
Abstract
Lung cancer is the most common cancer and leading cause of cancer death. While targeted therapies have redefined treatment options for non-small cell lung carcinoma (NSCLC) with genetic aberrations such as epidermal growth factor and anaplastic lymphoma kinase, many patients do not harbour these oncogenic drivers. Cancer immunology has enabled the development of immune modulators that has dramatically altered the therapeutic landscape of advanced NSCLC. The success of immune-checkpoint inhibitors in pretreated NSCLC has led to the conduct of multiple studies exploring their role in the first-line setting. This article provides an overview of the evolving landscape of immune-checkpoint inhibitors with a focus on the programmed cell-death 1 (PD-1; pembrolizumab, nivolumab) and programmed cell-death ligand 1 (PD-L1; atezolizumab, durvalumab, avelumab) immune-checkpoint inhibitors as single agent or in combination with either chemotherapy or with another immune-checkpoint inhibitor in the treatment of NSCLC, the challenges faced, as well as future perspectives.
Keywords
Introduction
Worldwide, lung cancer is the most common cancer and leading cause of cancer death. In 2018, 2.09 million people were diagnosed with lung cancer and there were 1.76 million deaths from lung cancer. 1 Non-small-cell lung carcinoma (NSCLC), divided into two major groups by histology: squamous and nonsquamous, is the most common type of lung cancer, accounting for 84% of all lung cancer diagnoses. 2 While tyrosine kinase inhibitors (TKIs) have redefined treatment options for patients with genetic aberrations such as epidermal growth factor (EGFR) and anaplastic lymphoma kinase (ALK), many patients do not harbour these oncogenic drivers. Standard treatment for oncogene-negative patients was cytotoxic chemotherapy but prognosis remains poor and novel treatment approaches are needed.
An improvement in understanding the cancer immunology has enabled the development of immune-checkpoint inhibitors that has dramatically altered the therapeutic landscape of advanced NSCLC. 3 In this review, the evolving landscape of immune-checkpoint inhibitors in the first-line treatment of NSCLC and its future perspectives will be discussed (Figure 1).

The evolving landscape of immune-checkpoint inhibitors in advanced non-small-cell lung cancer.
Mechanism of immune-checkpoint inhibitors
One of the hallmarks of cancer is immune evasion, where the immune system does not effectively eliminate malignant cells. 4 Programmed cell-death 1 (PD-1) is a negative costimulatory receptor expressed primarily on the surfaces of activated T cells. The binding of PD-1 to one of its ligands, PD-L1 or PD-L2, can inhibit a cytotoxic T-cell response, thus allowing tumours to escape T-cell-induced antitumour activity. Pembrolizumab and nivolumab are humanized monoclonal immunoglobulin G4 (IgG4) kappa isotype antibodies against PD-1. The binding of pembrolizumab interrupts the engagement of PD-1 with its ligands. Atezolizumab, avelumab and durvalumab are anti-PD-L1 antibodies which interrupt the binding of PD-L1 to PD-1. The inhibition of PD-L1 to PD-1 results in tumour recognition by cytotoxic T cells.5–7
Cytotoxic T-lymphocyte antigen 4 (CTLA-4), expressed on regulatory T cells, competitively binds CD80 and CD86. CTLA-4 activation leads to the downregulation of helper T-cell activity and increases T regulatory immunosuppressive activity.8,9 Ipilimumab, a fully human IgG1 anti-CTLA-4 inhibitor interrupts the binding of CTLA-4 to CD80 and CD86.
Immune-checkpoint inhibitors monotherapy in the first-line treatment in advanced NSCLC
The success of immune-checkpoint inhibitors in the pretreated advanced NSCLC when compared with docetaxel led to the approval of nivolumab and atezolizumab regardless of PD-L1 status and pembrolizumab in PD-L1 positive tumours (PD-L1 ⩾ 1%; Table 110–16). This subsequently led to the conduct of multiple studies exploring the role of immune-checkpoint inhibitors in the first-line setting (Table 2).
