
Abstract
Background:
Systemic therapy is the standard treatment against advanced gastric cancer. Fluoropyrimidine plus platinum doublet has been recommended as the preferred first-line strategy. However, there is still a lack of a comprehensive and hierarchical evidence that compares all eligible literature simultaneously.
Methods:
Record retrieval was conducted in PubMed, Web of Science, Cochrane Central Register of Controlled Trials, Embase, ASCO, and ESMO meeting library from inception to October 2018. Randomized controlled trials featuring comparisons between different first-line systemic treatments against advanced gastric cancer were eligible. Overall survival was utilized as the primary endpoint. Pairwise and network calculations were based on a random-effects model and the hierarchical ranking was numerically indicated by P-score. All procedures were conducted according to Cochrane Handbook 5.1 and PRISMA for Network Meta-analysis (Registration identifier: CRD42018084951).
Results:
A total of 119 studies were eligible for our pooled analysis. Concerning general analysis, ‘fluoropyrimidine plus platinum-based triplet’ topped the overall survival hierarchy (HR 0.91 [0.83–0.99], P-score = 0.903, p = 0.04) while it ranked in second place for progression-free survival and objective response rate. However, it displayed worse tolerability against ‘fluoropyrimidine plus platinum doublet’. More specifically, ‘Capecitabine plus cisplatin-based triplet plus targeted medication’ topped the ranking among all fluoropyrimidine plus platinum-based regimens in additional analysis. Nevertheless, it did not reach statistical advantage against fluoropyrimidine plus oxaliplatin doublet in terms of survival benefits, while still displaying significantly worse safety profile.
Conclusions:
Taken together, fluoropyrimidine plus oxaliplatin doublet (especially capecitabine or S-1) should still be considered as the preferred first-line regimen owing to its comparable survival benefits and lower toxicity.
Keywords
Introduction
Gastric cancer is the third leading cause of cancer-related mortality worldwide, and more than half of the cases occur in East Asia.1,2 It is estimated that over 950,000 cases were newly diagnosed in 2012, while 720,000 fatalities were reported, highlighting its relatively poor prognosis. 1
For early localized gastric cancer cases, surgery has been recognized as the optimal therapeutic option owing to its curability.3,4 Nonetheless, for those bearing incurable factors, such as locally advanced inoperable, recurrent, or metastatic gastric cancer, systemic therapy is often used as the preferred palliative treatment among cancer patients, which offers survival benefits compared with supportive treatments alone. 5
Currently, owing to its survival benefits and satisfactory safety profile, fluoropyrimidine and platinum-based doublet is widely recommended as the preferred first-line systemic regimen against advanced gastric cancer. Specifically, fluorouracil (5-FU) or capecitabine plus cisplatin, capecitabine plus cisplatin or oxaliplatin, S-1 or capecitabine plus cisplatin, and S-1 or capecitabine plus oxaliplatin are the first choices recommended by National Comprehensive Cancer Network (NCCN), 5 European Society for Medical Oncology (ESMO), 6 Japanese, 7 and Chinese 8 guidelines, respectively. In terms of fluoropyrimidine and platinum-based triplet, no consensus has been reached despite several phase III studies reporting positive survival results when comparing fluoropyrimidine and platinum-based triplet with the doublet regimen.9–11 Higher toxicity is the major concern about the clinical application of the three-drug regimen, therefore current guidelines only recommend the three-drug regimen for patients with better performance status (PS).5,6 Furthermore, the addition of targeted medications displayed comparable survival benefits against fluoropyrimidine and platinum-based triplet alone,12–15 adding more options on potential alternatives of fluoropyrimidine and platinum-based doublet in terms of preferred first-line systemic regimens.
However, comprehensive evidence of this topic is still scarce. Although three previously published high-quality systematic reviews had reported relevant results, each of them had specific imperfections. Wagner et al. updated their systematic review based on studies up to June 2016 (n = 64). 16 However, this systematic review was only quantitatively synthesized by pairwise meta-analyses rather than hierarchical network meta-analysis. Meanwhile, it only included first-line chemotherapy while excluding studies with targeted medications. Song et al. published a systematic review and pairwise meta-analysis based on studies up to December 2015 (n = 11), which was also an noncomprehensive review since it only included studies with molecular-targeted first-line therapy. 17 Moreover, Ter Veer et al. conducted a systematic review with network meta-analysis based on studies until June 2015 (n = 65). 18 Nonetheless, this systematic review contained both advanced esophageal and gastric cancer patients, while it discussed first-line chemotherapy only. Therefore, those systematic reviews were lopsided, outdated, or inadequate in their use of hierarchical rankings, which urged us to provide an updated and by far the most comprehensive systematic review and network meta-analysis.
Methods
Registration and guidelines
The protocol of our systematic review and network meta-analysis had been published in PROSPERO (CRD42018084951). The design, conduct, and writing of this systematic review and network meta-analysis was strictly in accordance with the requirements from the PRISMA Checklist for Network Meta-analysis and Cochrane Handbook 5.1. Each step was conducted by two investigators of our research group. Any discrepancy was resolved by a third investigator.
Search strategy
Electronic databases including PubMed, Web of Science, Cochrane Central Register of Controlled Trials, and Embase were examined comprehensively. In addition, we also thoroughly searched major databases for meeting abstracts, including American Society of Clinical Oncology (ASCO) and ESMO Meeting Library. The searching process started on 1 March until 4 October 2018, covering possible indexes published from inception to October 2018. Both the abstract and the main text of the retrieved entries were rigorously assessed in order to guarantee the accuracy of selection. Furthermore, in the case of omission, the reference lists of three previously published high-quality systematic reviews were also reviewed.16–18 The full electronic search strategy is presented in the supplementary material.
Selection criteria
Studies that simultaneously met the following inclusion criteria were eligible (PICOS framework).
