
Abstract
Background:
In the Italian Breast Cancer Intergroup Studies (IBIS) 3 phase III trial, we compared cyclophosphamide, methotrexate, 5-fluorouracil (CMF) alone to sequential epirubicin/CMF regimens in patients with rapidly proliferating early breast cancer (RPEBC). We performed a post hoc analysis in the subgroup of patients with hormone-receptor-positive RPEBC on the prognostic role of progesterone receptor (PgR) status.
Methods:
RPEBC was defined by thymidine labeling index (TLI) >3% or grade 3 or S-phase >10% or Ki67 >20%. We analyzed 466 patients with hormone-receptor-positive RPEBC receiving sequential epirubicin/CMF regimens followed by tamoxifen, and for whom the status of ER and PgR was available.
Results:
Considering both cut-off values of 10% and 20%, PgR expression was significantly associated with age, menopausal status, and ER expression; HER2 status was associated with PgR status only at a cutoff value of 20% PgR. Upon univariate analysis, tumor size, nodal status, and PgR were significantly associated with disease-free survival (DFS) and overall survival (OS), while age class and local treatment type were associated only with DFS. Patients with PgR <20% showed lower 5- and 10-year DFS [hazard ratio (HR) = 1.48; 95%CI: 1.01–2.18; p = 0.044] and OS (HR = 1.85; 95%CI: 1.08–3.19, p = 0.025) rates compared with patients with PgR ⩾20%. Upon multivariate analysis, only tumor size, nodal status, and PgR were independent prognostic factors.
Conclusions:
Our results highlight the independent prognostic relevance of PgR expression in patients with hormone-receptor-positive RPEBC treated with adjuvant chemotherapy and endocrine therapy, where the definition of prognostic subgroups is still a major need.
Keywords
Introduction
An estimate of prognosis in patients operated for early breast cancer (BC) is crucial to any decision about optimal systemic adjuvant treatment. Choice should also be guided by the predicted sensitivity to treatments, including endocrine therapy and chemotherapy.
Lack of progesterone receptor (PgR) expression is significantly associated with poorer prognosis in early BC, independently of other variables,1,2 and predicts involvement of axillary nodes at sentinel node biopsy. 3 The status of estrogen receptor (ER) and PgR are the best-known predictors of benefit from adjuvant endocrine therapy. PgR status determined by means of immunohistochemistry (IHC) seems to be a stronger predictive factor than ER status for the benefit of adjuvant tamoxifen in premenopausal patients. 4 PgR levels also independently predict benefit from adjuvant tamoxifen in postmenopausal patients,5,6 while they do not appear to affect the relative efficacy of aromatase inhibitors over tamoxifen.7,8
To establish the appropriate adjuvant treatment strategy for each patient, a comprehensive assessment should include many factors, such as ER, PgR, HER2, and Ki67. These factors are useful to define the surrogate intrinsic subtype, and may be integrated with some genomic tests if available (i.e. Mammaprint, Oncotype DX, Endopredict, PAM50). 9
Endocrine therapy is prescribed to all early BC patients with luminal phenotype. Luminal A-like tumors (defined as ER/PgR positive, HER2 negative, low Ki67) require no cytotoxic treatment, except those with high primary tumor burden or extensive nodal involvement. In luminal B-like, HER-2 negative tumors (ER positive, HER2 negative, high Ki67 and/or low PgR) adjuvant chemotherapy is often prescribed, although other factors, such as tumor extent, nodal involvement, grade, and lymphovascular invasion, are usually taken into account for treatment decision. Among these factors, the lack of PgR expression seems to be a key marker of reduced endocrine sensitivity. Finally, patients with hormone-receptor-positive, HER2-positive tumors nowadays receive adjuvant chemotherapy in combination with anti-HER2 therapy. 9
In patients with rapidly proliferating BC, adjuvant chemotherapy should always be taken into account also in luminal tumors. In the Italian Breast Cancer Intergroup Studies (IBIS) 3 trial by Amadori and colleagues, 10 two different sequences of epirubicin and CMF (cyclophosphamide, methotrexate and fluorouracil) were compared with CMF alone in patients with rapidly proliferating BC as defined by thymidine labeling index (TLI) >3% or histological grade 3 or S-phase >10% or Ki67 >20%.11,12
In the present study, we aimed to explore the prognostic role of PgR status in the subgroup of patients with rapidly proliferating, hormone-receptor-positive BC receiving adjuvant epirubicin-containing chemotherapy followed by tamoxifen within the IBIS 3 trial.
