
Abstract
The incidence of thyroid cancer has increased markedly in recent decades, but has been stable in terms of mortality rates. For the most part, these cancers are treated with surgery, which may or may not be followed by radioactive iodine depending on the tumor subtype. Still, many of these cancers will recur and may be treated with radioactive iodine or another surgery. It is unclear what treatment is best for cases of locally advanced or metastatic thyroid cancer that are refractory to radioactive iodine. Chemotherapy has a very low response rate. However, in the past few years, several systemic therapies, primarily targeted, have emerged to improve the overall survival of these patients. Alternative treatments are also of interest, namely peptide receptor radionuclide therapy or immunotherapy.
Keywords
Introduction/epidemiology
In terms of frequency, thyroid cancer represents 90% of endocrine cancers 1 and 2.5% of all cancers, with a predominance in women, affecting 3–4-fold more women than men.2,3 When considering all types of thyroid cancer, it most often occurs in the fifth decade of life.1,4 Thyroid cancer continues to have a good prognosis with a 5-year survival rate of 98.1%4,5 for all types and stages combined. Over the last 30 years, its incidence has tripled according to figures from the National Cancer Institute in the United States, increasing from 5 to 15/100,000 people 6 ; while, the mortality rate has not changed and remains at 0.5/100,000 cases.1,6 Compared with more common cancers, such as lung, breast or colon, the incidence of thyroid cancer has increased the most since the 1990s. 7 This increase is proportionately the same in France 3 and Europe. 8 The incidence rate is increasing for all age groups and above all for papillary carcinomas. However, the incidences of follicular, medullary and anaplastic carcinomas have stabilized. 9 The increased incidence is explained by two phenomena: a false increase associated with an improvement in diagnostic techniques and a so-called real increase associated with environmental factors, such as radiation.1,7 Two groups of patients must be distinguished. The first group consists of patients with cancer that can be cured with surgery, occasionally followed by additional treatment with radioactive iodine. They represent 90% of patients with thyroid cancer and the incidence is increasing. The second group represents 5–15% of thyroid cancer cases that are at high risk of relapse and death, but have a stable incidence.2,10,11
Histology
Thyroid cancers are subdivided into three categories. The first type includes differentiated thyroid carcinomas (DTCs) derived from follicular cells, which are follicular carcinomas, papillary carcinomas, and Hürthle cell carcinomas (or oxyphil cell carcinomas). They represent >90% of thyroid cancers.2,12 The second type is represented by medullary thyroid carcinomas (MTCs) derived from parafollicular cells. This type represents 3–5% of thyroid cancers 13 and it is hereditary in 25% of cases 14 ; in addition, it is primarily associated with type 2A or 2B multiple endocrine neoplasia (MEN 2A or MEN 2B). Pheochromocytomas occur in 40–50% and hyperparathyroidism in 10–20% of MEN 2A associated MTC cases. 15 The third type includes anaplastic carcinoma, which is defined as undifferentiated carcinoma derived from follicular cells. This type generally has a very poor prognosis, with a median survival of 3–9 months.4,16 It is rare and represents only 2% of thyroid cancers.
Genetic mutations
In the past two decades, research has made great strides in understanding the tumor mechanism. The identification of certain abnormal characteristics of cancer cells has led to the emergence of treatments. Gene mutations, translocations or amplifications are responsible for how the cell cycle is controlled and, thus, induce the survival and proliferation of the tumor cells. Two main intra-tumor signaling pathways are the targets of these mutations: the mitogen-activated protein kinase (MAPK) pathway and the phosphatidylinositol 3-kinase (PI3K)/AKT/mammalian target of rapamycin (mTOR) pathway (Figure 1). These pathways are directly related to cell quiescence, proliferation and longevity. Somatic mutations, including point mutations and chromosomal rearrangements influencing these two intracellular signaling pathways, are responsible for the development of cancer cells. 17 These genetic alterations vary depending on the subtype of thyroid carcinoma.

Intra-tumor signaling pathways in thyroid carcinoma.