Participant: patients with previously untreated advanced gastric cancer, including locally inoperable, recurrent, and metastatic cases. Studies that contained both gastric and esophageal cancer cases were eligible. However, if other types of malignancies existed such as pancreatic cancer, it was not qualified unless subgroup data were offered.
Intervention: different first-line systemic treatments against advanced gastric cancer, including chemotherapy and targeted medications. Regarding chemotherapeutic types, since intraperitoneal chemotherapy was still controversial among different countries, we only included oral and intravenous chemotherapeutic regimens. Moreover, the comparisons between different regimens of chemotherapy were qualified while the comparisons between different dosages or methods of administration by the same chemotherapeutic regimen were not eligible. Comparisons between auxiliary therapeutics (such as anti-inflammatory medications, nutritional supportive methods, unspecified herbal medicine, and immunomodulators) were also not qualified.
Comparator: ‘FP2’ (fluoropyrimidine plus platinum-based doublet), ‘FC2’ (5-FU plus cisplatin doublet), and ‘XC2’ (capecitabine plus cisplatin doublet) were common comparator nodes of network meta-analysis under different scenarios.
Outcome: time-to-event overall or progression-free survival (PFS) data [hazard ratio (HR) or Kaplan–Meier curves] were mandatory, while results of objective response rate (ORR) and adverse events were dispensable.
Study design: phase II and phase III randomized controlled trials reported from inception to October 2018 without language limitations. We only included the one with the longest follow-up period among different reports of the same registered trial.
Studies were excluded from systematic review owing to the following reasons.
Could not incorporate into network calculation among unselected population.
Sequential first-line therapy (Supplementary Table 1).
Risk of bias assessment
The quality of each eligible study was evaluated by The Cochrane Risk of Bias Tool. The entire scale was constituted by seven domains, namely random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. 19 According to the criteria in Cochrane Handbook 5.1, each domain could be judged as any of the three levels, low risk, unclear risk, or high risk of bias. If the majority of items were judged as low risk of bias, then the entire methodological design of network meta-analysis was regarded as low risk of bias, and vice versa. Here, studies were defined to be low quality if four or more items were scored as high risk of bias.
Data extraction
Predesigned forms were utilized to collect and organize the original data. General information, survival, and safety data were extracted from the main text, tables, survival curves, or supplementary materials, which had been cross-checked by two different investigators in our team before quantitative synthesis.
Nodes, baseline parameters, and endpoints
Our major principle for node classifications was to combine similar and less-significant regimens together so that sample size and the advantages of direct randomization could be enhanced, and meanwhile also individualize the clinically significant components based on their known mechanisms to lower the heterogeneity and maintain clinical availability. For general analysis among the unselected population, all nodes were in the form of alphanumeric combination. Each type of alphanumeric combination was selected based on the clinical significance and availability. Since leucovorin was routinely considered as a chemo-modulator, it was not calculated into a separate node. The node abbreviations in the general analysis were as follows: F, fluoropyrimidine; P, platinum; R, targeted medication; T, taxane; I, irinotecan; A, anthracycline; M, methotrexate; E, etoposide; Y, mitomycin-C; S, best supportive care; U, nitrosourea; 1, monotherapy; 2, doublet; 3, triplet. For example, ‘FP3R’ suggested that this regimen was a fluoropyrimidine plus platinum-based triplet plus one targeted medication, while ‘F1’ indicated that it was a fluoropyrimidine monotherapy. Meanwhile, different drugs within each regimen were orderly listed according to their clinical significance for systemic therapy (fluoropyrimidine, platinum, leucovorin, taxane, other drugs), which helped to eliminate the possible false classification of the same regimen into two different nodes. For additional analysis among unselected population, similar rationale had been applied. Moreover, since fluoropyrimidine and platinum were crucial components for gastric cancer systemic treatments with different subtypes inside each category that might function differently, we individualized diverse types of fluoropyrimidine and platinum when combining them into separate nodes. All abbreviations of nodes in additional analysis were as follows: S, S-1; C, cisplatin; X, capecitabine; R, targeted medication; O, oxaliplatin; F, 5-FU; H, heptaplatin; 1, monotherapy; 2, doublet; 3, triplet. For instance, ‘XC3’ was the node for capecitabine plus cisplatin-based triplet.
Unselected patients were those without specific pathological positivity, in contrast to those featuring specific positivity such as HER-2 positive gastric cancer. Since most studies were completed via multinational cooperation, the leading country of each study was defined by the nationality of its first corresponding author, who usually led the project. Age referred to the median age of overall population. Here, region referred to the source region of patients that had been analyzed in the studies. Western regions included Europe, North America, and Australia, while eastern regions usually referred to East Asian countries including Japan, South Korea, and China. If the study contained patients from both western and eastern regions, or patients from other areas of the world (such as South America), it was regarded as a versatile region. Visceral involvement suggested the metastatic involvement of liver and lung. In term of measurability, those nonmeasurable but assessable patients were also included as measurable cases. Owing to the potential disparity of efficacy in terms of different tumor locations and histological types, ratios between gastric cancer and gastroesophageal junction cancer, as well as intestinal type and diffused type were collected, respectively. Usually, patients with gastric cancer should significantly outnumber those with gastroesophageal junction cancer.
The primary endpoint was overall survival (OS), while secondary endpoints included PFS, ORR, hematological adverse events, and nonhematological adverse events. OS and PFS were defined as the time from randomization to death from any cause and the time from randomization to disease progression or death from any cause, respectively. ORR was the percentage of patients with complete and partial response. The hematological adverse events included leukopenia, neutropenia, anemia, thrombocytopenia, and other relevant events such as febrile neutropenia and infection with neutropenia. The remaining adverse events were categorized as nonhematological adverse events. We only counted grade 3 or higher (National Cancer Institute Common Terminology Criteria for Adverse Events) adverse events owing to their clinical significances. For early studies that failed to use this numerical grading system, we collected severe-toxicity adverse events in the nonhematological category and leukocyte count <2000/μl, platelets <50,000/μl, or hemoglobin <9.5 g/dl were collected in the hematological category.
