
Abstract
Cannabis has the potential to modulate some of the most common and debilitating symptoms of cancer and its treatments, including nausea and vomiting, loss of appetite, and pain. However, the dearth of scientific evidence for the effectiveness of cannabis in treating these symptoms in patients with cancer poses a challenge to clinicians in discussing this option with their patients. A review was performed using keywords related to cannabis and important symptoms of cancer and its treatments. Literature was qualitatively reviewed from preclinical models to clinical trials in the fields of cancer, human immunodeficiency virus (HIV), multiple sclerosis, inflammatory bowel disease, post-traumatic stress disorder (PTSD), and others, to prudently inform the use of cannabis in supportive and palliative care in cancer. There is a reasonable amount of evidence to consider cannabis for nausea and vomiting, loss of appetite, and pain as a supplement to first-line treatments. There is promising evidence to treat chemotherapy-induced peripheral neuropathy, gastrointestinal distress, and sleep disorders, but the literature is thus far too limited to recommend cannabis for these symptoms. Scant, yet more controversial, evidence exists in regard to cannabis for cancer- and treatment-related cognitive impairment, anxiety, depression, and fatigue. Adverse effects of cannabis are documented but tend to be mild. Cannabis has multifaceted potential bioactive benefits that appear to outweigh its risks in many situations. Further research is required to elucidate its mechanisms of action and efficacy and to optimize cannabis preparations and doses for specific populations affected by cancer.
Introduction
Cancer and cancer chemotherapy cause nausea and vomiting, pain, neuropathy, depression, sleep disorders, and other debilitating symptoms. 1 These symptoms often develop during treatment and can persist after cessation of chemotherapy, severely impacting long-term quality of life. 2 With more survivors than ever, and survivors living longer lives, 3 it is important to address these symptoms to maximize survivors’ quality of life.
Despite limited randomized clinical trials, cannabis shows promise to improve many symptoms of cancer and its treatments.4,5 Social acceptance is also greatly increasing its use, despite lack of scientific evidence of safety and efficacy. In fact, in one community oncology clinic, 18.3% of patients with cancer reported using cannabis in 2017. 6 In a Canadian study conducted in 2017, before cannabis was legalized in that country, 18% of patients with cancer used cannabis, often to relieve cancer-related pain, nausea, or other cancer symptoms. 7 Unfortunately, although 80% of clinicians are discussing cannabis (i.e., medical marijuana) with patients, only 30% feel adequately informed to make recommendations about its use. 8 It is crucial that scientific research on cannabis be accelerated to match patient demand. Only then will clinicians and patients have reliable safety and efficacy data to inform decisions that integrate information on patient symptoms, type of cannabis, delivery system, patient preference, dose, duration, and side-effects/adverse events.
This review describes how cannabis might modulate the most common and debilitating symptoms of cancer and its treatments in the context of cancer treatment, palliative care, and survivorship. While other reviews have examined the literature on medical cannabis related to cancer care (e.g., 4,5,9–12), we further explore cannabis in animal models and in other medical fields and cautiously extrapolate these findings to supportive and palliative care in cancer in humans. We urge patients and clinicians to recognize the potential drawbacks and dangers of cannabis, including allergic reactions, addiction/dependence, side effects, and interference with other medications. Nevertheless, we conclude that cannabis, in combination with guideline-based treatment regimens, tends to exhibit potential benefits that outweigh its risks.
Methods
We performed a review of the literature involving cannabis, cannabinoids, and marijuana for high priority symptoms of cancer and its treatments as identified by the National Cancer Institute Symptom Management and Quality of Life Steering Committee 13 : cognitive impairment, neurotoxicity, cardiovascular toxicity, fatigue, cancer-specific pain, sleep disorders, bone health toxicity, metabolic toxicity, and psychological distress. Chemotherapy-induced nausea and vomiting, loss of appetite/anorexia, and gastrointestinal (GI) distress were also included due to the historical use of cannabis for these cancer- and treatment-related ailments. The first author (A.S.K.) searched the PubMed database from the inception of the database to November 8, 2018. The results of this search are shown in Supplemental Table 1. Reference lists of recent review articles were also evaluated to identify additional trials. Only articles published in English were assessed, and results of clinical trials were prioritized.
Brief overview of the biological mechanisms of cannabis
Cannabis is a generic term used to describe plants from the genus Cannabis, as well as bioactive preparations thereof. Cannabis plants contain more than 400 secondary metabolites, many of which exert bioactive effects. Of these metabolites, two have been identified as the most bioactive: Δ9-tetrahydrocannabinol (THC) and cannabidiol (CBD). Further, cannabis contains terpenoids, which are responsible for the aroma of cannabis, and flavonoids, which are believed to be responsible for the health benefits of many vegetables, spices, and other foods. 14 It appears that many of the other metabolites of cannabis can have antagonist, additive, or synergistic properties with THC in regard to some, but not all, of its effects.14,15 The concentrations and ratios of the various phytocannabinoids (cannabinoids specific to the cannabis plant) differ depending on plant strain and growing conditions.16,17
Endogenous cannabinoids (‘endocannabinoids,’ or cannabinoids made in the body) comprise bioactive lipids, most derived from arachidonic acid. These include arachidonoyl-ethanolamide (AEA; previously known as anandamide) and 2-arachidonoylglycerol (2-AG), among others. 18 There are two major cannabinoid receptors: cannabinoid receptor type 1 (CB1) and cannabinoid receptor type 2 (CB2). Cannabinoid receptors are expressed in virtually all regions of the brain and in the peripheral nervous system, with notable density in the hippocampus, amygdala, thalamus, and association regions of the cortex (e.g., cingulate).19,20 These regions are part of interoceptive brain circuitry, which processes bodily sensations and supports mood, depression, anxiety, memory, pain, and other psychological functions (see review by Kleckner and colleagues 21 ). In other words, interoceptive brain circuitry helps translate sensation (the signal transduction from the periphery) to perception (the symptoms that patients experience and report). 22 Binding of a cannabinoid to one of these receptors leads to G-protein activation, which affects various cellular functions depending on the type of cell (Figure 1). Many of the metabolites of these endocannabinoids activate a number of other receptors that are involved in inflammation, thereby implicating endocannabinoids as inflammatory regulators. 18 Further, CB1 receptors are present on the mitochondrial membrane, where activation can directly control cellular respiration, energy production, and generation of reactive oxygen species.23,24

Mechanisms through which cannabinoids can affect cancer- and chemotherapy-related symptoms. ❶ Binding to a cannabinoid receptor. ❷ THC and other lipophilic cannabinoids can diffuse freely through the cellular membrane, where they are then transported intracellularly by fatty acid binding proteins. 25 Lipophilic cannabinoids also freely diffuse into the membranes of intracellular vesicles. 26 ❸Cannabinoids are hydrolyzed into various metabolites that can bind to CB1 and other receptors involved in immune function, cellular signaling, etc.
Phytocannabinoids are cannabinoids that are present in the cannabis plant. The major phytocannabinoid in cannabis is THC, which is responsible for approximately 20% of the total content of the plant (by weight), 27 and 20% of the bioactivity of cannabis extracts in various assays. 17 THC directly binds CB1 and CB2. CBD is the second most studied phytocannabinoid; it has a low affinity for the CB1 and CB2 receptors per se, but it blocks the fatty-acid binding protein that transports endocannabinoids to be hydrolyzed, hence prolonging the activation of the CB1 receptor.5,25 It also modulates other receptors such as the 5-hydroxytryptamine (5-HT1A) serotonin receptor, the peroxisome proliferator-activated receptor γ (PPAR-γ), and others. 28 CBD is thought to have a greater potential value for medicinal purposes than THC, mostly due to its lack of psychoactive properties. 29 Therefore, pharmaceutical companies and medical marijuana growers produce medicinal preparations with specific THC:CBD ratios (e.g., 1:1, 1:20). 30 There are now synthetic preparations of THC (dronabinol), CBD, THC analogs (e.g., nabilone), and CBD derivatives, though the characterization of the therapeutic value of these compounds is in its infancy. 31 Of note, the US Food and Drug Administration approved the first highly purified plant-derived compound from cannabis, CBD as Epidiolex®, in 2018, and many other preparations will likely follow.
