
Abstract
Pancreatic cancer is one of the most lethal solid organ tumors. Due to the rising incidence, late diagnosis, and limited treatment options, it is expected to be the second leading cause of cancer deaths in high income countries in the next decade. The multidisciplinary treatment of this disease depends on the stage of cancer at diagnosis (resectable, borderline, locally advanced, and metastatic disease), and combines surgery, chemotherapy, chemoradiotherapy, and supportive care. The landscape of multidisciplinary pancreatic cancer treatment is changing rapidly, especially in locally advanced disease, and the number of treatment options in metastatic disease, including personalized medicine, innovative targets, immunotherapy, therapeutic vaccines, adoptive T-cell transfer, or stemness inhibitors, will probably expand in the near future. This review summarizes the current literature and provides an overview of how new therapies or new therapeutic strategies (neoadjuvant therapies, conversion surgery) will guide multidisciplinary disease management, future clinical trials, and, hopefully, will increase overall survival.
Keywords
Introduction
Pancreatic cancer remains one of the greatest challenges in oncology, and is presently the fourth leading cause of cancer deaths in the United States. This review will cover different ways to increase survival or to manage this aggressive disease. We will review the criteria of surgical quality, new data on surgical care, progresses in adjuvant therapy, and the optimal timing of adjuvant chemotherapy. We will also provide an update on systemic therapies for advanced pancreatic cancer, and a comprehensive analysis of published clinical trials in second-line therapy, updates on new options in personalized medicine, management of borderline resectable pancreatic cancer, available data on the effectiveness of neoadjuvant therapies, new data on locally advanced pancreatic cancer, especially the role of conversion surgery, and, finally, supportive and palliative care.
Pancreatic cancer is expected to be the second or the third leading cause of cancer deaths in high-income countries in the next decade.1,2 Pancreatic ductal adenocarcinoma (PDAC) and its variants are the most frequent type, representing 85–90% of all pancreatic neoplasms. Median age at diagnosis is 70–71 years.3,4
The incidence of pancreatic cancer is increasing rapidly, particularly in Europe, North America, Australia, and New Zealand.5–7 This higher incidence is associated with socioeconomic development, and is due partly to increased life expectancy, as well as to the overweight/obesity epidemic. Despite recent advances in the management of PDAC, poor survival rates continue, with 8–11% of patients in Europe and United States alive at 5 years after diagnosis.6–8 Owing to the lack of early symptoms, and to the metastatic potential of PDAC cells, up to 80% of patients receive a diagnosis at an advanced stage, by which time the tumor is unresectable. 9
Advances in surgical management of pancreatic cancer
Surgery is the only potentially curative treatment for pancreatic adenocarcinoma, although only 10–20% of patients have clearly resectable disease after careful pretherapeutic staging. 9
Resectable adenocarcinoma [according to National Comprehensive Cancer Network (NCCN) classification 2019] 10 is defined by the absence of distant organ or distal lymph node metastases; the absence of evidence of superior mesenteric vein and portal vein distortion; tumor thrombus, or venous encasement > 180°; and the existence of clear fat planes around the celiac axis, hepatic artery, and superior mesenteric artery (SMA).
However, even after curative surgery, the oncological results of surgery alone are disappointing, with a median survival of 15–20 months and a 5-year survival of 8–15%, owing to the high frequency of local and distant relapses.9,11–13 Therefore, surgery must be integrated into a complete treatment sequence, also known as multimodal treatment. 14 With surgery and adjuvant chemotherapy, notable progress has been observed over the past 5 years, with a large increase in median overall survival in the most recent adjuvant trials.15–17 Complications after pancreatic resections are also reduced by progress made in perioperative and critical care, and in the standardization of surgical techniques.
Criteria of surgical quality are now internationally accepted and should be respected. However, the main progress that must be made is improvement in the selection of operable patients and a reduction of postoperative complications.
Criteria of surgical quality
Pancreaticoduodenectomy
In patients with adenocarcinoma located in the head of the pancreas, pancreaticoduodenectomy (PD) is the recommended surgical technique, and skeletalization of the SMA down to adventitia on anterior, lateral, and posterior borders is the standard of care.18,19 The SMA first approach facilitates lymphadenectomy, and optimizes oncological control of the retroperitoneal margin. In a recent meta-analysis, intraoperative blood loss, pancreatic fistula, delayed gastric emptying, and local recurrence were significantly lower with the SMA first approach than with standard PD. 20
Dissection of more than 15 lymph nodes is recommended,21,22 and standard lymphadenectomy must include lymph nodes of the following stations of the Japan Pancreas Society nomenclature 23 : suprapyloric (5), infrapyloric (6), along the common hepatic artery (8a), along the bile and cystic ducts (12b and 12c), on the posterior surface of the pancreatic head (13a, 13b), at the origin of the superior mesenteric artery (SMA) (14a), on the right side of the SMA (14b), and on the anterior surface of the pancreatic head (17a and 17b). 22 More aggressive surgery (i.e. extensive lymphadenectomy) does not improve long-term survival and is not recommended. 24 Para aortic lymph node sampling with frozen section examination is an option, and some authors recommend performing such sampling in all cases of PD due to the negative impact on survival of these metastases.25–27
Distal pancreatectomy
In patients with adenocarcinoma located in the left pancreas (body or tail), distal pancreatectomy with splenectomy is recommended. To obtain a histologically complete resection (R0 surgical margin status), Strasberg and colleagues described a modification of the standard technique based on an anterograde approach, complete dissection of N1 lymph node stations and enlargement to the left prerenal fascia of the posterior dissection plane (radical anterograde modular pancreatosplenectomy), which improves the retroperitoneal resection margin.28,29 However, the potential survival benefit of this procedure should be evaluated in a prospective study.
Regional lymphadenectomy carries the gastrosplenic lymph nodes and those from the left edge of the celiac trunk to that of the superior mesenteric artery. Lymphadenectomy must include lymph node levels 9, 10, 11, and 18.21,22,24–33 Dissection of ⩾15–20 lymph nodes and skeletalization of the SMA down to adventitia on anterior, left lateral, and posterior borders is recommended. 30
Surgical resection margin status
The main resection margins (at minimum, superior mesenteric vein, posterior pancreatic surface and the medial margin) of surgical specimens should be inked, examined, and reported using a standardized pathological protocol in agreement with guidelines of the College of American Pathologists, American Joint Committee on Cancer (AJCC), or the Royal College of Pathologists, to better assess the margin status.34,35 Tumor clearance is defined by the precise distance between the margin and the tumor cells. 31
The aim of surgery is to achieve complete resection of the tumor with microscopically negative margins (R0). According to the most recent publications, following PD, R0 resection should be defined as clearance (margin of healthy tissue around the removed tumor) of >1 mm.31–33 In cases with R1 margin status, additional information should be reported to distinguish cases with a tumor-free margin <1 mm [R1 (<1 mm)] and cases with tumor cells directly at the margin [R1 (direct)], direct invasion having a poorer prognosis. 32 This cut-off was recently validated as an independent determinant of survival after resection for pancreatic adenocarcinoma of the body and tail. 36
Laparoscopic approach for pancreatic cancer
Laparoscopic PD
According to data from the US National Cancer Database, higher mortality is associated with laparoscopic PD in low volume centers, as defined by thresholds of 10–25 procedures per year, depending on the study.37–40 In the most complete report, including only pancreatic cancers operated from 2010 to 2012, 40 there was no difference in terms of the rate of positive surgical margins (20.4% versus 22.1%, p = 0.15), a higher number of lymph nodes was removed in minimally invasive surgery in centers with low activity volume (17.4 versus 16.5, p < 0.01), and there were no differences in 30-day readmission rate (8.7% versus 9.5%, p = 0.42), 30-day mortality (2.7% versus 2.5%, p = 0.35) or 90-day mortality (5.1% versus 4.7%, p = 0.22). However, in multivariate analysis, minimally invasive surgery was associated with a significantly higher risk of short-term mortality [hazard ratio (HR), 1.95; p < 0.01]. There was no impact on the use of adjuvant chemotherapy. Equivalent results for long-term survival have not been demonstrated.
Despite growing interest in the minimally invasive approach for PD, the data in the literature are limited to comparative single-center studies, with few cases of pancreatic adenocarcinoma; hence, laparoscopic PD is not standard.
Laparoscopic distal pancreatectomy
A recent meta-analysis reported a significantly shorter hospital stay for patients who underwent laparoscopic versus open distal pancreatectomy. 41 However, there were no differences in mortality, severe morbidity at 3 months, overall morbidity, clinically significant pancreatic fistulas, and R1 resections. In a multicenter European case-control study, intraoperative blood loss (200 versus 300 ml, p = 0.001) and length of hospital stay (8 versus 9 days, p < 0.001) were significantly lower with minimally invasive versus open resection. No differences were observed in major morbidity and 90-day mortality. The R0 resection rate was significantly higher (67% versus 58%, p = 0.019), but the prerenal fascia resection rate (31% versus 60%, p < 0.001) and the number of lymph nodes removed (14 versus 22, p < 0.001) were lower in the minimally invasive group. Median overall survival was comparable between the two surgical approaches. 42
With regard to oncological results, the laparoscopic approach is now considered as an option for small pancreatic cancers of the left pancreas in high-volume centers.
Control of postoperative complications and access to adjuvant treatment
Despite improvements in mortality rates associated with pancreatectomy during the past decade, postoperative morbidity rates remain high.43–45 Given that postoperative complications may have a profound effect on quality of life, 46 access to adjuvant therapy, 47 and, ultimately, patient outcome, 48 reducing morbidity following surgery for pancreatic cancer should be a priority for surgeons.
Reduction of postoperative complications
Several surgical risk scales have been proposed to best select candidates for surgery and to screen patients at high risk of complications.
Some classifications, such as that published by Braga and colleagues, 49 as well as preoperative pancreatic resection (PREPARE) and SOAR (surgical results analysis and search) scoring systems,50,51 are based on the integration of multiple parameters and appear to be more precise than other methods.
For cancers with a particularly poor prognosis such as pancreatic cancer, the risks and benefits of surgical resection must be critically evaluated. Given that postoperative complications are associated with a reduction in patients’ access to adjuvant therapy and survival, immediate pancreatectomy should be discouraged for particularly high-risk surgical patients, that is, patients with altered performance status, severe pre-existing comorbidities, or advanced age. These patients should be managed actively by a multidisciplinary group of expert physicians, including a specialist dietitian following a pancreas-tailored treatment program, physical therapist, and other specialists as required.
Assessment of nutritional status
Before surgical resection, it is essential to achieve adequate nutritional status, and nutritional supplements, or even parenteral nutrition, should be considered for at least 1–2 weeks before surgery in patients who are malnourished.
Weight loss, low body mass index, and loss of muscle mass have been shown to correlate with poor surgical and oncological outcomes after operations for pancreatic cancer.52,53 Patients undergoing pancreatic surgery should receive a meticulous evaluation of their nutritional status and risk of developing malnutrition postoperatively. 54 In case of severe metabolic risk, 10–14 days of nutritional therapy are beneficial. 55
Enhanced recovery after surgery
Enhanced recovery programs (ERPs) are an amalgamation of pre-, intra-, and postoperative measures intended to improve the postoperative course of patients. ERPs originated in Northern Europe and represent a revolution in surgical care. 56 They bring together a technical component (a care protocol including multimodal analgesia, minimally invasive surgery, optimization of perioperative fluid loading, limited use of tubes and drains, reduction of insulin resistance) and an organizational component (team mindset, preoperative conditioning, early mobilization and refeeding, keeping the patient up to date with the anticipated discharge schedule, active patient participation in the healthcare process, and risk management after discharge). 57 Several studies have demonstrated multiple advantages of ERPs, including decreased overall morbidity, quicker return to normal activities, and decreased duration of hospital stay. 58 In addition, some studies suggest that ERPs could improve the prognosis of patients treated for digestive cancer through better nutritional management, a reduction in postoperative complications, possible earlier use of adjuvant treatment, and an improvement in perioperative immune status. 59
Although few data are available on the surgical management of pancreatic cancer, ERP has emerged as standard care, particularly in pancreatic surgery. Oncology benefit data should be available from current prospective registries.
