
Abstract
Langerhans cell histiocytosis (LCH) is a diagnostic and therapeutic challenge. We report on a rare case of its primary oral manifestation that was treated successfully with the BRAF-specific agent, vemurafenib, after insufficient standard LCH treatment. This case underlines the importance of proper diagnosis and the evaluation of targeted therapy as a valuable tool in LCH treatment. Furthermore, the close collaboration of surgeons, oncologists, and dentists is mandatory to ensure adequate treatment, restore the stomatognathic system in debilitating post-treatment situations, improve quality of life, and ensure effective disease control in infants and young patients.
Keywords
Introduction
Langerhans cell histiocytosis (LCH), formerly known as histiocytosis X, can occur at any age but is typically found in children.1,2 Its possible presence in any organ makes it a diagnostic chameleon as it mimics multiple diseases depending on the affected area. 3 According to Haupt and colleagues, the predominantly affected location is the skeleton, followed by the skin and the pituitary gland. 3 Less-frequently impaired sites such as the bone marrow, liver, spleen, and lungs seem to coincide with a higher risk of severe progression of the disease. 4 Typically, the disease causes granulomatous lesions in these organs.2,5 The pathogenesis of LCH is still poorly understood. Overstimulation of monocytes/dendritic cells seems to be the key mechanism involving genetically predisposed cells.2,6–8 Recent findings have led to the assumption that LCH should be considered as an inflammatory neoplastic process comprising qualities of a tumour as well as immunogenic components, as it appears to be caused by somatic mutations in bone marrow progenitor cells.2,5,9 One common characteristic is the proliferation, accumulation, and alteration of dendritic cells resembling Langerhans cells of the epidermis.1–3,10 Clinically, LCH is classified as ‘single-system LCH’ (SS-LCH) or ‘multisystem LCH’ (MS-LCH). SS-LCH includes only one organ or system such as bone, skin, lymph nodes, lungs, the central nervous system, the hypothalamic–pituitary system and other locations not specifically listed. Multifocal lesions in one organ, such as multiple bone sites, are also classified as SS-LCH. MS-LCH is classified as the involvement of two or more organs independent of risk assessment or location.3,11 Although involvement of the head and neck (HN) region is possible and observed in more than half of LCH cases, primary manifestations such as oral lesions seem to be rare.12,13 According to Lewoczko and colleagues, in this area, the skull, lymph nodes, and skin are the most frequently affected areas, followed by the orbit. Lesions in the maxilla (fewer than 6% of HN cases) and especially the mandible (about 3% of HN cases) have been rarely observed and therefore seem to account for only roughly 2–4% of all LCH cases.13,14
Case presentation
A 6-month-old girl presented with gingival swelling and intraoral fibrinous coating along the alveolar crests of the maxilla (Figure 1) and mandible as well as feeding problems (700 ml/day, maximum 140 ml per portion). White layers on the dorsum of the tongue could be observed. Apart from feeding or drinking, her general condition was not impaired. The child also demonstrated scaly light-brown macules on the torso. At 2 months before presentation in our hospital, the patient had been treated unsuccessfully for suspected thrush. Furthermore, osteomyelitis or aseptic necrosis of the jaw had been suspected. In this context, the lower first primary incisors and upper primary molars 55 and 65 as well as 61 had been removed. During hospitalization in our clinic, an HN magnetic resonance imaging (MRI) scan with a contrast agent was performed (Figure 2) under general anaesthesia and showed up to 1-cm-broad T2w hyperintense and inhomogeneously contrast-enhancing lesions in the maxilla on both sides, reaching the scarcely pneumatized sinus. Another lesion was localized in the rostral right mandible. While the patient was under general anaesthesia, biopsies were taken, and the primary prematurely erupted teeth (54, 53, 52, 51, 62, 63, and 64) had to be extracted from the loose tissue mass to prevent aspiration. These samples were sent in for histologic analysis. The immunohistochemical analysis revealed the questionable presence of the histiocytic markers, CD68 and lysozyme. In contrast, the strong presence of S100 and CD1a was found. Proliferation was elevated up to 20% (Ki67). CD1a and Langerin (CD207) confirmed the diagnosis of LCH. Analysis also revealed a BRAF mutation in exon 15 (V600E), leading to activation of the mitogen-activated protein kinase (MAPK) pathway. 5 A whole-body MRI was performed after diagnostic confirmation to complete staging of the disease. Since the facial bones were involved, systemic therapy according to LCH-III references was indicated despite the disease being classified as a single-system/single-bone disease.