Randomized phase III studies of immune-checkpoint inhibitors in pretreated advanced non-small-cell lung cancer.
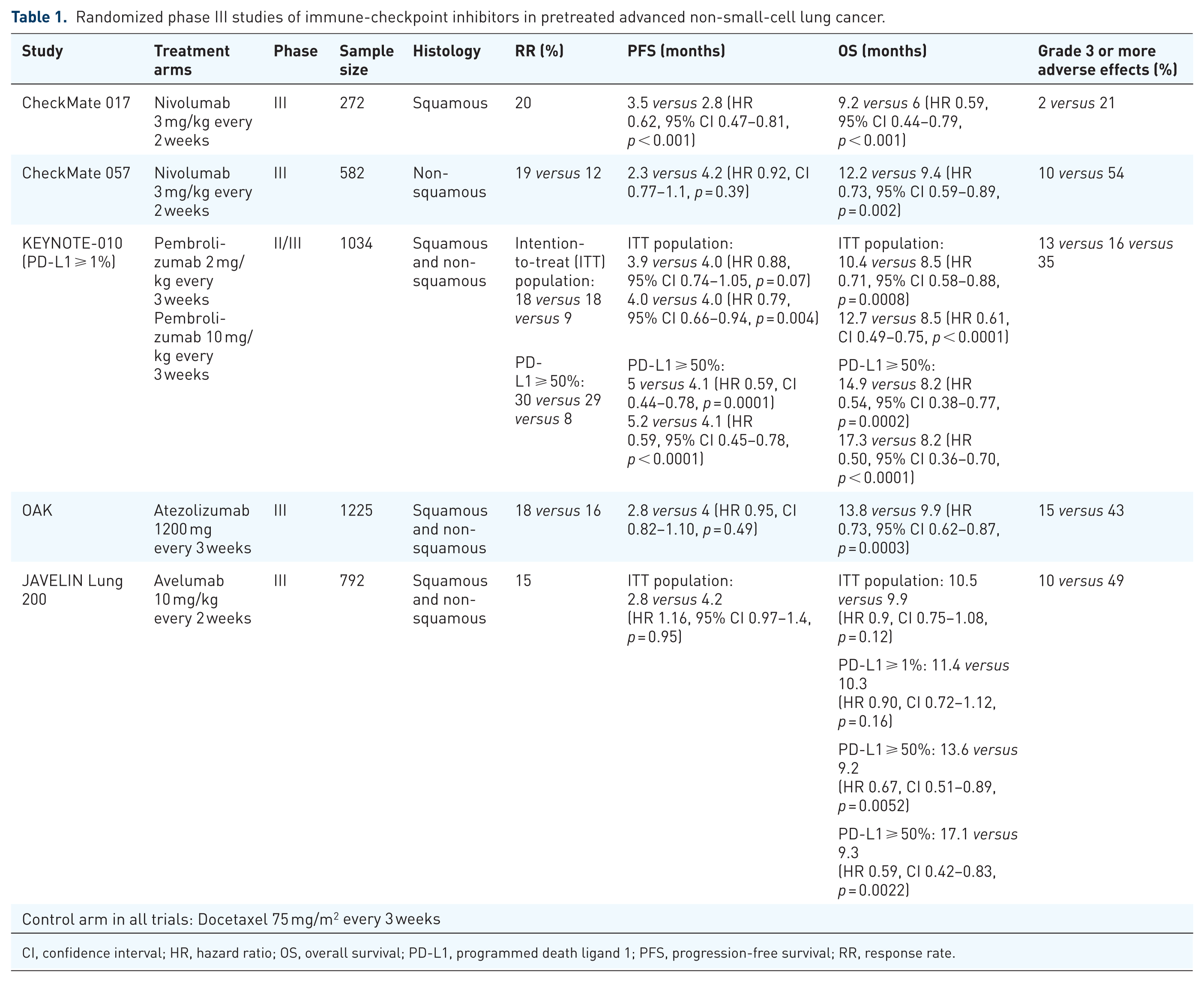
CI, confidence interval; HR, hazard ratio; OS, overall survival; PD-L1, programmed death ligand 1; PFS, progression-free survival; RR, response rate.
Immune-checkpoint inhibitors in the first-line treatment in advanced/metastatic NSCLC.

CI, confidence interval; HR, hazard ratio; IC, immune cell; ITT, intention to treat; NR, not reached; OS, overall survival; PD-L1, programmed cell-death ligand 1; PFS, progression-free survival; RR, response rate; TC, tumour cell; TMB, tumour mutational burden.
First-line pembrolizumab monotherapy
The role of pembrolizumab monotherapy in untreated advanced NSCLC was first explored in a large phase I study, KEYNOTE-001. In the cohort of patients with previously untreated advanced NSCLC, pembrolizumab was reported to show encouraging activity. In patients with tumour-expressing PD-L1 tissue polypeptide-specific antigen (TPS) ⩾ 50%, the objective response rate (ORR) was 66.7% whereas the ORR was 30.8% in patients with PD-L1 between 1 and 49%. Furthermore, reported progression-free survival (PFS) and overall survival (OS) in tumours with PD-L1 ⩾ 50% was promising.17,18
In a phase III study, KEYNOTE-024, patients with advanced NSCLC and a PD-L1 TPS ⩾ 50% were randomized to pembrolizumab for 35 cycles versus platinum-based chemotherapy for four to six cycles. The primary endpoint was met, with a significant improvement in median PFS seen in pembrolizumab versus chemotherapy treated patients and this benefit was evident in all subgroups examined. 19 In an updated analysis, the OS was 30.0 months in the pembrolizumab group versus 14.2 months in the chemotherapy group (Table 2). About 44% of patients who received chemotherapy crossed over to receive pembrolizumab. When adjusted for crossover, the OS still favoured pembrolizumab [hazard ratio (HR) 0.49, 95% confidence interval (CI) 0.34–0.69]. 20 Grade 3 or more treatment-related adverse events occurred in twice as many patients in the chemotherapy group as in the pembrolizumab group. 19
The results of KEYNOTE-024 led to the US Food and Drug Administration (FDA) approval of pembrolizumab for advanced NSCLC with PD-L1 TPS ⩾ 50%. However, what remained unknown was whether pembrolizumab was effective in patients with lower PD-L1 expression. Thus, a phase III study, KEYNOTE-042, was conducted to address the role of single-agent pembrolizumab in patients with PD-L1 TPS ⩾ 1%.
In this study, patients with advanced NSCLC without EGFR mutations or ALK rearrangement were randomized to receive pembrolizumab or platinum doublet. There were three primary endpoints: OS in patients with a PD-L1 TPS ⩾ 50%, ⩾20% and ⩾1%. The median OS was significantly higher across these three subgroups in patients treated with pembrolizumab versus chemotherapy (Table 2). In contrast to KEYNOTE-024, in patients with PD-L1 ⩾ 50%, pembrolizumab treatment was not associated with an improvement in PFS. In a prespecified exploratory analysis of the cohort with PD-L1 expression 1–49%, the OS in patients treated with pembrolizumab or chemotherapy was 13.4 months and 12.1months, respectively. This suggests the benefit seen in the overall population with a PD-L1 expression ⩾ 1% was driven by patients with high PD-L1 expression (>50%). Furthermore, the OS curves crossed, suggesting initial benefit with chemotherapy and subsequently a separate patient group that derived benefit from pembrolizumab. Identifying biomarkers in this group of patients with a PD-L1 TPS 1–49% who obtained benefit from pembrolizumab would therefore be of major interest. Grade 3 or more treatment-related adverse events were more frequent in the chemotherapy arm (Table 2). 20
Based on the results from KEYNOTE-042, the FDA recently granted approval for pembrolizumab monotherapy for patients with stage III NSCLC who are not candidates for surgical resection or definitive chemoradiation, or have metastatic NSCLC. Tumours must express PD-L1 ⩾ 1% and not harbour EGFR mutations or ALK rearrangement.