Biliary drainage
Systematic biliary stenting has been proposed in patients with serum bilirubin levels of >300 µmol/l, but preoperative biliary drainage has since been shown to significantly increase the morbidity rate compared with patients undergoing surgery first.60–62 However, this higher morbidity rate does not appear to affect long-term survival. 63 Patients with severe jaundice may have jaundice-related medical conditions, such as renal failure or malnutrition that may require preoperative biliary drainage before surgery. Thus, preoperative biliary drainage should be considered only when necessary in symptomatic patients or if surgery must be postponed because of any medical condition. Self-expandable metallic stents are currently considered the standard of care in line with published data on biliary stent patency. 64
Centralization of pancreatic surgery
Several nationwide studies have reported a hospital volume–outcome relationship after pancreatectomy, with significantly lower postoperative mortality in high-volume compared with low-volume centers.65–67 Recent reports indicate that postoperative mortality after pancreatic resection is mostly attributable to ‘failure to rescue’ patients with major complication(s), rather than to hospital volume by itself. Failure to rescue is defined as mortality among patients with one or more major complications within 90 days of surgery, and corresponds to ineffective management of postoperative complications. 68 El Amrani and colleagues demonstrated that higher failure-to-rescue rates are associated with lower hospital volume, highlighting variability in the management of postoperative complications. 69 The failure-to-rescue approach suggests that, in addition to a high-volume center and high-volume surgeons, a multidisciplinary team, an intensive care unit, and a surgical service that is available at all times, are key to good functioning of the infrastructure. Consequently, many authors and national healthcare societies have promoted the centralization of pancreatic surgery to high-volume centers to improve outcomes.69–71 National assessments are needed to clarify the impact and feasibility of centralizing pancreatic surgery, particularly for pancreatic cancer.
Progresses in adjuvant therapy
Patients undergoing curative resection for pancreatic cancer mostly develop recurrent tumor disease; 69–75% of patients relapse within 2 years and 80–90% relapse within 5 years. The main randomized phase III studies are shown in Table 1.
Where are we on adjuvant chemoradiotherapy?
Locoregional tumor recurrence is considered a main cause of relapse, with up to 80% of curatively resected patients undergoing an R1 resection. The potential of adjuvant radiotherapy to reduce locoregional recurrence was first tested in a gastrointestinal tumor study group (GITSG) randomized study using fluorouracil as a radiosensitizer in patients with negative resection margins. The GITSG GI 9173 trial compared observation with split-course radiotherapy of 40 Gy delivered over 6 weeks. 72 Bolus fluorouracil was administered on each of the first 3 days of the two sequences of radiotherapy and weekly for 2 years or until recurrence thereafter. The study ended prematurely after the inclusion of 43 patients because the interim analysis showed a statistically significant survival difference (p = 0.035) in favor of the chemoradiation and adjuvant chemotherapy arm. Similar results were achieved in a second nonrandomized cohort of 30 patients. 73
A European Organisation for Research and Treatment of Cancer (EORTC) trial also addressed the question of whether adjuvant chemoradiotherapy provided benefits following surgical resection in 114 patients with R0 or R1 resection. Patients in the chemoradiation arm received 40 Gy plus continuous fluorouracil infusion. Treatment was well tolerated, but no significant overall survival benefit was observed, either for patients who had adenocarcinoma located in the head of the pancreas or for the treatment group as a whole. However, the study lacked sufficient statistical power to reach definitive results. 80
The European Study Group for Pancreatic Cancer 1 (ESPAC-1) trial compared, with a two-by-two factorial design, three adjuvant strategies with observation: chemoradiotherapy, chemotherapy alone, and chemoradiotherapy followed by adjuvant chemotherapy. To encourage participation, patients could receive prior treatments before randomization (‘background’ therapy), and the trial was expanded to include two other randomization options of chemoradiotherapy versus observation, and chemotherapy versus observation. Chemoradiotherapy consisted of split-course external-beam radiotherapy of 2 × 20 Gy dose with bolus fluorouracil on the first 3 days of radiotherapy.74,75,80 A total of 353 patients were included in the chemoradiotherapy analysis. Background therapy was used in 41.9% of the patients. Unfortunately, after a median follow-up of 47 months, adjuvant chemoradiotherapy had a significant deleterious effect on survival [HR, 1.28; 95% confidence interval (CI), 0.99–1.66; p = 0.05].74,75 The main critiques of this trial were the absence of radiation quality control and the heterogeneous treatments fields.
The RTOG 9704 trial was designed to determine whether the addition of gemcitabine to postoperative radiation with fluorouracil improved survival compared with adjuvant fluorouracil. A total of 451 patients received 50.4 Gy radiation with concurrent continuous fluorouracil infusion after R0 or R1 resection, and were randomly assigned either fluorouracil or gemcitabine for 3 weeks before chemoradiation, then for 12 weeks after chemoradiation. 81 There was no difference in overall disease-free survival between treatment groups. In the subgroup with tumors located in the head of the pancreas (n = 388), a survival benefit trend (p = 0.08) was observed for the gemcitabine group. Patients with a postoperative carbohydrate antigen (CA) 19-9 serum level of ⩾180 U/ml had significantly worse survival than those with a CA 19-9 of <180 U/ml. 82
Adjuvant chemoradiotherapy with concurrent weekly gemcitabine was also tested in an European randomized phase II study, comparing two cycles of adjuvant gemcitabine followed by chemoradiation to four cycles of adjuvant gemcitabine. 83 This trial showed that adjuvant gemcitabine followed by gemcitabine-based chemoradiotherapy is feasible and well tolerated. Local recurrence as first cause of relapse was less frequent in the chemoradiation arm (11% versus 24%). This schedule is under investigation by the RTOG/EORTC 0848 trial, which is evaluating both erlotinib and chemoradiation as adjuvant treatments for patients with resected adenocarcinoma in the head of the pancreas. No benefit was observed for erlotinib after the inclusion of 336 patients, and further patients are being recruited to answer the chemoradiation question. 84
A retrospective analysis of the US National Cancer Database suggested that addition of radiotherapy to adjuvant chemotherapy is associated with improved overall survival. 85 Patients with resected pancreatic adenocarcinoma from 1998 to 2009, and with at least 3 months of follow up, were included; 2334 patients received chemotherapy alone, and 3831 received chemotherapy and radiation. The median overall survival was 22.3 months with chemotherapy and radiation versus 20.0 months with adjuvant chemotherapy alone (p = 0.001). The benefit of radiotherapy was greater for patients with R1 margins, or pT3 or pN1 tumors. Radiotherapy was associated with an overall survival benefit when radiotherapy began 1–3 months after the beginning of chemotherapy. Information on the radiotherapy target volume and radiotherapy technique were not available. A probable bias is the absence of data on disease-free survival, so the chemotherapy alone cohort may have included patients with early postoperative progression and palliative chemotherapy.
The above demonstrate the conflicting results that have been reported over the past three decades regarding the combination of chemotherapy and radiation therapy as adjuvant therapy; hence, the impact and the optimal schedule and timing of postoperative chemoradiation remain uncertain. Further trials are required to ascertain the role of chemoradiotherapy after resection of pancreatic cancer.
Progresses on adjuvant chemotherapy
Upfront resection followed by adjuvant chemotherapy is the gold standard for patients with resectable pancreatic cancer. Considerable advances have been made during the past decade and are summarized in Table 1.
Major randomized phase III trials of adjuvant treatments for pancreatic cancer.

p value between chemotherapy and no chemotherapy; chemoradiotherapy had a deleterious effect (p = 0.05).
Percentage of patients receiving full number of planned cycles.
5-FU, fluorouracil; CONKO, Charité Onkologie; DFS, Disease-Free Survival; GITSG, GastroIntestinal Tumor Study Group; ESPAC, European Group for Pancreatic Cancer; JASPAC, Japan Adjuvant Study of Pancreatic Cancer; NR, not reported; PRODIGE, Partenariat de Recherche en Oncologie DIGEstive; OS, overall survival.
Single-agent chemotherapy
The ESPAC-1 trial first demonstrated an overall survival benefit of adjuvant chemotherapy using fluorouracil and folinic acid. 74 A total of 473 patients were included in the chemotherapy analyses (238 were randomly assigned to adjuvant chemotherapy and 235 were randomly assigned to no chemotherapy). 75 Patients who received fluorouracil and folinic acid had significantly improved median overall survival compared with surgery alone (20.1 versus 15.5 months, respectively; p = 0.009). The 5-year survival rate was 21% among patients who received adjuvant chemotherapy and 8% among patients not receiving chemotherapy (p = 0.009).
The German CONKO-001 trial compared adjuvant gemcitabine administered for six cycles, 3 weeks out of 4, with observation alone.13,76 A total of 368 patients with completely resected pancreatic cancer were included. Patients with a CA 19-9 serum level greater than 2.5 times the upper limit of normal value were not eligible for this trial. Patients receiving gemcitabine had significantly increased median disease-free survival (13.4 versus 6.9 months; p < 0.001). Overall survival was significantly improved, with a 5-year overall survival rate of 20.7% versus 10.4%, and 10-year overall survival rate of 12.2% versus 7.7%. These data were subsequently confirmed by a smaller study in Japan, JSAP-2. 86
The ESPAC-3 study randomly assigned 1888 patients to a 6-month course of fluorouracil and folinic acid, or gemcitabine. Results showed no differences in disease-free survival and overall survival between the two chemotherapy regimens. 77 Patients receiving fluorouracil plus folinic acid had significantly more serious adverse events than patients receiving gemcitabine (14% versus 7.5%), with significantly higher incidence of stomatitis and diarrhea (p < 0.001), whereas gemcitabine was associated with lower leukocyte counts and higher incidence of thrombocytopenia. No significant differences in global quality-of-life scores were observed. In 2010, these results established gemcitabine as the standard of care.
The Japan Adjuvant Study Group of Pancreatic Cancer performed the randomized non-inferiority phase III trial JASPAC-1 comparing adjuvant S-1, an oral tegafur-based fluoropyrimidine, with gemcitabine in patients with resected pancreatic cancer. 78 A total of 385 patients were included. Of these patients, 91.5% had stage II disease. S-1 was well tolerated and fewer patients in the S-1 group (28%) discontinued treatment before completion than in the gemcitabine group (42%; p = 0.005). With a median follow-up of 82.3 months, the overall survival rate at 5 years was 24.4% in the gemcitabine group versus 44.1% in the S-1 group. The HR for overall survival of S-1 compared with gemcitabine was 0.57 (95% CI, 0.44–0.72; p < 0.0001 for non-inferiority, p < 0.0001 for superiority). The median relapse-free survival was also doubled in the S-1 group (22.9 months versus 11.3 months; HR, 0.60; p < 0.0001). A major limitation is that all of the patients enrolled were Japanese. Given the different pharmacokinetics and pharmacodynamics of S-1 between Western cancer patients and those from Asia, concerns have been raised on potential excess of gastrointestinal toxicities with S-1 in the Western population. The applicability of these results to a non-Japanese population is unknown. 87
Combination systemic therapy
Different approaches to improve outcomes with adjuvant combination therapy in patients with operable pancreatic cancer have been tested in phase III trials, but few have been successful. The addition of targeted agents (erlotinib or sorafenib) or immunotherapy (algenpantucel-L) to gemcitabine did not improve overall survival compared with gemcitabine alone.88,89,90
A randomized phase II study evaluated the efficacy of uracil/tegafur (UFT) in addition to gemcitabine, compared with gemcitabine alone. A total of 100 patients were included. With a 21-month follow up, no differences were seen in disease-free survival and overall survival between the two treatments. 91 The ESPAC-4 compared gemcitabine and capecitabine with gemcitabine alone, irrespective of CA 19-9 levels. 16 A total of 730 patients were included, of whom 91.5% had stage III disease. The authors reported a slight increase in toxicities and a significant overall survival benefit with adjuvant gemcitabine plus capecitabine compared with gemcitabine alone (HR, 0.82; 95% CI, 0.68–0.98; p = 0.032). However, overall survival curves began to separate after 2 years, and no significant benefit in recurrence-free survival was seen. Recurrence-free survival were not significantly different between arms (HR, 0.86; 95% CI, 0.73–1.02; p = 0.082), suggesting differences in postrecurrence survival between the two groups. Imbalance in venous resection [39 patients in the combination group (11%), 63 patients in the control group (17%); p = 0.019], a strong prognostic factor, and the inclusion of patients with poor prognosis may have favored the combination group. In fact, high postoperative CA19-9 levels > 92.5 KU/l (up to 8,112 KU/l), a powerful independent prognostic factor in the study (HR, 0.62; 95% CI, 0.68–0.98; p = 0.007), were seen in 17% of patients, for whom median overall survival was only 13.1 months. Indeed, CA19-9 levels greater than 92.5 KU/l were associated with a significant overall survival benefit for the gemcitabine and capecitabine group. This point and the fact that a computed tomography (CT) scan was required within 3 months before randomization, but was not mandatory postoperatively, suggest that patients with early metastatic disease may have been enrolled.