Clinical situation at first presentation at the age of 6 months, showing LCH and superinfection-affected upper jaw and prematurely erupted teeth.
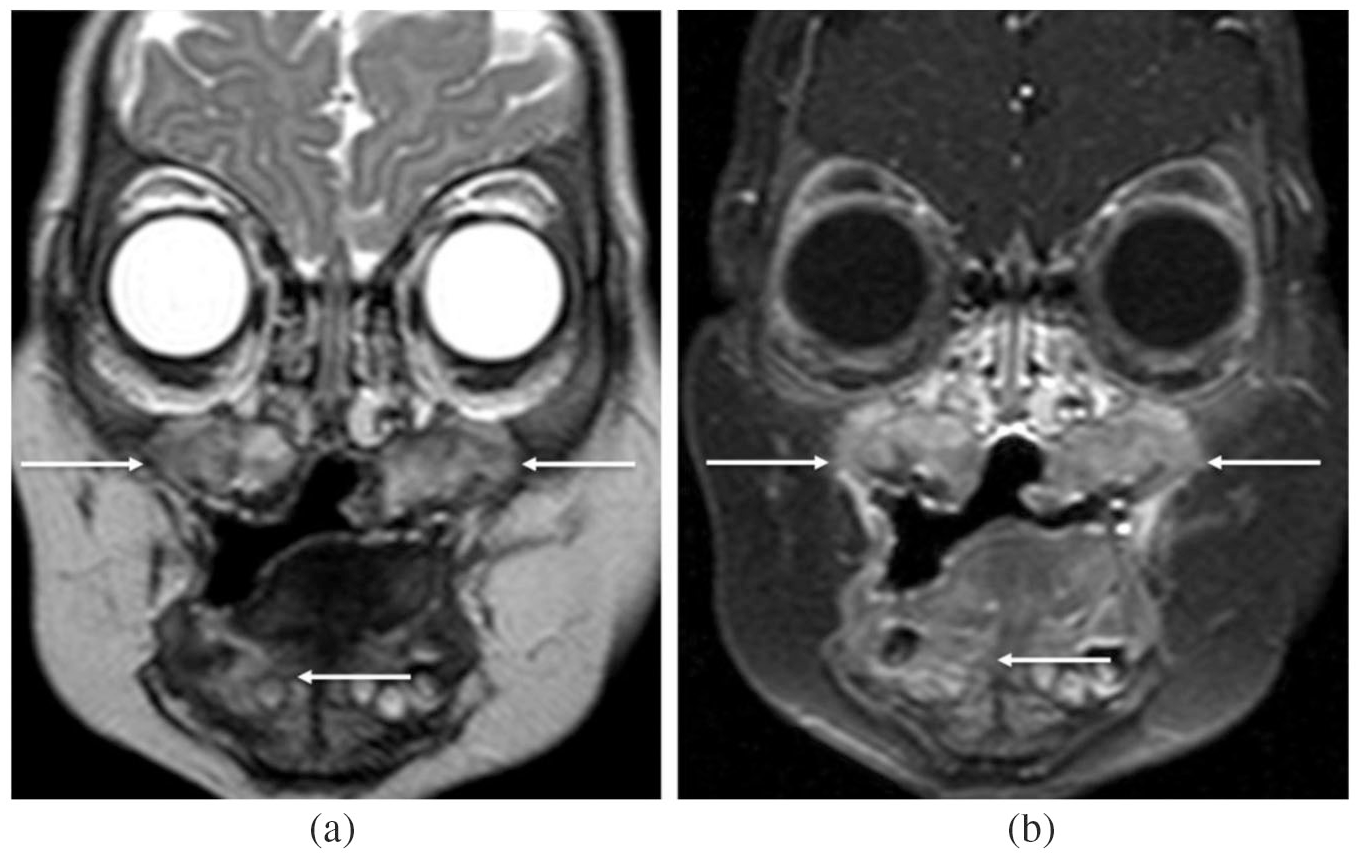
Initial diagnosis of LCH via MRI: T2w TSE (a) and T1w FS after gadolinium administration (b) show manifestations in both sides of the maxilla and in the right mandible.