The efficacy of pembrolizumab monotherapy in EGFR-mutant advanced NSCLC was reported recently. In a single-arm phase II study, EGFR TKI-naïve patients with advanced NSCLC with PD-L1 ⩾ 1% were recruited. Enrolment was halted because of lack of efficacy after 11 of 25 planned patients were treated. Despite being enriched for high PD-L1 expression (73% of patients with a PD-L1 ⩾ 50%), the ORR was 9% (1/11). Of the single responder, repeat EGFR mutation testing revealed the original report of EGFR exon 19 deletion to be erroneous, thus the actual ORR in 10 patients was 0%. 21 Of the seven patients receiving subsequent EGFR TKIs, six patients (86%) developed an adverse event attributed to TKI use, with one case of fatal pneumonitis 89 days after commencing erlotinib. It is unknown whether pembrolizumab contributed to the development of pneumonitis but its manifestation raises issues about the potential risks of sequencing with immune-checkpoint inhibitors and EGFR TKIs. Based on this study, pembrolizumab is not an appropriate treatment option for patients with treatment-naïve EGFR-mutant NSCLC expressing PD-L1 and concerns remain regarding the safety of sequencing EGFR TKIs after immune-checkpoint inhibitors.
First-line nivolumab monotherapy
A phase III study, CheckMate 026, explored the efficacy of nivolumab compared with platinum-based chemotherapy as first-line therapy in patients with advanced NSCLC with PD-L1 ⩾ 1%. The primary endpoint was PFS among patients with PD-L1 ⩾ 5%. There was no PFS or OS benefit seen with nivolumab (Table 2). 22
The results from CheckMate 026 are inconsistent with first-line nivolumab in phase I and II trials. 23 What could possibly account for this? First, the characteristics of patients in both arms of the study are different. The proportion of patients with PD-L1 ⩾ 50% are 47% and 32% in the chemotherapy and nivolumab group, respectively. Second, 43% of patients in the nivolumab arm crossed over to receive subsequent chemotherapy, and 64% of patients who received chemotherapy crossed over to receive immunotherapy. The lower rates of crossover in patients who received nivolumab might have contributed to the lack of OS benefit. In an exploratory analysis, the authors found higher response rates in patients with a high tumour mutational burden (47% versus 28%) and longer PFS.24,25
While KEYNOTE-024 established the role for pembrolizumab as first-line treatment for NSCLC with a PD-L1 TPS ⩾ 50%, the results from CheckMate 026 were discordant. The factors explaining the differences in results between KEYNOTE-024 and CheckMate 026 are unknown but might be attributable to differences in patient selection. Patient selection was based on a tumour PD-L1 expression cut-off of 1%. In contrast, a PD-L1 cut-off of 50% using a prospectively validated assay (22C3) was used in KEYNOTE-024.
First-line atezolizumab monotherapy
In the multicohort, single-arm phase II trial (BIRCH), a cohort of patients with chemotherapy-naïve advanced NSCLC was treated with first-line atezolizumab. All patients had PD-L1 ⩾ 5% on tumour cells (TCs) or immune cells (ICs) using the SP142 immunohistochemistry assay. The ORR, PFS and OS were 22%, 5.4 months and 23.5 months, respectively. In patients with TC3 (TC PD-L1 ⩾ 50%) or IC3 (IC PD-L1 ⩾ 10%), ORR was 31%. 26
In another multicohort phase II study (FIR), the efficacy and safety of patients with PD-L1 staining on ⩾5% of TCs or PD-L1 staining on ⩾5% of ICs were assessed. The cohort of patients who were chemotherapy naïve or more than 6 months between adjuvant chemotherapy and recurrence, were treated with single-agent atezolizumab, the ORR, PFS and OS were 32%, 5.5 months and 14.4 months, respectively. In patients with TC3 or IC3, the ORR was 43%. 27
A single-arm phase II trial, BF1RST, enrolled patients with PD-L1 unselected, advanced NSCLC, with high levels of blood tumour mutation burden to receive atezolizumab. The ORR in the overall intention-to-treat population was 14.5%. 28 Results based on tumour mutation burden (TMB) status will be discussed in a later section.
Combination first-line immune-checkpoint inhibitor and chemotherapy
Single-agent immune-checkpoint inhibitors have transformed the paradigm of advanced NSCLC in both front line and after failure of platinum-containing chemotherapy. Despite the improvement, not all patients will benefit from single-agent immune-checkpoint inhibitor with an ORR of 45% versus 27% in PD-L1 50% or more and 1% or more, respectively.18–20 Historically, it was thought cytotoxic chemotherapy was immunosuppressive but ample evidence has shown chemotherapy can modulate the immune response against tumours and may increase the efficacy of immune-checkpoint inhibitors. The overall goal of combination immune-checkpoint inhibitor and chemotherapy is to achieve additive or synergistic clinical activity. This objective can be achieved by two major approaches. First, by using chemotherapy to induce immunogenic cell death and second, by using chemotherapy to interfere with the mechanisms used by the tumour to evade immune recognition.29–32 This has led to the conduct of studies exploring the role of immune-checkpoint inhibitors and chemotherapy in the first-line treatment of advanced NSCLC.
Pembrolizumab and chemotherapy
In a phase II study (KEYNOTE-021G), patients with nonsquamous histology and without EGFR mutations or ALK rearrangement were randomized to carboplatin–pemetrexed and pembrolizumab or carboplatin–pemetrexed. The study reported an improvement in response rate, PFS and trend towards an improvement in OS (Table 2).33,34 The increased activity seen when combining pembrolizumab with chemotherapy in nonsquamous histology was confirmed in a subsequent phase III study, KEYNOTE-189.