Well-differentiated carcinomas
In 45–59% of cases, DTCs express a mutation of the gene coding the BRAF protein,18,19 more often in papillary carcinoma than in follicular carcinoma. This mutation activates the MAPK signaling pathway and is associated with a certain degree of tumor aggressiveness,17,19 resulting in a higher incidence in patients with a recurrence or metastasis of a papillary carcinoma. 20 In 40–50% of follicular carcinomas, there is also a RAS mutation leading to constitutive activation of the two MAPK and PI3K/AKT/mTOR signaling pathways.17,21,22 To a lesser extent, this RAS gene mutation is also found in variants of papillary carcinoma (about 10–20% of the time). 17 The RAS gene mutation is also significantly associated with the appearance of hematogenous metastases (particularly bone metastases), suggesting RAS activation influences the metastatic capacity of these tumors.23,24 The third most common genetic anomaly encountered is the PPAR/PAX8-PPARγ rearrangement in 29–63% of follicular carcinomas.25–27 To a lesser extent, there are also RET/PTC mutations, PI3K amplification and PTEN losses 28 leading to increased cell growth, proliferation and survival.
Medullary carcinoma
In most MTC cases there are alterations of the RET gene, which codes for a membrane receptor, with tyrosine kinase activity, that plays a crucial role in regulating the proliferation, migration, differentiation and survival of cells. 29 The Ret alterations are found in >95% of hereditary MTCs associated with MEN 2A. These alterations are mainly located in exons 10 (codons 609, 611, 618 or 620) or 11 (codon 634) of the gene.15,30 For hereditary MTCs associated with MEN 2B, 15 there is a germinal mutation of the RET gene in 95% of cases. The mutation is usually located in exon 16 (codon 918) and much more rarely in exon 15 (codon 883). 15 In addition, 65% of sporadic forms of medullary carcinoma have the M918T mutation.31–33 The correlations between the genotype, the phenotype and the aggressiveness of the MTC were able to be determined by studying families with hereditary medullary cancers. 30 The mutation of exon 16 (codon 918) is considered the most aggressive.15,30
Anaplastic carcinoma
Anaplastic carcinomas may occur de novo, but they can also evolve from DTCs. Indeed, in 20–25% of anaplastic carcinomas, there is a history of a differentiated thyroid tumor and in 20–30% of cases, anaplastic carcinoma and a well-differentiated carcinoma coexist. 34 The cumulative incidences of BRAF V600E and RAS mutations in anaplastic carcinomas are around 50–60%. 34 Bearing in mind that these mutations occur often in the development of well-differentiated thyroid carcinomas, these could be anaplastic carcinomas resulting from the evolution of well-differentiated carcinomas. 34 In nearly 80% of cases 35 of anaplastic carcinoma, there is P53 (TP53) inactivation. What’s more, constitutive activation of the PI3K pathway is also often found in 53% of cases. 36 This pathway can be amplified by PTEN inactivation, AKT1 overexpression, or PiK3K or RAS mutations. 35 These RAS mutations are found in 20–30% of anaplastic thyroid carcinomas. Finally, a mutation in the telomerase reverse transcriptase (TERT) gene promoter was identified in 42–50% of anaplastic carcinomas.35,37 The TERT gene codes for a catalytic subunit of telomerase that plays a key role in the maintenance of cellular immortality and in oncogenesis by allowing the telomere length to be maintained at the end of the chromosomes. The TERT mutations are significantly associated with a poor prognosis. 37
Recurrent or persistent disease
The treatment of choice for localized thyroid cancers remains surgery. It may be a lobectomy or a total thyroidectomy, with or without central, unilateral or bilateral lymph node dissection. The type of surgery proposed is based on the type of thyroid cancer, the stage and the patient’s age.30,38–40 In some DTCs considered to be at high risk of recurrence, surgery may be supplemented by radioactive iodine treatment. 41 In other cases, treatment with radiation therapy may also be discussed, as in the case of anaplastic carcinomas. 40 The DTCs generally have an excellent prognosis after initial treatment with surgery, whether or not they are supplemented by treatment with radioactive iodine (cases with a high risk of recidivism). However, tumor relapses are not uncommon (~20%). 42 Places that are partial to metastases are the lungs (50%) and the bones (25%).43,44 The treatment of these recurrences is based on the inhibition of thyroid-stimulating hormone (TSH) as well as radioactive iodine if these metastases capture iodine, which represents two-thirds of locally advanced or metastatic DTCs. 44 In cases of local or metastatic relapse, treatment with radioactive iodine is required. However, 20–30% of these tumors considered to be radiosensitive eventually become resistant44,45 due to a mutation of the sodium-iodide symporter (NIS) gene. 46
Other types of thyroid carcinomas, such as medullary or anaplastic, are inherently non-sensitive to radioactive iodine. The challenge is to find an alternative to the surgical and radioactive iodine treatments that are no longer feasible for these radiation-resistant locally advanced or metastatic thyroid tumors. 44 Systemic therapies are considered under these circumstances. However, thyroid cancers are often indolent (Figure 2); thus, determining when to start a systemic treatment is not obvious, the aim being to control the disease while minimizing morbidity.
