
Abstract
Background:
The optimal multimodality therapy for pancreatic ductal adenocarcinoma in the body or tail of the pancreas (PDAC-BT) is unclear. The purpose of this study was to compare overall 5-year survival between patients treated with adjuvant chemotherapy, adjuvant chemoradiation, and surgery alone.
Methods:
Patients from the National Cancer Database (1998–2012) with resected stage I or II PDAC-BT were included. Overall survival between the three treatment groups was compared using Cox proportional-hazards regression, propensity-score matching, and the Kaplan–Meier method.
Results:
Of the 700 patients included in the analysis, 189 (27%) were treated with chemotherapy, 226 (32%) were treated with chemoradiation, and 285 (41%) were treated with surgery alone. Chemoradiation was associated with higher survival than surgery alone [adjusted hazard ratio (HRadj): 0.67; 95% confidence interval (CI): 0.54, 0.84; p = 0.001], but there was no difference between chemotherapy and chemoradiation (HRadj: 0.82; 95% CI: 0.65, 1.05; p = 0.115). In propensity-score matched cohorts, median survival was 24.1 months (95% CI: 20.4, 28.4) with chemotherapy and 25.4 months (95% CI: 22.1, 31.7) with chemoradiation (log-rank p = 0.122). Among patients with positive resection margins, chemoradiation was associated with higher survival compared with chemotherapy (HRadj: 0.54; 95% CI: 0.32, 0.92; p = 0.022). In this subgroup of the propensity-score matched cohorts, median survival was 9.5 months (95% CI: 8.4, 16.0) with chemotherapy and 18.3 months (95% CI: 11.6, 26.3) with chemoradiation (log-rank p = 0.011).
Conclusion:
In patients with resected pancreatic body or tail adenocarcinoma, adjuvant chemoradiation was associated with higher survival compared with surgery alone. Among patients with positive resection margins, adjuvant chemoradiation was associated with higher survival compared with adjuvant chemotherapy.
Keywords
Introduction
Pancreatic cancer is the fourth leading cause of cancer death among men and women in the US, and will result in an estimated 44,330 deaths in 2018. 1 The optimal multimodality therapy for resectable pancreatic ductal adenocarcinoma (PDAC) is controversial. 2 Several clinical trials support the use of adjuvant chemotherapy,3–6 while other trials support the use of adjuvant chemoradiation.7–10 Due to a lack of definitive data, current National Comprehensive Cancer Network (NCCN) guidelines recommend either adjuvant chemotherapy alone or adjuvant induction chemotherapy followed by chemoradiation with or without subsequent chemotherapy. 11 The adjuvant regimen that includes chemoradiation is recommended for patients with high-risk features, such as positive resection margins or positive lymph nodes. 11
The most appropriate treatment for PDAC in the body or tail of the pancreas (PDAC-BT) is even less certain. These rare lesions are often excluded from clinical trials, 7 or are grouped with PDAC in the pancreatic head (PDAC-H)5,12 despite differences in tumor biology 13 and surgical management.
Of the studies that have investigated PDAC-BT, several found an association between adjuvant chemotherapy and higher survival compared with surgery alone,14–17 while another study found no association. 18 Redmond and colleagues 19 found an association between adjuvant chemoradiation and higher survival only in a subgroup of patients with positive lymph nodes. To our knowledge, no studies have compared outcomes of chemotherapy versus chemoradiation after distal pancreatectomy. In this study, we used data from the National Cancer Database (NCDB) to compare 5-year overall survival among patients with resected PDAC-BT. In one analysis, we used multivariable Cox proportional-hazards regression to compare overall survival between patients treated with adjuvant chemotherapy, adjuvant chemoradiation, and surgery alone. In a second analysis, we used propensity-score matching, Cox proportional-hazards regression, and the Kaplan–Meier method to compare survival between adjuvant chemotherapy and adjuvant chemoradiation. Patients with positive resection margins 20 or positive lymph nodes 19 may have a greater survival benefit from chemoradiation, so stratified analyses based on these risk factors were performed.