One of the major mechanisms by which cannabinoids can elicit a therapeutic response is via the immune response. Indeed, cancer and its treatments lead to systemic elevated inflammation responsible for chemotherapy-induced symptoms including: cognitive deficiencies such as problems with attention, memory, and executive functioning; fatigue and motivational deficit; and neuropathy.2,32–36 Endocannabinoids are produced as part of the innate immune response, and monocytes, B cells, T cells, and other immune cells all have cannabinoid receptors. 37 Indeed, many cannabinoids have an arachidonic acid moiety, which is the precursor of many pro- and anti-inflammatory molecules. 2-AG is an important metabolic intermediate in lipid synthesis and serves as a major source of arachidonic acid in prostaglandin synthesis. 15 Eicosanoids are produced from arachidonic acid, and they function to both initiate and reduce inflammation. Whereas cyclooxygenase-2 inhibitors suppress the synthesis of eicosanoids to attenuate the ramping up of inflammatory processes, cannabinoids increase the production of eicosanoids to slow it down. 16 Several preclinical studies have shown that cannabis can inhibit the production of TNF and other cytokines in several different models and by several different mechanisms, not all of which involve cannabinoid-specific receptors.37–39
Cannabis and common symptoms of cancer and its treatments
Cannabis use is a promising approach to symptom management in the context of cancer and its treatments because of its multifaceted bioactivities in multiple tissues. 40 In this section, we discuss several common symptoms and side effects of cancer and its treatments with a summary of preclinical and clinical studies of cannabis in cancer patients and other clinical populations (Table 1).
Cannabis for cancer- and cancer treatment-related toxicities: a summary.

THC, Δ9-tetrahydrocannabinol.
Nausea and vomiting
Chemotherapy-induced nausea and vomiting (CINV) is highly prevalent, with many common chemotherapy regimens classified as ‘highly-‘ or ‘moderately’ emetogenic. In general, modern anti-emetic regimens are extremely effective at preventing emesis, but these regimens are much less effective at controlling nausea.41,42 In fact, control of nausea remains poor, with 40–70% of patients reporting nausea while receiving highly or moderately emetogenic chemotherapy.43–51 However, little attention has been directed to the concept of chemotherapy-induced nausea as a discrete symptom, despite recognition that nausea and vomiting are two related but separate entities.52,53 Nausea and vomiting symptoms also vary over the course of chemotherapy via different mechanisms, and therefore different interventions are needed as treatment progresses. 53
The mechanism by which chemotherapeutic agents induce nausea and vomiting is fairly well understood. Chemotherapeutic agents promote excess serotonin release from enterochromaffin cells that line the GI tract, and elevated concentrations of serotonin bind to 5-hydroxytryptamine 3 (5-HT3) receptors on nearby vagal nerve afferents, which send information of excess chemicals to the brain and directly promote emesis. Further, toxicity to enterochromaffin cells can cause cell death and chronic elevation of serotonin and other secreted substances, which in turn sensitize the vagal nerve and cause delayed nausea and vomiting (reviewed by Janelsins and colleagues 34 ). The most widely used classes of anti-emetics for cancer patients are 5-HT3 receptor antagonists, and cannabinoids also directly inhibit these receptors. 54 Specifically, it is thought that CBD may act as a modulator of the 5-HT3 receptor and as an indirect agonist on the 5-HT1A autoreceptors, which ultimately reduces the availability of serotonin (5-HT3). 55
Increasing preclinical evidence suggests that the endocannabinoid system plays a role in the regulation of both nausea and vomiting. 56 Cannabinoid receptors CB1 and CB2, located within the brainstem and the GI tract, are associated with emetogenic control in rat, mouse, ferret, and shrew.57–59 For example, THC reduced the emetic effects of cisplatin chemotherapy induced in the least shrew. 59 In addition, CBD-induced suppression of vomiting was reversed by systemic pretreatment with a 5-HT1A antagonist, 59 suggesting that the anti-emetic effect of CBD may be mediated by activation of 5-HT autoreceptors. In a parallel mechanism, substance P may be a key neurotransmitter in chemotherapy-induced nausea and vomiting,60,61 and cannabinoids modulated release of substance P in several preclinical studies.62–64 For example, THC was shown to increase substance P release in adult rat brain. 64 In addition, CB1 receptor stimulation promoted its release in adult mouse spinal cord 62 and in cultured rat dorsal root ganglion cells. 63 As substance P tends to be a key first responder to noxious stimuli (i.e. chemotherapy), modulation of this neuropeptide with concomitant chemotherapy and medicinal marijuana could help alleviate acute nausea and vomiting.
Patient claims that cannabis relieves chemotherapy-induced nausea and vomiting are widely recognized, and increasing clinical evidence supports these anecdotes.58,65–68 For example, in 2001, Musty and colleagues published a review of previously unpublished technical reports from six states (e.g., Tennessee 69 and New Mexico 70 ) that conducted trials of smoked cannabis. They reported that 70–100% of subjects experienced relief from nausea and vomiting, while those taking oral THC experienced a 76–88% reduction. 66 In one of the only studies performed in the 21st century, Duran and colleagues recruited 16 patients on chemotherapy who experienced chemotherapy-induced nausea or vomiting despite standard anti-emetic treatment. 71 Patients were randomized to either an oromucosal cannabis-based spray containing THC and CBD or a placebo. Those in the treatment group experienced less nausea and vomiting than those on the placebo. In addition, in 2007, Meiri and colleagues randomized patients receiving moderately to highly emetogenic chemotherapy (n = 64) to dronabinol (synthetic THC), ondansetron, both, or a placebo in addition to standard anti-emetic treatments. 72 Dronabinol performed equal to ondansetron to prevent chemotherapy-induced nausea and vomiting, with no additive effects on the combination, and all treatment groups were more effective than the placebo. Combining these data with data from the 1970s and 1980s, a 2017 report concluded that there is conclusive evidence that oral cannabinoids are effective in the treatment of chemotherapy-induced nausea and vomiting. 73
A nonoral route (e.g., inhalation, intranasal) of drug delivery is particularly important for treatment of nausea and vomiting so the drug can reliably be delivered to the target site and not emitted itself. 53 Further, intravenous drugs are not optimal for delivery at home, and delayed nausea, which is more common than acute nausea, develops >24 h after infusion and commonly occurs in patients receiving cisplatin, carboplatin, cyclophosphamide, or doxorubicin. 34 New opportunities in smoking technology are becoming available such as e-cigarettes and vaporizing devices (see Table 2).
The appropriate delivery system allows bioactive compounds to be supplied to target tissues at an appropriate dose and rate.

THC, Δ9-tetrahydrocannabinol; CBD, cannabidiol.