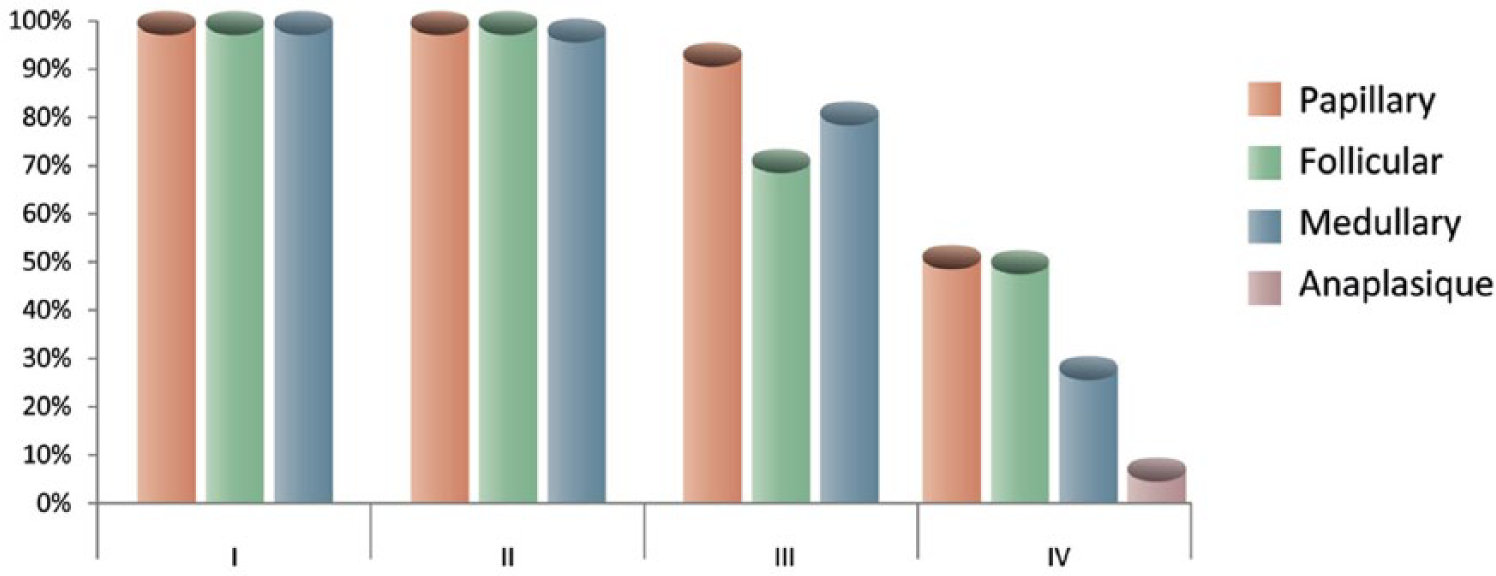
The 5-year survival of thyroid cancers according to stage. 47
Chemotherapy
For several decades before the development of targeted therapies, chemotherapy was the only systemic treatment available for thyroid cancers. The scarcity of advanced thyroid carcinoma limits the performance of large population and randomized studies. As a result, it is extremely difficult to compare data involving different chemotherapy regimens. 48 However, several chemotherapies, including bleomycin, doxorubicin alone or in combination, and paclitaxel, are potentially effective in treating thyroid cancers. Bleomycin was one of the first agents studied in the treatment of thyroid cancers. The first cohort reported by Harada and colleagues involved 17 patients and showed a partial response (PR) in seven patients. 