Materials and Methods
Patients
From 1997 to 2004, 1066 patients radically operated for node-negative or 1–3 node-positive, rapidly proliferating BC, were randomized from several Italian centers to receive either epirubicin (four cycles) followed by CMF (four cycles); CMF (four cycles) followed by epirubicin (four cycles); or CMF (six cycles) alone within the IBIS 3 study. The present analysis includes the subgroup of 466 patients with hormone-receptor-positive tumors treated with sequential epirubicin/CMF regimens (excluding those receiving CMF alone), and for whom immunohistochemical assessments of ER and PgR were available. As there was no difference in outcome between the two different sequences of epirubicin and CMF, this can be considered a homogeneous population with regard to the adjuvant treatment received. All patients had rapidly proliferating tumors as defined by TLI >3% or histological grade 3 or S-phase >10% or Ki67 >20%, and were also treated with adjuvant tamoxifen for 5 years, started at the end of chemotherapy.
This retrospective study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki, and was approved by the Medical Scientific Committee of Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS and the Ethical Committees of Area Vasta Romagna, Italy (Approval no. 1164 of 17.07.2014), and by the institutional review boards of each participating center. It has been registered as a National Cancer Institute trial (ClinicalTrials.gov identifier: NCT01031030). Informed consent was obtained from each patient at the time of enrollment into the study.
Biomarker determination
ER and PgR receptors were assessed at each participating center by IHC with different platforms and antibody clones, as previously reported,10,13 and semiquantitatively quantified as the percentage of immunopositive tumor cells out of the total number of tumor cells. Tumors with ⩾10% immunopositive cells were considered positive, as in most studies published in the period when the present study was carried out. Ki67 was assessed with MIB 1 monoclonal antibody (Dako Corporation) in all tumors, and quantified as the ratio of immunoreactive to total number of tumor cells × 100. HER2 was determined using HercepTest (DAKO Corporation) in 329 cases and CB11 monoclonal antibody (Biogenex, San Ramon, CA) in 96 cases. With the first test, positivity was assessed by considering the percentage of immunoreactive neoplastic cells where we measured the intensity and completeness of membrane staining, using a 0–3+ scale as recommended by the Dako criteria. The cases scored as 3+ were considered HER2-positive. For the cases processed with the CB11 antibody, tumors were classified as positive if any grade of immunostaining was present in more than 10% of tumor cells. To assess consistency of biomarker expression data, the stained slides of about 200 available cases were reread centrally for the four biomarkers at IRST laboratory by two independent readers and any disagreement of >10% positive cells was resolved by consensus after joint review using a multihead microscope.
Statistical analysis
Disease-free survival (DFS) was defined as the time from randomization to local or distant disease recurrence, contralateral BC, or death from any cause, whichever occurred first. Patients without events were censored at the last follow up. Overall survival (OS) was defined as time from randomization to death from any cause or censored at the date of the last follow-up visit. A receiver operating characteristics (ROC) analysis was conducted to identify the best PgR cutoff able to divide patients in two classes according to 5-year and 10-year DFS. Univariate analyses were carried out using Chi-square test for comparison of proportions, and the Kaplan–Meier estimator with the log rank test for the estimation and comparison of survival curves. Estimated hazard ratios (HR) and their 95% confidence interval (95% CI) were calculated from univariate and multivariate Cox regression models. All reported p values were two-sided, and p < 0.05 was considered statistically significant. All statistical analyses were performed using SAS statistical software (release 9.4; SAS Institute, Cary, NC, USA).