There are some limitations and gaps in the literature before cannabis-derived therapeutics can be prescribed as a first-line treatment for nausea and vomiting. For example, most of the studies evaluating the efficacy of cannabinoids were performed in the 1980s, and have not yet been compared with modern anti-emetic regimens. 74 In addition, paradoxically, an increasingly recognized symptom of cannabis use is cannabinoid hyperemesis syndrome, which presents as intractable cycles of vomiting. 75 This syndrome tends to be associated with frequent, high doses of recreational cannabis. The etiology of cannabinoid hyperemesis syndrome is largely unknown, but is expected to involve the endocannabinoid system. 75
Anorexia and loss of appetite
Decreased appetite and anorexia are ranked among the most troublesome side effects of cancer and its treatment; more than half of patients with advanced cancer experience a lack of appetite or weight loss.78–80 Appetite-stimulating drugs that are currently used include megestrol acetate (similar to the female hormone progesterone), metoclopramide (a gut mobility stimulator), steroids including prednisone or dexamethasone, and dronabinol (synthetic THC). All of these drugs except dronabinol are recommended for short-term use only due to potential side effects. Further, radiation therapy in head and neck cancer patients includes irradiation of the mouth and salivary glands, and many patients suffer from dysgeusia (distortion of taste), anatomical intraoral defects, or oral mucosal damage, 81 which can lead to loss of appetite and body mass.
Endocannabinoids regulate eating behavior via several biochemical pathways in the brain and the periphery: the hypothalamus and hindbrain (integrative functions), the limbic system (for hedonic evaluation of foods), the intestinal tract, and adipose tissue. 82 These pathways modulate peptides involved in appetite regulation, including ghrelin, leptin, and melanocortins. 82 Endocannabinoids AEA and 2-AG stimulate food intake in rats,83–85 and SR141716, a CB1 antagonist, attenuated those increases in rats 84 and induced appetite suppression in mice. 86 Medical cannabis and THC, specifically, are known to boost appetite in humans and laboratory animals.85,87–92
Overall, studies assessing the effects of cannabis or phytocannabinoids on appetite in cancer patients have shown benefits, although there appears to be a placebo effect, and a 2017 report found insufficient evidence to support or refute its use. 73 In one study in 469 patients with advanced cancer and documented weight loss or reduced food intake, 93 and another in 243 patients with advanced cancer and cancer-related anorexia–cachexia syndrome (CACS), 94 appetite increased in all groups including comparison groups treated with dronabinol (synthetic THC), megestrol acetate, 93 cannabis extract, and placebo, 94 suggesting that cannabis-derived products are no better than a placebo. One smaller study (n = 46) of dronabinol in advanced cancer patients demonstrated enhanced taste of food compared with placebo. 95 Appetite also improved in several other prospective or randomized studies in patients with cancer, though caloric intake was not significantly greater.92,95
Much of the clinical research on cannabis and appetite has been performed in patients with human immunodeficiency virus (HIV), who often suffer from decreased appetite and weight loss. In three independent randomized, placebo-controlled trials, smoked cannabis and oral THC increased caloric intake and weight gain in patients with HIV compared with placebo, especially in patients who were underweight.96–98 Moreover, in 15 patients with Alzheimer’s disease who were refusing food, dronabinol (synthetic THC) increased body weight compared with placebo. 99
The limitations of this research thus far is that there has not yet been a randomized controlled trial to systematically evaluate the efficacy of cannabis-derived products on both appetite and weight gain as primary endpoints in patients with cancer. Future studies to this end should consider the composition of the diet (e.g., macronutrient composition) and the weight that has been gained (e.g., fat versus lean mass). Future studies will need to have appropriate control groups, including current remedies and a placebo.
Pain
More than half of all cancer patients experience moderate to severe pain. 100 Management of cancer pain has improved, generally via optimization of nonpharmaceutical practices such as exercise,101–104 and cognitive behavioral therapy.105,106 However, insurance companies often do not reimburse these practices, leaving opiates as the first-line of treatment for cancer-associated pain. 107 With that said, alternatives for opiates are sought by patients because: opiates do not provide an adequate analgesic effect for some patients; the required opiate dose may lead to debilitating side effects such as constipation; there is a potential to overdose on opiates; finding the individualized, appropriate dose of opiates requires titration, which can take days or weeks; and the potential for dependence on opiates is extremely high, and patients with a high likelihood for survival from the cancer or an inclination toward addiction should avoid frequent opiate use.
The etiology of cancer-related pain is complex and not well understood. Its presentation stems from interaction between the cancer and peripheral sensory neurons (i.e., nociceptors) as well as morphological, physiological, and immunological changes that cause sensitization of the peripheral and central nervous system (CNS) as well as increases in spontaneous activity. 108 These effects vary drastically depending on the type and location of the cancer. 108 There is evidence that cannabis can affect both sensation (signal transduction in the nervous system) and perception (the experience of symptoms); therefore, studies at the biochemical, neurological, psychological, and social levels are all important. 109 Nociceptors have CB1 receptors, allowing cannabinoids to have a direct analgesic effect by modulating nociceptor activity in the periphery (i.e., sensation). CB1 and CB2 receptors throughout the nervous and immune systems allow for parallel mechanisms of cannabinoids to modulate pain sensation. In addition, there is evidence that cannabinoids potentiate the analgesic effects of opioids, thus allowing for dose-reductions of opioids. 110
Preclinical studies have demonstrated that cannabinoid receptor agonists can reduce cancer-related pain behavior, though it is unclear through which receptors the relationship is mediated. For example, WIN55,212-2, an agonist of the CB1 and CB2 cannabinoid receptors, attenuated cancer-related pain behavior in mice.111,112 In mice, a CB2-selective agonist reduced cancer-related pain behavior. 112 However, fully blocking either of these receptors did not prevent WIN55,212-2 from having analgesic effects. 111
Anecdotal evidence suggests that recreational cannabis can alleviate cancer-related pain, 113 and two recent reviews on the effects of cannabis on cancer-related pain concluded that cannabis-derived compounds can alleviate chronic and neuropathic pain in advanced cancer patients.113,114 Since these two reviews were published, in a 2018 prospective analysis, 92 Bar-Lev Schleider and colleagues showed that 52.9% of patients with cancer reported a pain level of 8–10 on a 10-point scale at baseline, while only 4.6% reported that intensity of pain after 6 months of cannabis treatment. Because there was no control group, it is not possible to know if cannabis per se reduced pain, or if time or other factors were involved. However, the authors concluded that cannabis appears to be a safe and effective palliative treatment for patients with cancer pain. Fallen and colleagues also conducted two randomized controlled trials with patients with cancer-related pain who were not getting adequate analgesia from opioids. 115 Compared with the control arm, those in the THC:CBD group did not experience relief from pain, though a subgroup analysis showed that participants from the United States did experience pain relief.