49 Subsequently, several series and case reports were published with a failure of response or significant long-term toxicity associated with the use of bleomycin. Therefore, the value of this chemotherapy was considerably reduced. 50
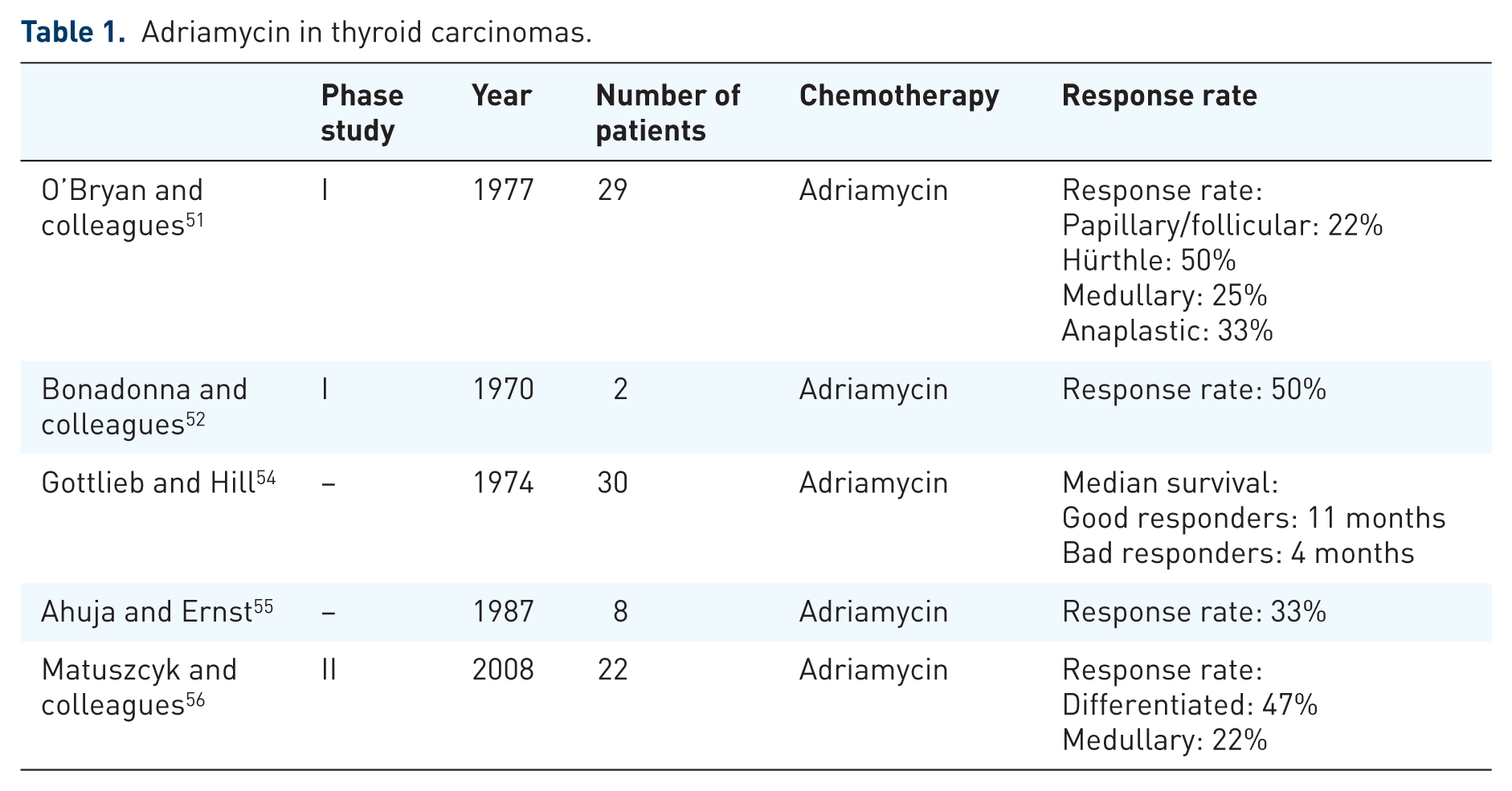
A second type of chemotherapy reported to be potentially effective is the class of anthracyclines, such as Adriamycin (doxorubicin), which offer response rates between 20% and 50% depending on the series and the subtype of thyroid carcinoma, with a better response rate for Hürthle carcinomas (Table 1).51–53 The recommended dose is usually 60–75 mg/m2 every 3 weeks with a maximum cumulative dose of 450 mg/m2. 50 A randomized study published by Shimaoka and colleagues 48 in 1985 showed the superiority of the combination of Adriamycin and cisplatin compared with Adriamycin alone. However, this difference only seems to be significant for anaplastic carcinomas.