KEYNOTE-189 and KEYNOTE-407 enrolled patients with advanced nonsquamous and squamous NSCLC respectively. KEYNOTE-189 randomized patients to platinum-pemetrexed with or without pembrolizumab, followed by maintenance pemetrexed or pemetrexed/pembrolizumab. There was clear OS and PFS benefit with the addition of pembrolizumab to chemotherapy. OS benefit was seen across all patient subgroups including a cohort without PD-L1 expression. It should be noted that the degree of benefit with combination therapy was associated with PD-L1 status with a larger benefit seen with tumours with a higher PD-L1 expression. There was also PFS benefit in most subgroups except in patients aged > 65 years or PD-L1 TPS < 1%. Likewise, in KEYNOTE-407, both OS and PFS were improved in the overall patient population, as well as all subgroups. With the caveat of cross-trial comparisons, in these studies, the response rates with the combination therapy were higher than seen in monotherapy (47.6% in KEYNOTE-189 and 57.9% in KEYNOTE-407). Toxicities were generally manageable and rates of all-grade toxicities and grade 3–5 toxicities were similar in both arms, with expected rates of immune-related adverse effects in the immunotherapy arms (Table 2; Figure 3).35,36 Based on the results from KEYNOTE-189 and KEYNOTE-407, the FDA recently approved pembrolizumab in combination with chemotherapy in previously untreated advanced nonsquamous and squamous NSCLC.
Currently, we believe that in patients without EGFR mutations or ALK rearrangement and with PD-L1 = 1–49%, combination chemotherapy and pembrolizumab is the best option in the treatment of first-line advanced NSCLC (Figure 2) and single-agent pembrolizumab perhaps considered in patients who are unfit or unwilling to receive platinum-based chemotherapy. For patients without EGFR mutations or ALK rearrangement with PD-L1 ⩾ 50%, treatment options include either single-agent pembrolizumab or the combination of chemotherapy and pembrolizumab. It should be noted no study has compared chemotherapy plus pembrolizumab versus pembrolizumab monotherapy. In the absence of direct comparative data for these patients, we believe that single-agent pembrolizumab should be considered for the majority of patients, which would allow the option of using a platinum-based doublet in the second-line setting, whereas first-line combination chemotherapy and pembrolizumab should be considered in patients with symptomatic or rapidly progressive disease. In such patients, early progression with single-agent pembrolizumab may lead to a decline in performance status, precluding a second-line platinum doublet. Studies comparing single-agent pembrolizumab with chemotherapy and pembrolizumab in patients with NSCLC PD-L1 ⩾ 50% may provide further clarity on the optimal treatment approach.

Case of a 57-year-old man, never smoker, who presented with a retrocardiac mass on routine health screening.
Nivolumab and chemotherapy
CheckMate 227 is a multipart phase III trial evaluating different nivolumab-based regimens versus chemotherapy in distinct patient populations (PD-L1 < 1% and PD-L1 ⩾ 1%). Patients with PD-L1 < 1% were randomized to platinum-based chemotherapy alone, platinum-based chemotherapy with nivolumab or nivolumab with ipilimumab. Patients with PD-L1 ⩾ 1% were randomized to platinum-based chemotherapy alone, nivolumab alone or nivolumab with ipilimumab. 37
Part 1 of the CheckMate 227 evaluated PFS and OS of combination immune-checkpoint inhibitor versus chemotherapy. In patients with PD-L1 < 1%, PFS was improved with nivolumab and chemotherapy combination versus chemotherapy alone (HR 0.74, 95% CI 0.58–0.94). Among histological subgroups, benefit was more pronounced in nonsquamous NSCLC (HR = 0.68) relative to squamous NSCLC (HR = 0.92). The rates of treatment-related adverse events leading to discontinuation were 13% and 14%, respectively.37,38 The ongoing part 2 CheckMate 227 will be evaluating OS in PD-L1% unselected patients receiving chemotherapy with or without the addition of nivolumab.
Atezolizumab and chemotherapy
Multiple phase III studies examining the role of combination atezolizumab with chemotherapy in the first-line treatment of advanced NSCLC have been conducted (Table 2). IMpower 150 randomized patients with advanced, untreated nonsquamous NSCLC to carboplatin and paclitaxel combined with atezolizumab (ACP), atezolizumab plus bevacizumab (ABCP) or bevacizumab (BCP). ABCP demonstrated improved and OS over BCP. Based on these results, ABCP has been approved by the US FDA and the European Medicines Agency (EMA) for first-line treatment of patients with NSCLC without EGFR mutation or ALK rearrangement. 39 Outcomes in a subset of patients harbouring EGFR mutations or ALK rearrangement (14% of the study population) were also analysed. In this molecularly defined group treated with ABCP versus BCP, the PFS and OS was 9.7 months versus 6.1 months (HR 0.59, 95% CI 0.37–0.94) and not reached versus 17.5 months (HR 0.54, 95% CI 0.29–1.03), respectively.39,40 IMpower 150 is the first study to demonstrate an improvement in outcomes in patients with EGFR mutations or ALK rearrangement treated with the combination of chemotherapy, BCP and atezolizumab. Based on these findings, the EMA has approved the use of ABCP in the treatment of patients with NSCLC harbouring EGFR mutations or ALK translocation after failure of appropriate targeted therapies.