Statistical analysis
HRs and 95% confidence intervals (95% CIs) were used as the effect size for OS and PFS. Risk ratios (RR) and 95% CIs were applied as the effect size for ORR, hematological and nonhematological adverse events. If survival data or its CI was not directly provided, we estimated the values from the Kaplan–Meier curves by methods described elsewhere. 20 In terms of adverse events, the total amount of grade 3 or higher adverse events were used for calculation, instead of the number of patients suffering grade 3 or higher adverse events.
As was known to all, the prominent strength of network meta-analysis was to provide a hierarchical ranking for multiple arms even without direct comparisons. 21 This key feature reflected on and highlighted the two fundamental assumptions of network meta-analysis, known as transitivity and consistency. 22
When the head-to-head results of A versus C and B versus C were respectively provided, then the hypothesis of transitivity also validated a statistical comparison between A and B. However, it required comparable general features within each node as the prerequisite condition to eliminate selection bias and justify statistical connections among indirect arms. 23 Since all included studies were randomized controlled trials without significant methodological heterogeneity, the baseline parameters were the crucial factors to determine the clinical heterogeneity and therefore transitivity. We carefully compared the main baseline features of different arms within each node and eliminated those with significant differences by sensitivity analysis. Apart from clinical and methodological heterogeneity, we also evaluated statistical heterogeneity of the network meta-analysis, which was known as the overall degree of disparity within the same pairwise comparison. 24 The I2 statistic was the chief indicator of statistical heterogeneity, with values of <25%, 25–50%, and >50% indicating low, moderate, and high heterogeneity, respectively. In addition, the Q statistic of heterogeneity and its p value also facilitated the assessment of statistical heterogeneity. If the p value of the Q statistic was less than 0.05, it suggested that there was significant heterogeneity.
On the other hand, the consistency, another crucial assumption for network meta-analysis, referred to the statistically consistent results between direct and indirect effect sizes regarding the same comparison. Significant differences between direct and indirect calculations might indicate inconsistency within the network meta-analysis while also suggest the unsuitability for transitivity. 25 Here, we employed several methods to assess the network consistency, including the comparison between direct and indirect results as well as the Q statistic. We performed a pairwise meta-analysis via both fixed-effects and random-effects calculations to generate direct results before network meta-analysis. Concerning the same therapeutic comparison, the results were regarded as consistent if the 95% CI of both pairwise and network meta-analysis significantly overlapped. Meanwhile, the Q statistic of inconsistency was another statistical indicator to numerically estimate the consistency within the comparisons, whose p value (<0.05) could suggest a significant inconsistency between pairwise and network meta-analysis. Both consistency and homogeneity were crucial bases to offer reliable outcomes by network meta-analysis. If inconsistency or significant heterogeneity occurred, we deleted the original data from the most inconsistent or heterogeneous pairwise comparisons to examine whether the results remained unchanged, otherwise it was not appropriate for pooled analysis.24,26
For the network calculation of general analysis, ‘fluoropyrimidine plus platinum’ (FP2) was chosen as the common comparator since it was the regimen preferred by different guidelines. A network plot and comparison-adjusted funnel plot were used to display the network structure and examine the publication bias across the included trials, respectively, where the more symmetrical it was, the lower the probability of publication bias the merged results would have.27,28 We conducted the random-effects network meta-analysis based on a frequentist model, with either HR or RR as the effect size. A network forest plot or league table were used to demonstrate the entire regimens with their relative CIs. In addition, we also utilized P-score to rank all regimens based on their network estimates. The closer the P-score moved to 1, the better the regimen. Sensitivity analysis was performed to detect the stability of pooled outcomes, which included using fixed-effects model and deleting studies with significant clinical heterogeneity. For the network calculation of additional analysis, ‘5-FU plus cisplatin’ (FC2) was chosen as the common comparator since they were recommended by NCCN guidelines, while the remaining statistical methods were similar to those of the general analysis.
Both pairwise and network meta-analysis were conducted in R software 3.4.3, assisted by STATA 14.0 in terms of graphical functions.
Role of the funding source
The sponsors had no role in study design, data collection, data analysis, data interpretation, or writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Results
Literature retrieval
After screening through 15,262 preliminary records, a total of 119 randomized controlled trials were eligible for inclusion in our systematic review (Figure 1). Among 119 eligible trials, 94 studies were included in the general analysis of unselected population, 39 studies were selected into the additional analysis of unselected population (including 22 studies overlapping with general analysis), while 8 trials were systematically reviewed in terms of specific pathological positivity. Both systematic review and network meta-analysis were conducted among unselected population, irrespective of general or additional analysis. However, owing to the limited number of eligible studies, we only performed systematic review for studies concerning specific pathological positivity.

Selection flow chart for network meta-analysis.
General analysis: baseline features and transitivity
Overall, 94 randomized controlled trials were included in the general analysis, containing a total of 17,976 participants. Japan (n = 19), USA (n = 15), and China (n = 12) were the top three leading countries. A total of 52 studies recruited patients from western region, while 37 and 5 studies featured patients from the eastern region and versatile region, respectively, displaying a relatively balanced geographical distribution between eastern and western regions. ‘Fluoropyrimidine plus platinum doublet’ was the most frequent node in the network (n = 45), followed by ‘fluoropyrimidine plus platinum-based triplet’ (n = 31), and ‘fluoropyrimidine monotherapy’ (n = 28). The majority of the studies featured populations with a median-age around 60 and male-dominant sex ratio. Predominantly, patients were metastatic measurable cases and had a PS of either 0 or 1. Meanwhile, the ratio of visceral or peritoneal involvement, primary locations (dominant proportion of gastric cancer cases) and histological types were largely comparable across different studies. Therefore, the demographic characteristics of included trials were generally comparable. Several studies might introduce potential heterogeneity owing to incompatible baseline features with other studies, such as recruiting elderly patients (>70 years old),12,29–32 containing esophageal,13–15,29,31,33–36 fake registration identifier, 37 nonmeasurable cases only, 38 and peritoneal metastasis only 39 (Table 1). The influence on pooled results by these studies was further detected in sensitivity analysis.