Adriamycin in thyroid carcinomas.
In 2016, Albero and colleagues 57 published a meta-analysis covering prospective or retrospective series studying chemotherapy in DTCs, whether alone (Adriamycin, cisplatin, etoposide, carboplatin, methotrexate, mitoxantrone) or combined with another chemotherapy (Adriamycin and cisplatin or Adriamycin-based chemotherapy without cisplatin). The meta-analysis found a significant difference in terms of overall survival (OS) in favor of the combination of Adriamycin-based chemotherapy versus monotherapy: 15.2 months versus 35.6 months (p = 0.001). However, the study found it difficult to draw any conclusions, particularly in the determination of the various thyroid subtypes and the various study designs intended to evaluate therapeutic responses. 57
Recent data showed an interesting response rate for paclitaxel in anaplastic carcinomas. A phase II study published by Ain 58 in 2000 showed a response rate of 53% in a small series of 20 patients. In 2010, Higashiyama and colleagues 59 published a series of 13 patients with a stage IVb or IVc anaplastic thyroid carcinoma treated with paclitaxel with a response rate of 30.7%. This group compared the OS with untreated patients and concluded that the OS of patients with stage IVb is significantly better when they are treated with paclitaxel than if they have no treatment; however, patients with stage IVc had no improvement in their survival with paclitaxel. 59 In 2010, Kawada and colleagues also published a prospective study of seven patients with an anaplastic carcinoma treated with first-line docetaxel with a response rate of 14% and a disease control rate of 43%. 60 Given the small number of patients included in these studies, it is not possible to draw any relevant conclusions as to the efficacy of the first-line taxane treatment for anaplastic thyroid carcinomas. The last prospective study, published by Sosa and colleagues 61 in 2014, evaluating anaplastic carcinomas was stopped early due to too little recruitment: its aim was to evaluate the OS of treatment with paclitaxel and carboplatin with or without fosbretabulin. The study did not see a statistically significant difference in terms of OS. 61
Targeted therapies
Phase II studies have been carried out in patients with a radioactive iodine-refractory DTC evaluating axitinib, 62 motesanib, 63 pazopanib, 64 sunitinib, 65 vandetanib 66 and sorafenib. 67 However, only four phase III studies have been conducted, and they showed a benefit for sorafenib, lenvatinib, vandetanib and cabozantinib (Table 2). It is these four molecules that we will explain in detail due to their immediate benefit in the treatment of thyroid cancer: two for DTCs (sorafenib and lenvatinib) and two for medullary carcinomas (cabozantinib and vandetanib).
Phase III studies in locally advanced or metastatic thyroid cancers resistant to radioiodine.

DTC, differentiated thyroid carcinoma; HR, hazard ratio; MTC: medullary thyroid carcinoma; OS, overall survival; PFS, progression-free survival.