Combination chemotherapy with fluorouracil, folinic acid, irinotecan, and oxaliplatin (mFOLFIRINOX, with no bolus fluorouracil and 150–180mg/m2 dose of irinotecan) was compared with gemcitabine in the PRODIGE24-CCTG PA6 trial. 17 Patients aged 18–79 years with ductal adenocarcinoma (R0 or R1 resection) resected within 12 weeks of randomization, and with no evidence of contraindication to the used drugs, no metastatic disease, no severe diarrhea, and postoperative serum CA 19-9 levels ⩽180 U/ml, were eligible for inclusion. Postoperative CT scans were mandatory before inclusion to exclude any tumor relapse. The primary endpoint was disease-free survival. A total of 493 patients were included in French and Canadian centers. After a median follow up of 33.6 months, median disease-free survival was 21.6 months in the mFOLFIRINOX group and 12.8 months in the gemcitabine group (stratified HR, 0.58; 95% CI, 0.46–0.73; p < 0.0001). The median disease-free survival for patients who received single-agent gemcitabine was in the range reported by previous adjuvant studies (11.3–15.3 months). There was no heterogeneity in the mFOLFIRINOX regimen effect in patient subgroups. Median overall survival was 54.4 months in the mFOLFIRINOX group and 35.0 months in the gemcitabine group (HR, 0.64; 95% CI, 0.48–0.86; p = 0.003). These results are the best disease-free survival and overall survival data reported so far for an adjuvant treatment of resectable pancreatic cancer. Grade 3–4 adverse events occurred in 75.9% of patients in the mFOLFIRINOX group and 52.9% of patients in the gemcitabine group but the toxicities were manageable, and the rate of grade 4 toxicities was the same for the two groups (12%). The predominant toxicity of mFOLFIRINOX was grade 3–4 diarrhea, in 19% of the patients, mainly after the first two cycles of treatment. These results suggest that combination chemotherapy, especially using mFOLFIRINOX regimen should now be the standard of care in fit patients [Eastern Cooperative Oncology Group (ECOG) performance status of 0–1, no contraindication to fluoropyrimidines, and no severe postsurgical diarrhea]. In frail patients not candidates for mFOLFIRINOX (for example, performance status score of 2, prior peripheral neuropathy) but with no contraindications to fluoropyrimidines, the combination of gemcitabine and capecitabine is a treatment option. mFOLFIRINOX is now the preferred adjuvant regimen in fit patients for ESMO,9,92 NCCN, 93 and ASCO. 94
The APACT trial (NCT01964430) has explored nanoparticle albumin-bound nab-paclitaxel and gemcitabine in the adjuvant setting compared with gemcitabine alone. 95 Patients over 18 years with ductal adenocarcinoma (R0 or R1 resection), performance status 0–1, and with no prior therapy, normal postoperative CT scan, and postoperative serum CA 19-9 levels ⩽100 U/ml, were eligible for inclusion; 866 patients were randomized. Primary endpoint, as assessed by an independent reviewer, was disease-free survival. Unfortunately, median DFS was not different between arms, 19.4 months (nab-paclitaxel/gemcitabine) and 18.8 months (gemcitabine); HR, 0.88; 95% CI, 0.729–1.063; p = 0.1824). A modest but significant increase in overall survival was seen at interim analysis in favor of the combination arm (HR, 0.82; 95% CI, 0.68–0.996; p = 0.045). Consistently with the PRODIGE24 trial, the survival in the gemcitabine arm was markedly improved (median 36.2 months), probably due to patient selection, optimal follow up, and benefit from contemporary treatments at relapse.
Optimal follow-up schedule for potentially curable pancreatic cancer has not been defined, and varied significantly between trials. 88 Looking at the more recent trials, APACT and CONKO-005 used visits and CT scans at 3-month intervals, PRODIGE24 and JASPAC 01 planned the same follow-up plus CA19-9, while each site determined its own follow-up in the ESPAC-4 trial.
What is the optimal timing for adjuvant chemotherapy?
A further analysis of the ESPAC-3 study was performed to investigate the optimal timing between surgery and the start of chemotherapy, and the optimal duration of chemotherapy. 96 No difference in survival was seen between patients commencing chemotherapy within 8 weeks of surgery and those commencing chemotherapy later than 8 weeks after surgery. Patients who completed all six planned cycles of treatment had better survival than those who received between one and five cycles only (HR, 0.516; 95% CI, 0.443–0.601; p < 0.001). Completion of therapy was also an independent factor associated with survival. Thus, an important conclusion of this study is that it is possible to delay the start of adjuvant chemotherapy until full recovery from surgery, and that it is necessary to complete the six cycles of adjuvant chemotherapy. In another retrospective series, including 488 patients from five institutions, delayed initiation of adjuvant chemotherapy >12 weeks after surgery is associated with the same survival benefit than the timely initiation group as compared with no adjuvant chemotherapy. 97
Data from the SEER-Medicare database suggested the benefit of adjuvant chemotherapy in elderly people (66 years of age and above). 98 Among 4105 patients who underwent a pancreatectomy, early adjuvant therapy (commencing within 12 weeks after surgery) significantly reduced 6-month and 1-year mortality, compared with patients who underwent surgery alone (odds ratio = 0.71; p = 0.000). Late initiation of adjuvant therapy was also associated with better outcomes (odds ratio = 0.51; p = 0.000) compared with surgery alone.
Significant delays in initiating adjuvant therapy are not uncommon, and at least 20% of patients are unable to recover sufficiently following surgery to receive any adjuvant therapy. Moreover, population data suggest that many patients do not receive chemotherapy: In a nationwide population-based analysis, 46% of the patients between 2008 and 2013 did not received adjuvant chemotherapy after complete resection, with large differences between centers (26–74%). Patients with stage II–III, age <60 years, and those treated after 2011 were more likely to receive adjuvant chemotherapy. 99 In the Medicare beneficiaries in the US, adjuvant treatment was delivered to 51% in patients aged 64 years or older, with some increase over time, from 50.5% (1991–1996) to 56.1% (2003–2005). 100 In another cohort of patients over 66 years, adjuvant therapy was applied in 51.7% of patients, and was associated with a significant increase in survival. 98 Chemotherapy omission is linked to severe operative morbidity in the American College of Surgeons experience. 101
Neoadjuvant treatment for resectable pancreatic cancer
The standard treatment for patients with resectable pancreatic cancer is surgical resection followed by adjuvant chemotherapy.16,17,102 Theoretical advantages of neoadjuvant versus adjuvant therapy are testing of chemosensitivity, control of tumor disease (treatment of circulating tumor cells and micrometastases prior to surgery), higher rate of completion of systemic therapy, higher R0 resection rate (downsizing), reduced pancreatic leakage, and better selection of patients (avoidance of surgery in case of disease progression under neoadjuvant therapy). In contrast, a toxic neoadjuvant regimen may be deleterious as it may limit the possibility of surgical resection. The neoadjuvant approach has become the standard of care for most gastrointestinal cancers. Contrary to general concerns, neoadjuvant therapy has been shown previously to be better tolerated than adjuvant therapy, and the rate of access to a complete therapeutic sequence is greater if oncological treatment is started preoperatively. The introduction of neoadjuvant treatment for resectable pancreatic cancer more than 20 years ago seemed an interesting alternative, 103 but data from comparative randomized controlled trials are still lacking, partly because of difficulties in recruiting patients. The main ongoing studies that are attempting to provide evidence for this approach are listed in Tables 2 and 3.
Results of randomized trials of neoadjuvant treatments for resectable and borderline pancreatic cancer.

p values: * < 0.001; † = 0.023; ‡ = 0.01; § = 0.028B
RPC, borderline resectable pancreatic cancer; DFS, disease-free survival; OS, overall survival; PEXG, cisplatin, epirubicin, gemcitabine, and capecitabine.
Main ongoing randomized phase III trials of neoadjuvant treatments for pancreatic cancer.

FOLFIRINOX, Oxaliplatin, irinotecan, folinic acid and fluorouracil; FOLFOX, Oxaliplatin, folinic acid and fluorouracil.
Impact of postoperative complications on systemic therapy
The main pitfalls related to the surgical management of pancreatic cancer are the risks of early recurrence, performance status deterioration, and postoperative complications that could prevent the completion of adjuvant therapy. Approximately 50% of patients could not receive adjuvant treatment following pancreatic cancer surgery. 47 In a mono-institutional retrospective study, Tzeng and colleagues found that, in the setting of neoadjuvant therapy, 83% of patients received the complete oncological sequence compared with 58% in the surgery first group. 14 In the surgery first group, the reasons for failure of the complete sequence were: early progression of the disease (n = 13, 26%), (major complications (n = 5, 10%), and deterioration of performance status (n = 3, 6%). The median overall survival of patients who received the complete oncological treatment sequence was significantly longer than those with incomplete treatment (36.0 versus 11.0 months, p < 0.001).
Impact of neoadjuvant therapy on postoperative course after pancreatic excision surgery
Neoadjuvant treatment is generally well tolerated, with no impact on the postoperative course. In noncomparative phase II trials assessing neoadjuvant chemotherapy, no patient was excluded from the surgical project because of toxicity of neoadjuvant therapy.109,110
A recent systematic review evaluated the rates of complications after neoadjuvant chemotherapy or chemoradiotherapy and PD for pancreatic cancer. 111 Neoadjuvant therapy was associated with comparable fistula (3–11%) and infection rates (3–7%) and equivalent mortality (0–4%) compared with surgery first. Other studies showed specific complication rates (pancreatic fistula, haemorrhage) outside gastroparesis significantly reduced after neoadjuvant chemoradiotherapy or FOLFIRINOX.112,113 The most plausible explanation for these findings is that neoadjuvant therapy, in particular chemoradiotherapy, may induce pancreatic fibrosis, which would result in a lower incidence of pancreatic fistula, and, thus, reduce the risk of associated complications.
Downsizing and downstaging effect of neoadjuvant therapy
A recent meta-analysis assessed the impact of neoadjuvant therapy on pathological response. 114 This study confirms the tumor downsizing and downstaging effects of neoadjuvant therapy, with lower T and N stages, lower rates of perineural and lymphovascular infiltration, and higher R0 resection rates. The rate of tumors classified as T3/T4 was 75% and 88% in the neoadjuvant and surgery first groups, respectively, with a relative risk of 0.78 (95% CI, 0.69–0.89; p = 0.0002). N0 status was significantly more frequent following neoadjuvant therapy (58% versus 35%; relative risk, 2.14; 95% CI, 1.85–2.46; p < 0.00001). In the neoadjuvant therapy group, 83% of patients were classified as R0 versus 73% after surgery first (relative risk, 1.13; 95% CI, 1.08–1.18; p < 0.0001).
On the basis of these data, but also with regard to the impact of the aforementioned histoprognostic factors (tumor size, lymph node status and resection margin status) on the risk of recurrence and survival, indications of neoadjuvant therapy are regularly discussed.32,33,115–117 In addition, with regard to the recent ASCO guidelines, surgery first should be proposed only in the following situations88,118:
(1) No clinical evidence of metastatic disease;
(2) A performance status and comorbidity profile appropriate for a major abdominal operation;
(3) No radiographic interface between primary tumor and mesenteric vasculature on high-definition cross-sectional imaging;
(4) A CA 19-9 level (in the absence of jaundice) suggestive of localized disease.
Selection of good candidates for neoadjuvant therapy
Risk of tumor progression and testing of the tumor biology
The risk of disease progression during neoadjuvant therapy should be analyzed as part of the optimal selection of good candidates for surgery. Indeed, disease progression during neoadjuvant therapy might be considered equivalent to an early recurrence (within 6 months) after surgical resection. The true rate of resectability, based on surgical exploration after neoadjuvant treatment for resectable pancreatic adenocarcinoma (excluding borderline and locally advanced lesions), is estimated to be between 66% and 88%, in the four available meta-analyses.103,119–121
Should priority go to surgery or to comprehensive pretherapeutic assessment?
The waiting time before surgery is often considered a measure of quality of care. However, even if the waiting time before surgery is due to overloaded operating rooms, it has been shown that this time may allow selection of the best patients for surgery, and preparation of the patients for surgery (for example, prerehabilitation, preoperative nutrition). Two retrospective cohort studies from the US national cancer database122,123 evaluated the impact of waiting time before surgery. Mirkin and colleagues suggested that long-term survival was not affected by the waiting time. 123 In the study published by Swords and colleagues, the delay in access to surgery was short (1–14 days) for 34.4% of patients, average (15–42 days) for 51.6% of patients, and long (43–120 days) for 14.0% of patients. 122 Mortality rates were lower for patients with average (risk ratio 0.94; 95% CI, 0.90–0.97) and long (risk ratio 0.91; 95% CI, 0.86–0.96) waiting times for surgery. There were no differences in lymph node involvement, locoregional, or metastatic unresectability at exploration, or positive margins. The 90-day mortality was lower in the average waiting time group (odds ratio 0.75; 95% CI, 0.65–0.85) and in the long waiting time group (odds ratio 0.72; 95% CI, 0.60–0.88).
Survival after neoadjuvant therapy
Owing to the lack of fully published randomized trials, current evidence of an effect of neoadjuvant therapy on long-term outcomes comes mainly from phase II trials and retrospective analyses. According to the systematic review by Gillen and colleagues, 103 performed before the advent of efficient combination chemotherapy regimens, the overall survival of patients receiving neoadjuvant treatment was slightly better than the survival of those having surgery first. According to this meta-analysis, the median overall survival of patients after surgery alone and after surgery first followed by adjuvant treatment was 16.9–20.2 months and 20.1–23.6 months, respectively, whereas, following neoadjuvant therapy, the median intention-to-treat survival was 23.3 months.