Baseline characteristics of eligible studies for general analysis (unselected population).

E/T, events/total patients; G/J, gastric/junction; hAE, hematological adverse events; HR, hazard ratio; I/D, intestinal/diffused; M/F, male/female; NA, not available; non-hAE, nonhematological adverse events; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; P/T, responsive patients/total patients;
First, all included studies were randomized controlled trials that minimized the methodological heterogeneity induced by different study designs. Second, patients in most studies shared similar and comparable baseline characteristics that guaranteed the treatment effects not to be artificially biased owing to unbalanced confounding information. For example, in most studies, patients were PS < 2, metastatic, measurable, and gastric cancer cases, without specific inclination of histological types. Other potential difference in baseline features were either unable to alter the results (such as small amount of esophagogastric junction cases) or addressed by sensitivity analysis (Table 1). All these had justified the transitivity and performance of our network meta-analysis.
General analysis: risk of bias
Overall, the included studies had low risk of bias since nearly half of the assessment parameters were scored as low risk of bias (45%), while unclear risk (39%) or high risk of bias (16%) took up relatively small proportions (Figure 2). None of the eligible studies were at high risk of bias concerning methodological design (Supplementary Table 2).
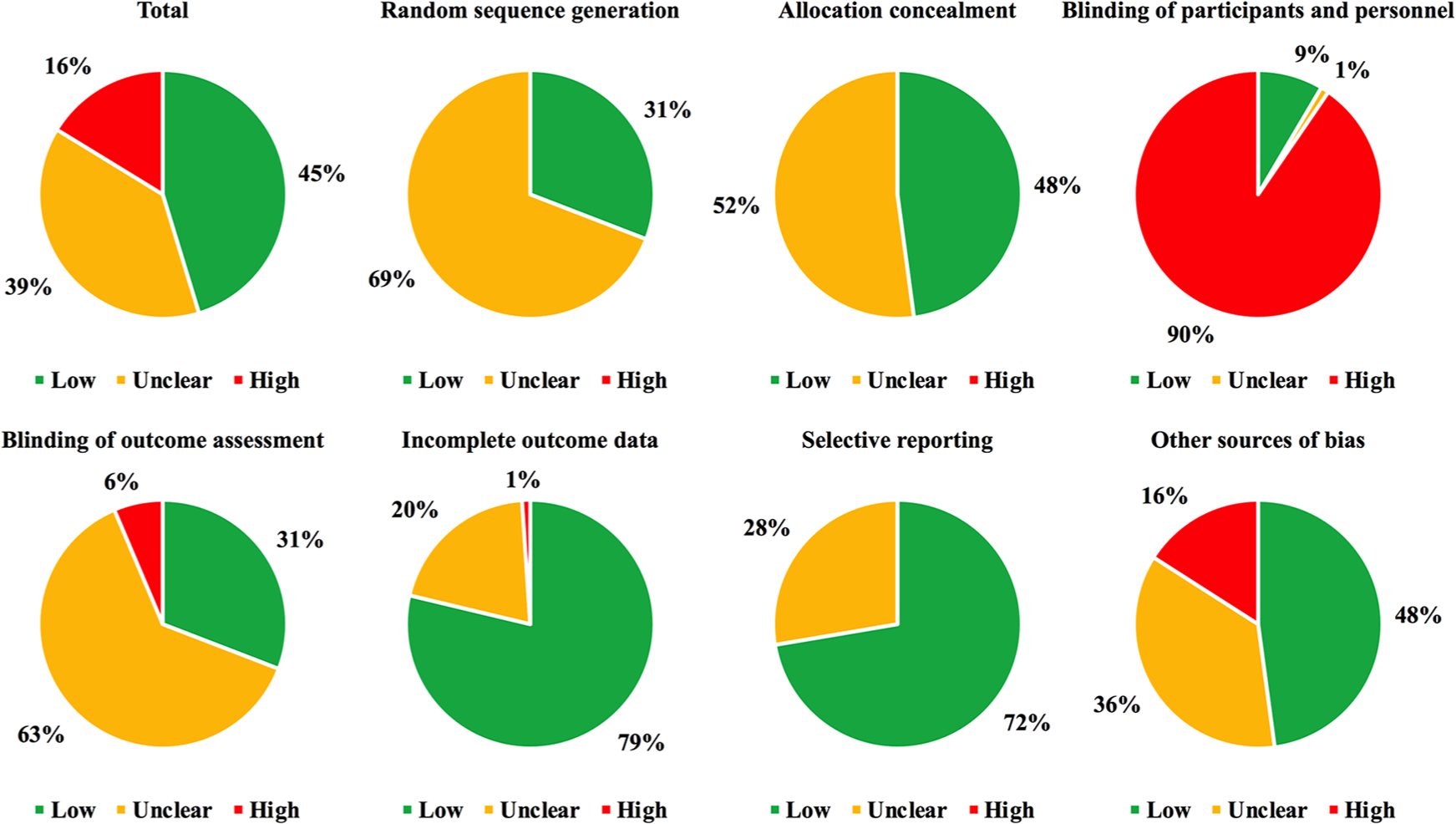
Risk of bias assessment in general analysis.