Methods
Data source
The study was performed using data from the NCDB. The NCDB is sponsored by the American College of Surgeons and the American Cancer Society, and includes data collected from over 1500 Commission on Cancer-accredited facilities. 21 More than 70% of newly diagnosed cancer cases nationwide are represented in the database. 21 All patient information in the NCDB was de-identified so the study was exempt from Institutional Review Board evaluation.
Patient population
The NCDB was queried for subjects ⩾18 years old who were diagnosed with pancreatic cancer between 1998 and 2012. Inclusion criteria were stage I or II adenocarcinoma located in the body or tail of the pancreas (ICD-O-3 C25.1 and C25.2, respectively) that was treated by partial pancreatectomy. Patients treated with neoadjuvant therapy, immunotherapy, intra-operative radiation, or adjuvant radiation without chemotherapy were excluded. Patients with missing follow-up data were excluded. Patients who died within 90 days of surgery were excluded, as this was evidence of rapidly progressive disease or severe postoperative complications.
Patients were classified into the chemoradiation cohort if they were treated with adjuvant chemotherapy and adjuvant radiation therapy. This included patients who began radiation therapy concurrent with or after beginning chemotherapy. NCCN guidelines recommend initiating chemotherapy within 3 months of surgery, 11 so patients who began chemotherapy ⩾12 weeks (84 days) after surgery were excluded. American Society of Clinical Oncology (ASCO) guidelines recommend initiating chemoradiation after 4–6 months of chemotherapy, 22 so patients who began radiation therapy more than 6 months (180 days) after beginning chemotherapy were also excluded. The NCDB had data indicating that chemotherapy involved a single agent or multiple agents, but the database did not capture details about specific chemotherapy regimens.
Statistical analysis
Cox proportional-hazards models were used to estimate hazard ratios (HRs), 95% confidence intervals (95% CI), and p values for the association between treatment modality (adjuvant chemotherapy, adjuvant chemoradiation, and surgery alone) and death within 5 years. The multivariable analysis adjusted for the following categorical variables: sex, age (<65 or ⩾65), tumor size (<3 cm or ⩾3 cm), lymph-node status (positive or negative), tumor grade (well differentiated, moderately differentiated, poorly differentiated, undifferentiated, or unknown), margin status (positive or negative), and comorbidities according to the Charlson/Deyo index 23 (0, 1, or ⩾2). The Charlson/Deyo index 23 is a comorbidity index that is frequently used for risk adjustment in clinical outcome research. It is based on ICD-9-CM secondary diagnoses codes for conditions including myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, chronic pulmonary disease, rheumatologic disease, peptic ulcer disease, liver disease, diabetes, paralysis, liver disease, and acquired immunodeficiency syndrome. 23
We also performed a propensity-score-matched analysis of the chemotherapy and chemoradiation cohorts. Propensity scores for receiving chemoradiation were estimated using a multivariable logistic regression model with the following independent variables: sex, age, tumor size, lymph-node status, tumor grade, margin status, and comorbid conditions (Charlson/Deyo index 23 ). Matching was performed in a nearest-neighbor one-to-one fashion without replacement. Patient and tumor characteristics were compared with two-sided t tests or Pearson’s chi-square tests. The 5-year overall survival was compared using Cox proportional-hazards regression and the Kaplan–Meier method.