Results
Patient and tumor characteristics are reported in Table 1. The median age was 51 years (range 29–70). Almost all patients had T1-2 tumors, and about half were node-positive. All were ER-positive, but one-third had ER expression levels <50% and almost two-thirds had PgR levels ⩾20%. A total of 48 patients showed no PgR expression (0%). Due to the selection of patients with highly proliferating tumors, the rate of HER2-positivity was higher than expected (about 40%), whereas, despite this selection, about one-third had Ki67 <20%. Grade, Ki67, TLI and S-phase were determined on 441, 438, 166, and 35 patients, respectively. Patients for whom both Grade and Ki67 were available were 413, while the concomitant information on TLI, Grade and Ki67 was available on 125 patients. The presence of cases with Ki67 <20% is due to the incomplete overlapping of measures of cell proliferation accepted for enrollment into the IBIS 3 trial: the TLI estimates the fraction of tumor cells that are in the S phase of DNA synthesis, while Ki67 is expressed in all phases of the cell cycle (G1, S, G2, M) apart from G0, and grade is scored based on three contributing parameters, among which only mitotic count is related to proliferation. Thus, enrollment of patients based on high TLI or grade 3 may have resulted, in some cases, in the inclusion of patients with low Ki67.
Patient and tumor characteristics (n = 466).

ROC analyses were conducted to identify the best PgR cutoff, dividing patients in two classes according to DFS status at 5 and 10 years. PgR ⩾20% better classified patient based on DFS status at 10 years, with overall accuracy of 60.6% (95% CI 54.1–67.1), while there were no clear-cut best cutoff values according to DFS status at 5 years, or OS status at 5 and 10 years. PgR ⩾10% appeared the best choice based on sensitivity/specificity balance (71.2% / 43.6%) for DFS status at 5 years, with an overall accuracy of 66.6% (95% CI 60.3–72.9). Based also on literature data, 2 we therefore considered the two PgR cutoffs of 10% and 20%.
The relationships between PgR expression and other patient and tumor characteristics are reported in Table 2.
Patient characteristics on the basis of the different PgR cut off values.

PgR, progesterone receptor; RT, radiation therapy.
PgR expression was significantly associated with patient age and menopausal status (with values ⩾20% more frequent in women <60 years old and in premenopausal women), as well as with ER status, at both PgR cut off values of 10% and 20% (Table 2). HER2 status was significantly associated with PgR expression only when using the 20% cut off value for PgR, and Ki67 was never associated with PgR expression.
Table 3 reports univariate analyses of the impact of clinicopathological features on DFS and OS. Tumor size and nodal status were significantly associated with DFS and OS, while the type of local treatment and age class were associated with DFS (better in patients 40–60 years old than in those very young or over 60) but not with OS. Among biological features, only PgR status was associated with both DFS and OS. Patients with PgR <20% had 5- and 10-years DFS rates of 71% and 65%, respectively, compared with 89% and 74% for patients with PgR ⩾20%, with hazard ratio (HR) 1.51 (95% CI: 1.04–2.19, p = 0.030) (Table 3 and Figure 1). Similarly, patients with PgR <20% had 5- and 10-years OS rates of 92% and 80%, respectively, compared with 95% and 89% for patients with PgR ⩾20%, with HR 1.87 (95% CI: 1.11–3.16, p = 0.018) (Table 3 and Figure 2). Similar results, both for DFS and OS, were obtained with a PgR cutoff of 10% (Table 3, Figures 1 and 2).
Univariate analysis of DFS and OS.
