the HRs.
Sensitivity analyses
The one-way sensitivity analyses revealed that the HR of OS for atezolizumab plus nab-paclitaxel versus nab-paclitaxel in PD-L1(+) subpopulation was the most sensitive model input (Figure 3 and Appendix Figure 4). When its lower and upper boundaries were applied, the ICERs of PD-L1-guided strategy versus chemotherapy strategy in the scenario 1 setting changed from $165,922/QALY to $252,203/QALY, and the atezolizumab strategy versus the chemotherapy strategy in the scenario 2 setting changed from $172,716/QALY to $319,932/QALY. Other parameters to consider included the cost of atezolizumab, HRs of PFS, and utilities of progression-free, and progressed disease, whose variation might drive the ICERs of PD-L1-guided strategy versus chemotherapy strategy in the scenario 1 setting to be over the threshold of $200,000/QALY. Other parameters, such as the cost and disutilities associated with adverse drug reactions (ADRs), had a minimal impact on the outcome.

Tornado diagram of one-way sensitivity analyses of PD-L1-guided strategy versus chemotherapy strategy in the scenario 1 setting.
At the threshold of $200,000/QALY (Figure 4), the CEAC showed a nearly 63% probability of the PD-L1-guided strategy being cost-effective, while the ezolizumab strategy in scenario 1 had a zero probability of cost-effectiveness, and the atezolizumab strategy in scenario 2 had a 46% probability of cost-effectiveness.

Cost-effectiveness acceptability curves of atezolizumab and PD-L1-guided strategy versus chemotherapy strategy in scenario 1 and atezolizumab strategy versus chemotherapy strategy in scenario 2.
Discussion
Reports of a clinical benefit from atezolizumab plus nab-paclitaxel treatment in the IMpassion130 trial caused great interest among both oncologists and patients. 6 However, the price of an anticancer drug should be reasonable and affordable, reflect the clinical value of the drug, ensure patients can access the drug, and be sustainable for national healthcare systems, reimbursement platforms, and pharmaceutical companies. 27 Due to the huge demand for treating TNBC, and the rising interest in the economic evaluation of healthcare interventions, the unmet need for a precise economic assessment of atezolizumab plus nab-paclitaxel use in this clinical context has motivated research. 28 By stratifying patients according to PD-L1 status, our analysis demonstrated that atezolizumab plus nab-paclitaxel treatment for advanced TNBC anchoring PD-L1-positive is likely to be optimal for WTP thresholds greater than $200,000 per QALY. This finding is generally consistent with the results of probabilistic sensitivity analyses. At a threshold of $200,000/QALY, more than half of the subgroups with PD-L1-positive were better suited for atezolizumab plus nab-paclitaxel treatment due to its positive trend of gaining net health benefits compared with nab-paclitaxel treatment.
The nature of atezolizumab plus nab-paclitaxel to prolong survival was a major driver of economic outcomes. The findings of one-way sensitivity analysis demonstrated that the HR of OS was the most influential model input. This result indicates that atezolizumab plus nab-paclitaxel would become more cost-effective in patients with more favorable HR of OS, such as for those patients with only lymph node metastasis. However, in some patients with more unfavorable HR of OS who have a high risk of death, such as those with bone metastases and previous anthracycline treatment, the atezolizumab plus nab-paclitaxel might be less cost-effective. The cost of atezolizumab plus nab-paclitaxel was also found to be a substantially influential factor. When the unit cost of atezolizumab decreased by 50%, the ICER for atezolizumab plus nab-paclitaxel decreased to close to $100,000/QALY in the PD-L1-positive subpopulation. Recently, the US government has proposed indexing the prices that Medicare pays for drugs to those paid by health systems in other developed countries, to help bring down the relatively high prices paid by US patients, 29 which might lead to a reduction in the price of atezolizumab, and achieve more favorable economic outcomes. When the price of atezolizumab per 840 mg is lower than $600, the ICERs of PD-L1-guided atezolizumab versus chemotherapy strategy would be lower than $30,000/QALY, which indicates that a atezolizumab regimen would be cost-effective in many middle-income regions, such as China (appendix Figure 5).
The strengths of this study are worth highlighting. First, to our knowledge, this is the first analysis to simultaneously evaluate the economic outcomes of atezolizumab plus nab-paclitaxel for advanced TNBC by synthesizing the latest evidence through an economic modeling approach. Immunotherapy is a new concept in advanced TNBC and has demonstrated promising results in early studies. 30 However, the economic outcomes of the immunotherapy for advanced TNBC have not been examined. Second, the current analysis checked the economic outcomes of near 30 subgroups prespecified by the IMpassion130 trial, 6 including the subpopulations with PD-L1-positive. The findings of subgroup analyses indicate that there is a need to enrich the targeted population for improving the economic outcomes of atezolizumab plus nab-paclitaxel treatment. The information on subgroup economic analysis would be helpful for physicians and patients.
There are several weaknesses with the analysis that produce uncertainty in the results. Firstly, due to the lack of data, we did not include other immunotherapies, such as pembrolizumab plus chemotherapeutic agents, because trials are still ongoing. 30 The current analysis needs to be updated as evidence becomes available. Secondly, health benefits beyond the observation time of the IMpassion130 trial were assumed through the fitting of parametric distributions to the reported KM PFS and OS data, which might have resulted in uncertainty in the model outputs, although the predicted and observed data were validated. Thirdly, we did not measure the budget impact of atezolizumab plus nab-paclitaxel on society. Wide prescription of atezolizumab plus nab-paclitaxel might raise the financial burden substantially. Finally, the costs of grade 1/2 AEs were excluded from the evaluation, which might have led to an overestimation of the economic results of atezolizumab plus nab-paclitaxel, although only small influence was found in one-way sensitivity analysis. These limitations notwithstanding, because the findings of this evaluation reflected the general clinical conditions of managing advanced TNBC, they might be a valuable reference for physicians and policy-makers.
These estimates demonstrated that atezolizumab plus nab-paclitaxel, at a WTP threshold of US$200,000/QALY, is likely to be a cost-effective option for patients with advanced TNBC testing PD-L1-positive in a US payer setting. These findings might contribute to aiding clinicians in making the optimal decisions in the treatment of metastatic triple-negative breast cancer (TNBC).
Supplemental Material
Appendix_file – Supplemental material for Cost-effectiveness of adding atezolizumab to first-line chemotherapy in patients with advanced triple-negative breast cancer
Supplemental material, Appendix_file for Cost-effectiveness of adding atezolizumab to first-line chemotherapy in patients with advanced triple-negative breast cancer by Bin Wu and Fei Ma in Therapeutic Advances in Medical Oncology
Footnotes
Author contributions
BW and FM were involved in the design of the study, collected the data, performed the economic analysis, and wrote the first draft of the manuscript. Both of them have approved this version for publication. The views expressed are those of the authors. The funding agencies played no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethics approval
This study was based on a literature review and modelling techniques; this study did not require approval by an institutional research ethics board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (No. 81874122).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.