A 2017 analysis of five systematic reviews and several more recent trials concluded that there is substantial evidence that cannabis is an effective treatment for chronic pain in adults (not necessarily cancer patients).73,116 Indeed, the analgesic effects of cannabis tend to be the most sought-after properties of medicinal cannabis among all patients (not necessarily cancer patients) who elect to use it.117–119 With that said, the authors of a 2015 systematic review concluded that, although effective, currently available cannabis-based medications reduce pain only to a modest extent, similar to other drugs on the market. 116 A review by Hill in 2015 on cannabis for the treatment of chronic pain concluded that evidence is beginning to accumulate that cannabis/cannabinoids are promising for the treatment of chronic pain, neuropathic pain, and pain from multiple sclerosis. 30 Amato and colleagues published a review demonstrating that three out of four studies showed benefits of cannabis compared with placebo in reducing pain in patients with multiple sclerosis, chronic pain, dementia, Tourette syndrome, and cancer. 65 Further, a prospective single-arm study published in 2018 followed 338 medicinal cannabis users with various chronic pain conditions. Pain intensity decreased significantly over the course of 12 months. 120
Cannabis may present itself as a promising alternative to opioids for cancer-related pain in the future, though more data are needed. Indeed, there is anatomic and physiologic evidence of an interaction between cannabinoids and opioid receptors. 121 Cannabinoids may directly and effectively target the opioid system and also work with opioids to modulate both cannabinoid and opioid pathways in tandem.82,121–124 In a retrospective study of 244 medicinal cannabis users with chronic pain, cannabis was associated with a 64% decrease in opiate use, fewer side effects of all drugs, and improved quality of life. 125 In another survey in 2897 medicinal cannabis users, 97% reported that they were able to reduce their dose of opiates after initiation of cannabis use. 126 However, others studies, such as a three-arm randomized controlled trial evaluating THC:CBD versus THC versus placebo for cancer-related pain, have not shown a reduction in opiate use; dosing of opiates did not change significantly over the 2-week study for any arm. 127 System-wide data corroborate reports of the use of cannabis for pain or as an analgesic potentiator: physicians in states where medicinal cannabis was legalized prescribe more than 10% fewer daily doses of pain medication, 128 and, particularly promisingly, legalization of medicinal cannabis is associated with a reduction in opioid overdoses. 129 However, a 2017 report by the National Academy of Sciences concluded that, at this point, there is not enough evidence to recommend or discourage cannabinoids in the treatment for addiction. 73
There are several limitations to the current body of literature related to pain. For example, both cancer and pain are heterogeneous manifestations with complex features that change during disease progression and treatment, making pain difficult to target. As such, treatments that work for radiation-induced pelvic pain might not work for chemotherapy-induced neuropathic pain. In addition, studies that have been performed in the United States using cannabis plants all used product from the National Institute on Drug Abuse, which differs in bioactive concentration from what is available in dispensaries, 130 and likely interacts differently with opiates and other pain medications. The placebo effect appears to be particularly strong, which is beneficial to patients in general, but makes it more difficult to study the biochemical and physiological analgesic effects of cannabis-based therapies.
Chemotherapy-induced peripheral neuropathy
Chemotherapy-induced peripheral neuropathy (CIPN) is a serious side effect and dose-limiting toxicity of several commonly used chemotherapeutic agents, and can lead to dosage reductions or cessation of therapy. The symptoms of CIPN primarily include abnormal sensory discrimination of touch, vibration, temperature variations, and pain. 131 A recent meta-analysis found a CIPN prevalence of 68.1% within the first month of chemotherapy, 60% within 3 months, and 30% at 6 months or later. 132 CIPN occurs most frequently with platinum-based chemotherapeutic agents (i.e., oxaliplatin and cisplatin) and taxane-based chemotherapeutic agents (i.e., paclitaxel and docetaxel). It is widely believed that cisplatin-induced neuropathy is irreversible, while taxane-induced neuropathy generally resolves but can persist for years in up to 30% of patients. 133 CIPN is notoriously difficult to treat, and treatment options remain limited, as antiepileptic or antidepressant agents used to treat other neuropathic pain conditions have not been successful in cancer patients.134–136
The exact mechanism(s) of CIPN and mechanisms by which cannabis might reduce CIPN and its symptoms are unknown, although recent preclinical studies have elucidated potential pathways. In one such study, a CB1/CB2 agonist reduced paclitaxel-induced thermal hyperalgesia and tactile allodynia (proxies for neuropathy) in rats. This effect was reversed by the use of a CB1 antagonist, suggesting a role for CB1 receptor in CIPN. 137 In addition, another preclinical study found the same CB1/CB2 agonist suppressed vincristine-induced mechanical allodynia (a proxy for neuropathy) through activation of both CB1 and CB2 receptors. 138 Moreover, activation of CB2 receptors partially attenuated vincristine-induced neuropathy 138 and fully attenuated paclitaxel-induced mechanical allodynia139,140 and cold allodynia 140 in rats. Other researchers have presented evidence that CBD plays a role in reducing neuropathic pain. In one study, researchers induced neuropathy with paclitaxel, and found that subsequent administration with CBD prevented the development of cold and mechanical allodynia, with no latent neuropathy emerging after the cessation of CBD treatment. 141 In a follow-up study, lower doses of CBD were administered to rats prior to inducing neuropathy with paclitaxel. 142 Administration of CBD prevented the development of paclitaxel-induced mechanical sensitivity. This effect was reversed by administration of the 5-HT(1A) antagonist, but not with a CB1 or CB2 antagonist. Based on these results, it is possible cannabis may reduce both chemotherapy-induced nausea and vomiting and CIPN through a shared mechanism: 5-HT.
Several placebo-controlled clinical trials have examined the effect of smoked or vaporized cannabis for neuropathic pain of various etiologies, though none yet for patients with cancer or CIPN. Patients suffering from chronic neuropathic pain of various etiologies, including HIV, trauma/surgery, and diabetes, reported that smoked cannabis significantly decreased central and peripheral neuropathic pain compared with placebo.143–148 In addition, studies in mouse and rat models have demonstrated that THC and/or CBD reduce the quantity of circulating pro-inflammatory cytokines and alleviate neuropathic symptoms associated with constriction injury 149 and chemotherapy.137–142,150
CIPN is a particularly difficult symptom to treat due to its elusive etiology and largely unpredictable pattern of presentation. Currently, it is unclear if the observed effects of cannabis are due to its action on the peripheral nerves by reducing damage, on the CNS by reducing or attenuating hypersensitization, both, or other mechanisms. A variety of measures are needed to answer these questions, including both nerve conduction and patient report. It is also not yet clear if primary prevention or treatment after presentation will be the most impactful.
GI distress
Chemotherapy-induced GI distress (e.g., bloating, cramps, flatulence, diarrhea, abdominal pain) is a common and understudied toxicity of cancer treatment. In fact, up to 80% of patients receiving chemotherapy report diarrhea, and approximately 16% experience constipation (up to 87% of patients with advanced cancer).151,152 GI distress is associated with worsening quality of life, and also contributes to malnutrition, dehydration, fatigue, anxiety, depression, and other symptoms.151,153 These symptoms can be so debilitating that 22% of patients reduce their life-saving chemotherapy doses, 28% delay treatments, and 15% terminate chemotherapy completely. GI distress and diarrhea are strongly correlated with chemotherapy dose, as well as certain chemotherapy regimens such as 5-fluorouracil and irinotecan. 151 In fact, the majority of patients on these regimens experience diarrhea and more than 30% of patients report severe (grade 3 or 4) diarrhea. 151 Furthermore, symptoms seldom resolve at the completion of chemotherapy, and GI distress persists for 10 years in some patients. 151
The mechanisms by which chemotherapy induces diarrhea are largely elusive, but cancer- and chemotherapy-induced increases in inflammatory cytokines are largely implicated. 151 In addition, microbiota are implicated in chemotherapy-induced GI distress, but it is not clear if inflammation causes disruption of microbiota, or vice versa. 154 Cannabis-derived treatments could moderate GI symptoms via inflammatory pathways, and also more directly via the endocannabinoid system, which contributes to regulation of peristalsis and gut motility both at the site of the tissue and centrally via the brain-gut axis.155–157 Cannabis tends to slow GI motility, 157 but also relax the bowels, allowing it to have potential effects for both diarrhea and constipation.