Systemic treatment was performed by the Department of Paediatrics, Division of Oncology and Haematology. After the implantation of a port-a-cath system for safe drug application, treatment with daily prednisolone (40 mg/m², with dose tapering during weeks 5 and 6) and weekly vinblastine (6 mg/m² for 6 weeks) according to the LCH-III regimen was initiated.
Because of an absent treatment response, a second modified LCH-III cycle with prednisolone pulse therapy (3 days per week) was administered for another 6 weeks.
As a result of persisting active LCH in the affected gingiva, further prematurely erupted teeth had to be removed, leaving only a few remaining germs of permanent teeth (Figure 3). Since the histology showed ongoing vital LCH, treatment was intensified to the second-line regimen for nonrisk patients according to the Histiocyte Society guidelines with a combination of vincristine, prednisone, and cytarabine. 11 This method was poorly tolerated and had to be stopped because of a recurring fever. The treatment was changed to intensified LCH-III maintenance therapy with 3-weekly pulses of vinblastine and prednisolone supplemented by daily 6-mercaptopurine and weekly methotrexate. In the course of treatment, pulse intervals were extended to 6 weeks. In contrast with the last drug combination, this treatment was well tolerated; however, a relevant response of the tumour was not observed. C-reactive protein levels remained between 40 and 100 mg/dl as a sign of persisting LCH activity.

Dental status after successful treatment with vemurafenib at the age of 3 years, showing only a few remaining germs in the upper and lower jaw.
Owing to relevant disease progression after almost 2 years of conventional LCH-III therapy with the newly diagnosed involvement of the skull, skull base, periorbital tissue [Figures 4 and 5(a)], temporal muscles on both sides, and pituitary stalk with resulting diabetes insipidus, the treatment regime was altered to a targeted approach, with the BRAF inhibitor vemurafenib as monotherapy owing to the BRAF V600E mutation found in primary tumour samples. After informed consent from the parents was obtained, vemurafenib was given orally twice (240 mg) per day as crushed suspended