IMpower 130 evaluated the addition of atezolizumab to carboplatin and nab-paclitaxel in patients with previously untreated nonsquamous NSCLC. There was a PFS and OS benefit seen in all PD-L1 subgroups in patients treated with atezolizumab, carboplatin and nab-paclitaxel. In contrast to IMpower 150, in this study, where BCP was not part of the treatment, there was no PFS and OS benefit seen in the subset of patients with EGFR/ALK genomic alterations. Nab-paclitaxel was chosen because it does not require steroid premedication which may affect response to immune-checkpoint inhibitors. 41
In IMpower 132, patients with advanced nonsquamous NSCLC were randomized to cisplatin or carboplatin plus pemetrexed and atezolizumab followed by maintenance pemetrexed and atezolizumab or to platinum/pemetrexed followed by maintenance pemetrexed. There was a significant PFS benefit and a nonsignificant trend towards an improvement in OS seen. 42
IMpower 131 was designed to evaluate the addition of atezolizumab to carboplatin with paclitaxel/nab-paclitaxel in previously untreated, PD-L1 unselected squamous NSCLC. While there is a PFS benefit, the interim OS result was not significantly different with the addition of atezolizumab (Table 2). 43
Combination first-line immune-checkpoint inhibitor and immune-checkpoint inhibitor
Dual immune-checkpoint blockade has also shown promise. PD-1 and CTLA-4 modulates the immune system through distinct, complementary mechanisms and enhances antitumour activity. 44
Nivolumab and ipilimumab
The phase I CheckMate 012 trial combined nivolumab with ipilimumab and found encouraging efficacy with a tolerable safety profile. 45 The phase II CheckMate 568 trial confirmed this and found that a TMB ⩾ 10 mutations/megabase was associated with response, irrespective of tumour PD-L1 expression. 46
Part 1 of CheckMate 227 had two coprimary endpoints: to evaluate PFS with nivolumab and ipilimumab versus chemotherapy based on TMB status with a cut-off of ⩾10 mutations/megabase as determined from CheckMate 568 and to look at OS based on PD-L1 expression level.37–38 TMB was evaluable in 57.7% of the study population (1004 patients). Out of these patients, 444 (44.2%) had TMB ⩾ 10. In patients with a high TMB, nivolumab/ipilimumab was associated with longer PFS than chemotherapy. The 1-year PFS rate was also significantly higher with nivolumab plus ipilimumab (42.6% versus 13.2%).
Of note, there was no association between TMB and PD-L1 expression, suggesting TMB is an independent biomarker predicting benefit from nivolumab and ipilimumab, separate from PD-L1 status (Table 2).37,38 In a recent update, there was no difference in OS between patients with high or low TMB levels. In patients with TMB ⩾ 10 mutations/megabase treated with ipilimumab and nivolumab, the OS was 23.03 months versus 16.72 months for chemotherapy (HR 0.77, 95% CI 0.56–1.06), whereas in patients with a TMB < 10 mutations/megabase, the median OS was 16.20 months versus 12.42 months, respectively (HR, 0.78, 95% CI, 0.61–1.00). 47
In an analysis of patients with low PD-L1 expression (<1%), in patients with high TMB (⩾10 mutations/megabase), the combination of nivolumab/ipilimumab was associated with a longer PFS versus chemotherapy (HR 0.48, 95% CI 0.27–0.85). In patients with low TMB (<10 mutations/megabase), there was no difference in PFS for nivolumab/ipilimumab versus chemotherapy (HR 1.17, 95% CI 0.76–1.81) or for chemotherapy/nivolumab versus chemotherapy (HR 0.87, 95% CI 0.87–1.33). 39
Durvalumab
A phase Ib trial showed manageable safety profile of durvalumab and tremelimumab with antitumour activity regardless of PD-L1 expression. As such, the dose of durvalumab 20 mg/kg plus tremelimumab 1 mg/kg every 3 weeks was selected for the phase III studies in the first-line setting. 48
MYSTIC, a randomized phase III study, assigned patients to durvalumab alone, durvalumab plus tremelimumab or chemotherapy in patients with NSCLC and unselected PD-L1. Durvalumab alone or with tremelimumab versus chemotherapy did not improve OS (HR 0.76, 95% CI 0.56–1.02 and HR 0.85, 95% CI 0.61–1.17, respectively). There was also no PFS benefit from durvalumab plus tremelimumab compared with chemotherapy (HR 1.05, 95% CI 0.722–1.534). 49 In a post hoc exploratory analysis, a high blood TMB [⩾20 mutations/megabase as determined by analysis of circulating tumour deoxyribonucleic acid (DNA)], was associated with an improved OS with combination durvalumab plus tremelimumab compared with chemotherapy (22 months versus 10 months; HR 0.49, 95% CI 0.32–0.74) and a nonsignificant improvement in OS for durvalumab versus chemotherapy (13 versus 10 months; HR 0.72, 95% CI 0.50–1.05). 50 The safety and tolerability of durvalumab alone or in combination with tremelimumab were consistent with previously reported studies.
NEPTUNE is a phase III study that randomized patients of any PD-L1 status to durvalumab and tremelimumab versus chemotherapy, 51 and POSEIDON randomized patients to platinum-based doublets alone, durvalumab and chemotherapy versus durvalumab/tremelimumab and chemotherapy. 52 Both studies are ongoing and results may provide further clarity on the role of durvalumab and tremelimumab in the first-line setting.
Challenges and future directions in first-line treatment of NSCLC
Since the FDA approval of nivolumab in 2015 in pretreated NSCLC, immune-checkpoint inhibitors have rapidly transited to the first-line setting, with approval obtained for multiple immune-checkpoint inhibitors in a short period of time (Figure 1). Studies of other single-agent immune-checkpoint inhibitors such as atezolizumab, durvalumab and avelumab versus chemotherapy in the first-line setting are ongoing (Table 3).
Selected ongoing phase III studies of immune-checkpoint inhibitor trials in first-line setting.