Specifically, 31% and 48% of the studies were evaluated as low risk of bias concerning random sequence generation and allocation concealment, respectively, while no high risk of bias was reported in these two key domains. Largely due to the open-label design, 90% of the included trials were scored as high risk of bias in terms of blinding or participants and personnel. Meanwhile, since there was a lack of details on whether the response evaluation was independent enough, more than half of the studies (63%) were evaluated as unclear risk of bias regarding blinding of outcome assessment. In addition, because most of the studies were analyzed based on the intent-to-treat population as well as having reported enough endpoints, 79% and 72% of the eligible trials had low risk of bias in terms of incomplete outcome data and selective reporting, respectively. Moreover, since the majority of studies were completely performed without early termination and also described adequate baseline details, nearly half of the studies (48%) were appraised as low risk of bias with respect to other source of bias (Figure 2).
General analysis: primary endpoint (OS)
Network geometry
There were a total of 91 randomized controlled trials merged into the quantitative analysis, with 17,529 participants and 24 nodes of therapeutic regimen (Figure 3 and Table 1).
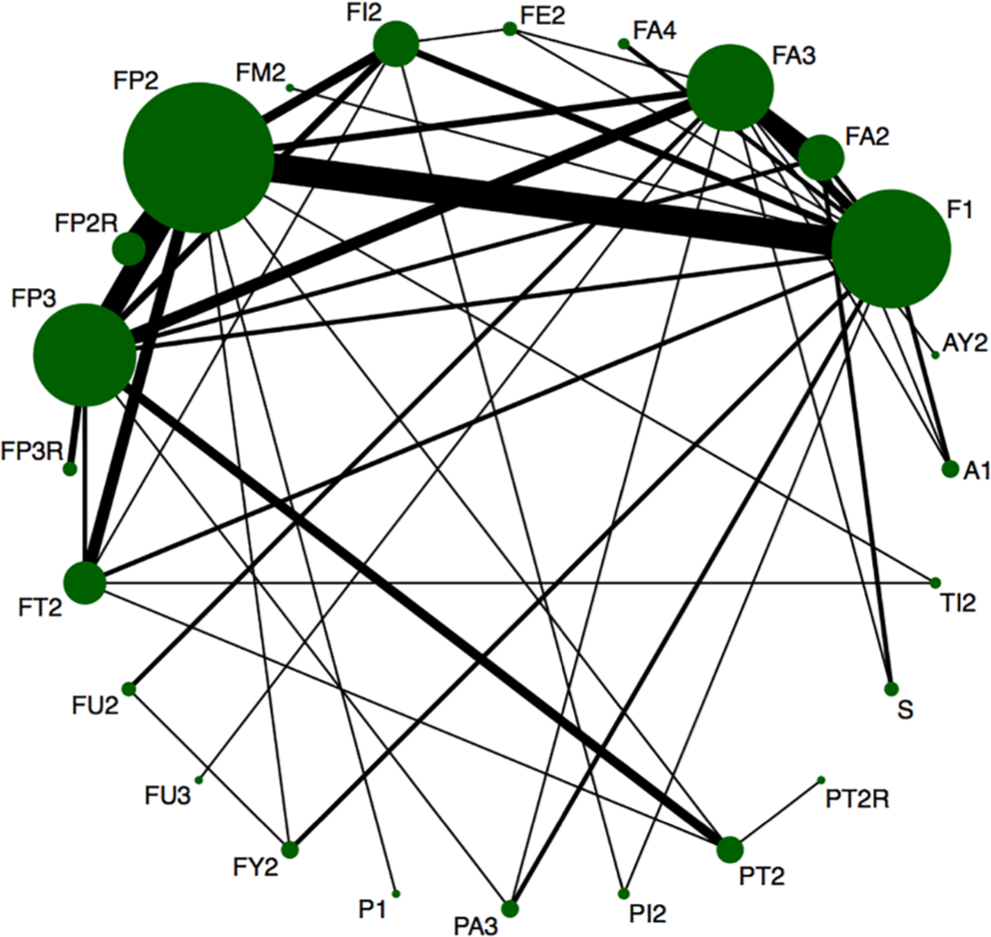
Network structure plot of overall survival in general analysis.
Consistency and statistical heterogeneity
In addition to the value of Q statistic (Q inconsistency: p = 0.08), the effect size and CI between direct and indirect results were highly overlapped (Supplementary Table 3), both of which suggested that results inside the entire network were consistent. In terms of statistical heterogeneity, both I2 statistic (I2 = 15.00%) and Q statistic (Q heterogeneity: p = 0.29) implied that there was no significant heterogeneity across the network.
Publication bias
There was no publication bias among the included studies owing to the symmetrical distribution of effect sizes inside the funnel plot (Supplementary Figure 1).
Network calculation
Based on P-score ranking of the network meta-analysis, ‘fluoropyrimidine plus platinum-based triplet’ (network HR 95% CI: 0.91 (0.83–0.99), P-score = 0.903) was the best ranking regimen, displaying statistical superiority against common comparator ‘fluoropyrimidine plus platinum doublet’ (p = 0.04). The network forest plot and league table are shown in Figures 4 and 5, respectively. These results were also consistent with pairwise meta-analysis, where ‘fluoropyrimidine plus platinum-based triplet’ was better than ‘fluoropyrimidine plus platinum doublet’ (random HR 95% CI: 0.86 (0.75–0.98), p = 0.03; Supplementary Table 3).

Network forest plot of overall survival in general analysis.

Network league table of overall survival in general analysis.
Sensitivity analysis
After changing to a fixed-effects model (network HR 95% CI: 0.91 (0.84–0.98), P-score = 0.916) or removing clinically heterogeneous studies (network HR 95% CI: 0.90 (0.82–0.99), P-score = 0.903), ‘fluoropyrimidine plus platinum-based triplet’ remained as the top node with statistical advantage against ‘fluoropyrimidine plus platinum doublet’ (figures not shown).