tablets on off-label use. Skin irritation and itching efflorescence were observed initially as side effects. At 1 week after the initiation of vemurafenib therapy, C-reactive protein levels normalized, and the patient’s general condition was excellent. Ultrasound and MRI scans in routine check-ups showed improvement of the aforementioned lesions [Figure 5(b)].

Extension of the disease in the craniofacial region after 2 years of conventional chemotherapy. Although T2w TSE FS MRI (a, c) and T1w TSE + gadolinium FS MRI (b, d, e) shows regression in the maxillary region (a, b), new manifestations are observed in the skull base, temporal region, and pituitary stalk and are still focused in the right mandible.
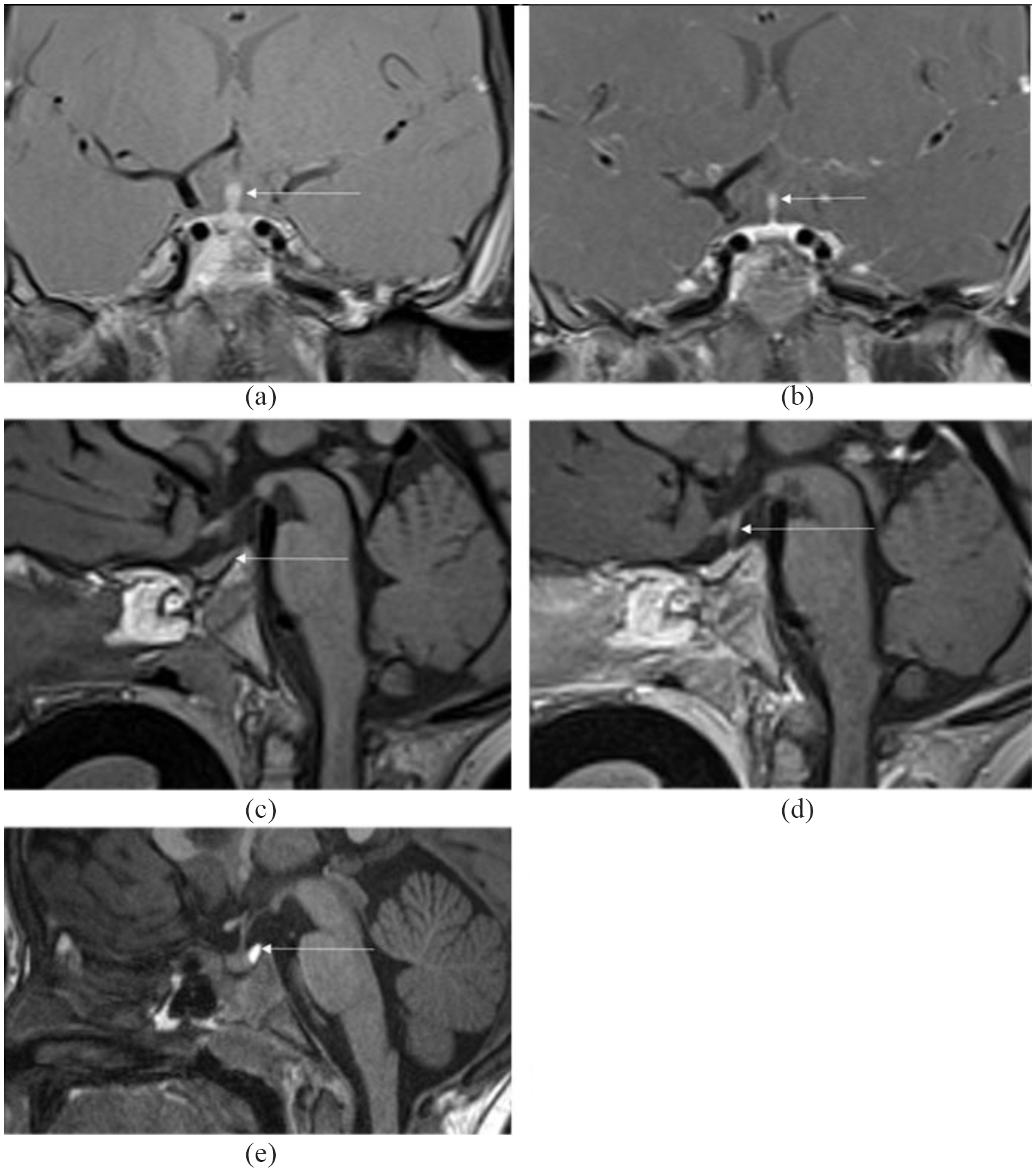
MRI scans showing pituitary involvement: (a) Coronal T1w TSE FS with contrast agent, where the arrow shows a thickened pituitary stalk; (b) Coronal T1w TSE FS with contrast agent showing normal pituitary stalk 3 months after initiation of treatment with vemurafenib; (c) T1w sagittal view after BRAF-specific therapy (without contrast agent): neurohypophysis is not delimitable after therapy (first complete remission); (d) T1w sagittal view after BRAF-specific therapy (with contrast agent): normal shape of pituitary stalk (first complete remission); (e) Normal neurohypophysis in a healthy patient: hyperintense signal in sagittal T1w without contrast agent.
After 1 year of treatment, MRI scans showed complete remission [Figures 5(c,d) and 6], and withdrawal from treatment was attempted. Dental rehabilitation with partial- and full-interim prostheses was necessary, but problems concerning their retention remained and hampered patient compliance. Unfortunately, the control MRI after 6 months showed new lesions in the left zygoma (Figure 7) as well as suspected infiltration of the pituitary gland and stalk. Vemurafenib therapy was reinitiated. After another 3 months, the findings were stable, and contrast enhancement in the pituitary stalk had decreased. At 6 months later, a second complete remission was confirmed by MRI. The diabetes insipidus persisted and did not resolve completely. Other endocrine sequelae were not observed. The entire case is summarized in Table 1.