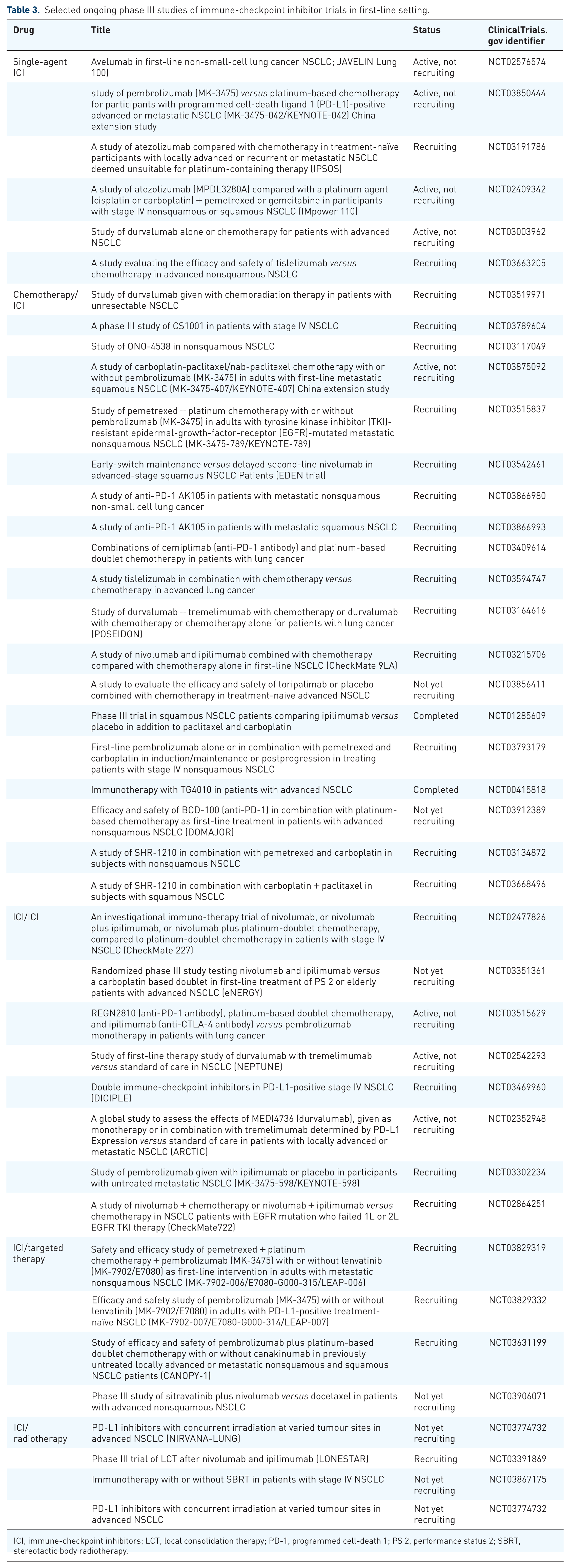
ICI, immune-checkpoint inhibitors; LCT, local consolidation therapy; PD-1, programmed cell-death 1; PS 2, performance status 2; SBRT, stereotactic body radiotherapy.
The superiority chemotherapy combined with an immune-checkpoint inhibitor versus chemotherapy in the first-line setting has provided greater therapeutic options but has simultaneously created some uncertainty on what is the optimal approach in patients with PD-L1 expression of at least 50% where either single-agent pembrolizumab or combination chemotherapy with an immune-checkpoint inhibitor are both superior to chemotherapy. As discussed earlier, pembrolizumab monotherapy can be considered for most patients, as this would enable the use a platinum-based doublet in the second-line setting and combination chemotherapy and pembrolizumab should be considered in patients with symptomatic or rapidly progressive disease. Further research in identifying biomarkers that predict response and allow selection for monotherapy versus combination therapy is required.53,54
Another challenge involves the issue of treatment after first-line therapy. In patients who have progressed after treatment with an immune-checkpoint inhibitor, standard treatment would be either a platinum-based doublet if the patient was chemotherapy naïve, or if they have received platinum-based chemotherapy with an immune-checkpoint inhibitor, second-line chemotherapy, which would be docetaxel with or without nintedanib 11 or ramucirumab 10 and Titanium silicate (TS)-1. 55 It should be noted in these phase III trials in the pretreated setting, none of the patients have received a prior immune-checkpoint inhibitor. The benefit of immune-checkpoint inhibitors in patients who have progressed after first-line immune-checkpoint-inhibitor treatment represents an unmet need with research, focusing on understanding the mechanisms of resistance56–58 and novel combination immunotherapy studies targeting the tumour microenvironment, increasing costimulatory signals and T-cell priming being areas of major therapeutic interest.59–61
While responses have been observed in patients who were rechallenged in the pretreated setting, 62 in patients who have progressed several months or years after the last dose of first-line immune-checkpoint inhibitor, the role of rechallenge with immune-checkpoint inhibitor either as monotherapy or in combination with chemotherapy is unknown.
The management approach of patients treated with a first-line PD-1 or PD-L1 inhibitor and have developed disease progression in one or two sites is also unknown. In the pretreated setting, a retrospective study reported local therapy to the sites of progression with radiofrequency ablation, radiotherapy, or surgery with continuation of systemic therapy with immune-checkpoint inhibitor may be effective, with a 2-year survival rate of 92%. 63 It should be noted that data supporting this approach is scant and systemic therapy is still standard. Further studies examining the management of oligo-progression in patients with advanced NSCLC treated with first-line immune-checkpoint inhibitors should be explored.