Neoadjuvant chemotherapy for resectable pancreatic adenocarcinoma [specifically excluding borderline resectable pancreatic cancer (BRPC)] has been reported in only two phase II studies.109,110 These phase II trials showed a median overall survival of 26.5 months and 27.2 months after 2 months of neoadjuvant chemotherapy with or without adjuvant therapy. Again, it is important to note that the intention-to-treat approach was used to analyze these results. Indeed, all patients, regardless of surgical complications, were included in these trials, in contrast to randomized trials on adjuvant chemotherapy, in which only 40–50% of patients are included. 47
Recent large cohort studies also suggest a survival benefit for patients who receive neoadjuvant treatment for resectable pancreatic cancer.11,124 In two separate analyses of the US National Cancer Database, perioperative chemotherapy was associated with survival benefit in patients with early stage pancreatic cancer compared with surgery first. In a study by Lutfi and colleagues, 11 completion of postoperative chemotherapy complementary to preoperative chemotherapy had a significant overall survival advantage over adjuvant chemotherapy alone (HR 0.75; 95% CI, 0.65–0.85). Achieving neoadjuvant chemotherapy alone showed a marginal overall survival benefit compared with adjuvant chemotherapy (HR 0.89; 95% CI, 0.81–0.98). In a study by Mokdad and colleagues, 124 median overall survival was significantly longer in the neoadjuvant group than in the surgery first group (26 versus 23 months; p = 0.01). Using multivariate analysis, the authors demonstrated a significant survival benefit for patients in the neoadjuvant group compared with the surgery first group following adjuvant chemotherapy (HR 0.83; 95% CI, 0.73–0.89). The main biases of these cohort studies result from the absence of intention-to-treat analysis, and the lack of standardization of criteria for resectability and indications of treatment (for example, chemotherapy versus chemoradiotherapy, duration, doses) depending on the stage.
The Milan group reported a randomized three-arm phase II trial, in which patients were randomly assigned to receive surgery followed by adjuvant gemcitabine, surgery followed by six cycles of adjuvant PEXG (cisplatin, epirubicin, gemcitabine, and capecitabine), or three cycles of neoadjuvant PEXG and three further cycles postoperatively (perioperative group). 106 A total of 93 patients were included but five patients from the same institution were excluded because of noncompliance with the protocol. Progressive disease was seen in 1 out of 26 patients during neoadjuvant treatment. No toxic death was observed in any arm. Evidence of the efficacy of neoadjuvant chemotherapy was reported with increase in R0 surgery, median DFS and median overall survival. Intention-to-treat estimates of 5-year overall survival were 13% in the surgery plus gemcitabine group, 24% in the surgery plus adjuvant PEXG group, and 49% in the perioperative PEXG strategy. Despite these promising results, this trial will not continue to phase III, due to different new active regimens available for the metastatic setting.
Randomized phase III studies comparing neoadjuvant treatment with upfront surgery are warranted. These studies are difficult to design and to conduct. Pretherapeutic pathological proof is mandatory, and biliary stenting is often necessary before neoadjuvant treatment. The calculation of the number of patients should take into account the risks of dropout during neoadjuvant treatment, complications related to drainage or chemo(radio)therapy, early progressive disease, risk of surgery refusal, and the risk of unexpected metastases or tumor nonresectability during surgical exploration. For these reasons, the survival results of neoadjuvant trials cannot be compared with adjuvant trial results that include selected populations with no metastases and adequate recovery after surgery. This may explain why the median survivals were disappointing in both arms (17.1 months after preoperative chemoradiotherapy compared with 13.7 months with upfront surgery) in the phase III PREOPANC trial shown in Table 2. 104 However, this first randomized clinical trial demonstrates that preoperative treatment improves outcomes for patients with borderline or resectable pancreatic cancer and is described in the BRPC section.
Discussions of future projects will be based on the use of intensified chemotherapy regimens (with or without stereotactic radiotherapy), which seem promising.
Management of BRPC
There are no universally accepted criteria for defining BRPC. However, the anatomic definitions of BRPC according to European and American guidelines are similar and cover the same standard radiological criteria: arterial contact of <180° (celiac trunk, SMA, common hepatic artery), and venous contact of ⩾180° without vein contour irregularity (superior mesenteric vein or portal vein) or <180° amenable to vein reconstruction.9,18 The MD Anderson classification of BRPC identifies a patient’s subgroup (type C) with a marginal performance status or a severe pre-existing comorbidity profile (including advanced age) that puts them at high risk for a major surgical procedure. 125
The management of BRPC has been subject to debate, mainly as to whether neoadjuvant treatment is required. Although many concepts support the neoadjuvant approach (including the selection of patients with ‘good’ tumor biology), there is lack of evidence for its efficacy. A meta-analysis published recently by the Dutch Pancreatic Cancer group 126 compared upfront surgery with neoadjuvant treatment in resectable pancreatic cancer and in BRPC. The authors analyzed 38 studies involving 3884 patients. In the BRPC subgroup, upfront surgery assessed in 4 retrospective studies (n = 1051 patients) was compared with neoadjuvant strategies assessed in 21 studies (n = 976 patients). Median overall survival was 12.8 months in the upfront surgery group versus 19.2 months in the neoadjuvant group. With regard to the type of neoadjuvant therapy, various drugs and designs were used for chemotherapy and chemoradiotherapy, and this heterogeneity made the analysis of subgroups impossible. A patient-level meta-analysis on neoadjuvant FOLFIRINOX in patients with BRPC was recently performed and included 24 studies (8 prospective, 16 retrospective), comprising 313 BRPC patients treated with FOLFIRINOX. 127 The resection rate was 67.8% and the R0-resection rate was 83.9% (95% CI: 76.8–89.1). Patient-level median OS was 22.2 months, with a median progression-free survival of 18.0 months. The authors concluded that BRPC patients treated with neoadjuvant FOLFIRINOX had favorable outcomes, and these results need to be assessed in a randomized trial.
In 2018, two prospective randomized clinical trials specifically assessed the value of neoadjuvant treatment in BRPC (summarized in Table 2).104,105 In a Korean trial, the authors addressed the role of chemoradiotherapy in the preoperative versus postoperative setting. 105 Chemoradiotherapy consisted of 54 Gy in 30 fractions with weekly gemcitabine, then adjuvant gemcitabine for 4-monthly cycles. The primary outcome was the 2-year overall survival rate. The trial closed early after the first interim analysis, and only 58 patients were enrolled; 8 patients were excluded from the analysis because they withdrew consent. Authors showed that the preoperative strategy had a significant advantage: the neoadjuvant group showed a higher resection rate (51.8% versus 26.1%) and higher 2-year survival (40.7% versus 26.1%; HR, 1.495; 95% CI, 0.66–3.36; p = 0.028). Few patients who underwent tumor resection completed maintenance chemotherapy: eight in the neoadjuvant group and six in the upfront surgery group. The recurrence rate was high: 88.2% in the neoadjuvant treatment group and 88.9% in the upfront surgery group. Median overall survival was 21 months versus 12 months for neoadjuvant chemoradiotherapy versus adjuvant chemoradiotherapy, respectively.
Preliminary results of the PREOPANC-1 trial were communicated in 2018. 104 A total of 248 patients with resectable pancreatic cancer (51%) or BRPC (49%) were randomly assigned to preoperative gemcitabine-based chemoradiotherapy or immediate surgery. In an intent-to-treat analysis, the resection rate was slightly lower with neoadjuvant chemoradiotherapy than with upfront surgery (60% versus 72%; p = 0.065) but the R0 resection rate was significantly increased (61% versus 31%; p < 0.001). Moreover, the median time until recurrence was significantly longer after preoperative treatment (9.9 versus 7.9 months; p = 0.023). Analysis was performed after the occurrence of 149 out of the 176 required events for the primary outcome: overall survival. The median overall survival was 17.1 months after preoperative chemoradiotherapy compared with 13.7 months after upfront surgery followed by adjuvant chemotherapy, but the difference was not statistically significant (p = 0.074). Longer follow up and final survival results are needed before any definitive conclusion, although Dutch guidelines have already endorsed the preoperative chemoradiotherapy strategy. The FOLFIRINOX regimen has been evaluated as an neoadjuvant therapy in BRPC in small and mainly retrospective studies, and reviewed in a very recent meta-analysis. 128 Based on data from 288 patients in an intention-to-treat analysis, authors calculated a median overall survival of 22.2 months (95% CI, 18.9–25.6 months), comparable with results obtained for patients with resectable pancreatic cancer operated upfront. The main ongoing randomized studies are presented in Table 4. These trials will hopefully answer two important questions: is induction therapy improving overall survival in patients with BRPC? And should we use chemotherapy or chemoradiotherapy to achieve this goal?
Main ongoing randomized trials of induction treatments for borderline pancreatic cancer.
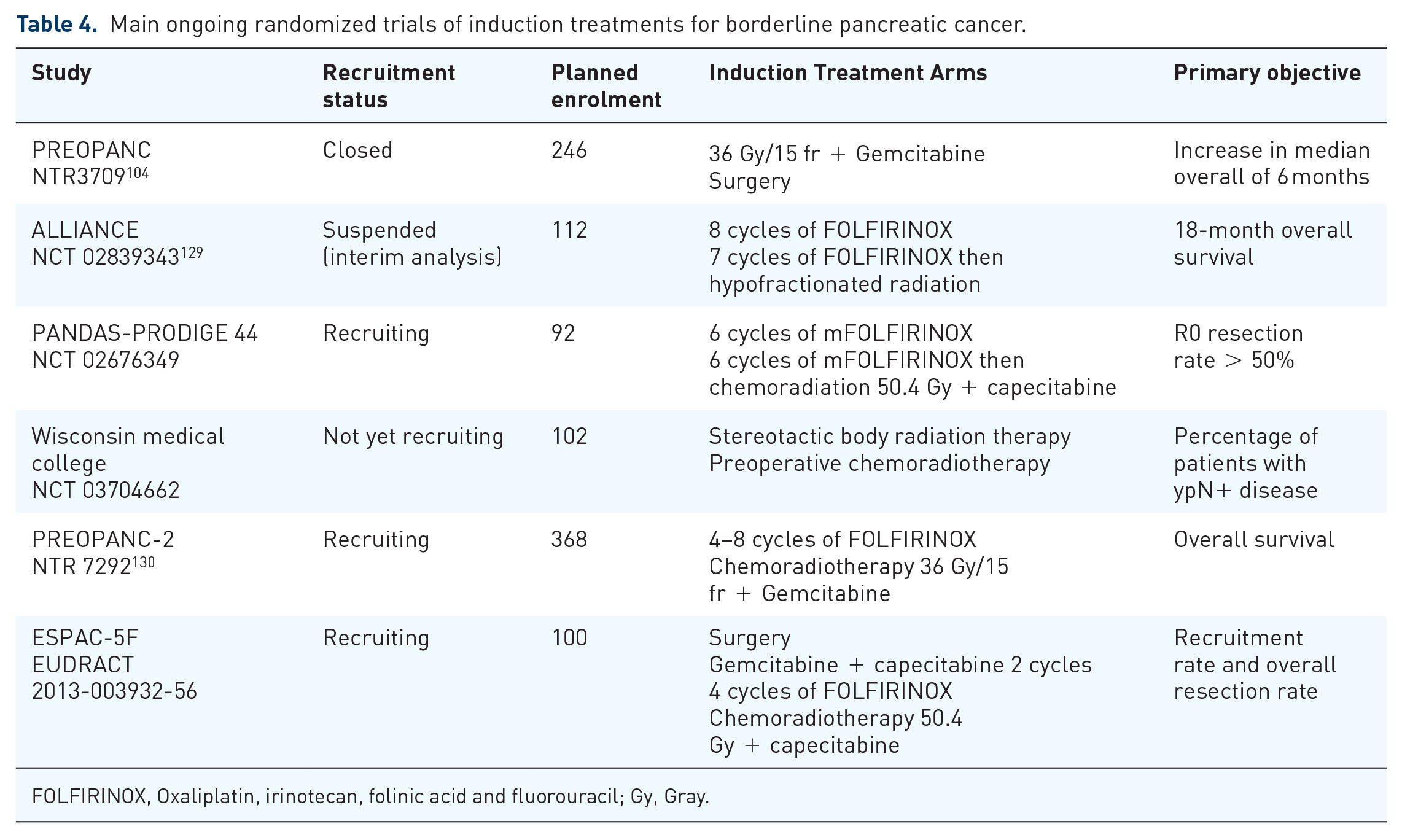
FOLFIRINOX, Oxaliplatin, irinotecan, folinic acid and fluorouracil; Gy, Gray.
Locally advanced pancreatic cancer
What is the standard of care?