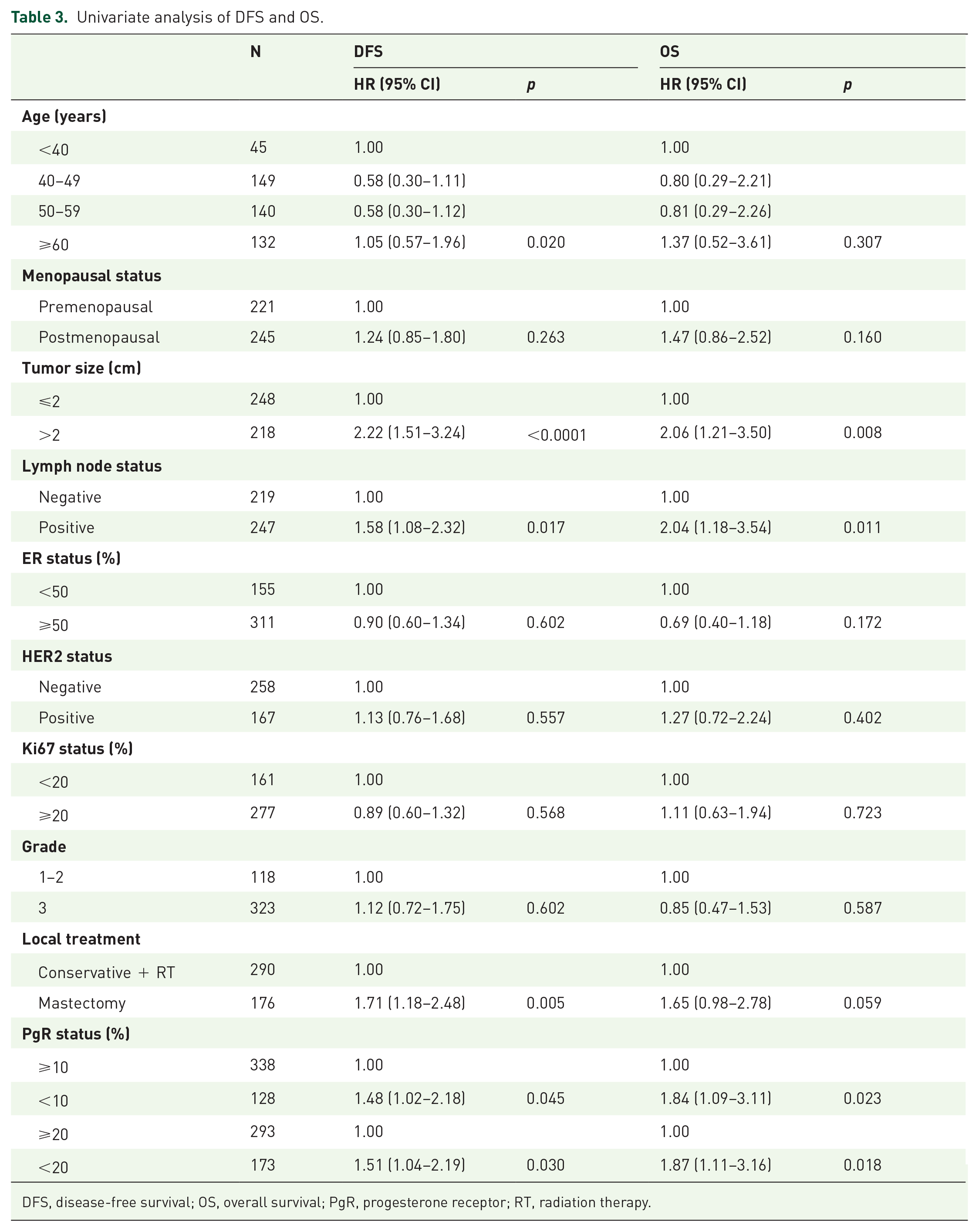
DFS, disease-free survival; OS, overall survival; PgR, progesterone receptor; RT, radiation therapy.