All statistical analyses were performed using STATA 14.1 (StataCorp, College Station, TX). The propensity-score analysis was performed using the STATA package psmatch2. 24
Results
A total of 234,033 cases of pancreatic adenocarcinoma were identified in the NCDB. A total of 22% (n = 52,422) were in the body or tail of the pancreas, of which 15% (n = 7628) were stage I or II disease. Of these, 26% (n = 1942) were treated with partial pancreatectomy, while 20% (n = 1528) were treated with a resection other than partial pancreatectomy (0.4% (n = 32) had local excision of tumor, 12% (n = 923) had pancreaticoduodenectomy, 5% (n = 378) had total pancreatectomy, and 3% (n = 258) had an unknown type of pancreatectomy. Among patients who underwent partial pancreatectomy, 1242 met exclusion criteria, leaving 700 patients for analysis. Of these, 27% (n = 189) were treated with chemotherapy, 32% (n = 226) were treated chemoradiation, and 41% (n = 285) were treated with surgery alone (Figure 1).
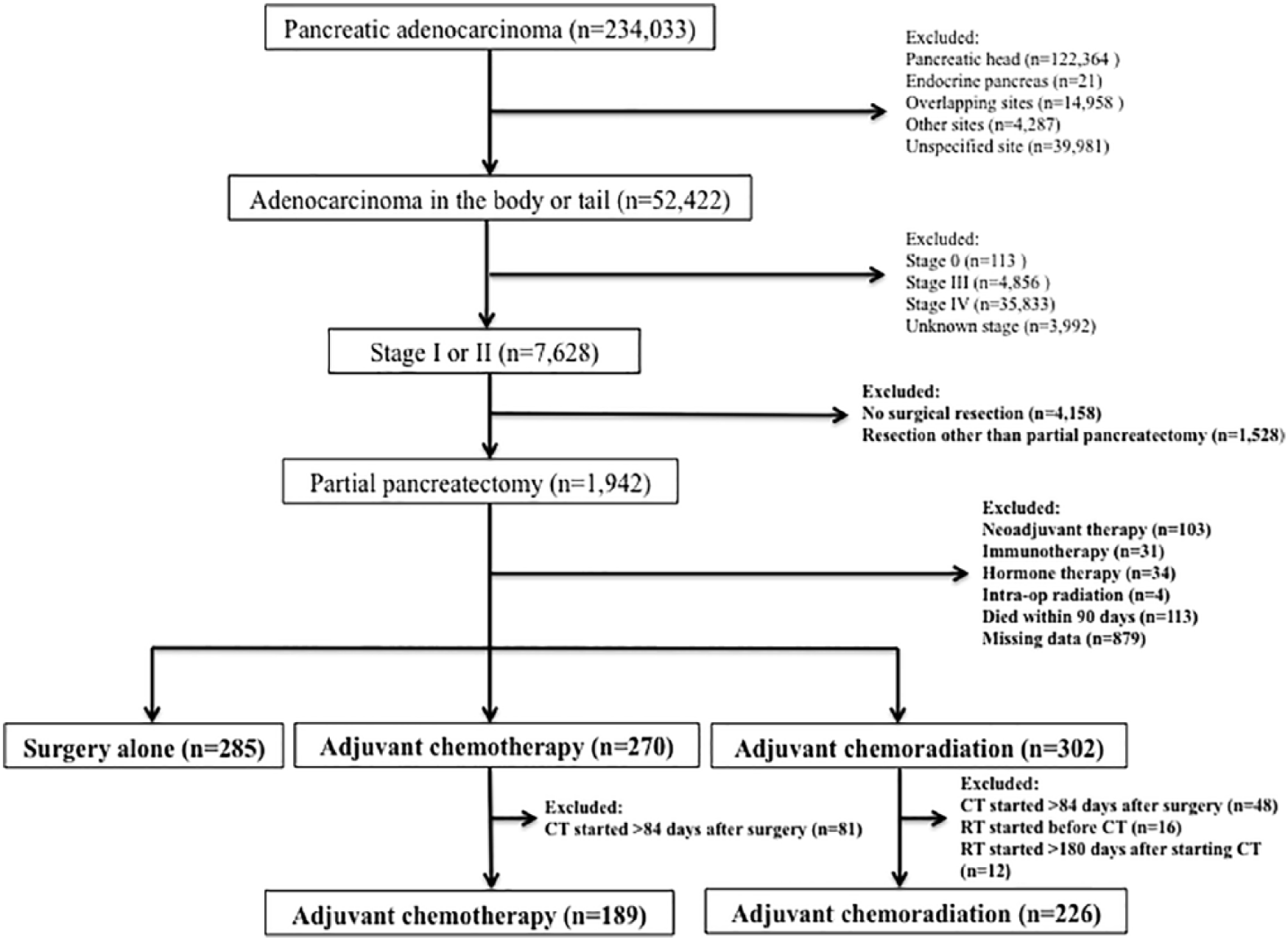
CONSORT diagram.