Patients with LAPC represent approximately 20–30% of all patients with pancreatic cancer at diagnosis. Median overall survival ranges from 10 to 30 months, depending on the reported series (these differ widely in terms of definitions and treatments). By definition, locally advanced tumors are those that are not metastatic and not potentially resectable owing to ‘irreversible’ vascular invasion. However, this definition varies and is also evolving over time and with therapeutic strategies.131,132 Practically, unresectable tumors are those that encase the aorta, obliterate the portal vein or the superior mesenteric vein (confluence), or involve more than 180° of the SMA or celiac trunk, precluding achievement of negative margins at surgical resection. 133 Owing to the difficulty of relying on strict criteria for unresectability, it should now be recommended that all cases with nonmetastatic tumors are discussed by a multidisciplinary board in high-volume centers, and that these evaluations are repeated after treatment induction to confirm definitive unresectability.
Standard management is based on chemotherapy administration as historically generated by the results obtained in randomized trials performed in metastatic disease. Today, the reference treatment remains gemcitabine (grade A recommendation) while active regimens in metastatic pancreatic cancer can be considered good options in patients with performance status scores of 0–1 (FOLFIRINOX, grade B) or 0–2 (nab-paclitaxel–gemcitabine, expert recommendation). 133 There is not yet prospective validation of superior efficacy of these regimens over gemcitabine alone, and the recent reports are mainly observational studies, small phase II or pooled analyses of mixed approaches combining induction chemotherapy with FOLFIRINOX or nab-paclitaxel–gemcitabine with additional chemoradiation in nearly half of the patients. In this setting, a recent pooled analysis of 355 patients from 13 studies reported a median survival of 24.2 months and a median progression-free survival of 15 months with FOLFIRINOX induction therapy that favourably compares to gemcitabine alone (median overall survival of 6–13 months). 134 Similar data were also reported for the nab-paclitaxel–gemcitabine combination, with a median overall survival of 18 months (and not yet reached for resected patients). 135 From these reports, it is important to note that 26% of these patients had secondary resection (conversion surgery). However, it is to be acknowledged that nearly half of the patients had received complementary chemoradiation, the relative contribution of each modality being therefore highly difficult to distinguish, and even more so in populations that mixed BRPC and LAPC.
Adjunction of radiation therapy in the setting of LAPC has not proven to be of benefit, either upfront or after gemcitabine induction for 4 months; after conflicting data derived from small trials, the LAP07 phase III trial clearly showed no benefit of adding chemoradiation (grade A recommendation).133,136 Chemoradiation was only shown to improve local control in a subgroup of patients and, consequently, can be proposed as an individual option in selected patients using capecitabine as a radiosensitizer partner (it is suggested to be a better radiosensitizer partner than gemcitabine according to a randomized phase II study). 137 Recently, a meta-analysis of data from 593 pooled patients confirmed that chemoradiation is not superior to chemotherapy alone, with similar overall survival and higher rates of grade 3–4 adverse events. 138 Conversion surgery should be discussed and proposed in all operable cases with good response or local tumor control after induction chemotherapy with or without chemoradiation.
Perspectives and challenges to improve the management of locally advanced pancreatic cancer
New approaches
Practically, LAPC should deserve specific trials in fit patients to evaluate new treatment options, sequences, and strategies based on new drugs and new loco-regional ablative therapies such as stereotactic body radiotherapy (SBRT), proton beam radiation therapy, irreversible electroporation, endoscopic ultrasonography-guided radiofrequency ablation, or intratumoral delivery of innovative agents such as radioactive 32 P phosphorus. Multidisciplinary tumor boards make sense for these complex situations and should encourage case-by-case discussions with several represented specialties (i.e. surgeon, radiation oncologist, medical oncologist, pathologist, and radiologist).
Several randomized phase II and III trials are ongoing to evaluate the impact of FOLFIRINOX versus gemcitabine alone (NEOPAN; NCT02539537) and nab-paclitaxel–gemcitabine as an induction therapy followed by intensified radiation therapy versus continuous chemotherapy, using DPC4 gene activation as a stratification factor (RTOG 1201; NCT01921751). These studies will provide important information about the best backbone regimen that can be used to add new agents, such as antistromal, immunotherapeutic, or antimetabolic agents.
Beyond the LAP 07 study, there is now room to investigate more active chemotherapy regimens as induction therapies followed by new radiation therapy techniques, such as intensity-modulated radiation therapy or SBRT. In addition to the classical therapeutic tools, emerging local ablative or intratumoral delivery therapies should be also evaluated prospectively.
Finally, the setting of LAPC deserves new strategies to treat these patients by assessing maintenance therapy or therapy-free period in well-controlled tumors; trials combining immunotherapy with chemotherapy, with monitoring by functional imaging and liquid biopsies, are underway.
Role of conversion surgery
The possible role for surgery has been extended recently to LAPC. Induction combination chemotherapy, often followed by chemoradiation, may lead to reconsideration of surgery in patients with initially unresectable disease and responding disease. This prompted colleagues from the Medical College of Wisconsin to propose a new classification for LAPC. This classification may help multidisciplinary boards to define the optimal strategy and the goal of care, potentially curative or palliative intent 131 :
(1) Type A are tumors that may be considered for conversion resection after induction therapy.
(2) Type B are definitively unresectable tumors. Type B tumors are defined as LAPC with >270° SMA encasement, celiac artery with >180° encasement, abutment or encasement of the aorta, and >180° encasement of the hepatic artery with extension beyond bifurcation of the proper hepatic artery into right and left hepatic arteries.
All other patients fit for surgery and chemotherapy may receive induction chemotherapy. In LAPC patient cohorts receiving gemcitabine-based chemotherapy plus chemoradiation, conversion surgery has been infrequent (1–8%).136,139,140 Median survival after resection has not been reported. In a large retrospective study of patients scheduled for resection after restaging, 322 patients received induction chemoradiation with gemcitabine, and 46% of patients had conversion surgery, of which 31.3% were R0 resections. 141
The role of more intensive chemotherapy regimens has been explored. Unfortunately, only one phase II randomized study from the Milan group is available, and included only 54 patients with BRPC or LAPC. Induction regimens were nab-paclitaxel plus gemcitabine with or without capecitabine and cisplatin (PAXG). The response rates and conversion surgery rates are comparable, with a higher rate of R0 resection (67.5% versus 44%) under the PAXG regimen. 142
Numerous studies have used induction FOLFIRINOX followed, or not, by chemoradiation, and reported promising results. In a recent meta-analysis including data from 365 patients, the response rate after induction FOLFIRINOX was 29%, with a conversion surgery rate of 28%. The R0 resection rate was high, at 77%. 143 In other, smaller, cohorts, median survival for all patients was between 22 months and 35.4 months.144–146 In two large retrospective studies of patients scheduled for resection post restaging after FOLFIRINOX, the conversion surgery rates were 60.8% and 78.0%, with R0 resection rates from 40.8% to 80.6%.141,147 The University Hospital of Colorado retrospectively analyzed data from 120 patients with BRPC or LAPC receiving induction chemotherapy with either gemcitabine and nab-paclitaxel or FOLFIRINOX. The tumor progression rate was significantly lower with FOLFIRINOX (13.3% versus 40.5%; p = 0.001). The R0 resection rate was higher with FOLFIRINOX (66.3% versus 32.4%; p = 0.002). The perioperative complication rate was also lower (52.7% versus 83.3%; p = 0.051), and progression-free survival was significantly increased with FOLFIRINOX (15.3 versus 8.2 months; p = 0.003). No significant increase in median overall survival was observed. 148
A recent United States National Cancer Database (NCDB) analysis of 8689 patients with LAPC showed that the best chance for survival of LAPC was the ability to undergo pancreatectomy, compared with either no surgery or a more local procedure (HR, 0.39; 95% CI, 0.34–0.46; p < 0.001). 149 Patients with LAPC who underwent pancreatectomy had significantly improved survival compared with those who did not (22 versus 10.6 months). Multi-agent induction chemotherapy followed by chemoradiotherapy improved the resection rate (9.8%) compared with concurrent chemoradiotherapy (5%) or multi-agent chemotherapy alone (3.3%).
In retrospective studies, SBRT has been suggested to be beneficial. In a retrospective study carried out by the Johns Hopkins University, the addition of SBRT to induction FOLFIRINOX has been shown to correlate with increased probability of conversion surgery. 150
Specific recommendations for surgical management following induction therapy
After induction therapy for LAPC type A, surgical exploration should be attempted in patients with stable disease or remission to rule out or confirm true vascular infiltration. Induction therapy significantly decreases the accuracy of CT scan in determining operability, T-staging, and R0 resectability of pancreatic head carcinoma.151,152 Overestimation of tumor size and vascular invasion significantly reduces CT scan specificity after preoperative treatment.
In the setting of LAPC, with superior mesenteric artery or celiac trunk involvement, a surgical exploration with dissection and biopsy of the peri-adventitial tissues (arterial sheaths) is recommended. In case of positive extemporaneous examination, a PD with arterial resection may be attempted with high immediate risk153,154 and must be weighed against a palliative procedure without resection. Hackert and colleagues recommended biopsy of arterial sheaths, and in case of positivity, nonresection, and palliative treatment. 155 In case of absent viable tumor, the described technique allows to perform radical surgery without arterial resection in this subgroup of patients. 155
Current guidelines recommend that resected patients who received preoperative therapy be considered for additional postoperative chemotherapy. 118 Carefully selected patients with LAPC (20–30%) who had responded to induction therapy can benefit from conversion surgery.
Update in therapy for advanced pancreatic cancer
Which strategy for first-line chemotherapy?
There are few validated regimens for the treatment of advanced pancreatic cancer in first-line treatment. There has been little novelty regarding the first-line treatment in this setting and several chemotherapy regimens, alone or in combination, have shown an improvement in progression-free survival, most often without overall survival improvement, 156 so we summarized below main trials and current recommendations.
Until the approval of gemcitabine in 1997, fluorouracil was the gold standard chemotherapy agent in advanced pancreatic cancer. 157 Gemcitabine significantly increased the ‘clinical benefit response’, median progression-free survival and overall survival (from 4.4 months to 5.7 months; p = 0.0025) with an acceptable tolerance compared with bolus fluorouracil in a randomized phase II study. 157 Table 5 shows the main randomized trials for first-line regimens in advanced pancreatic cancer.
Main randomized trials performed in first-line therapy for advanced pancreatic cancer.

FOLFIRINOX, Oxaliplatin, irinotecan, folinic acid and fluorouracil; HR, hazard ratio; N/A, Not available; OS, overall survival; QoL, quality of life.
More than 20 randomized trials addressed the comparison of gemcitabine to gemcitabine with addition of a second cytotoxic agent or targeted therapy. All failed to show any survival improvement, 156 except erlotinib, which provided a statistically significant, albeit modest median overall survival benefit of 6.24 months versus 5.91 months (p = 0.038) and a 1-year survival of 23% versus 17% (p = 0.023) in a NCIC phase III trial that included 569 patients with both metastatic and locally advanced pancreatic cancer (LAPC). 158 This improvement in median overall survival of 10 days, although significant, is not relevant in clinical practice. There were no significant differences between the gemcitabine and gemcitabine–erlotinib arms in response rate or quality of life, with worse diarrhea change scores in the erlotinib plus gemcitabine arm (p = 0.001). Toxic effects were significantly increased in this combination arm; mainly rash, diarrhea, and stomatitis. Furthermore, there were six protocol-related deaths and seven patients with interstitial pneumonitis in the combination arm. Survival benefit was not confirmed by the later LAP07 trial; this trial included 449 patients with LAPC for whom no benefit from use of erlotinib was found. 136
In 2005, Reni and colleagues first tested an aggressive polychemotherapy regimen with cisplatin, epirubicin, fluorouracil, and gemcitabine (PEFG) versus gemcitabine alone. A total of 99 patients were included, and the response rate was 38.5% in the PEFG group versus 8.5% with gemcitabine. The primary endpoint (4-month progression-free survival) was significantly increased in the PEFG arm (60% versus 28%; HR, 0.46, p = 0.001), but there was no significant difference in overall survival. 162
The pivotal PRODIGE 4-ACCORD11 trial compared FOLFIRINOX, a combination of oxaliplatin, irinotecan, folinic acid, and fluorouracil to gemcitabine in patients below 75 years of age with metastatic pancreatic cancer. 159 Overall survival was significantly increased, with median survival of 11.1 months for FOLFIRINOX and 6.8 months for the gemcitabine regimen (HR 0.57; 95% CI, 0.45–0.73; p < 0.001). 159 Moreover, FOLFIRINOX significantly delayed quality of life deterioration compared with gemcitabine. 163 These results were confirmed by another, still unpublished, phase III study, in which the median overall survival was 10.8 months in the FOLFIRINOX group and 7.4 months in the gemcitabine group (HR, 0.48; 95% CI, 0.41–0.68; p < 0.001). 160 Since then, FOLFIRINOX has become the standard regimen for fit patients with metastatic disease, ECOG performance status score of 0 or 1, no significant cardiac comorbidity, and no increase in bilirubin level.