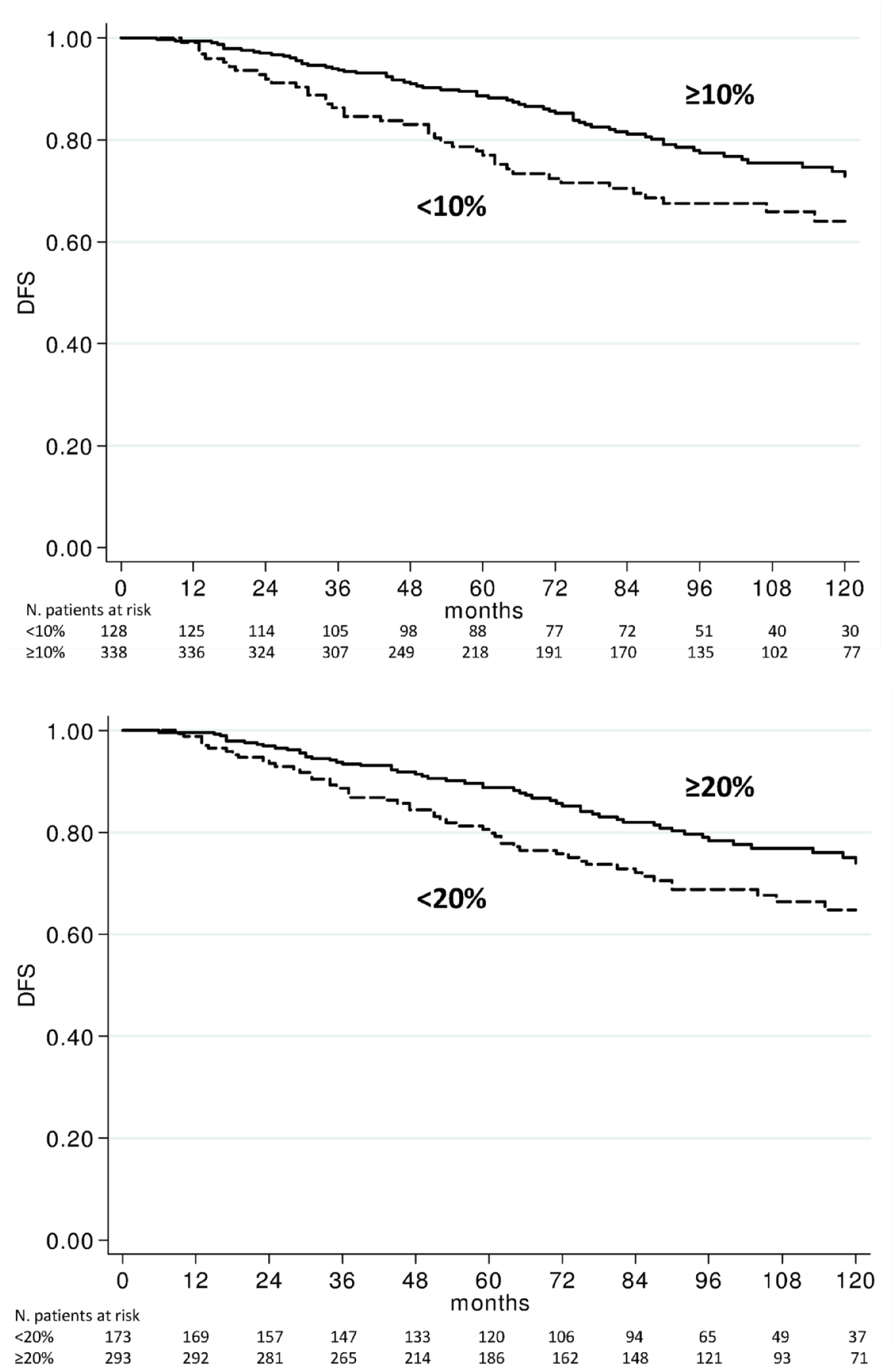
DFS according to 10% and 20% PgR cut off values.