In the chemoradiation cohort, radiation was initiated on the same day as chemotherapy in 35% of patients (n = 80) and after the initiation of chemotherapy in 65% of patients (n = 146). In the latter subgroup, the median interval between initiating chemotherapy and radiation therapy was 40 days [interquartile range (IQR): 28, 76]. The clinical and histopathological characteristics of the cohorts are described in Table 1. The majority of tumors in all treatment groups were stage II and were resected with negative margins.
Baseline patient and tumor characteristics by treatment group.

Continuous variables are described by median (IQR, interquartile range). Categorical variables are described by n (%). Hospital length of stay: postoperative hospital length of stay. Surgery/chemotherapy interval: time between surgery and the initiation of chemotherapy. Surgery/radiation interval: time between surgery and the initiation of radiation therapy. Chemotherapy/radiation interval: time between the initiation of chemotherapy and the initiation of radiation therapy.
p value comparing propensity-score matched chemotherapy and chemoradiation cohorts. Categorical variables were compared by two-sided Pearson’s chi-square tests and continuous variables were compared by two-sided t tests.
Propensity-score matching
The chemotherapy and chemoradiation cohorts were propensity-score matched in a one-to-one fashion. After matching, there were 189 patients in each cohort. The matching variables were well balanced between the two cohorts (all p values ⩾ 0.496; Table 1). The median interval between surgery and the initiation of chemotherapy was 48 days (IQR: 36, 56) in the chemotherapy cohort and 47 days (IQR: 35, 57) in the chemoradiation cohort (p = 0.894; Table 1). More patients in the chemoradiation cohort were treated with multiagent chemotherapy regimens (37% versus 22%; p = 0.006; Table 1). In the chemoradiation cohort, radiation was initiated on the same day as chemotherapy in 63 patients (33%) and after the initiation of chemotherapy in 126 patients (67%). In the latter subgroup, the median interval between initiating chemotherapy and radiation therapy was 41 days (IQR: 28, 76).
Main analysis
In multivariable Cox proportional-hazards regression, chemoradiation and surgery alone were not associated with survival compared with chemotherapy (HRadj: 0.82; 95% CI: 0.65, 1.05; p = 0.115; and HRadj: 1.22; 95% CI: 0.97, 1.53; p = 0.092; respectively) (Table 2). Chemoradiation was associated with higher survival compared with surgery alone (HRadj: 0.67; 95% CI: 0.54, 0.84; p = 0.001). There was no difference in survival between chemotherapy and chemoradiation when also adjusting for type of chemotherapy (single agent or multiagent) (HRadj: 0.78; 95% CI: 0.59, 1.02; p = 0.069).
Multivariable Cox proportional-hazards regression for the risk of death within 5 years of diagnosis, stratified by margin status and lymph-node status.

Adjusted for sex, age, tumor size, lymph nodes status, tumor grade, margin status, and comorbidities according to the Charlson/Deyo index.
CI, confidence interval; HR, hazard ratio.
In the propensity-score-matched analysis, median survival was 24.1 months (95% CI: 20.4, 28.4) in the chemotherapy cohort and 25.4 months (95% CI: 22.1, 31.7) in the chemoradiation cohort (log-rank p = 0.122). Kaplan–Meier survival estimates are shown in Figure 2. In Cox proportional-hazards regression that adjusted for type of chemotherapy (single agent or multiagent), there was also no difference in survival [adjusted HR (HRadj): 0.84; 95% CI: 0.64, 1.10; p = 0.191].