General analysis: secondary endpoint
PFS
A total of 63 studies were included in the network calculation. ‘Fluoropyrimidine plus platinum-based triplet plus targeted medication’ became the best regimen in the entire hierarchy (network HR 95% CI: 0.75 (0.54–1.04), P-score = 0.919), closely followed by ‘fluoropyrimidine plus platinum-based triplet’ (network HR 95% CI: 0.83 (0.71–0.96), P-score = 0.881). However, only ‘fluoropyrimidine plus platinum-based triplet’ had shown statistical superiority against ‘fluoropyrimidine plus platinum doublet’ (p = 0.01) (Supplementary Figure 2).
ORR
A total of 89 studies were eligible and merged into the hierarchical comparisons. ‘Fluoropyrimidine plus platinum-based triplet plus targeted medication’ (network RR 95% CI: 1.48 (1.11–1.98), P-score = 0.964) and ‘fluoropyrimidine plus platinum-based triplet’ (network RR 95% CI: 1.20 (1.06–1.36), P-score = 0.857) again ranked as the top two nodes in the entire hierarchy, both of which demonstrated statistical advantage against common comparator ‘fluoropyrimidine plus platinum doublet’ (FP3R: p = 0.008; FP3: p = 0.004) (Supplementary Figure 3).
Hematological adverse events
A total of 74 studies were included in the network meta-analysis. ‘Best supportive care’ was certainly the most tolerable node in the rankings (network RR 95% CI: 0.16 (0.02–1.28), P-score = 0.952). Meanwhile, based on the hierarchical data, both ‘fluoropyrimidine plus platinum-based triplet plus targeted medication’ (network RR 95% CI: 1.31 (0.75–2.29), P-score = 0.414) and ‘fluoropyrimidine plus platinum-based triplet’ (network RR 95% CI: 1.55 (1.25–1.90), P-score = 0.272) had worse rankings than ‘fluoropyrimidine plus platinum doublet’ while the difference between ‘fluoropyrimidine plus platinum-based triplet’ and ‘fluoropyrimidine plus platinum doublet’ was statistically meaningful (p = 0.0001) (Supplementary Figure 4).
Nonhematological adverse events
A total of 78 studies were included in the network meta-analysis. Undoubtedly, ‘Best supportive care’ was the most tolerable node concerning nonhematological adverse events (network RR 95% CI: 0.07 (0.01–0.50), P-score = 0.993). Both ‘fluoropyrimidine plus platinum-based triplet’ (network RR 95% CI: 1.15 (0.99–1.34), P-score = 0.315) and ‘fluoropyrimidine plus platinum-based triplet plus targeted medication’ (network RR 95% CI: 1.44 (1.02–2.03), P-score = 0.176) displayed lower rankings than ‘fluoropyrimidine plus platinum doublet’ while the difference between ‘fluoropyrimidine plus platinum-based triplet plus targeted medication’ and ‘fluoropyrimidine plus platinum doublet’ was statistical meaningful (p = 0.04) (Supplementary Figure 5).
Additional analysis
Although the results from general analysis seemed to be very consistent, however, since there were several subtypes of medications included in fluoropyrimidines and platinum, we decided to perform an additional analysis by only including studies with pairwise comparisons between fluoropyrimidine plus platinum-based regimens. This not only helped to lower the heterogeneity across the network but also enhanced the clinical specificity and availability. Overall 39 randomized controlled trials were eligible for additional analysis, containing a total of 10,959 patients. ‘5-FU plus cisplatin’ (FC2) was chosen as the common comparator. Since fluoropyrimidine plus oxaliplatin doublet (especially capecitabine plus oxaliplatin) was commonly used in clinical applications, we also observed relative results between fluoropyrimidine plus oxaliplatin doublet and other alternative regimens by network league tables. Similar to that of general analysis, the majority of studies featured metastatic and measurable gastric cancer cases, exhibiting a low level of clinical heterogeneity and therefore a well transitivity (Table 2). Overall, none of the included studies were at high risk of bias regarding methodological design (Supplementary Table 4).
Baseline characteristics of eligible studies for additional analysis (unselected population).

E/T, events/total patients; G/J, gastric/junction; hAE, hematological adverse events; HR, hazard ratio; I/D, intestinal/diffused; M/F, male/female; NA, not available; non-hAE, nonhematological adverse events; ORR, objective response rate; OS, overall survival; PFS: progression-free survival; P/T, responsive patients/total patients; Y/N, yes/no.
Primary endpoint: OS
A total of 38 studies were included in the network calculation. The pooled results were in low heterogeneity and high consistency (I2 = 0.16%, Q heterogeneity: p = 0.405, Q inconsistency: p = 0.508). ‘Capecitabine plus cisplatin-based triplet plus targeted medication’, ‘5-FU plus oxaliplatin-based triplet’, and ‘Capecitabine plus oxaliplatin-based triplet’ closely ranked as the top three regimens in the entire hierarchy, all of which displayed superiority against ‘5-FU plus cisplatin’ and ‘Capecitabine plus cisplatin’. However, none of them displayed superiority against ‘5-FU plus oxaliplatin’, ‘S-1 plus oxaliplatin’, or ‘Capecitabine plus oxaliplatin’ (Supplementary Figures 6 and 7).
Secondary endpoint: PFS
A total of 36 randomized controlled trials were merged into the pooled analysis. Again, ‘Capecitabine plus cisplatin-based triplet plus targeted medication’, ‘5-FU plus oxaliplatin-based triplet’, and ‘Capecitabine plus oxaliplatin-based triplet’ were the best three nodes in the rankings, statistically superior to ‘5-FU plus cisplatin’ and ‘Capecitabine plus cisplatin’. In addition, except for ‘Capecitabine plus cisplatin-based triplet plus targeted medication’, none of the top three regimens demonstrated enough advantage against ‘5-FU plus oxaliplatin’, ‘S-1 plus oxaliplatin’, or ‘Capecitabine plus oxaliplatin’ (Supplementary Figures 8 and 9).