OS according to 10% and 20% PgR cut off values.
Multivariate Cox regression models, including all the variables significantly associated with outcome at univariate analysis, indicated that tumor size nodal involvement and PgR were independent predictors of both DFS and OS (Table 4).
Multivariate analyses.

CI, confidence interval; HR, hazard ratio; PgR, progesterone receptor; RT, radiation therapy.
Because PgR expression levels are affected by menopausal status, we analyzed their distribution and prognostic impact separately in subgroups of premenopausal and of postmenopausal women. PgR status was associated with DFS in postmenopausal but not in premenopausal patients, while OS was not significantly affected by PgR in either subgroup (data not shown). When analyzing results separately in subgroups defined by HER2 status, PgR expression levels significantly affected DFS in patients with HER2-positive disease but not in those with HER2-negative tumors. Tumor size was significantly associated with DFS in all subgroups, but was less consistently associated with OS, and nodal status was not consistently associated with outcome in these subgroup analyses.
Discussion
The conventional biomarkers ER, PgR, Ki67, and HER2 are evaluated routinely in early BC to estimate prognosis and to support adjuvant treatment decisions.
Some studies on the prognostic role of PgR expression have been reported in the literature in different subsets of BC,1–6,13–16 but limited data are available on its role in highly proliferating tumors. We previously compared adjuvant epirubicin followed by CMF versus CMF followed by epirubicin (and versus a third arm with CMF alone, closed in advance) in 1066 patients with node-negative or 1–3 node-positive rapidly proliferating BC. 10 To our best knowledge, this is the first trial specifically enrolling patients with highly proliferating tumors. We concluded that no important differences in clinical outcome were observed between the two different sequences, making both a valid option in early BC, although further molecular characterization of the tumors might help identify subgroups achieving higher benefit from either sequence. In a subsequent subgroup analysis, we showed that patients with highly proliferating tumors, such as triple negative BC, benefit from epirubicin-containing regimens, while patients with less aggressive tumors could be spared the toxicity of anthracyclines. 13 In that study, lack of PgR expression was the single strongest poor prognostic biomarker, associated with both DFS and OS in the whole patient population, and was significantly associated with benefit from anthracycline-containing regimens versus CMF alone.
We also analyzed the impact of PgR expression on the efficacy of endocrine therapy in advanced BC. 14 We demonstrated that, in an ER-high population, PgR >20% in metastases identified patients with a long time to progression on endocrine treatment, while Ki67 >20% was associated with an increased risk of nonresponse. However, there is still the need to confirm the prognostic and predictive role of PgR in different clinical contexts.
The present subgroup analysis from a randomized trial highlights the prognostic role of PgR in patients with hormone-receptor-positive, rapidly proliferating BC receiving adjuvant chemotherapy and endocrine therapy. In this clinical setting, PgR emerges as an independent predictor of both DFS and OS at multivariate analysis, being the only biological feature complementing tumor size and nodal status in defining prognosis. This finding assumes even more importance considering the need to better classify highly proliferating tumors in subclasses with different prognosis in order to tailor adjuvant treatments.
Our results agree with those from other studies showing a stronger prognostic value of PgR status in luminal B-like compared with luminal A-like tumors, 15 while others found a stronger impact of PgR in low proliferating tumors,16,17 or in those with intermediate Ki67. 18 Differences in the definition of luminal A- and B-like tumors and in the cutoffs of Ki67 and PgR might explain these discrepancies, at least in part.