Dinitrobenzene sulfonic acid-induced colitis is a standard mouse model for studying inflammatory bowel disease. Pagano and colleagues examined the effects of cannabis on mucosal inflammation in this model, as well as hypermotility in a croton oil-induced mouse model of intestinal hypermotility. 155 They used four experimental conditions: high-CBD Cannabis sativa extract or pure CBD administered intraperitoneally or orally via gavage. The extract reduced the extent of pathologic damage and reduced hypermotility; pure CBD did not alleviate inflammation but reduced hypermotility. Borrelli and colleagues also explored the effects of CBD on symptoms of dinitrobenzene sulfonic acid-induced colitis in a mouse model; CBD reduced colon injury and inflammation. 158
No data are available on the efficacy for cannabis-derived products to prevent or treat cancer- or chemotherapy-induced gastrointestinal distress in humans, but cannabis has been used in traditional medicine for centuries to alleviate both diarrhea and constipation, 159 and there have been quite a few population-based surveys examining patterns of cannabis use among patients with irritable bowel syndrome or inflammatory bowel disease. Participants with inflammatory bowel disease, ulcerative colitis, and Crohn’s disease are more likely to have used cannabis or hashish compared with individuals without the disease specifically to help alleviate their symptoms (e.g., abdominal pain, diarrhea, loss of appetite).160–164 Interestingly, in Massachusetts, Merker and colleagues showed that recreational and medicinal use of cannabis among approximately 300 patients with inflammatory bowel disease nearly doubled from 2012, before medical cannabis was legalized, to 2017, after it was legalized. 165 Despite the empirical benefits of cannabis for abdominal pain and other forms of GI distress, 161 there have not been many randomized controlled trials evaluating cannabis for GI distress; a review of the literature by Ahmed and colleagues and the National Academy of Sciences could not definitively conclude that cannabis was able to mitigate symptoms of inflammatory bowel disease.73,166
This body of literature is very much in its infancy and more clinical trials are needed. Further research should explore the effects of cannabis on various aspects of gut health in patients with cancer, including inflammation and the microbiome, especially in regard to chemotherapy insults. GI distress is often a side effect of treatment, and it is often difficult to accurately attribute symptoms to the cancer or a drug (e.g., constipation is a common side effects of opiates). 151 Owing to the direct delivery, this is one symptom where ingestion of cannabis products might be more reliable, predictable, and beneficial than inhalation, but more studies are needed determine the efficacy of edibles for GI distress.
Cognitive complaints
Cancer-related cognitive impairment is one of the most common symptoms of patients undergoing cancer treatment for non-CNS disease. Indeed, up to 30% of patients experience cancer-related cognitive impairment even before treatment, and this number increases to 75% during treatment. 32 Furthermore, cognitive impairment affects cancer patients across multiple cognitive domains (e.g., memory, executive function) for at least 6 months postchemotherapy and some experience longer term cognitive problems. 167 Cognition relies on the function of many interrelated neural systems, with complex processes.24,32 The impact of cancer and cancer treatments may cause direct or indirect effects on CNS function. 168 Proposed biologic mechanisms include inflammation, neuroinflammation, mitochondrial dysfunction, neural cell genesis disruption, and disruption of neural network connectivity (e.g., synaptic connections).32,169–171 Cognitive behavioral therapy, cognitive brain training, and physical activity have shown promise for managing cancer- and chemotherapy-related cognitive impairment.32,172 However, these approaches come with barriers, including time, availability, preference, and physical abilities. Also, modafinil and methylphenidate have shown promise, but further research is needed to confirm their efficacy.172–176
Many preclinical rodent models, including wild type as well as those for neurodegenerative diseases (e.g., Alzheimer’s disease), neuro-inflammatory disorders (e.g., meningitis), and others, 177 have been used to assess the effects of cannabis and cannabinoids on cognition, but there have not yet been any studies in cancer or chemotherapy-based models. It is clear that the endocannabinoid system is involved in cognitive function. 178 In general, moderate-to-large doses of THC and other cannabinoid receptor agonists appear to lead to acute impairment in memory, attention, and working memory in animal models, but there is evidence that these effects are merely transient.178,179 On the other hand, CBD could be beneficial to cognitive function.177,178 In addition, the endocannabinoid system is significantly affected by aging, and preclinical evidence shows that cannabinoids can reverse age-related cognitive impairment.76,180 For example, CBD reversed the neurodegenerative effects of iron in a rat model 181 and attenuated brain ischemia-induced cognitive deficits in a mouse model. 182 In addition, in older mice, a chronic low dose of THC restored learning 76 and a single low dose of THC improved spatial learning and memory. 180 Results have been mixed on the effects of cannabis on Alzheimer’s symptoms, suggesting interactions between cannabis and genetic factors; for example, CBD and/or THC alleviated Alzheimer’s-like symptoms in mice genetically predisposed to the disease, although the cannabinoids impaired cognition in wild type mice.177,183–185 Myers and colleagues studied the effects of cannabinoids on cognition in wild type mice. 186 They saw that THC and/or a CB1/CB2 receptor full agonist led to cognitive impairment in a maze task (assessing spatial memory) but not in a conditional discrimination task (assessing learning); CBD had fewer effects on cognition. Similarly, Murphy and colleagues showed that THC impaired object/working memory in adult mice; cotreatment with CBD prevented these impairments, and CBD alone led to no impairment.76,187 A 2017 systematic review of 18 studies in mice, rats, or Rhesus monkeys concluded that preclinical models point to CBD improving cognitive function in regard to learning and memory. 177
In humans, there have not yet been any studies using cannabis that test cognitive function as a primary outcome in patients with cancer. In general, acute cognitive impairment has been broadly cited as a side effect of cannabis use, including memory loss and reduced ability to concentrate and learn.188,189 However, there is very little research on whether the acute cognitive side effects are generally tolerable to patients with cancer, and no research on whether cannabis or cannabis-derived products can treat late-effects of cancer and its treatments (especially chemotherapy). Bar-Sela and colleagues followed cancer patients who had obtained a medical marijuana license during their cancer treatment, and, overall, the only negative effect of cannabis they observed was that patients’ memories declined with 6–8 weeks of cannabis use. 190 However, these researchers performed a follow-up prospective study among patients with advanced cancer undergoing chemotherapy and demonstrated improvement in executive function among patients who opted to use cannabis treatment over a 3-month period. 191 There have not yet been any studies on the effects of CBD to treat chemotherapy-induced cognitive impairment, though a 2017 systematic review of nine clinical trials (participants included healthy volunteers, patients with multiple sclerosis, patient with schizophrenia, and others) demonstrated that CBD tends to have no effect or a benefit in memory, attention, executive function, processing speed, and other measures of cognition. 177 Also, cannabis has shown promise in treating Alzheimer’s disease, a disorder associated with progressive memory loss. 184
Epidemiological research shows an association between chronic cannabis use and long-term, more permanent, impairments, though aging and educational level are major confounding factors not adequately considered.192,193 Similarly, chronic cannabis use, especially in adolescents, leads to a decline in neurophysiological function (reviewed by Broyd and colleagues 194 ). In cross-sectional studies, recreational cannabis is associated with defects in brain structure, especially in adolescents. 195 Thus, clinicians should use greater caution in discussions of cannabis with adolescent patients with cancer than with adult patients.
All in all, there could be unappreciated benefits of specific types of cannabinoids (especially CBD) for cognitive function in specific populations of patients with cancer, but the literature is currently very limited. Indeed, cannabis can be anti-inflammatory, 18 and could therefore theoretically attenuate and inflammatory-mediated cognitive impairment.32,37 Controlled preclinical studies are needed to optimize the dose and type of cannabis/cannabinoids to maximize the beneficial effects seen in preliminary data while minimizing the acute toxicities. More research should also explore individual genotypes 185 that could exacerbate or benefit cannabis-induced effects on cognition.