Secondary endpoint: ORR
A total of 37 studies were eligible for the network calculation. ‘Capecitabine plus cisplatin-based triplet plus targeted medication’, ‘5-FU plus oxaliplatin-based triplet’, and ‘Capecitabine plus cisplatin plus targeted medication’ reigned the hierarchy with statistical advantage against ‘5-FU plus cisplatin’. However, none of them displayed superiority against ‘5-FU plus oxaliplatin’, ‘S-1 plus oxaliplatin’, or ‘Capecitabine plus oxaliplatin’ (Supplementary Figures 10 and 11).
Secondary endpoint: hematological adverse events
A total of 34 trials were included into the pooled analysis. ‘Capecitabine plus cisplatin-based triplet plus targeted medication’ appeared to have statistical inferiority against ‘5-FU plus cisplatin’, ‘5-FU plus oxaliplatin’, ‘S-1 plus oxaliplatin’, and ‘Capecitabine plus oxaliplatin’ (Supplementary Figures 12 and 13).
Secondary endpoint: nonhematological adverse events
A total of 35 studies were eligible for network meta-analysis. ‘Capecitabine plus cisplatin-based triplet plus targeted medication’ was statistically inferior to ‘S-1 plus oxaliplatin’ while comparable to ‘5-FU plus cisplatin’, ‘5-FU plus oxaliplatin,’ and ‘Capecitabine plus oxaliplatin’ (Supplementary Figures 14 and 15).
Patients with specific positivity
There were a total of eight randomized controlled trials were analyzed in this section of the systematic review, including four HER-2 positive studies, two MET-1 positive studies, one CLDN18.2 positive study, and one EGFR positive study (Table 3). None of the included studies were at high risk of bias with regard to methodological design (Supplementary Table 5).
Baseline characteristics of eligible studies for patients with specific positivity.

E/T, events/total patients; G/J, gastric/junction; hAE, hematological adverse events; HR, hazard ratio; I/D, intestinal/diffused; M/F, male/female; NA, not available; non-hAE, non-hematological adverse events; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; P/T, responsive patients/total patients; Y/N, yes/no.
HER-2 positive
Three studies were large-scale phase III randomized controlled trials and only one trial reported phase II results, with sample sizes ranging from 28 to 780 patients. According to Bang et al, 40 adding trastuzumab to capecitabine plus cisplatin could significantly enhance its survival benefits among HER-2 positive patients compared with capecitabine plus cisplatin alone (OS HR: 0.74 [95% CI, 0.60–0.91]; PFS HR: 0.71 [95% CI, 0.59–0.85]). Recently, Tabernero et al. 41 also confirmed that dual HER-2 targeting strategy with both pertuzumab and trastuzumab failed to generate OS benefit compared with trastuzumab-based regimen, despite the difference of OS coming close to crossing the boundary value (OS HR: 0.84 (95% CI, 0.71–1.00); PFS HR: 0.73 (95% CI, 0.62–0.86)). Moreover, either pertuzumab or trastuzumab was well tolerable compared with its control arm. On the other hand, however, adding lapatinib failed to produce survival benefits in contrast to capecitabine plus oxaliplatin alone 42 (OS HR: 0.91 [95% CI, 0.73–1.12]; PFS HR: 0.84 [95% CI, 0.69–1.03]), irrespective of gastric (p = 0.30), gastroesophageal junction (p = 0.77), or esophageal cancer subgroups (p = 0.77). Similarly, the addition of lapatinib to capecitabine-based triplet also failed to have enough survival benefit (OS HR: 0.90 [95% CI, 0.35–2.27]; PFS HR: 0.86 [95% CI, 0.37–1.99]), despite that the results were less credible owing to lower statistical power on small sample size (n = 28) 43 (Table 3).
MET-1 positive
Two large-scale phase III randomized controlled trials reported the first-line options for MET-1-positive gastric cancer patients. Based on 609 patients, Catenacci et al. 44 surprisingly described that adding rilotumumab not only failed to increase but also significantly decreased the survival time among MET-1-positive patients compared with capecitabine plus cisplatin plus epirubicin alone (OS HR: 1.34 [95% CI, 1.10–1.63]; PFS HR: 1.26 [95% CI, 1.04–1.51]). Furthermore, Shah et al. 45 reported that addition of onartuzumab also failed to display survival benefit among MET-1-positive patients compared to 5-FU plus oxaliplatin plus leucovorin alone (OS HR: 0.82 [95% CI, 0.59–1.15]; PFS HR: 0.90 [95% CI, 0.71–1.16]) (Table 3).
Others
Based on a CLDN18.2-positive 161-patient phase II trial, adding IMAB362 could significantly enhance the survival time while maintaining comparable tolerability against capecitabine plus oxaliplatin plus epirubicin alone 46 (OS HR: 0.51 [95% CI, 0.36–0.73]; PFS HR: 0.47 [95% CI, 0.31–0.70]). For EGFR-positive patients, the addition of matuzumab failed to generate survival benefits compared with capecitabine plus cisplatin plus epirubicin alone 47 (OS HR: 1.02 [95% CI, 0.61–1.70]; PFS HR: 1.13 [95% CI, 0.63–2.01]) (Table 3).
Discussion
Currently, systemic therapy is still the preferred measure against advanced inoperable gastric cancer, in which fluoropyrimidine plus cisplatin doublet is the most recommended regimen in virtue of both clinical efficacy and tolerability. 5 However, previously published systematic reviews failed to make a panoramic summary about the systemic therapy against gastric cancer, let alone a credible hierarchical ranking that fit the diversity of regimens.16–18 Therefore, we have conducted by far the most comprehensive systematic review and network meta-analysis based on 119 high-quality randomized controlled trials, covering both chemotherapy and targeted medications.