When PgR is not expressed, this might be a consequence of a lack of ER activity and/or of a hyperactivated cross talk between ER and some growth factor receptors. 19 The subgroup of ER-positive/PgR-negative BC has a prognosis more similar to that of hormone receptor-negative BC than to ER-positive/PgR-positive tumors. 20 This phenomenon of PgR loss among ER+ tumors is explained by the two main ways of ER activity: classical or genomic, and nonclassical or nongenomic activity. The former works when ER acts as a nuclear transcription factor, which recruits coregulators for the transcription of specific genes, such as the PR gene coding for PgR. Tamoxifen exerts its function as agonist or antagonist depending on the impairment of different coregulators. 19 The latter form of ER activity is characterized by the cytoplasmic location or plasma membrane binding. This happens for instance when expression of epidermal growth factor receptor (EGFR) is high, and, consequently, the cross talk between ER and growth factor receptors is favored. The related downstream signaling pathways downregulate PgR expression, leading to tamoxifen resistance.21,22 Other mechanisms of PgR loss in ER+ tumors include low circulating levels of estrogen in postmenopausal patients and the methylation of promoter in PR gene.23,19 These preclinical findings provide an explanation for the worse clinical behavior of ER-positive/PgR-negative BC.
We are aware of some limitations to our study, such as the lack of a centralized analysis of all biomarkers. This was due to the fact that the centers involved in the study found some difficulties in retrieving slides on which biomarkers were analyzed from the archives. However, the main study objective was to explore the prognostic role of PgR status in patients with highly proliferating, hormone-receptor-positive BC homogeneously treated with adjuvant chemotherapy and tamoxifen, a selected cohort of patients prospectively enrolled in the IBIS 3 clinical trial. We have not confirmed our data in other datasets, since our study is a retrospective subgroup analysis of patients enrolled in a clinical trial. The definition of high proliferation was based on different assays, although most patients turned out to have high Ki67 even if enrolled based on other proliferation markers (TLI >3% or histological grade 3 or S-phase >10% or Ki67 >20%). Patients were treated homogeneously and therefore we could not assess the predictive value of PgR for benefit from specific treatments. The pathological and immunohistochemical assessments were done at different hospitals, but a large part of the slides for IHC were reviewed centrally independently and homogeneously.
High PgR expression was seen mainly in patients aged 40–49 years, compared with younger and older age classes, and in premenopausal compared with postmenopausal women, independently of the cut off used. Moreover, PgR was expressed principally in tumors expressing higher levels of ER. No association was seen between PgR and the proliferative index Ki67. This could be explained by the fact that all tumors had high proliferation evaluated as TLI >3% or histological grade 3 or S-phase >10% or Ki67 >20%.10,11 Given that we observed higher DFS and OS in patients with PgR positive tumors, we can speculate that the majority of patients aged 40–49 years that are highly expressing PgR would have better prognosis. The prognostic impact of age at diagnosis is still debated, but recent works show worse prognosis in very young and elderly patients.24,25 The impact observed for the type of local treatment on DFS was likely due to the association of local treatment with tumor stage, and disappears upon multivariate analysis.
Our study shows that, in patients with highly proliferating tumors, PgR may still retain an independent prognostic value. The immunohistochemical procedure for the evaluation of PgR is more standardized than that of Ki67, and is a low cost assay normally done in clinical practice for all BCs and affordable by most countries.
These results on PgR have an impact on prognosis and therapy for patients with rapidly proliferating tumors, although further studies are necessary to confirm our findings.
Conclusion
Our results suggest that the evaluation of PgR by IHC is useful to predict the prognosis of patients with rapidly proliferating BC. PgR expression levels should be carefully taken into account when deciding adjuvant treatments in patients with hormone-receptor-positive early BC.
Footnotes
Acknowledgements
Authors Sara Bravaccini and Giuseppe Bronte contributed equally. The authors thank the following contributors: Riccardo Roagna (Mauriziano Hospital “Umberto I”, Turin, Italy), Giuliana Drudi (Infermi Hospital, Rimini, Italy), Britt Rudnas, Emanuela Montanari, Alessandra Piancastelli, Bernadette Vertogen, Federica Zumaglini, and Monia Dall’Agata (IRST IRCCS, Meldola, Italy).
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.