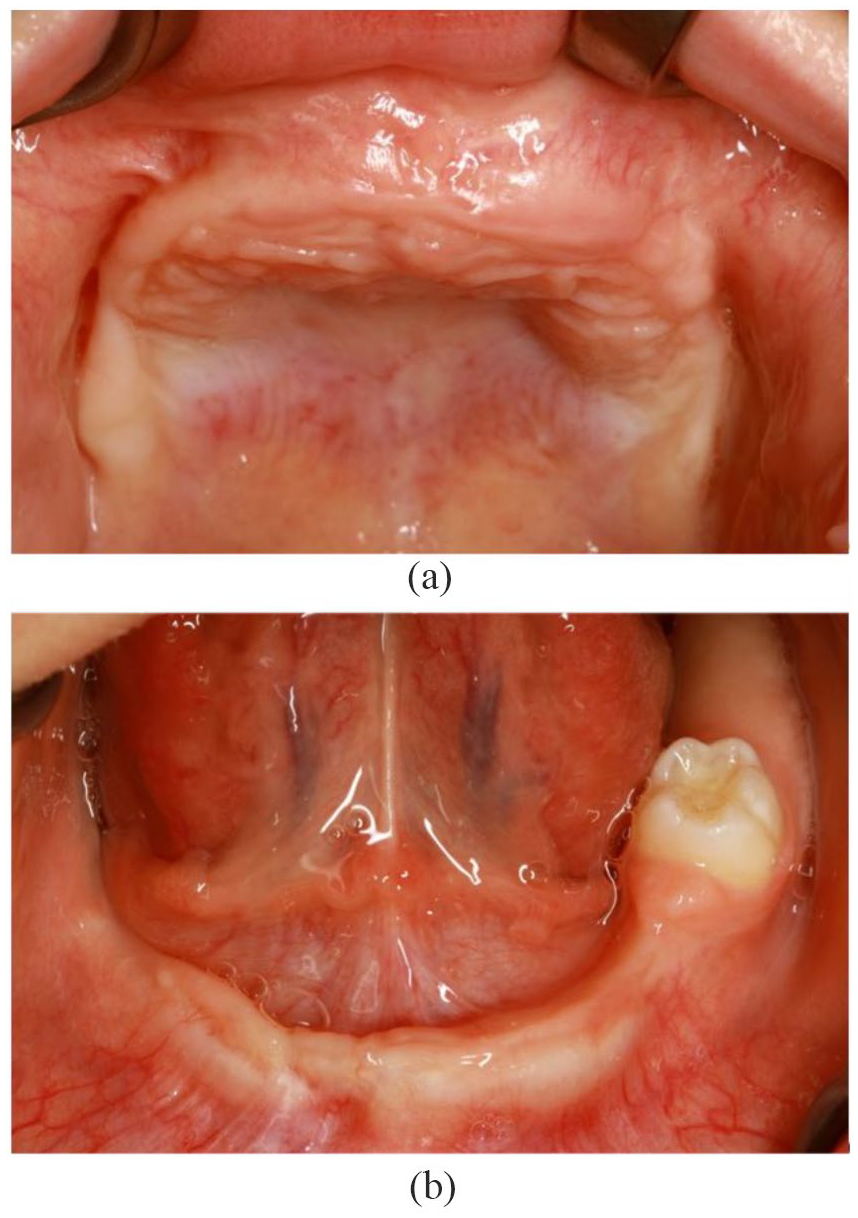
Clinical situation after the first complete remission at the age of 4 years: upper jaw (a) and lower jaw (b).

T2w TSE FS (a) and T1w TSE + gadolinium FS (b) MRIs show a new lesion 6 months after the cessation of treatment in the left zygoma.
Case synopsis and temporal sequence.

LCH, Langerhans cell histiocytosis; MRI, magnetic resonance imaging
Diagnosis
Definitive diagnosis requires the positive CD1a or CD207 (Langerin) staining of affected cells.3,11 Histologically, LCH also shows typical patterns, but electron microscopy to reveal the presence of Birbeck granules is no longer necessary, since Langerin correlates with their existence, although in rare cases, both parameters can be negative.3,15 Since manifestations can occur in every type of tissue, imaging has to be adjusted to the specific situation. 16 In the case of oral or alveolar manifestations, dental radiographs or orthopantomography may be necessary. 17 For three-dimensional evaluations, cone-beam computed tomography (CT) is a potential option, but is inferior in terms of soft-tissue visualization in comparison with multislice CT, and MRI must also be considered.18–21 Multislice CT has the advantage of shorter scan periods and therefore fewer movement artefacts than cone-beam CT, especially in younger or noncompliant patients.22,23 MRI, especially when combined with a gadolinium contrast medium, is highly sensitive and is therefore the method of choice for soft-tissue evaluation, including perifocal oedema and invasion into neighbouring structures, including the central nervous system (CNS).16,24–26 MRI can help detect multiple lesions as a non-invasive whole-body scan as well as for follow up during treatment.27,28 According to Goo and colleagues, whole-body MRI is superior to plain radiography and bone scintigraphy and therefore should be considered as a valid method in evaluating bony and pulmonary lesions, especially considering radiation protection.3,28,29 As alternatives in specific indications, positron emission tomography and scintigraphy can indicate altered tissue metabolism;16,24,30,31 however, the optimal method of bone evaluation is still controversial and should not be changed during follow up.3,24,32,33 When craniofacial bone lesions are suspected, an MRI scan with a gadolinium IV contrast medium should be performed, including all craniofacial bones as well as the brain and the hypothalamus–pituitary axis. 11
The classification of LCH into SS-LCH and MS-LCH helps to facilitate treatment decisions. One important factor is the definition of so-called risk organs and special sites, as proposed by the Histiocyte Society; risk organs include the hematopoietic system, spleen, liver, and lungs. Craniofacial bones, eyes, ears, oral involvement, and CNS lesions are seen as special sites. 11 Referring to the dento-alveolar region, differential diagnoses comprise oral infections or inflammation, such as periodontitis and periapical pathologies, and can mislead dentists and physicians towards incorrect assumptions.34–36 Clinical symptoms include bleeding, bone loss with pathologic probing depths, tooth mobility, ulcers, red and white lesions, osteolytic lesions, demineralization of tooth substance and structure, and glandular involvement. 17 Apart from the typical dental manifestations, this leaves basically every hard- and soft-tissue pathology of the HN area as potential differential diagnoses. Skin alterations and symptoms include pruritus, vesicles, bullae, nodules dermatitis, and petechiae. 3 In the oral mucosa, lesions can present as ulcers and are possible clinical expressions of underlying bone involvement. 37 Bone lesions can also be confused with bone cysts, sarcoma, myeloma, osteomyelitis, leukaemia, lymphoma, fibrous dysplasia, bone angiomatosis, and infectious alterations.3,38,39 Lymphadenopathy and its various origins must be considered as frequent manifestations in the HN area as well.13,40
Therapy