Kaplan–Meier curves for overall survival of the chemotherapy and chemoradiation cohorts.
Stratified analyses
Margin status
A total of 35 patients (19%) in the chemotherapy cohort, 57 patients (25%) in the chemoradiation cohort, and 42 patients (15%) in the surgery-alone cohort had positive margins (Table 1). In multivariable Cox proportional-hazards regression of this subgroup, chemoradiation was associated with an approximately 46% lower risk of death within 5 years compared with chemotherapy (HRadj: 0.54; 95% CI: 0.32, 0.92; p = 0.022; Table 2). The difference in survival remained significant after adjusting for the type of chemotherapy (single agent or multiagent; HRadj: 0.46; 95% CI: 0.25, 0.85; p = 0.012). Among patients with negative margins, surgery alone was associated with lower survival compared with chemotherapy (HRadj: 1.36; 95% CI: 1.05, 1.78; p = 0.022); however, there was no difference in survival between chemotherapy and chemoradiation (HRadj: 0.91; 95% CI: 0.68, 1.20; p = 0.499; Table 2). Chemoradiation was associated with higher survival compared with surgery alone among patients with positive (HRadj: 0.56; 95% CI: 0.33, 0.95; p = 0.033) and negative margins (HRadj: 0.67; 95% CI: 0.52, 0.86; p = 0.002).
In the propensity-score-matched analysis, median survival among patients with positive margins was 9.5 months (95% CI: 8.4, 16.0) in the chemotherapy cohort and 18.3 months (95% CI: 11.6, 26.3) in the chemoradiation cohort (log-rank p = 0.011). Kaplan–Meier survival estimates are shown in Figure 3(a). In Cox proportional-hazards regression that adjusted for type of chemotherapy (single agent or multiagent), chemoradiation was associated with higher survival (HRadj: 0.47; 95% CI: 0.26, 0.86; p = 0.015). There was no difference in survival among patients with negative margins [log-rank p = 0.639; Figure 3(b)].