The use of PD-1 and PD-L1 inhibitors in patients with NSCLC harbouring EGFR mutations or ALK rearrangement after progression with standard targeted therapy remains a challenge for several reasons. First, EGFR-mutant and ALK-rearranged NSCLC are associated with a lower TMB and an uninflamed and an immunosuppressive tumour microenvironment; factors associated with reduced sensitivity to immune-checkpoint inhibition.64,65 Second, blunted efficacy with single-agent immune-checkpoint inhibitor has been observed in the first-line 21 and pretreated setting.66–68 Third, there is limited randomized data. With the exception of IMpower 150 and IMpower 130, many first-line immune-checkpoint-inhibitor studies excluded patients with EGFR mutant and ALK rearranged NSCLC. In the treatment-naïve setting, EGFR TKIs and ALK TKIs remain the standard of care in advanced EGFR- and ALK-positive NSCLC. In patients who have progressed after EGFR TKI therapy, platinum-doublet chemotherapy remains standard of care with atezolizumab/BCP/carboplatin/paclitaxel being an option. The role of immune-checkpoint inhibitors in combination with chemotherapy in patients with EGFR-TKI-resistant EGFR-mutant NSCLC are being explored in KEYNOTE-789 [ClinicalTrials.gov identifier: NCT03515837] and CheckMate 722 [ClinicalTrials.gov identifier: NCT02864251; (Table 3)]. Studies of potential therapeutic targets including CD73 and the adenosine pathway69,70 are ongoing [ClinicalTrials.gov identifiers: NCT03454451, NCT02503774, NCT03381274, NCT03819465, NCT03822351].
Currently, PD-L1 expression using immunohistochemistry is the only approved biomarker in the first-line setting and its expression plays an important role in the selection of treatment for patients with EGFR-/ALK-negative advanced NSCLC. Pembrolizumab monotherapy was initially approved with a tumour PD-L1 expression ⩾ 50% 18 and was subsequently approved for a PD-L1 expression ⩾ 1%, based on the results of KEYNOTE-042. 20 In KEYNOTE-042, the benefit of pembrolizumab appears to be greater with increasing PD-L1 expression with the HR for OS 0.69, 0.77 and 0.81 for PD-L1 cut-offs of ⩾50%, ⩾20% and ⩾1%, respectively. Furthermore, in KEYNOTE-042, exploratory analysis found no survival benefit in the subgroup with PD-L1 expression 1–49%, suggesting the benefit seen in the population with PD-L1⩾1% was carried by the cohort expressing ⩾50% expression. The observation of a higher PD-L1 expression being associated with a greater magnitude of benefit was also seen in studies of combination and pembrolizumab,35,36 as well as in the second-line studies.12–16 Based on these data, in patients with a PD-L1 expression ⩾ 50%, we recommend single-agent pembrolizumab and combination chemotherapy and pembrolizumab in selected cases such as symptomatic or rapidly progressive disease. In patients with PD-L1 1–49%, we suggest chemotherapy and pembrolizumab should be standard and pembrolizumab monotherapy perhaps considered in patients unfit for, or who decline, chemotherapy. In patients with a PD-L1 expression < 1%, chemotherapy and pembrolizumab is recommended.
Although not yet standard clinical practice, TMB as a predictive marker is gaining traction. TMB has been shown associated with improved outcomes in patients with pretreated NSCLC treated with pembrolizumab 71 atezolizumab 72 and ACB and with nivolumab in the first-line setting. 23 In the BF1RST study, a prospective study evaluating the clinical utility of blood TMB as a predictive biomarker for first-line ACB, in patients with high (⩾16 mutations/megabase) versus low (<16 mutations/megabase) blood TMB, the ORR was 28.6% and 4.4%, respectively, the PFS was 4.6 months and 3.7 months, respectively (HR 0.66, 90% CI 0.42–1.02) and the OS was not estimable versus 13.1 months, respectively (HR 0.77, 90% CI, 0.41–1.43). 73 Based on these promising results, the BFAST, a randomized phase III study [ClinicalTrials.gov identifier: NCT03178552], is ongoing to confirm these findings. With combination therapy, nivolumab/ipilimumab 46 and durvalumab/tremelimumab 49 was associated with improved outcomes versus chemotherapy in patients with high TMB. Despite the emerging promising data, TMB as a predictive marker for combination CTLA-4/PD-1 inhibition is currently not part of routine clinical practice, as this combination has not been shown to improve OS;46,47 but it has been suggested as an optional treatment regimen for patients with NSCLC with a high TMB. 74 Although challenges exist in the use of TMB in routine practice, such as cost of TMB testing, high tumour DNA requirements and long turnaround time, 75 these potential barriers are being addressed with the rapid technological advances in next-generation sequencing (NGS), the potential utility of plasma TMB 73 and the increasing affordability of NGS, to enable the use of TMB in routine clinical practice. 76
A subset of patients, however, do not benefit from single immune-checkpoint inhibition in the first-line setting, with some patients experiencing early progression in KEYNOTE-024, KEYNOTE-042 and CheckMate-026. Much work remains to identify other, more accurate predictive biomarkers that will allow better patient selection, even among patients with high PD-L1 expression.
With regards to immune-related toxicities, while any organ or tissue may potentially be involved, some immune-related adverse events (irAEs) occur much more commonly than others (Figure 3). Hypothyroidism and hyperthyroidism occur frequently (6–12% and 3–7%, respectively) but most are low-grade adverse events. The incidence of grade 3 or more adverse events is highest for pneumonitis (1–3%). The incidence of irAEs is similar in single-agent immune-checkpoint inhibitor and immune-checkpoint inhibitor/chemotherapy combination (22–29%).