Psychological distress
Anxiety and depression are common reactions to the cancer and treatment experience, are often linked in the construct of ‘psychological distress,’ and are considered a sixth vital sign in cancer care.196–198 While a majority of patients experience some level of anxiety and depression after a cancer diagnosis, about one-third of patients experience severe and unremitting psychological distress that requires clinical treatment. 199 Anxiety can manifest as worry, difficulty concentrating, poor sleep quality, recurrent panic attacks, and other symptoms, while signs of depression include listlessness, changes in appetite and energy levels, and suicidal ideation. Even after treatment, the prevalence of depression and anxiety are greater in cancer survivors than in the general population.196,197 Current treatments include support groups to discuss feelings, cognitive behavioral therapy to learn coping strategies, exercise, and medication (often in conjunction with therapy).104,200
The biological underpinnings of both anxiety and depression have not been elucidated, 197 but the endocannabinoid system is involved in mood regulation201,202 and cannabis-derived treatments could theoretically modulate the development or progression of mood disorders. There have not been any preclinical studies evaluating cannabis-derived treatments for cancer- or treatment-related anxiety or depression, but there is promising evidence for CBD as a treatment for generalized anxiety disorder in rodents (review: 203 ) For example, CBD alleviated anxiety-like behaviors in mice subjected to chronic unpredictable stress.204,205 In addition, THC increased anxiolytic-like effects while CBD prevented anxiolytic effects in response to foot-shock stress in rats. 206
In humans, cannabis has exhibited a broad therapeutic potential across a range of psychiatric disorders. 203 Anxiety and depression, along with pain, are the top three reasons why people in the general population use cannabidiol, 207 and anxiety and depression are common symptoms for which patients with cancer seek medical cannabis.119,208 No studies to our knowledge have assessed cannabis for mitigating anxiety or depression in cancer patients as a primary aim, though there have been several longitudinal studies following patients who elected to use medicinal cannabis during their cancer treatment.208,209 Patients in these studies tended to experience alleviation of their symptoms, though anxiety was reported as a side effect in some patients 209 and as a withdrawal symptom in some patients upon ceasing use. 208
The noncancer literature is mixed as to whether cannabis is associated with increased or decreased depression and anxiety. Randomized clinical trials among clinical populations with exploratory measures of anxiety or depression suggest reduced or no effect compared with placebo for anxiety and depression among patients with cancer, 209 Alzheimer’s disease, 99 or diabetes. 210 Systematic reviews in healthy populations from 2003 211 and 2018, 212 a large prospective study in 2007, 213 and a meta-analysis in 2014 214 suggested that heavy cannabis use is associated with increased anxiety and depression symptoms among some users, although all studies discussed confounding factors and cautioned against making causal inferences. A recent review by Twomey, 215 however, concluded that cannabis poses no more than a minor increased risk for anxiety, citing publication bias and low-quality studies for contrary conclusions, especially in studies published before approximately 2007. Indeed, the vast majority of studies to date have evaluated associations between recreational cannabis (ab)use and anxiety and depression, where it is very likely that participants’ symptoms and environment encourage them to use cannabis for self-treatment; therefore, these studies are limited in the generalizability to patients with cancer. Indeed, several surveys indicate that cannabis alleviates symptoms of depression in a variety of recreational and medical users.208,216 These discrepancies might stem from THC promoting anxiety while CBD alleviates it, or a much more complex interaction of bioactive compounds might be at play.217–219 Of note, a CB1 receptor antagonist, SR 141716A or rimonabant, was available in Europe as a treatment for obesity from 2006 to 2008; 220 it was then removed worldwide because of high levels of anxiety, nightmares, depression, and increased suicidality.82,221,222 These data suggest that CB1 activity reduces anxiety and promotes positive affect.
Overall, the literature on use of cannabis for anxiety and depression is currently limited in that much of the data are epidemiological, both in clinical populations and in healthy individuals, and there are many confounding factors. In addition, depression and anxiety are both normal and common responses to a cancer diagnosis, and therefore diagnosing clinical levels of anxiety and depression and studying treatments to address these levels in the context of cancer is difficult. 197 More studies are sorely needed in preclinical models and in humans to assess the effects of individual cannabinoids and combinations of cannabinoids on cancer- and treatment-related anxiety and depression.
Sleep disorders and fatigue
Up to 80% of patients with cancer experience trouble sleeping. 223 In fact, three times more patients with cancer have insomnia compared with the general population. 223 Inflammation and metabolic dysregulation are potential contributing mechanisms for disrupted circadian rhythms. 224 Sleep disorders (e.g., insomnia, poor sleep quality) are also highly associated with cancer-related fatigue,223,224 one of the most common and debilitating side effects of cancer and its treatment. 225 Thus, both symptoms are discussed here.
The endocannabinoid system is integrated into circadian rhythm and sleep-wake cycles. For example, in rats, AEA is higher in the dark phase of the dark-light cycle, and 2-AG is higher during the light in areas of the brain related to sleep (reviewed by Prospero-Garcia and colleagues 226 ). In addition, the expression of CB1 receptors in the cerebral cortex of rats undergoes diurnal fluctuations, as does CB1 receptor mRNA concentrations in pertinent brain regions.226,227 In humans, similar patterns have been observed, where 2-AG peaks at approximately 13:00 and reaches its minimum at approximately 02:00, in the middle of the night. 228 Preclinical studies with exogenous cannabinoids have suggested that endocannabinoids regulate circadian rhythm, rather than other activities of the sleep–wake cycle affecting cannabinoid concentration and activity. 226 CBD in particular may help induce sleep, with less of a subsequent ‘hangover’ effect than common sleep aids such as benzodiazepines.229,230
No studies, to our knowledge, have specifically assessed cannabis in humans as a treatment for sleep disorders or fatigue, cancer-related or otherwise, as a primary aim. However, in studies among patients with irritable bowel disease, 160 Crohn’s disease, 231 Parkinson’s disease, 232 multiple sclerosis, 232 and post-traumatic stress disorder (PTSD), 233 for whom fatigue is a serious issue, users of cannabis or hashish (recreational or medicinal) reported less fatigue than patients who did not use cannabis. Similarly, a THC–CBD oromucosal spray reduced sleep disturbances in patients with multiple sclerosis, 234 and a recent report concluded that there is moderate evidence that cannabinoids, primarily nabiximols, are an effective treatment to improve short-term sleep outcomes in individuals with obstructive sleep apnea syndrome, fibromyalgia, chronic pain, and multiple sclerosis. 73
The use of cannabis for sleep disorders and to alleviate fatigue is limited in ways similar to other sleep aids in that patients could become dependent. 230 In addition, the literature thus far has not involved patients with cancer, and therefore the mechanisms by which fatigue and sleep disorders arise might be affected by endocannabinoid regulators differently than fatigue/sleep disorders from other conditions.
Metabolic, cardiovascular, and bone health toxicity
Many modern chemotherapy agents are associated with cardiotoxicity, including congestive heart failure, myocardial infarction, systemic hypertension, and others; 235 metabolic toxicity including declining insulin sensitivity, dysregulated circulating lipids, loss of skeletal muscle mass (i.e., cachexia), and overall worsening metabolic profiles; 236 and bone health toxicities including reduced bone mineral density and increased risk of osteoporotic fractures. 237 Indeed, more and more patients are surviving cancer, but many of these patients have an increased risk for morbidities and mortality from cardiovascular and metabolic diseases. Via the endocannabinoid system, inflammation, and other pathways, cannabinoids have the potential to modulate cardiovascular function,238,239 bioenergetics, 240 bone formation, 241 and many other metabolic processes.