Sorafenib
Sorafenib is an inhibitor of various kinases, particularly the signaling pathway of rapidly accelerated fibrosarcoma (RAF) kinases involving the RAS/RAF/MEK/ERK proteins successively. In doing so, it inhibits angiogenesis and tumor growth. Sorafenib is also an inhibitor of kinases involved in angiogenesis such as c-KIT, FLT-3, vascular endothelial growth factor receptor (VEGFR)-2 and -3, and platelet-derived growth factor receptor (PDGFR)-β. It was approved by the Food and Drug Administration (FDA) in November 2013 as a treatment for advanced and progressive radioactive iodine-refractory DTCs following the publication of the phase III DECISION study.67,68 This was a phase III, randomized, double-blind study evaluating the efficacy of sorafenib versus placebo in patients with locally advanced or metastatic radiation-resistant DTCs progressing within the past 16 months according to Response Evaluation Criteria in Solid Tumor (RECIST) after iodine 131 therapy despite iodine-131 avidity at time of treatment or cumulative activity of iodine-131 >600 mCi. The findings of this study demonstrated a significant increase in progression-free survival (PFS) of 10.8 months versus 5.8 months [hazard ratio (HR) 0.49; 95% CI 0.39–0.61; p < 0.0001] for the sorafenib group. The OS in the study did not increase due probably in part to the crossover initially planned for by the study design, enabling patients in the placebo group to receive sorafenib upon progression.
Lenvatinib
Lenvatinib is an oral molecule capable of inhibiting VEGFRs 1, 2 and 3, fibroblast growth factor receptors 1–4, PDGFR-α, RET and KIT; receptors involved in the modulation of angiogenesis and lymphangiogenesis. This molecule showed clinical activity in a phase II study on patients with DTCs that were refractory to radioactive iodine. 72 As a result, Schlumberger and colleagues 69 conducted a phase III, double-blind, placebo-controlled study in patients with a pretreated or non-pretreated radioactive iodine-resistant DTC; this was the SELECT study. Radioactive iodine-resistant DTC was defined by a progression within the past 12 months according to RECIST after iodine 131 therapy despite iodine-131 avidity at time of treatment or cumulative activity of iodine-131 >600 mCi. The findings showed a marked increase in median PFS for the lenvatinib group of 18.3 months versus 3.6 months (p < 0.001). The OS showed a non-significant HR of 0.73 (p < 0.10). This can be explained by the possibility of crossover in the study. Because of these particularly positive findings, the FDA allowed it to be put on the market on 13 February 2015, despite its toxicity.
We note a significant difference in PFS between the two DTC studies, but inclusion criteria were different. Patients included in the SELECT trial were at an earlier stage in their disease than those in the previous study (DECISION). It is therefore difficult to conclude that one molecule is superior to the other in terms of PFS.
Vandetanib
Vandetanib is also an oral, multi-kinase inhibitor molecule mainly targeting the VEGFR, the epidermal growth factor receptor (EGFR) and RET-tyrosine kinase. Alterations of the RET gene are found in >95% of hereditary medullary cancers and in 65% of sporadic medullary cancers. A phase III study (ZETA study) carried out by Wells and colleagues and published in 2012 studied the effectiveness of vandetanib versus placebo in patients with a locally advanced or metastatic MTC in a randomized, double-blind study. 70 A significant extension of PFS was observed for the group receiving vandetanib compared with the placebo, with a HR of 0.46 (p < 0.001). The median PFS in the vandetanib group was not reached, but was estimated at 30.5 months; it was 19.3 months in the placebo group. In subgroup analyses, a benefit for both hereditary and sporadic cancers was noted. The highest response rate was obtained in the hereditary medullary carcinoma subgroup with the M918T mutation. The study could not, however, reach a conclusion for patients with an unmutated RET sporadic medullary carcinoma because there were not enough of them. The most common side effects are diarrhea, rash, nausea, high blood pressure and headache. In the study, treatment is described as well tolerated with only 12% of treatments stopped due to toxicity. Vandetanib was approved by the FDA in April 2011.