Therapeutic strategies are based on individual staging and classification of the disease. Treatment guidelines for good practice were released in 2008 by the Histiocyte Society after evaluation in LCH-III multicentre studies.3,11 The recent LCH-IV study is set to run until 2025. 41 Craniofacial lesions, including the eyes, ears, and oral cavity, especially bear an increased risk of diabetes insipidus and therefore justify systemic therapy.11,42 Small and noncraniofacial bone lesions can be treated via local excision and curettage as well as local cortisone application.3,43,44 Surgical excision can also be an option for strictly limited skin lesions and the rare case of SS-LCH of the lymph nodes.3,45 Systemic therapy is indicated for SS-LCH with ‘CNS-risk’ lesions, multifocal bone lesions, or ‘special site’ lesions. 11 MS-LCH must be treated systemically, independent of risk-organ involvement. 11 The Histiocyte Society suggests initial treatment with vinblastine and prednisolone for 6 weeks, as administered in our case. In patients that do not respond to treatment but do not experience risk-organ involvement, a second term of 6 weeks of prednisolone in combination with vinblastine is recommended and has been administered in our patient. 11 Unfortunately, salvage therapy was necessary as treatment failure was observed. At present, no official guidelines for second-line therapy for nonrisk patients exist. Therefore, the scheme of the LCH Register 2013 Stratum II SL-IT with vincristine, cytarabine pulses, and prednisone was chosen. 46 This combination, together with cladribine, is clinically documented and mentioned in the literature as a treatment alternative.3,11,47 This approach had to be dismissed because of poor tolerance to treatment and severe side effects. On the grounds of these effects, treatment was changed to an LCH-III maintenance regime with 6-mercaptopurine and methotrexate as permanent medications and pulse treatment with vinblastine and prednisolone.3,11
With the lack of conventional treatment options as well as severe disease progression in the course of this treatment, alternative options had to be found. Possible targets in tumour therapy are BRAF alterations, such as BRAF V600E.1,48,49 As an essential part of the MAPK pathway of receptor tyrosine kinases, it is responsible for the transmission of extracellular proliferative signals to the nucleus. 50 This mutation can be classified together with BRAF V600D/K/R as a class I BRAF mutation, the most commonly identified in human tumours.50,51 BRAF V600E does not rely on dimerization and therefore shows increased kinase activity, leading to RAS (rat sarcoma)-independent signalling.50,52,53 Reproducible evidence shows that targeted BRAF V600E therapy with vemurafenib is effective on Erdheim–Chester disease (ECD) without the development of relevant resistance for up to 16 months. 54 Based on molecular features, including alterations in BRAF V600E and clinical appearance, ECD was classified by the World Health Organization in 2016, together with LCH, as histiocytic and dendritic cell neoplasms. 55 This justifies the assumption of a close relationship between the two diseases. In our patient, the treatment regime had to be changed because salvage chemotherapy failed, so we decided to administer targeted therapy against the BRAF V600E-mutated protein. Recent data show good and prolonged efficiency of targeted BRAF therapy with vemurafenib in LCH and ECD, which led the authors to conclude that the agent can be used as a standard of care for V600E mutant manifestations of these diseases. 56 Given the absence of data on the treatment of children with vemurafenib, the dosage and form of application was chosen as described by Heretier and colleagues, following recommendations and serum levels for the treatment of malignant melanoma.57,58
Dental rehabilitation