There have not been any studies, to the best of the authors’ knowledge, that have assessed the effects of cannabis on cancer- and treatment-related cardiovascular, metabolic, or bone toxicities in humans. However, CBD protected against the doxorubicin-induced effects on mitochondrial function and biogenesis, which precipitate declines in cardiovascular health, in mice. 242 In addition, several but not all epidemiological studies have shown that current marijuana users had lower fasting insulin levels than former or never users.243–245 A 2016 review concluded that there is not enough evidence to recommend or discourage the use of cannabinoids for the treatment of cancer-related cachexia.243,246 In regard to bone health, the endocannabinoid system plays a major role in regulating bone metabolism, 247 and preclinical mouse models have shown that AM1241, a cannabinoid type 2 receptor agonist, reduced bone loss, bone pain, and the incidence of cancer-induced bone fractures while suppressing cancer growth.248,249
In brief, the therapeutic benefit and mechanistic insight into cannabis for these side effects is particularly limited, and future research is sorely needed to evaluate the role of cannabis and cannabinoids in the etiology of cardiovascular, metabolic, and bone toxicities.
Adverse side effects
In general, cannabis is well tolerated, often with pleasant side effects and few and minor short- and long-term negative side effects. 4 Acutely, cannabis causes strong psychoactive effects, which are chiefly attributed to THC. This is the ‘high’ that recreational cannabis users are seeking, and these effects include euphoria, relaxation, alterations in perception, and time distortion. 250 However, anxiety, paranoia, and panic attacks are also side effects of THC, especially in first-time users and with particularly high doses. 250 Cognitive abilities such as attention and memory can also be compromised. Moreover, cannabis use can impair judgment and reaction time, thus reducing the ability to operate a motor vehicle.251–253 Unlike THC, CBD lacks psychoactive properties and attenuates the psychoactive effects of THC administered simultaneously 254 (reviewed by Abrams and Guzman 4 ). But CBD does have potential side effects including diarrhea and drowsiness. 255 Frequent high doses of recreational cannabis has been associated with cannabinoid hyperemesis syndrome, or intractable vomiting. 75 Toxicities of the lung and heart have been reported but are rare. 256
Allergies to cannabis have been reported. These allergic reactions are IgE-mediated and can vary in severity depending on the route of exposure. For example, smoking or vaporizing can lead to rhinitis, conjunctivitis, and asthma, while direct skin contact can lead to hives and contact dermatitis, and ingesting it can lead to anaphylaxis. 257 Cannabis use has been associated with an increased risk for ischemic stroke in young adults. 258
Cannabis use also has documented long-term adverse effects. Chronic cannabis users tend to have respiratory problems and may be more susceptible to respiratory infections. 250 Preclinical evidence demonstrates that chronic cannabis use can have negative effects on reproduction for both men and women, including low testosterone, impaired sperm motility and viability, and disruption of the ovulatory cycle. 250 Long-term use can lead to cardiovascular issues, especially in middle-aged and older adults, including angina and exacerbation of cardiovascular disease.259,260 An association between cannabis use and schizophrenia has been well documented, especially when use is initiated at a young age. However, a recent sophisticated two-sample Mendelian randomization study concluded that, while causation might be occurring in both directions, it is more likely that schizophrenia risk causes cannabis use, rather than vice versa. 261 Further, there is evidence of associations between habitual cannabis use and long-term cognitive problems.192,193 Heavy cannabis use is also associated with low bone mineral density and increased risk of osteoporotic fractures, perhaps through negative effects on mesenchymal stem cells and osteogenesis.247,262 Addiction is a concern among some prescribers and, although approximately 9% of long-term recreational users of cannabis become addicted, 255 studies among patients with either cancer or AIDS found that treatment with THC did not lead to addiction or dependency. 82 Furthermore, heavy cannabis use disrupts sleep, and cannabis use to reduce sleep latency could become habit-forming; therefore, patients should use caution and frequently discuss their patterns of use, dose, motivations, and symptoms/side effects with their treatment team. 263
There are many other dangers of recreationally sold cannabis and cannabinoids due to the currently unregulated market. Synthetic cannabinoids and ‘dabs,’ inhalable concentrates that comprise a high concentration of THC, can impose serious psychotic, neurotoxic, cardiotoxic, and renal side effects.264,265 Moreover, cannabis plants and products largely remain untested for contaminants including fungi (mold), bacteria, heavy metals, and pesticides, as well as adulterants.266,267 With that said, more and more States are implementing stringent testing standards to uphold the safety of their products. Considering patients with cancer are already immune-compromised, contaminated and adulterated products could cause more harm than good.
Links between cannabis and cancer
With the strong evidence of association between tobacco use and cancer268–270 and the inherent similarities of tobacco and cannabis, it is important to assess the impact of cannabis use on cancer risk, progression, and recurrence. However, the available data among these relationships is scarce and equivocal. 73 There may be a relationship between current, frequent, or chronic cannabis use and the incidence of nonseminoma-type testicular germ cell tumors, 271 though evidence is lacking for incidence of all other cancers at this point. 73 Owing to the recent introduction of medical marijuana to the clinic, studies on cannabis and cancer progression and recurrence are largely absent.
There is also a real possibility that cannabis and cannabis-derived treatments can interact with cancer treatments such as chemotherapy and immunotherapy. 272 For example, Taha and colleagues recently published a retrospective study among patients with advanced melanoma, non-small cell lung cancer, or renal clear cell carcinoma on immunotherapy. This study was conducted in Israel, where cannabis use is more prevalent; 140 patients on immunotherapy were observed, 51 of whom elected to use cannabis. They showed that the use of cannabis during treatment reduced the response rate to immunotherapy. 273
Practical application in the clinic
The social and political climate is increasing patients’ and clinicians’ interest in cannabis for treatment of cancer-related symptoms. However, because of the extreme dearth of research on cannabis among patients with cancer, data are as yet insufficient to recommend cannabis instead of any current treatments. 68 With that said, minimal drug–drug interactions have been reported, side effects tend to be mild, and very preliminary reports indicate that cannabinoids tend to have anticancer rather than procancer effects,40,73,274,275 so it is reasonable to try cannabis in addition to guideline-based treatments. Table 3 serves as a communication guide for clinicians and patients to determine if and how cannabis could be considered in cancer care, and Table 2 describes the most common delivery mechanisms (inhalation, oral consumption, and topical) though extremely scant research has been done to evaluate the bioavailability of cannabinoids in most forms that are publicly available at dispensaries. 276 Clinicians should emphasize that patients should not forgo evidence-based therapies in favor of cannabis, as the risks and benefits of cannabis are still being discovered. Clinicians and patients also need to be aware that there may be yet undiscovered interactions between cannabis and the cancer, as well as negative drug–drug interactions (e.g., nivolumab immunotherapy and cannabis, 273 valproic acid and CBD 255 ). Over the next several years and decades, different forms of cannabis and cannabinoids will likely surface as more efficacious for different symptoms. Users should also be aware that the ratios of the bioactive compounds vary between plant strains and growth conditions, and therefore the therapeutic benefits and risks of side effects might not be predictable (even with repeat purchasing of the ‘same’ product), especially in the young cannabis market.
Discussion topics to guide clinical recommendations for cannabis.