Cabozantinib
Cabozantinib is once again an inhibitor of tyrosine kinases targeting c-MET, VEGFR 2, AXL and RET, which are involved in normal cellular functions and pathological processes such as angiogenesis, invasion, tumor metastases and resistance to treatment. After showing a good response rate in a phase I study, 73 a randomized, double-blind, phase III study (EXAM study) 71 was carried out to show the efficacy of this molecule versus placebo in patients with a locally advanced or metastatic MTC. This study differs from the ZETA study in that patients had to show radiological progression at the time of inclusion, since this type of disease is relatively indolent. For its part, cabozantinib showed its superiority in terms of its PFS of 11.2 months versus 4 months in the placebo group (p < 0.001). The most common side effects were diarrhea, hand-foot syndrome, fatigue, hypertension, hemorrhage, fistula and gastrointestinal perforation. These events are traditionally described with treatments with tyrosine kinase inhibitors. Grade 3 and 4 adverse effects were reported in 69% of patients treated with cabozantinib versus 33% of patients receiving the placebo; 79% of patients receiving cabozantinib had their treatment interrupted and/or their dose reduced versus 9% in the placebo arm. As with the drugs mentioned above (sorafenib, vandetanib and lenvatinib), the efficacy of cabozantinib is clearly demonstrated, but it is important to make both prescribers and patients aware of the side effects.
All these new targeted therapies show significant improvements in survival in patients with DTC or MTC. However, side effects of the different molecules can be high and thus decrease the patient’s quality of life. Grade 3 or 4 treatment-related adverse effect was 69% with cabozantinib, 75% with lenvatinib, 37% with sorafenib and 30% with vandetanib.67,69,70 Moreover, natural progression of the DTC and MTC is usually slow; it would therefore be interesting to determine when to introduce treatments. Should we follow the inclusion criteria defining the progression of disease in studies and thus the early introduction of the treatment with a risk of decreased quality of life due to side effect? Or should we wait for symptomatic disease but at the risk of being confronted with a more advanced tumor? There is no answer yet to this question in the literature.
Treatment with a somatostatin analog and radionuclide
Neuroendocrine tumors, including thyroid tumors such as medullary carcinomas, are known to express somatostatin receptors,74,75 and this can be diagnosed by performing an octreotide scan 76 and, more recently, by performing a Ga-DOTATATE PET/CT. 75 The binding of analogs to the somatostatin receptor and, therefore, the tumor detection rate on imaging, varies depending on the histological subtype of DTC. In the study by Binse and colleagues, the 68 Ga-DOTATOC PET/CT identified a tumor relapse in all patients with poorly differentiated tumors (three patients) and Hürthle carcinoma (one patient). 75 Although the octreotide scan had been a promising tool for Hürthle carcinoma in previous studies,74,77–80 reports concerning octreotide receptor imaging in poorly differentiated thyroid carcinomas are rare.80,81
The use of somatostatin analogs in traditional neuroendocrine tumors helps control the symptoms and the disease. 82 Clinical trials on thyroid tumors have shown contradictory responses. 46 Two series of eight and six patients reported by Zlock and colleagues 83 and Kohlfuerst and colleagues 84 involving DTC and medullary tumors both reported treatment failure. On the other hand, a study on two patients reported by Robbins and colleagues 85 showed a tumor response in these two patients. The efficacy of using the somatostatin analogs still needs to be demonstrated through a randomized study. In contrast, patients with tumor lesions who have a strong avidity for DOTATATE may benefit from a new type of radionuclide-based therapy. This is a molecule of lutetium-177 or yttrium-90 linked to a somatostatin analog. This technique is called peptide receptor radionuclide therapy (PRRT). Several series reported a good response rate for both DTCs and MTCs (Table 3). These findings warrant a randomized study.
Studies of locally advanced or metastatic thyroid cancers resistant to radioiodine and treated with PRRT.

DP, disease progression; NA, not applicable; OS, overall survival; PR, partial response; SD, stable disease; TTP, time to progression.