With the MPACT trial in 2013, Von Hoff and colleagues reported that a combination of gemcitabine with nab-paclitaxel was superior to gemcitabine alone as a first-line regimen for the treatment of patients with metastatic pancreatic cancer. 161 This study involved 861 patients with an ECOG performance status score of 0–2. The median overall survival was 8.5 months in the nab-paclitaxel arm and 6.7 months in the gemcitabine arm (HR 0.72; 95% CI, 0.62–0.83; p < 0.001).
To date, no prospective trial has compared directly FOLFIRINOX to nab-paclitaxel plus gemcitabine. Retrospective studies comparing both regimens suggest greater activity of FOLFIRINOX, but caution should be taken outside randomized studies. A phase II trial is currently underway in the Japanese population to compare the 1-year overall survival rate of both regimens (UMIN Clinical Trials Registry: UMIN000023143). To the best of the authors’ knowledge, no other trial is running or even scheduled. Recently, Kim and colleagues compared FOLFIRINOX and nab-paclitaxel–gemcitabine in a real-world retrospective review that showed similar trends for both regimens in terms of overall survival. 164
In routine practice, the FOLFIRINOX regimen is recommended as standard for metastatic pancreatic cancer by the NCCN, the American Society of Clinical Oncology (ASCO), and the European Society for Medical Oncology (ESMO) for patients with an ECOG performance status score of 0 or 1 and a favorable comorbidity profile.9,18,88,165,166
This regimen should be considered with caution for fragile or elderly people. Between 2008 and 2015, Baldini and colleagues enrolled 42 patients retrospectively with a median age of 73 (range 70–79), an ECOG performance status score of 0 or 1 for the large majority (93%), and few comorbidities (median Charlson index = 10). 167 This study found that patients with metastatic disease (n = 37 out of 42; 88%) benefited from a dose reduction of FOLFIRINOX from the first cycle (57%), and reported similar trends as the pivotal PRODIGE 4-ACCORD11 trial in terms of overall survival (12.6 months). Moreover, dose reduction did not appear to have an effect on overall survival (median, 11.7 versus 16.6 months, p = 0.69). Yet, toxicity was easier to manage. It was recently suggested by a retrospective analysis conducted by Kang and colleagues that modified FOLFIRINOX (mFOLFIRINOX) has comparable efficacy to FOLFIRINOX, and better tolerance than standard FOLFIRINOX. 168 mFOLFIRINOX typically consists of a fluorouracil bolus suppression or a dose reduction of irinotecan (or both). To date, no well-conducted trial has formally demonstrated the equivalence of FOLFIRINOX and mFOLFIRINOX in metastatic pancreatic cancer. A proposed algorithm for choosing first-line therapy is shown in Figure 1.

Proposed algorithm for choice of first- and second-line chemotherapy in metastatic pancreatic cancer.
Facing these alternatives, prognostic factors are to be considered to help decision making between treatments. The ECOG performance status score, or Karnofsky index, are historically the strongest predictors of survival, but an analysis of the phase III MPACT study showed that liver metastases, age, and number of metastatic sites were also good prognostic factors for survival, and should be considered for treatment decisions. 169 Sarcopenia at diagnosis and depletion of skeletal muscle during chemotherapy are also prognostic factors for survival, 170 as is nutritional index, 171 and might also be considered. High carcinoembryonic antigen serum level, synchronous metastatic disease (stage IV disease), sarcopenia, neutrophilia, and high lactate dehydrogenase serum level have been confirmed as independent prognostic factors for overall survival in a retrospective chart review. 172
Undoubtedly, performance status is the primary factor when it comes to choose a FOLFIRINOX regimen. However, Sehdev and colleagues showed a promising way to help decision making, in a single-institution, retrospective study concluding that the presence of DNA damage response (DDR) gene mutations are associated with improved overall survival in patients with pancreatic cancer treated with FOLFIRINOX. 173 BRCA tumor suppressor gene mutations are also correlated with better survival under exposure to platinum chemotherapy. 174
What options for second-line chemotherapy?
After progression under first-line chemotherapy, approximately 40–50% of patients with advanced pancreatic cancer are able to receive second-line chemotherapy or subsequent lines. 175 In a retrospective series of patients with metastatic pancreatic cancer, 45% and 21% of patients received two or more lines of treatment after failure of gemcitabine, respectively. 176 In a systematic review of 24 first-line studies (52 treatment arms) conducted between 1998 and 2012, the pooled mean rate of second-line therapy (noted in 17% of all studies) was 43% (range, 16–68%). 177 This rate increased significantly from 35% for studies published before 2007 and 48% for those published after 2007. Of note, all of these studies were conducted in the pre-FOLFIRINOX and nab-paclitaxel–gemcitabine era, and thus mostly included patients who received a gemcitabine-based first-line regimen. In the combination chemotherapy arms of PRODIGE 4-ACCORD 11 159 and of MPACT 161 trials, 47% and 38% of patients received subsequent anticancer therapy, respectively.
The higher efficacy of upfront combination regimens is likely to result in improved patient outcomes, increasing the proportion of patients fit for second-line therapy. According to guidelines recommending the avoidance of cancer-directed therapies for patients with solid tumors and altered general condition, 178 most clinical trials included patients with ECOG performance status scores of 0 or 1. In the real-world setting, the majority of patients are ineligible for such clinical trials and have a poor prognosis (median overall survival with best supportive care alone of approximately 2 months, compared with 5–6 months in treated patients). 179
There is no definite standard of care after disease progression under upfront chemotherapy. In a systematic review of second-line therapy, combination therapies resulted in improved progression-free survival (2.5 versus 1.9 months; p = 0.018) but not overall survival (5.1 versus 4.3 months; p = 0.169) compared with single-agent therapies. 177 Gemcitabine–platinum and fluoropyrimidine–platinum combination regimens seem to provide similar survival results in meta-analyses of second-line studies.177,180,181
Three randomized phase III trials have explored the role of oxaliplatin-based chemotherapy after failure of first-line, single-agent gemcitabine therapy (Table 6). The German CONKO group conducted a phase III trial in which patients were randomly assigned to a combination of oxaliplatin, folinic acid, and 5-FU (OFF regimen), or to best supportive care alone. 182 This trial was terminated early after only 46 patients were enrolled because of slow accrual. Nevertheless, there was a significant overall survival benefit in the OFF group (4.8 versus 2.3 months; p = 0.008). As expected, there was a higher incidence of grade 1–2 hematological, gastrointestinal, and sensory neurotoxicity in the OFF group, but no significant increase in grade 3–4 toxicity. In the subsequent CONKO-003 trial, the OFF regimen provided a significant overall survival benefit over 5-FU–folinic acid (FF regimen; median, 5.9 versus 3.3 months; HR, 0.66; p = 0.01). 183 By contrast, no benefit in progression-free survival (the primary endpoint), objective response rate, or time to deterioration was seen with the modified FOLFOX6 regimen (mFOLFOX6) compared with 5-FU–folinic acid in the PANCREOX trial 184 ; indeed, patients in the 5-FU–folinic acid arm had longer overall survival (median, 9.9 months versus 6.1 months; p = 0.02). This somewhat surprising result was thought to be caused by an imbalance in use of postprogression therapies (7% versus 23%; p = 0.015), and by an increased toxicity in the mFOLFOX6 arm (grade 3–4 adverse events, 63% versus 11%) with a higher number of patients withdrawing from the study owing to adverse events (20% versus 2%). Of note, because these randomized trials were conducted during a period in which single-agent gemcitabine was the only standard of care in the first-line setting, their results cannot be extrapolated to the vast majority of patients treated with upfront FOLFIRINOX or nab-paclitaxel–gemcitabine (furthermore, both being neurotoxic). In fact, at the present time they may only be relevant to the small subset of patients who are deemed unfit for upfront combination chemotherapy and are treated with single-agent gemcitabine, and who are fit enough for oxaliplatin-based combination chemotherapy in the second-line setting, with the controversial results of the randomized trials summarized above.
Randomized trials in advanced pancreatic cancer after first-line gemcitabine progression.

Time to disease progression.
Combination therapy control.
Monotherapy control.
5-FU, fluorouracil; BSC, best supportive care; CI, confidence interval; CONKO, Charité Onkologie; FA, folinic acid; FOLFIRI, fluorouracil, folinic acid, and irinotecan; FOLFOX, modified FOLFOX (oxaliplatin day 1, LV day 1, FU days 1 and 2, every 2 weeks); HR, hazard ratio; Nal-Iri, nanoliposomal irinotecan; IRIS, irinotecan plus S-1; LV, leucovorin; mFOLFIRI.3, modified FOLFIRI.3 (irinotecan days 1 and 3, FA day 1, and FU days 1 and 2, every 2 weeks); MK-2206, AKT inhibitor; Nal-Iri, nanoliposomal irinotecan; NR, not reported; OFF, oxaliplatin, FA and 5-FU; OFF, oxaliplatin, folinic acid and 5-fluorouracil; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; R, randomized; Selumetinib, MEK inhibitor; SOX, S-1 plus oxaliplatin.
Nanoliposomal irinotecan (MM-398), a novel formulation of irinotecan encapsulated in polyethylene glycolated nanoliposomes, has been developed to improve the therapeutic index of irinotecan by increasing the exposure of tumor tissue to this drug, irinotecan nanoliposomes accumulate in tumor-associated macrophages, and reducing exposure of normal tissues as potential sites of toxicity.195,196 In pancreatic cancer, after a single-arm phase II study in 40 patients with metastatic disease after progression on first-line gemcitabine-containing regimens met its primary endpoint, with 75% of patients surviving at least 3 months, 197 the NAPOLI-1 phase III trial randomly assigned 417 patients with metastatic pancreatic cancer previously treated with gemcitabine-containing regimens to nanoliposomal irinotecan monotherapy (120 mg/m2 every 3 weeks), 5-FU-folinic acid (every 2 weeks) or, after a protocol amendment, nanoliposomal irinotecan (80 mg/m2), 5-FU, and folinic acid (every 2 weeks). 194 Approximately one-third of the patients received two or more previous lines of chemotherapy for metastatic disease. Patients assigned to nanoliposomal irinotecan plus 5-FU and folinic acid had a longer overall survival than patients treated with 5-FU and folinic acid (median, 6.1 months versus 4.2 months; HR, 0.75; p = 0.012). Other efficacy endpoints (progression-free survival, objective response rate, time to treatment failure, and CA19-9 responses) were also significantly superior in patients assigned to the experimental arm compared with those in patients receiving 5-FU and folinic acid. In contrast, there was no overall survival benefit of nanoliposomal irinotecan monotherapy over 5-FU-folinic acid. The most common grade 3–4 toxicities in the nanoliposomal irinotecan plus 5-FU and folinic group were neutropenia (27%), fatigue (14%), diarrhea (13%), and vomiting (11%). 198 Nevertheless, patients’ quality of life was maintained during treatment, and there were no significant differences in quality of life compared with patients treated with 5-FU-folinic acid. 199 These results led to the approval of nanoliposomal irinotecan in combination with 5-FU and folinic acid in this setting. It may be more suitable after first-line nab-paclitaxel-gemcitabine, a regimen associated with substantial neurotoxicity, than would be the neurotoxic oxaliplatin-based regimens (which could then be administered as a third line). 200 Whether nanoliposomal irinotecan may have significant clinical activity in irinotecan-pretreated patients (notably with upfront FOLFIRINOX) deserves further analysis before clinical application.
Data on second-line treatments in patients with metastatic pancreatic cancer progressing on gemcitabine plus nab-paclitaxel or FOLFIRINOX are limited to retrospective studies.201–204 In one of these studies, the progression-free and overall survival medians with gemcitabine and nab-paclitaxel after failure of upfront FOLFIRINOX were 5.1 months and 8.8 months, respectively, with no influence of response to first-line FOLFIRINOX on response to nab-paclitaxel–gemcitabine. 203 In a post hoc analysis of the phase III MPACT trial, approximately 40% of patients received a second-line therapy. 204 Patients (n = 18) who received FOLFIRINOX as second-line therapy after nab-paclitaxel–gemcitabine failure had a median overall survival of 15.7 months.
To date, other cytotoxic agents or targeted agents evaluated in the second-line setting (and beyond) for patients with advanced pancreatic cancer have shown no benefit in randomized studies (for example, glufosfamide, 205 or the Jak1 and Jak2 tyrosine kinase inhibitor ruxolitinib190,191) or were tested only in small, single-arm phase II studies.