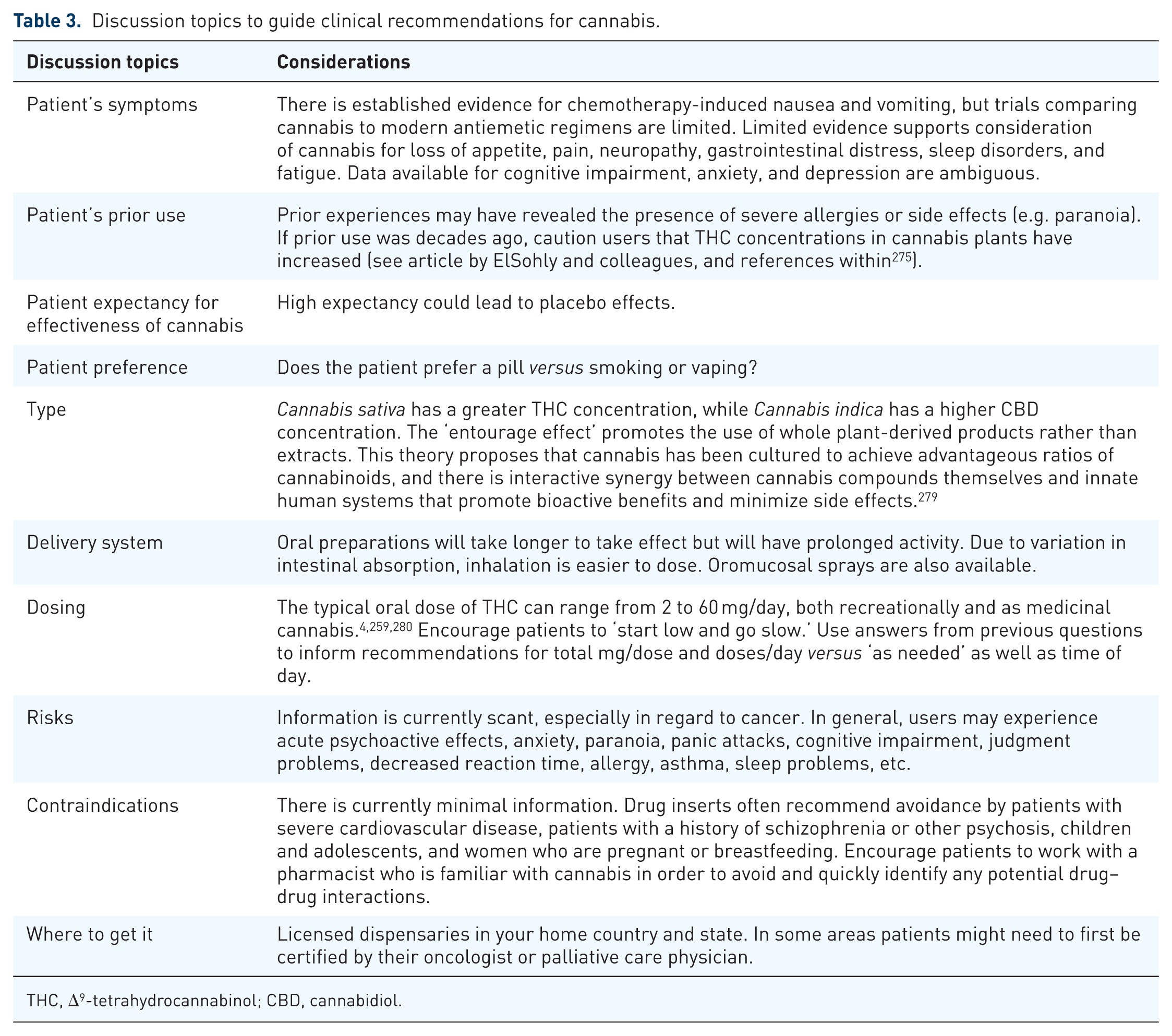
THC, Δ9-tetrahydrocannabinol; CBD, cannabidiol.
In addition, of the studies that have been performed in the US, all of them that used the cannabis plant (vaporized or smoked) procured it from the National Institute on Drug Abuse. 73 However, this strain varies drastically from the cannabis that is currently available (legally and illegally) in concentrations of THC, CBD, and other bioactive compounds.128,277,278 Indeed, US federally supplied cannabis for research purposes cannot be used to assess the efficacy of cannabis that is marketed and used for any given symptom from cannabis dispensaries.
Future research
It is our hope that research will accelerate to meet the needs of patients and clinicians in this rapidly growing field. Cancer is not one disease but a heterogeneous class of diseases that vary greatly in progression and symptom burden. In addition, current treatments vary drastically in their effectiveness against the cancer as well as their side-effect profile. Therefore, ‘medical marijuana’ will likely quickly evolve into more granular treatments for more specific ailments as evidence supporting and contraindicating its use accumulates.
There are, to date, very few studies evaluating the use of cannabis and cannabinoids to alleviate side effects of cancer and cancer treatments in humans. Regulatory barriers need to come down so that researchers have adequate access to cannabis in the US. 276 Studies looking specifically at certain symptoms including CIPN, cognitive impairment, anxiety, depression, sleep disorders, and fatigue are sorely needed. Studies for palliative use need only focus on short-term toxicities, but supportive care studies will need to incorporate longer timelines. Researchers need to be cognizant of the wide range in the presence and severity of cancer-related symptoms, adverse effects, and unknown interactions with other medications. 94 A well-documented placebo effect needs to be accounted for in research designs.94,95 The current literature is critically limited in that many cross-sectional studies are performed at medical marijuana dispensaries, which are biased toward patients who experience benefits, and many cannabis studies are prospective, thereby preventing assessment over time compared with a control. In addition, especially in regards to chemotherapy-induced nausea and vomiting, cannabis has not been compared with modern treatments. Further research not just describing the efficacy but also elucidating the mechanism of action of cannabis will help optimize more targeted interventions on specific symptoms and populations.
Conclusion
Cannabis offers many opportunities for supportive and palliative care in cancer, and recent changes in the social climate and legalization of cannabis will hopefully facilitate randomized studies to more accurately weigh the risks and benefits of cannabis use and optimize dose and administration methods. Currently, clinical evidence in populations with cancer is beginning to emerge to support the use of cannabis for treating chemotherapy-induced nausea and vomiting, loss of appetite, pain, and chemotherapy-induced peripheral neuropathy; data from other populations suggest that cannabis could be used to potentially alleviate gastrointestinal distress, anxiety, and sleep disorders (Table 1). However, there are not yet data available to specify the optimal cannabis-derived treatment, dose, or delivery system. Clinicians should stay up-to-date with cannabis regulations and guidelines,68,281 and work with patients within their preferences to alleviate symptoms. 282 Indeed, 58% of patients wish they had more information on the benefits and risks of medical cannabis, 283 so clinicians should have go-to references available for patients. Cannabis has the potential to quickly assume a large role in medicine over the next decade, and scientists and clinicians have both opportunities and responsibilities to learn and disseminate its intricacies.
Supplemental Material
Suppl-Table-1 – Supplemental material for Opportunities for cannabis in supportive care in cancer
Supplemental material, Suppl-Table-1 for Opportunities for cannabis in supportive care in cancer by Amber S. Kleckner, Ian R. Kleckner, Charles S. Kamen, Mohamedtaki A. Tejani, Michelle C. Janelsins, Gary R. Morrow and Luke J. Peppone in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We thank Dr Susan Rosenthal for her editorial assistance and the thoughtful feedback from the reviewers.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by NIH/NCI UG1CA189961 to G.R.M. and Karen M. Mustian, NIH/NCI K07CA221931 to I.R.K, NIH/NCI K07CA168911 to L.J.P., and NIH/NCI R01CA200579 to L.J.P.
Conflict of interest statement
The authors declare no conflicts of interest. M.A.T. obtained research support from Bayer Pharmaceutics, but that collaboration is not relevant to this work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.