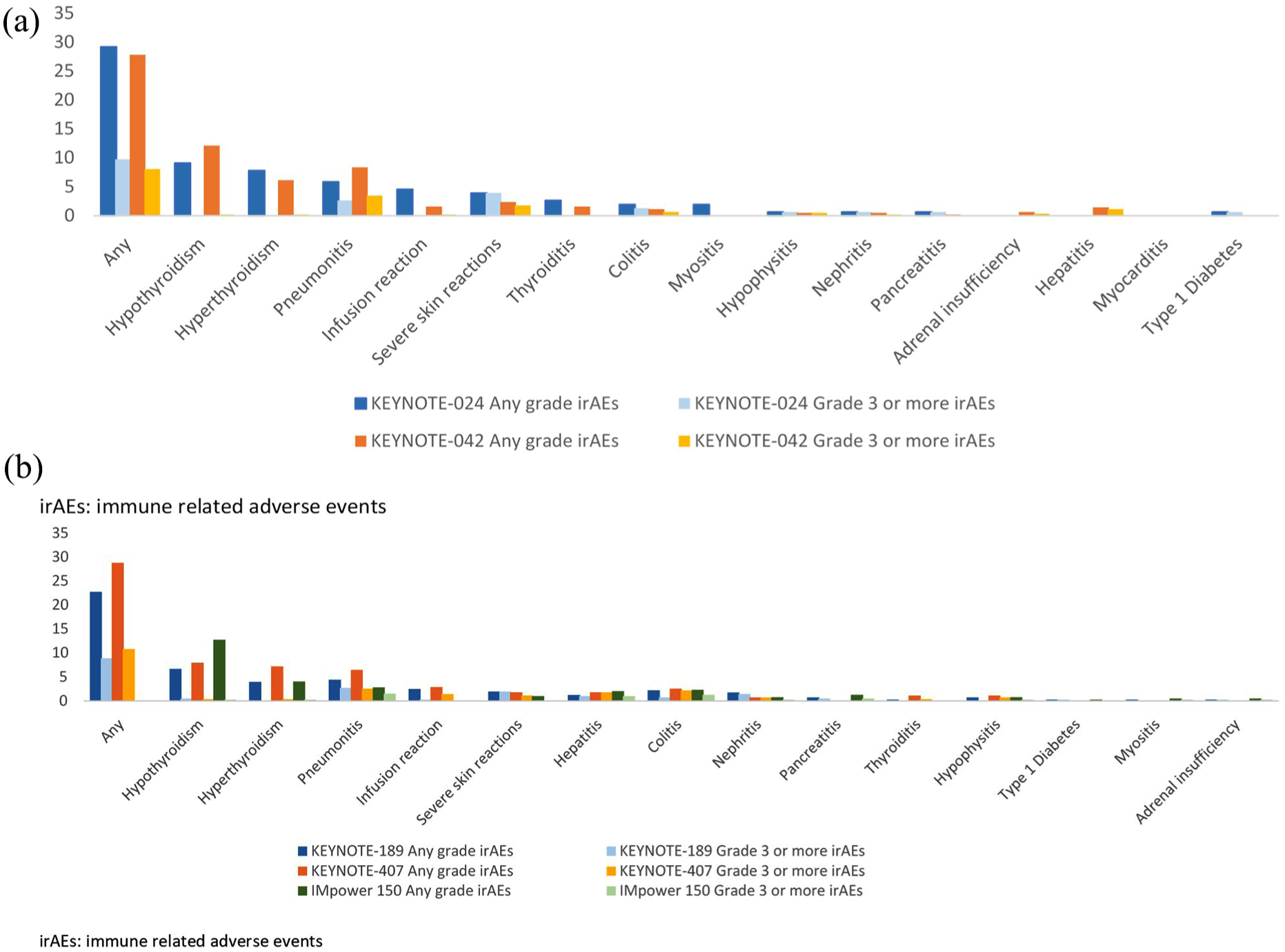
Percentage of immune-related adverse events in selected phase III studies.
Future research should focus on the management of irAEs, attempting to understand why some patients respond better, increasing the response rates to immune-checkpoint inhibitors and lastly, identifying other pathways to target to improve clinical outcomes. Selected ongoing phase III immune-checkpoint inhibitor trials for first-line treatment of advanced NSCLC are summarized in Table 3.
Conclusion
Treatment of advanced NSCLC with immune-checkpoint inhibitors has evolved over recent years. In the second-line setting, treatment options have previously included docetaxel, with or without ramucirumab, an antivascular endothelial growth factor receptor-2 antibody 10 or nintedanib, 11 an oral angiokinase inhibitor. In 2015, the FDA approved nivolumab for use in pretreated advanced NSCLC based on the results of two phase III studies, CheckMate 017 and CheckMate 057.12,13 In these studies, nivolumab was superior to second-line docetaxel in terms of response rate (RR) and OS for squamous cell and nonsquamous histology, respectively. Subsequently, pembrolizumab and atezolizumab were also approved for use in patients with advanced NSCLC who have progressed on platinum-based therapy, based on an improvement in OS compared with docetaxel14,15 (Figure 1; Table 1). Avelumab, in contrast, did not show any OS benefit over docetaxel in the overall population in JAVELIN Lung 200.
Subsequent research, outlined in the review above, has established a role for immune-checkpoint inhibitors in first-line treatment of patients with advanced NSCLC expressing PD-L1 without EGFR or ALK aberrations, either as a monotherapy or in combination with chemotherapy. In patients with PD-L1⩾ 50%, options are either single-agent pembrolizumab or the combination of chemotherapy and pembrolizumab; whereas for patients with PD-L1 1–49%, chemotherapy and pembrolizumab should be considered the best option and pembrolizumab monotherapy is an acceptable option for patients who are unfit or unwilling to receive platinum-based chemotherapy (Figure 4). Multiple studies have also shown chemotherapy with atezolizumab, as well as carboplatin/paclitaxel/ABCP, is active in the first-line setting. When compared with cytotoxic chemotherapy, the use of single-agent immune-checkpoint inhibitors is associated with less toxicities and with combination chemotherapy and immune-checkpoint inhibitor, side effects were higher but tolerable. Ongoing major areas of research include the identification of other biomarkers beyond PD-L1 expression to select patients for combination therapy or immune-checkpoint inhibitor monotherapy, characterization of mechanisms of resistance and determining treatment strategies to overcome resistance and optimise efficacy.

Potential first-line treatment options for advanced non-small-cell lung cancer.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
RAS has received honoraria from Astra-Zeneca, BMS, Boehringer Ingelheim, Celgene, Lilly, Merck, Novartis, Pfizer, Roche, Taiho, Takeda, and Yuhan; and research funding from Astra-Zeneca and Boehringer Ingelheim. The other authors report no conflict of interest.