One notable exception relates to patients who tested positive for deficient mismatch repair (dMMR) or high microsatellite instability (MSI-H) by immunohistochemistry (IHC), polymerase chain reaction (PCR) or next-generation sequencing (NGS). In a study of 86 patients with 12 different cancer types testing positive for dMMR, and who had received at least one prior therapy and had evidence of progressive disease, there was a complete radiographic response to the PD-1 immune checkpoint inhibitor pembrolizumab in 21% of cases, an objective response rate of 53%, and a disease control rate of 77%. 206 Among the eight patients with pancreatic cancer included in this study, two experienced complete radiographic response, and disease control was obtained in six patients. In 2017, the US Food and Drug Administration approved pembrolizumab for dMMR/MSI-H tumors, regardless of disease site. Thus, although approximately 1% of pancreatic cancers are expected to have tumors with this characteristic, 207 the potential for effective treatment is high. Tumor mutation burden, as measured by NGS, is thought to indicate potential for response to immunotherapy because it may be associated with a greater number of neoantigens. These, in turn, can be recognized by the immune system in response to immune checkpoint blockade. Tumor mutation burden may be predictive of greater and more durable responses to immunotherapy in a variety of solid tumors. 208 Whether a high tumor mutation burden may also be a predictor of response to immunotherapy in metastatic pancreatic cancer is still unknown, thus recommendation of the use of immunotherapy for such tumors is premature. Clear definitions of high tumor mutation burdens and reduced variability among commercially available assays are also necessary for appropriate clinical implementation of this potential biomarker.
Looking at another process of DNA instability, the rate of positive tests for BRCA mutation is approximately 5% in the population with advanced pancreatic cancer, 209 and poly ADP-ribose polymerase (PARP) inhibitors are promising as a targeted therapy, and are, therefore, being studied in patients with advanced pancreatic cancer and a known BRCA mutation.210,211
American and European guidelines suggest that the choice of second-line therapy should depend on performance status, comorbidities, organ function, residual toxicities from first-line therapy, and a support system for aggressive medical therapy (Figure 1)9,165:
(1) In patients with an ECOG score of 0–1 and a favorable comorbidity profile: (a) After first-line treatment with gemcitabine plus nab-paclitaxel, 5-FU plus nanoliposomal irinotecan is the preferred option. 5-FU plus irinotecan or 5-FU plus oxaliplatin can be offered when there is a lack of availability of nanoliposomal irinotecan or when residual toxicity from first-line therapy or comorbidity profile precludes the use of 5-FU plus nanoliposomal irinotecan. The choice between 5-FU plus irinotecan or 5-FU plus oxaliplatin depends on, for example, the existence of limiting neuropathy after upfront nab-paclitaxel. These recommendations (5-FU plus nanoliposomal irinotecan, irinotecan, or oxaliplatin) may also apply to the small subset of patients fit for second-line therapy after first-line gemcitabine monotherapy. (b) After first-line treatment with FOLFIRINOX, gemcitabine plus nab-paclitaxel is preferred (off-label use in the EU); gemcitabine alone should be offered when there is a lack of availability of nab-paclitaxel.
(2) In patients with either an ECOG score of 2 or a comorbidity profile that precludes more aggressive regimens and who wish to pursue cancer-directed therapy, gemcitabine or 5-FU is recommended.
(3) In patients with an ECOG score of >2, best supportive care alone is recommended.
(4) For patients who are considered to be candidates for checkpoint inhibitor therapy (when available), routine testing for dMMR or MSI using IHC, PCR, or NGS is recommended, and pembrolizumab (when available) is recommended as second-line therapy for patients with dMMR or MSI tumors.
(5) No data are available to recommend third-line (or above) therapy with a cytotoxic agent. Inclusion in a clinical trial is encouraged.
Update on personalized medicine
Personalized medicine has improved the prognosis of very aggressive cancers such as lung cancers. It is easy to imagine that personalized medicine could help to solve the major therapeutic problem that is pancreatic cancer. Furthermore, it has long been known that the tyrosine kinase signaling pathways that encompass the RAS–MAPK but also the PI3K–AKT cascades have a major role in the carcinogenesis and proliferation of pancreatic cancer. 212 Unfortunately, attempts to target this pathway (e.g. tipifarnib, lonafarnib) have yielded very disappointing results. 213 The personalized medicine approach still needs to remove some barriers to be effective in routine, as shown by the results of the IMPaCT study where 93 patients were included and only 73 were screened. 214 To date, 22 candidate cases have been identified: 14 KRAS wild type, 5 cases of HER2 amplification, 2 mutations in BRCA2, and one ATM mutation, but no patient has been successfully treated on the IMPaCT study. Main reasons were worsening of their general condition, biological status, or death; the occurrence of an intercurrent pathology; final other cancer diagnosis; refusal to participate after screening; or even start of chemotherapy before molecular results.
However, a small subgroup of patients (~2%) with BRCA1 or BRCA2 mutations could be candidates for treatment with PARP inhibitors such as olaparib or veliparib. 215 The POLO (Pancreas Cancer Olaparib Ongoing) trial evaluated the efficacy of maintenance therapy with olaparib in patients with a germline BRCA mutation and metastatic pancreatic adenocarcinoma that had not progressed during first-line platinum-based chemotherapy. 216 A total of 154 patients were randomized between olaparib and placebo. The median progression-free survival was significantly longer with maintenance olaparib than with placebo (7.4 months versus. 3.8 months; HR 0.53; 95% CI, 0.35–0.82; p = 0.004). Overall survival and health-related quality of life were not significantly different and toxicity was mild.
These modest results could be the consequence of the complexity of the carcinogenesis of pancreatic cancer, involving multiple pathways. New personalized medicine programs will need to take into account recent molecular genomic approaches. A comprehensive integrated genomic analysis of 456 pancreatic cancer samples and their histopathological variants identified 32 recurrently mutated genes that aggregate into 10 pathways: KRAS, TGF-β, WNT, NOTCH, ROBO/SLIT signaling, G1/S transition, SWI/SNF, chromatin modification, DNA repair, and RNA processing. Expression analysis defined four subtypes that correlate with histopathological characteristics: squamous, pancreatic progenitor, immunogenic, and aberrantly differentiated endocrine exocrine. 217 The Cancer Genome Atlas work confirmed the complex molecular landscape of pancreatic cancer and provides a roadmap for precision medicine in pancreatic cancer. 218 For example, COMPASS is the first prospective translational study to establish the feasibility of comprehensive real-time genomic analysis of advanced pancreatic cancer using whole-genome and RNA sequencing with the possibility of clinically meaningful routine use. 219 Early results from COMPASS demonstrate that there are unique advanced pancreatic cancer genomic and transcriptomic subtypes with molecular heterogeneity between individual cases, and with differing responses to chemotherapy. This is the first prospective evidence that molecular profiling that defines classical versus basal-like subtypes may predict differential responses to chemotherapy among patients with advanced pancreatic cancer with different RNA subtypes. 219
Targeting the stromal desmoplastic reaction
PEGPH20, a recombinant pegylated hyaluronidase enzyme, was developed to specifically target hyaluronan in the tumor stroma. A large randomized phase II study reported promising results with this drug combined with nab-paclitaxel–gemcitabine. 220 In patients with tumor hyaluronic acid overexpression (IHC; 47/136 patients), the addition of PEGPH20 to nab-paclitaxel–gemcitabine significantly increased median progression-free survival from 5.2 to 9.2 months (HR: 0.51, p = 0.048). A large phase III trial (420 patients) that includes the specific subpopulation of patients with positive hyaluronidase IHC is evaluating PEGPH20 in combination with nab-paclitaxel–gemcitabine. 221 However, these results should be weighted with the recent publication of the randomized phase IB/II trial SWOG S1313, which found a deleterious effect of PEGPH20 in patients unselected for tumor hyaluronan status when combined with an mFOLFIRINOX protocol. 222
Another potential way to decrease the putative protective effect of the stroma is to block the Hedgehog signaling pathway. 223 After disappointing results of the agents of this therapeutic class in phase I/II studies,224,225 a phase III evaluating vismodegib is ongoing.
Immunotherapy
Immune checkpoint inhibitors
The first experimental attempt to use a CD40 agonist in combination with gemcitabine was relatively successful. 226 However, subsequent studies evaluating either anti-CTL4 or anti-PD1/PDL1 agents were disappointing. For example, in the case of anti-CTL4 agents, phase II studies of ipilimumab 227 and tremelimumab 228 reported no clinically significant effects. In a randomized phase II trial evaluating durvalumab in one arm and durvalumab plus tremelimumab in the other arm as a second-line treatment for pancreatic cancer, the disease control rate was less than 10% in both arms. 229 The development of this combination as a second-line treatment for pancreatic cancer has been cancelled. However, in the safety run of a randomized phase II study assessing the efficacy and safety of nab-paclitaxel–gemcitabine versus nab-paclitaxel–gemcitabine, durvalumab, and tremelimumab in 10 patients with untreated pancreatic cancer, the disease control rate was 100%, and median progression-free survival was 7.9 months. 230 Results of other studies evaluating the combination of ipilimumab and nivolumab plus chemotherapy (NCT022688825, NCT02558894) are pending.
Despite lack of hope that immune checkpoint inhibitors will show major efficacy in this disease, for the very few patients with a pathologically proven pancreatic cancer harboring a dMMR phenotype, a very high response rate has been observed with PD1/PD-L1 inhibitors in such dMMR/MSI tumors, 231 including in patients with pancreatic cancer. However, this eventuality is exceptional among cases of pancreatic cancer. 232
Vaccines
Cellular-based vaccines have given encouraging results but there is currently no clear proof that they will be used in clinical practice in the near future.
Peptide-based cancer vaccines
After a promising phase I/II study, a phase III trial evaluating a combination of chemotherapy with a telomerase vaccination (GV1001) failed to show a benefit. 233 Personalized peptides that aim to prevent progressive tolerance to cancer-related antigens have been developed and tested in combination with gemcitabine, with promising results. 234 G17DT, an immunogen producing neutralizing antibodies against the tumor growth factors amidated and glycine-extended forms of gastrin-17 was tested in an international multicenter randomized controlled trial. 235 Patients developing anti-G17DT responses (73.8%) survived longer than nonresponders or those on placebo (median survival, 176 versus 63 versus 83; log-rank test, p = 0.003).
Further clinical investigation is warranted to determine the effectiveness of such new combination therapies.
Whole-cell cancer vaccines
The concept of GVAX is based on the development of genetically engineered tumor cells that secrete granulocyte-macrophage colony-stimulating factor. GVAX has been combined with different substances, and, especially, with a Listeria vaccine expressing mesothelin. However, results remain disappointing at this time. Algenpantucel-L, composed of irradiated cancer cells expressing alpha-1,3-galactosyltransferase, gave promising results in a phase II study combining this whole-cancer vaccine with radiochemotherapy in an adjuvant setting (60 patients, median disease-free survival of 17.3 months). 236 However, a phase III trial (IMPRESS) did not meet its primary endpoint and the development of this compound has been stopped. 90
Combination of vaccines and immune checkpoint inhibitors
Ipilimumab combined with GVAX gave favorable survival results compared with ipilimumab alone in a small phase Ib randomized study (5.7 months versus 3.6 months). 237 Larger randomized trials evaluating the efficacy of this approach are ongoing (NCT01896869, NCT02548169). Depletion of tumor-associated fibroblasts by targeting the CXC112–CXCR4 axis may enhance T-cell infiltration and could be combined specifically with immune checkpoint inhibitors. An ongoing phase II trial is evaluating the efficacy of the combination of an anti-CXCR4 antibody (ulocuplumab) and nivolumab in pancreatic cancer and other solid tumors (NCT02472977).
Adoptive T-cell transfer
This kind of treatment requires collection of the patient’s T cells, followed by expansion and activation of the cells before they are reinfused. Three different types of T cells can be produced according to the method used for activation: tumor infiltrating lymphocytes (TILs), engineered T cells expressing a specific cancer T-cell receptor (TCR), and T cells that express a chimeric antigen receptor (CAR). The CAR-T cell method appears to be the most effective of these techniques. Preliminary data on the use of antimesothelin CAR-T cells suggest some activity in pancreatic cancer. 238 The carcinoembryonic antigen can also be targeted in pancreatic cancer, and there are trials ongoing to evaluate the role of CAR-T cells activated with carcinoembryonic antigen in pancreatic cancer. 239 The efficacy of CAR-T cells may even be increased in combination with immune modulators such as cyclophosphamide, or anti-CTLA4 and anti-PD1 agents, and several randomized trials are ongoing.
Cancer stemness inhibitors
A phase Ib/II trial testing a cancer stemness inhibitor, napabucasin (BBI-608), in combination with nab-paclitaxel–gemcitabine in metastatic pancreatic adenocarcinoma showed favorable trends in terms of response rate and survival. 240 Among 71 intent-to-treat patients, disease control was observed in 55 (77%), with 1 complete response (1.4%) and 26 partial responses (37%). A phase III trial is currently underway to confirm these data (NCT02231723).
Which treatments for elderly patients?