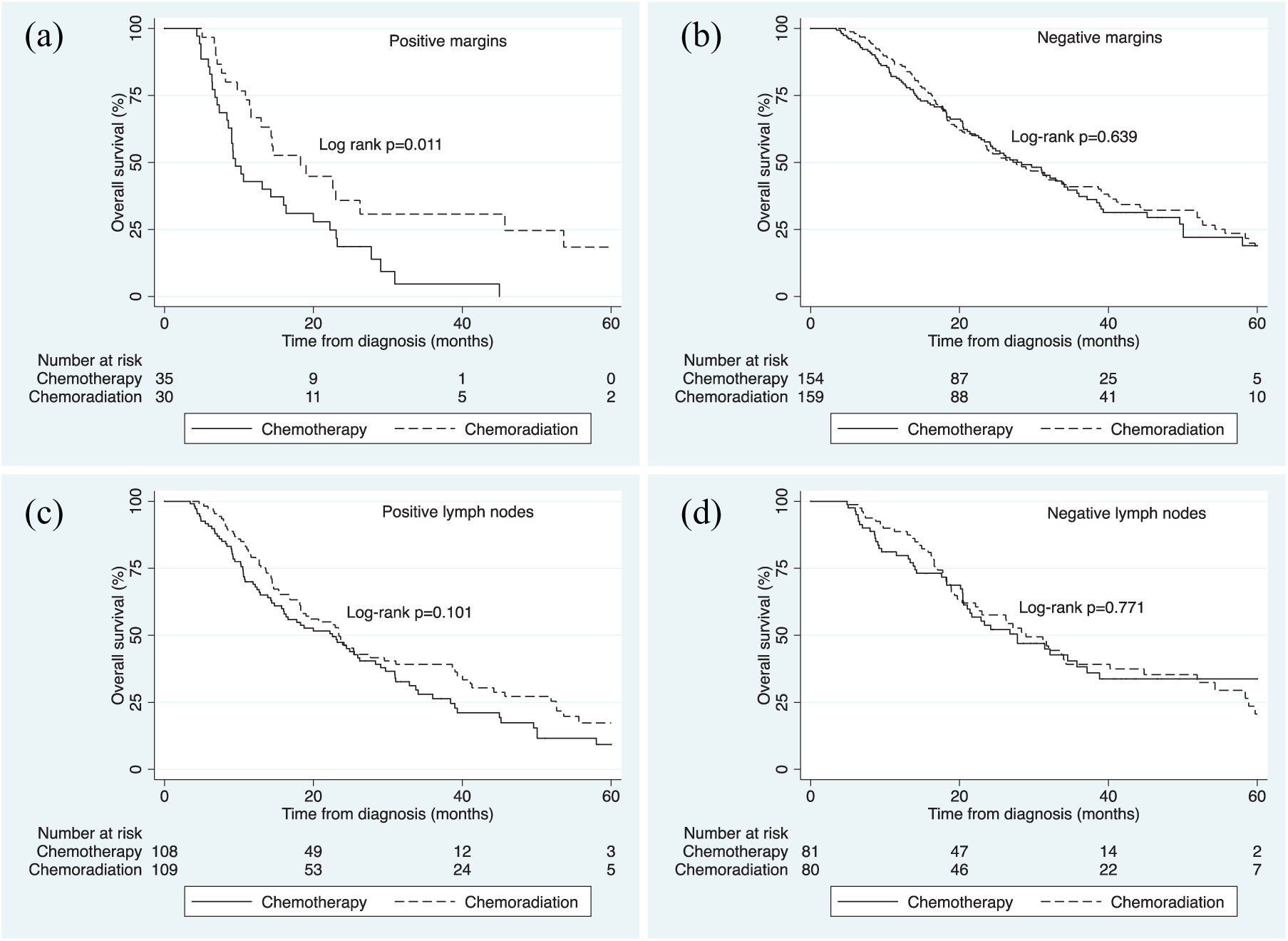
Kaplan–Meier curves for overall survival of the chemotherapy and chemoradiation cohorts, stratified by margin status and lymph-node status.
Lymph-node status
A total of 108 patients (57%) in the chemotherapy cohort, 133 patients (59%) in the chemoradiation cohort, and 135 patients (47%) in the surgery-alone cohort had positive lymph nodes (Table 1). In this subgroup, there was no difference in survival between chemotherapy and chemoradiation (HRadj: 0.80; 95% CI: 0.59, 1.09; p = 0.154) or surgery alone (HRadj: 1.33; 95% CI: 0.98, 1.80; p = 0.066; Table 2). There was also no difference in survival between chemotherapy and chemoradiation after adjusting for type of chemotherapy (single agent or multiagent; HRadj: 0.74; 95% CI: 0.52, 1.04; p = 0.086). Among patients with negative lymph nodes, there was no difference in survival between chemotherapy and chemoradiation (HRadj: 0.79; 95% CI: 0.52, 1.21; p = 0.284; Table 2). Chemoradiation was associated with higher survival compared with surgery alone among patient with positive lymph nodes (HRadj: 0.60; 95% CI: 0.45, 0.81; p = 0.001) and negative lymph nodes (HRadj: 0.66; 95% CI: 0.46, 0.95; p = 0.025).
In the propensity-score-matched analysis, median survival among patients with positive lymph nodes was 22.5 months (95% CI: 15.7, 28.4) in the chemotherapy cohort and 23.4 months (95% CI: 18.3, 31.1) in chemoradiation cohort (log-rank p = 0.101). Kaplan–Meier survival estimates are shown in Figure 3(c). In Cox proportional-hazards regression that adjusted for type of chemotherapy (single agent or multiagent), there was again no difference in survival (HRadj: 0.78; 95% CI: 0.56, 1.10; p = 0.151). Among patients with negative lymph nodes, there was no difference in survival between chemotherapy and chemoradiation [log-rank p = 0.771; Figure 3(d)].