In this case, our patient suffered severe multiple tooth loss of both primary teeth and the germs of permanent teeth. This led to functional and aesthetic insufficiencies that may result in underdevelopment of the jaws, malocclusion, and nutritional and social problems, affecting proper articulation and speaking. Thus, the lack of teeth itself, apart from other LCH-related comorbidities, can negatively impact the patient’s quality of life.59,60 Therapy in those cases generally consists of paedodontic protheses, which can also function as an orthodontic apparatus for the proper development of the jaws.61–63 For adults, dental implants are a valuable alternative. 64 Nevertheless, facial growth and the eruption of secondary teeth have to be taken into account considering the ankylosis of dental implants, which leads to a lack of alveolar growth with consecutive infra-occlusion and interference with the eruption of adjacent teeth.65–68 Therefore, evaluating the best time for implantation, if needed, is crucial. According to the German Association of Oral Implantology, dental implants in patients under 12 years of age should be an exception in special cases and respect typical growth patterns. 69 Definitive restoration is not recommended until growth is completed, which may, given structural changes within the jaw, not be the case until the third decade of life. 69 Growth patterns in the maxilla and mandible also vary depending on the existence of teeth influencing alveolar growth. 70 Reports in the literature suggest the possibility of early implantation in younger children with extreme hypodontia because of syndromes such as ectodermal dysplasia.65,70 Compared with the maxilla, with a high risk of implant failure, the growth pattern in the edentulous mandibula seems to allow for earlier implantation in the anterior region of the mandible.65,70–73 In contrast with this situation, the panoramic radiography of our patient showed four remaining germs in the lower jaw. Because of the high risk of tooth loss or implant failure when placed in the vicinity of premature teeth or germs, a conservative procedure with interim prostheses was chosen. Given insufficient retention in the toothless upper jaw, a temporary palatal implant is planned and would serve as anchor for the currently necessary full denture.
Nevertheless, the risk of LCH recurrence is apparent. In any case, close multidisciplinary treatment by an oncologist, orthodontists, and oral and maxillofacial surgeons is essential for treatment success. If facial asymmetry following growth inhibition occurs, orthodontic surgery might be necessary. 15 In every case of oral LCH, treatment should be based on interdisciplinary collaboration, risk evaluation, and frequent recalls. 74 Given that the assessment of LCH recurrence can be hampered by chronic or acute inflammation of oral tissues, proper hygiene is indispensable.73,74
Conclusion
LCH is a challenge both diagnostically and therapeutically. A histological examination of the involved tissue and genetic testing for BRAF V600E mutations are obligatory for the diagnosis and selection of treatment. Although compared with most differential diagnoses, LCH is a rare disease, physicians, surgeons, and dentists should keep it in mind, particularly when observing symptoms refractory to initial therapy according to the working hypothesis. Therapy should be evaluated in an interdisciplinary approach and, especially in advanced stages, be provided in specialized centres. 3 Targeted therapy with BRAF inhibitors has been shown to be effective in individual patients and is being investigated in prospective clinical trials.75,76 A BRAF-specific approach must be considered when conventional LCH therapy fails. Following successful treatment, dental rehabilitation should be accomplished to improve the quality of life of the patient. This requires a multidisciplinary approach as well as a close follow up and consequent re-biopsy of suspicious lesions.
Footnotes
Acknowledgements
We acknowledge support from the German Research Foundation and the Open Access Publication Funds of Charité, Universitätsmedizin Berlin.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Informed consent
Written parental consent for publication was obtained before submission of this article.