In general, analysis among unselected population, ‘fluoropyrimidine plus platinum-based triplet’ was the top-ranking node regarding OS, which was consistent with the result of pairwise meta-analysis and was confirmed to be stable by sensitivity analysis. In terms of PFS and ORR, ‘fluoropyrimidine plus platinum-based triplet plus targeted medication’ and ‘fluoropyrimidine plus platinum-based triplet’ ranked as the top two nodes, demonstrating statistical superiority against ‘fluoropyrimidine plus platinum doublet’. However, in 2014, one ASCO expert meeting stated that a risk reduction of HR 0.80 might be clinically relevant. In addition, the ESMO clinical benefit scale even recommends that HR 0.65 is clinically relevant. Therefore, in consideration of survival efficacy and safety profile, it is still inappropriate to conclude that ‘fluoropyrimidine plus platinum doublet’ could be replaced by ‘fluoropyrimidine plus platinum-based triplet’ in terms of first-line regimens. Moreover, since the general analysis did not further clarify different subtypes inside fluoropyrimidine and platinum, we still had concerns about the statistical credibility about the pooled results and, thus, we performed a specific additional analysis.
The additional analysis that individualized different types of fluoropyrimidine and platinum gave detailed comparisons across diverse fluoropyrimidine and platinum-based regimens. Concerning survival benefits, ‘capecitabine plus cisplatin-based triplet plus targeted medication’ was the best regimen in the entire hierarchy, statistically superior against both ‘5-FU plus cisplatin’ and ‘capecitabine plus cisplatin’ while comparable with ‘5-FU plus oxaliplatin’, ‘S-1 plus oxaliplatin’, and ‘Capecitabine plus oxaliplatin’. On the other hand, it also featured unfavorable tolerability as expected, especially compared with ‘S-1 plus oxaliplatin’. However, although more specific categorizations helped to lower heterogeneity, it also raised concerns about low statistical power owing to the small sample-size in each node. In addition, the third component and targeted medication besides fluoropyrimidine and platinum were not always consistent within the same node, which could introduce heterogeneity into the final results as well. Therefore, we feel that it is more appropriate to maintain the recommendation of fluoropyrimidine plus oxaliplatin doublet (especially capecitabine or S-1) as the preferred first-line regimen, which has been widely applied in clinical settings.
Among patients with specific pathological positivity, HER-2 is the most widely investigated target against advanced gastric cancer. Based on a large-scale phase III randomized controlled trial by Bang et al., 40 the addition of trastuzumab to fluoropyrimidine plus cisplatin doublet has been confirmed as the preferred regimen against HER-2 overexpressing metastatic gastric cancer. Despite the negative result of OS (p = 0.056), a dual HER-2-targeting strategy with both pertuzumab and trastuzumab displayed a significant benefit in terms of PFS, as well as the comparable tolerability compared with trastuzumab-based first-line regimen. 41 Since the difference in OS was quite close to statistical boundary, it hinted that other combination of dual HER-2-targeting strategy might possibly reach statistical significance in future designs. In addition, lapatinib plus capecitabine plus oxaliplatin failed to surpass capecitabine plus oxaliplatin doublet, 42 therefore fluoropyrimidine plus cisplatin plus trastuzumab is still the best regimen for HER-2 overexpressing advanced gastric cancer at present. According to two large-scale phase III studies, adding rilotumumab or onartuzumab failed to generate survival benefits among MET-1-positive patients compared with fluoropyrimidine plus platinum-based chemotherapy alone.44,45 This suggests that fluoropyrimidine plus cisplatin may still serve as the preferred first-line regimen against MET-1-positive advanced gastric cancer. Moreover, in a phase II trial by Schuler et al. 46 , the addition of IMAB362 significantly elongated survival lifespan among patients with CLDN18.2 positivity compared with capecitabine plus oxaliplatin plus epirubicin alone. Since CLDN18.2 is believed to widely exist in nearly half of gastric cancer cells, IMAB362 is a very promising medication and, thus, a phase III trial is currently ongoing.
Although our systematic review was rigorously designed and conducted, there were still some limitations within. First, this network meta-analysis was not based on individual-patient data. However, since the network was verified to be highly consistent, stable, and homogenous, conclusions of our pooled analysis were therefore also credible and applicable. Second, even though in additional analysis, several different regimens were still forced to merge into one node in order to perform the network calculations, since the third component and targeted medication in addition to fluoropyrimidine and platinum were not further specified. All these could bring potential biases into the network meta-analysis despite of the low overall statistical heterogeneity as mentioned previously. Third, the overall number of studies especially for top-ranking nodes such as ‘capecitabine plus cisplatin-based triplet plus targeted medication’ were still inadequate, which might lower the statistical power of the entire quantitative analysis.
Taken together, fluoropyrimidine plus oxaliplatin doublet (especially capecitabine or S-1) should still be considered as the preferred first-line regimen owing to its comparable survival benefits and lower toxicity.
Supplemental Material
Supplemetary_Materials – Supplemental material for First-line systemic therapy for advanced gastric cancer: a systematic review and network meta-analysis
Supplemental material, Supplemetary_Materials for First-line systemic therapy for advanced gastric cancer: a systematic review and network meta-analysis by Ji Cheng, Ming Cai, Xiaoming Shuai, Jinbo Gao, Guobin Wang and Kaixiong Tao in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We thank all staff in our department for providing clinical and methodological advices during the entire performance of our meta-analysis.
Author contributions
Study design: Ji Cheng, Guobin Wang and Kaixiong Tao; Manuscript writing and revision: Ji Cheng and Kaixiong Tao; Literature retrieval: Ji Cheng and Ming Cai; Discretion of eligibility: Ji Cheng and Ming Cai; Quality assessment: Ji Cheng and Xiaoming Shuai; Data extraction: Ji Cheng and Jinbo Gao; Statistical analysis: Ji Cheng and Kaixiong Tao.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: The meta-analysis was funded by National Natural Science Foundation of China (81902487) and the Scientific Research Training Program for Young Talents (Union Hospital, Tongji Medical College, Huazhong University of Science and Technology) to Ji Cheng and the National Natural Science Foundation of China (grant number 81572413) to Kaixiong Tao.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.