Discussion
The optimal multimodality therapy for PDAC-BT is unclear. While surgical resection is the cornerstone of management, the benefits of adjuvant chemotherapy compared with adjuvant chemoradiation remain controversial. Clinical guidelines vary in their recommendations for adjuvant therapy for patients who were not treated with neoadjuvant therapy. The NCCN recommends either adjuvant chemotherapy or induction chemotherapy followed by adjuvant chemoradiation with or without subsequent chemotherapy. 11 The European Society for Medical Oncology recommends routine adjuvant chemotherapy, with the addition of adjuvant chemoradiation only for patients in clinical trials. 25 ASCO guidelines also recommend routine adjuvant chemotherapy, with the addition of adjuvant chemoradiation for patients with positive resection margins or positive lymph nodes. 22 Notably, none of the guidelines distinguish between PDAC-H and PDAC-BT.
The majority of patients in the landmark studies of pancreatic cancer had lesions in the pancreatic head rather than the body or tail. The GITSG 9173 study 7 included only one patient in each arm with PDAC-BT. The EORTC study 26 excluded patients with PDAC-BT. The ESPAC-1 5 and CONKO-001 studies 12 did not report tumor locations. In the RTOG 97-04 study, 27 only 13% of patients in the chemoradiation plus fluorouracil treatment arm and 15% of patients in the chemoradiation plus gemcitabine treatment arm had PDAC-BT, and the gemcitabine treatment arm was associated with a survival benefit only when PDAC-BT patients were excluded from the analysis.
Conclusions about treatment modalities for PDAC-H may not generalize to PDAC-BT, as there are important biological and anatomical differences between these lesions. PDAC-BT is associated with a lower resectability rate and lower survival than PDAC-H. This is possibly due to a tendency to present at a more advanced stage; 28 however, location in the body or tail has been shown to be an independent predictor of poor survival. One study found that among patients with nonmetastatic resected PDAC, those with PDAC-BT had lower survival compared with those with PDAC-H despite having smaller lesions and a lower rate of positive lymph nodes. 29
The poor prognosis of PDAC-BT is likely due to aggressive tumor biology. A study of genomic and transcriptonomic data found that PDAC-BT is associated with the squamous subtype of PDAC, 13 which is a subtype characterized by poor differentiation, higher grade, and poor prognosis. 30 Genes involved in tumor invasion, epithelial–mesenchymal transition, and antitumor immune suppression are highly expressed in PDAC-BT. 13 Moreover, the route of lymph-node metastasis and vascular invasion differ based on tumor location. PDAC-H tends to metastasize to the lymph nodes of the hepatoduodenal ligament, superior mesenteric artery, and anterior and posterior areas of the pancreatic head.31,32 These lesions frequently invade directly into the hepatic artery, superior mesenteric vessels, and portal vein. 33 PDAC-BT lesions, on the other hand, frequently metastasize to splenic artery lymph nodes32,34 and invade directly into the splenic artery and vein. 35 Finally, surgical management of the lesions is different: PDAC-H is typically managed with pancreaticoduodenectomy, whereas PDAC-BT is typically managed with distal pancreatectomy.
Few studies have examined the role of adjuvant therapies for PDAC-BT. De Rooji and colleagues 14 performed a retrospective analysis of 141 patients from 17 institutions. Those treated with surgery alone had lower overall survival compared with those treated with adjuvant chemotherapy (HRadj: 1.51; 95% CI: 1.01, 2.26; p < 0.045). A study by Paye and colleagues 36 included 278 patients from 28 centers and found that adjuvant chemotherapy was not associated with survival. Other smaller studies also have conflicting results: two found that adjuvant chemotherapy was associated with higher survival15,17 while one found no association with survival. 18
We identified only one study that investigated adjuvant chemoradiation after distal pancreatectomy. Redmond and colleagues 19 performed a single-institution retrospective study of patients treated with distal pancreatectomy. Of the 94 patients included in the final analysis, 72% were treated with adjuvant chemoradiation and 28% were treated with surgery alone. There was no significant difference in median, 1- or 2-year survival between the treatment groups. However, among patients with node-positive disease, adjuvant chemoradiation was associated with higher survival compared with surgery alone (HRadj: 0.23; 95% CI: 0.10, 0.52; p < 0.01).