Patients over 65 years are unrepresented in clinical trials, and no randomized study is available in any setting. Concerning resectable patients, a large (n = 9533) retrospective study evaluated trends in resection rates and operative mortality in adults aged ⩾66 with locoregional pancreatic cancer and showed that the resection rate decreased with increasing age. 241 Increasing age also decreased the likelihood of evaluation by a surgeon (81% of those <70 versus 45% ⩾85 years). Surgical evaluation and resection rates decreased with age regardless of comorbidity status.
But, more generally, age is not correlated with an increased risk of death. 242 Given a significant increased rate of complications, surgical candidates need to be carefully selected, but PD is not excluded in elderly patients. 243 Some adjuvant trials with chemotherapy reported survival outcomes in patients ⩾65 years. In ESPAC-1, 74 ESPAC-3, 77 and JASPAC-1, 78 age was not found to be a prognostic factor for survival. In PRODIGE 24, no difference of efficacy was seen in patients ⩾65 compared with those ⩽ 65, demonstrated a preserved benefit in the older group. 17 However, the benefit for FOLFIRINOX in patients ⩾70 years was not significant.
Looking at palliative chemotherapy, older patients are less likely to received chemotherapy. Aldoss and colleagues reviewed cases of 440 metastatic patients aged ⩾ 80 years in the Veterans Affairs Central Cancer Registry from 1995 to 2007 and analyzed their median overall survival as their baseline comorbid conditions. 244 The multivariate analysis demonstrated that chemotherapy was associated with significant superior median overall survival (4.9 months, 95% CI 3.57–5.77) compared with no therapy (1.7 months, 95% CI 0.9–1.3) (HR = 0.41, p < 0.0001). A recent literature review found a number of studies showing that aging did not exclude the use of chemotherapy, since older patients appeared to have similar benefits to younger patients, although reduced-dose chemotherapy and enhanced supportive care were often required to ensure good safety. 245 Similar data were found in patients ⩾ 70 or 75 years receiving gemcitabine.246,247
Regarding gemcitabine + nab-paclitaxel and FOLFIRINOX pivotal trials, no difference of efficacy was seen between older and younger patients.159,161 Another small series confirmed the PRODIGE4 Accord 11 data using modified FOLFIRINOX. 248 A retrospective analysis of systemic therapy use of 237 patients ⩾75 years with metastatic disease, conducted between 2005 and 2013, found that systemic therapy was associated with longer survival in elderly patients. No significant difference was detected in survival between age groups 75–79, 80–84, and ⩾85 years of age among those who received systemic therapy. 249 Specific screening tools, such as Comprehensive Geriatric Assessment, may help to identify frail patients and better guide treatment decision in this population. 242
Supportive care and palliative care
In patients with locally advanced or metastatic pancreatic cancer, the objectives of palliative care are as follows.
(1) To promote the integration of a palliative care specialist as early as possible. Indeed, to be most effective, the concept of palliative care should be introduced early in the course of an illness, in conjunction with active disease treatment, 250 and, according to ASCO, preferably at the first visit. 166
(2) To encourage the palliative care specialist to view the patient’s care as his or her sole focus. This implies clear and accurate information regarding the disease diagnosis, including the communication of incurability, in order to choose ‘the right treatment, for the right patient, in the right setting’. 250 Therefore, multidisciplinary management (involving an oncologist, surgeon, radiotherapist, and palliative care physician) and shared decision making are needed at every stage of disease.
(3) To pay close attention to the physical comfort, psychosocial concerns, and spiritual well-being of the patient throughout the trajectory of illness. 166
(4) To take charge of the main physical symptoms related to the disease and their evolution (for example, pain, anorexia, weight loss, depression and anxiety, jaundice, gastric or duodenal obstruction, ascites, venous thromboembolism, asthenia). The aim is to maintain or improve quality of life.
(5) To address the issues of the end of life, and to encourage the writing of advance directives.
(6) To accompany and support the family, the entourage, and the caregivers.
Pain management
The ASCO recommends aggressive treatment of pain for patients with advanced pancreatic cancer. 166 Of these patients, 75% present with abdominal or back pain, and 80% of patients with advanced pancreatic cancer experience severe pain prior to death, commonly associated with malignant invasion of the celiac plexus. 250
Pain in pancreatic cancer has a complex physiopathology. It implies neural invasion and neurogenic inflammation. Therefore, the pain is nociceptive and neuropathic. 251 Pain management is based on several modalities: medical approach, chemotherapy and radiation therapy, interventional therapies, intrathecal therapy, and alternative medicine.
Medical approach
Opioids are considered to be the first-line medical therapy for visceral cancer pain, including pain from cancer of the pancreas (tramadol, morphine, oxycodone, or fentanyl). 166 Antiepileptics such as gabapentin and pregabalin are used as first-line treatment for neuropathic pain. Their effectiveness is also demonstrated in cancer-related neuropathic pain. 251 Nortriptyline and duloxetine also have analgesic efficacy. 166 Methadone can also be used in refractory neuropathic pain. However, its use must be managed by expert teams because of its long half-life and multiple drug–drug interactions. 252 Corticosteroids have proved particularly useful as adjuvant therapy for visceral pain. 251
Chemotherapy and radiation therapy
Pain control is largely implemented as a secondary end point in trials evaluating chemotherapy regimens in pancreatic cancer. For instance, FOLFIRINOX has been shown to be associated with better quality of life and pain control than gemcitabine in the management of metastatic pancreatic cancer. 163 Radiation therapy is particularly effective in controlling and relieving pain caused by large tumors compressing other organs or structures, such as nerves or the spine. The radiation therapy can shrink the tumor, which may help in relieving the pain. 251
Interventional therapies
For patients whose pain is refractory to opioids or who develop dose-limiting side effects from opioids, a block of the celiac plexus with local anesthetic is often employed. 251 The major component of pancreatic cancer pain is mediated by sympathetic fibers from the pancreas, and is relayed through the celiac plexus to the splanchnic nerves. A local anesthetic, usually bupivacaine, can be used in combination with steroids to temporarily inhibit the celiac plexus. Celiac plexus neurolysis represents the prolonged interruption of the plexus by the injection of alcohol or phenol. This technique is performed by anesthetists, radiologists, or endoscopists (using endoscopic ultrasonography). 252 In a double-blind, randomized clinical trial by the Mayo Clinic, early execution of neurolytic celiac plexus block was found to deliver a larger initial decrease in pain, and the improvement lasted longer than systemic analgesic therapy. 253 A meta-analysis of eight randomized studies reported that pancreatic cancer patients treated with celiac plexus block experienced lower levels of pain at 4 weeks and required less opioid medication than those on standard analgesics, but the difference in pain score did not maintain significance at 8 weeks. 254
Intrathecal therapy
Intrathecal therapy can be proposed for end-of-life stages or for refractory pain. Various molecules can be used, including morphine, fentanyl, local anesthetics, baclofen, or clonidine.255,256
Alternative medicine
Acupuncture 257 and hypnosis258,259 are increasingly common approaches to control pain in patients with cancer. They are an effective adjunctive method to manage cancer pain, and pain relief is improved compared with drug therapy alone.
Anorexia and weight loss
Patients with pancreatic cancer experience cachexia owing to appetite loss, malnutrition, and hypercatabolism. 250 The weight loss leads to weakness, fatigue, and a poor quality of life. Nutritional management must be carried out by a nutritionist or dietitian. 166 Patients on pancreatic enzymes along with dietary counseling gain body weight. 260 Appetite stimulant medications such as anamorelin may be considered in severe cases, 166 and achieved significant increases in hunger and caloric intake in a recent phase I study. 261
Depression and anxiety
The severity of the prognosis of pancreatic cancer can lead to depression and anxiety, even early in the course of disease. From 33% to 50% of patients with pancreatic cancer have depressive symptoms. Symptoms of clinical depression may include anorexia and weight loss, negative thoughts and behavior, sleep disturbance, anhedonia, fatigue, and feelings of hopelessness.262,263 Psychosocial factors (financial concerns or emotional support), medical factors (prognosis or metabolic derangements), and psychological factors (coping ability or perceptions of illness) can cause depression. Most experts recommend an approach that combines supportive psychotherapy, patient and family education, and stimulants or antidepressants/anxiolytics, or both. 254 Methylphenidate can be used by patients with limited life expectancy. It can improve energy, alertness, and weakness. 264 When the life expectancy of the patient is longer, selective serotonin reuptake inhibitors are used first. 252
Jaundice
During the course of disease, 70% to 80% of patients with tumors located in the head of the pancreas develop obstructive jaundice through blockage of the biliary tree. 265 The preferred treatment is endoscopic placement of a self-expanding stent in the bile duct to re-establish drainage to achieve relief of jaundice and pruritus. 166
Gastric or duodenal obstruction
Nearly 10% of patients will have gastric or duodenal obstruction. 265 Symptoms include early satiety, nausea, postprandial vomiting, and weight loss. Endoscopic duodenal stenting is usually successful.
Ascites
Ascites cause abdominal discomfort, nausea, and vomiting, and dyspnea from pressure of the fluid against the diaphragm. Their management is based on intermittent paracentesis, the use of diuretics such as spironolactone, or placement of a long-term drainage catheter. 166
Venous thromboembolism
Patients with pancreatic cancer have one of the highest risk of deep vein thrombosis or pulmonary embolism, with incidences ranging from 17% to 57% with a relative risk of venous thrombosis of 8.8. 266 The ASCO guidelines recommend primary prevention of venous thromboembolism with the use of low-molecular-weight heparins in all patients with potentially curable pancreatic cancer after resection, and in a case-by-case selection of high-risk patients undergoing systemic therapy. 166
Asthenia
Asthenia is one of the commonest symptoms of pancreatic cancer. Exercise during oncological treatment reduces fatigue and improves quality of life. 267 Studies dedicated to pancreatic cancer are ongoing. An adapted physical activity program should be proposed to limit this symptom. Medications such as corticosteroids, megestrol acetate, and stimulants (adrafanil, methylphenidate) can be used but they have limited effectiveness over time, and are a source of side effects such as the increase of thromboembolic risk with megestrol acetate. 268
To conclude, controlling physical symptoms, providing emotional support, preserving dignity, exploring realistic goals, and discussing day-to-day living are important to maintain hope in patients who are terminally ill with cancer, and in their families. 269 This is only possible with close collaboration between oncology teams and teams providing support and palliative care.
Conclusions
Pancreatic cancer is extremely difficult to treat. The goals of care and patient preferences should be discussed and precised with every patient diagnosed with pancreatic cancer. The absence of early warning symptoms, rapid metastatic dissemination, frequent sudden adverse events, and degradation of performance status score makes many patients unfit for chemotherapy. Palliative care will help to relieve main physical symptoms and to postpone degradation of quality of life. More efficient first-line regimens, such as FOLFIRINOX and gemcitabine with nab-paclitaxel, have improved overall survival in fit patients with metastatic disease, and may lead to conversion surgery in some patients with LAPC. Second-line chemotherapy regimens have been validated, mainly after gemcitabine as first-line therapy. Personalized medicine and immunotherapy had so far failed to improve the prognosis of these patients, yet a small subgroup of patients with BRCA mutations appear to be good candidates for treatment with PARP inhibitors.
Surgery combined with chemotherapy is still the only potentially curative treatment, but must be integrated into a complete multidisciplinary treatment sequence to optimize its effectiveness. Surgical progress has been made, improving overall survival, with perioperative and critical care and standardization of the surgical technique. In the borderline setting, the American and European definition criteria are similar, and allow a staging of the disease that must be used in routine practice. The two main remaining questions are: does induction therapy improve overall survival? And should we use chemotherapy or chemoradiotherapy to achieve this goal? Current trials underway should provide us with answers.
After resection, in the adjuvant setting, the mFOLFIRINOX regimen has recently shown superiority over gemcitabine alone and is a new standard of care in fit patients. The impact of chemoradiation remains uncertain both as adjuvant treatment and in locally advanced disease. The future major issue will be to test and to validate neoadjuvant or perioperative regimens using combination chemotherapy regimens.
Footnotes
Acknowledgements
The authors wrote the paper and agreed on the content. The manuscript has been revised for English by an independent scientific language editing service, Angloscribe, and the Institut de Cancérologie de Lorraine paid for this editing assistance.
Author Note
Thierry Conroy is also affiliated to Laboratoire EA4360 APEMAC, Université de Lorraine Ecole de Santé Publique Faculté de Médecine 9, avenue de la Forêt de Haye BP 20199 54505 Vandoeuvre Lès Nancy.
Funding
The author(s) received no financial support for the research, authorship, and publication of this article.
Conflict of interest statement
D.M. reports personal fees and nonfinancial support from Amgen, Bayer, Merck Serono, MSD, Roche, Sanofi, and Servier, personal fees from Shire, Halio Dx, Agios, and Pierre Fabre Oncologie, outside the submitted work; M.D. reports personal fees and nonfinancial support from Roche, MSD, Amgen, personal fees from Merck Serono, Bayer, Ipsen, Lilly, Servier, HalioDX, Sanofi outside the submitted work.
The other authors declare that they have no conflict of interest.