In our NCDB study of patients with resected PDAC-BT, there was no difference in overall survival between chemotherapy and chemoradiation among the entire cohort. However, among patients with positive margins, chemoradiation was associated with an approximately 46% lower risk of death within 5 years (HRadj: 0.54; 95% CI: 0.32, 0.92; p = 0.022), and median survival with chemoradiation was 18.3 months (95% CI: 11.6, 26.3) compared with only 9.5 months (95% CI: 8.4, 16.0) with chemotherapy (log-rank p = 0.011). Although the chemoradiation cohort had a higher proportion of patients treated with multiagent chemotherapy regimens, the association with survival remained significant after adjusting for this difference (HRadj: 0.46; 95% CI: 0.25, 0.85; p = 0.012). There was no difference between chemotherapy and chemoradiation among patients with negative margins, or when the cohort was stratified by lymph-node status. Chemoradiation was associated with higher survival compared with surgery alone in all risk strata (p ⩽ 0.033). Among patients with negative margins, surgery alone was associated with lower survival compared with chemotherapy (HRadj: 1.36; 95% CI: 1.05, 1.78; p = 0.022).
Our finding that patients with positive resection margins have the greatest benefit from chemoradiation is consistent with a prior study of pancreatic adenocarcinoma. In a meta-analysis of four randomized controlled trials, Butturini and colleagues 20 found that patients with positive resection margins had a 28% lower risk of death after adjuvant chemoradiation (HR 0.72; 95% CI: 0.47, 1.10), while patients with negative resection margins had a 19% higher risk of death after adjuvant chemoradiation (HR: 1.19; 95% CI: 0.95, 1.49). Neither of these reached statistical significance. Other studies found no effect of margin status37–39 on treatment response. In their study of PDAC-BT, Redmond and colleagues 19 found that median survival for patients with positive resection margins was 8.6 months with no adjuvant therapy and 14.3 months with adjuvant chemoradiation.
This study had several limitations. As a retrospective analysis, there was potential bias related to patient selection for particular adjuvant therapies; the decision to treat with chemotherapy or chemoradiation may have depended, in part, on a patient’s postoperative course. We limited this selection bias by excluding patients who died within 90 days of surgery and those who did not begin chemotherapy within 12 weeks of surgery. In addition, we propensity-score matched the chemotherapy and chemoradiation cohorts based on patient and disease characteristics that may have influenced the treatment decision. Another limitation was likely variability in chemotherapy regimens, as the NCDB did not capture details about particular types of chemotherapies other than single agent or multiagent. Similarly, our study did not have a standardized chemoradiation regimen. Different chemoradiation protocols were commonly used at different times during the study period (1998–2012). In the earlier years, chemoradiation was often the initial adjuvant therapy,5,19 whereas the current standard is adjuvant chemotherapy followed by chemoradiation followed by additional chemotherapy. 11 Finally, many patients were excluded from the study due to missing data, which may have introduced bias.
In conclusion, we found evidence that patients with resected pancreatic body or tail adenocarcinoma with positive margins had higher overall survival when treated with adjuvant chemoradiation compared with adjuvant chemotherapy or surgery alone. There were no differences in survival between chemoradiation and chemotherapy among patients with negative margins or in subgroups stratified by lymph-node status. Clinical trials are needed to confirm these findings.
Footnotes
Acknowledgements
The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigator.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.