Immunotherapy
Immunotherapy is a new systemic therapy that has grown in the past decade with the development of cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) 95 antibodies in metastatic melanoma and anti-programmed cell death-1 (anti-PD-1) also in melanoma,96,97 as well as non-small-cell lung cancer, kidney cancer, urothelial tumors, head and neck cancers, and Hodgkin’s disease.98–101 The PD-1 protein receptor is a negative regulator of T-cell activity. It is involved in controlling the immune response of T-cells and thus plays a pivotal role – by binding to its ligand (PDL-1 or PDL-2) expressed by tumor cells – in the ability of the tumor cells to escape the immune system. 102 A PD-1 antibody is a human immunoglobulin G4 monoclonal antibody that binds to the PD-1 receptor and blocks its interaction with PDL-1 and PDL-2, thereby generating anti-tumor activity by activating the patient’s immune system. The first two checkpoint inhibitors developed targeting PD-1 are pembrolizumab and nivolumab. 103
Testing for PD-L1 expression is not currently validated as a predictive biomarker in tumors such as melanoma. 103 However, the overexpression of PDL-1 in small-cell lung carcinomas is predictive of better PFS and OS. 104 Moreover, PDL-1 is overexpressed in many cancers and is associated with a poorer prognosis in cancers such as kidney or lung. 103 Chowdhury and colleagues conducted a retrospective study on the overexpression of PD-L1 in papillary thyroid cancers and showed it is correlated with an increased risk of relapse and, thus, is a marker of poor prognosis. 105 In addition, Zwaenepoel and colleagues described overexpression of PDL-1 in 28.3% of the anaplastic carcinomas analyzed. 106
This type of therapy is in its infancy in thyroid cancer. A phase I, dose-escalating study with nivolumab included one patient with an MTC. It had a PR with a median response of 13 months, which is very encouraging in terms of continuing to investigate this treatment. 107 A second case of response was observed in advanced thyroid cancer. 108 The two responses observed during immunotherapy are encouraging in terms of continuing research on the subject.
Re-sensitization to radioactive iodine
Differentiated thyroid tumors usually respond to radioactive iodine. However, by suppressing NIS expression, these tumors can become refractory to radioactive iodine. Several studies have demonstrated that when the BRAF V600E mutation is present, NIS expression is suppressed, thereby interfering with radioactive iodine uptake.109,110 Based on these new data, Rothenberg and colleagues 111 evaluated the administration of an anti-BRAF, such as dabrafenib, for 25 days in 10 patients with a BRAF mutation to see whether this had an impact on re-sensitization to radioactive iodine. Of these 10 patients, six once again showed iodine uptake and could be re-treated with radioactive iodine; two patients showed a PR; and four other patients showed stabilization of their disease.
In addition, selumetinib was tested in a phase II study to re-sensitize certain patients to radioactive iodine. Selumetinib is an MEK inhibitor that is located downstream of RAF on the intracellular MAPK signaling pathway; thus, if there is a BRAF mutation, the administration of an anti-MEK can inhibit the over-activation of this signaling pathway. Ho and colleagues 112 published a series of 20 patients, nine of whom had a BRAF mutation and five of whom had an NRAS mutation. Of these 20 patients, 12 rediscovered iodine uptake and eight could once again be treated with radioactive iodine with six PRs and two stable diseases. Of these eight patients re-treated with radioactive iodine, there were five with NRAS mutations and one with a BRAF mutation. Given these findings, a phase III study with selumetinib is underway to re-sensitize patients with DTCs that have become refractory to radioactive iodine treatment.
Conclusion
Systemic thyroid cancer treatments have evolved considerably over the past 10 years with the advent of targeted therapies, particularly for DTCs and MTCs. Sorafenib, lenvatinib, cabozantinib and vandetanib were effective in phase III, randomized studies, replacing traditional chemotherapy. However, given the indolence of these carcinomas and the side effects of these treatments, the appropriate time to initiate them is unclear. Only anaplastic carcinomas do not currently benefit from these advances in treatments; thus, chemotherapy remains the primary option despite its very limited efficacy. The PRRT track is also currently under development given that somatostatin receptors are often expressed in DTCs and MTCs. The possibility of re-sensitizing DTCs that have become refractory to radioactive iodine to iodine is also being studied with anti-BRAFs and anti-MEKs. The rise of immunotherapy may further alter the fate of patients with thyroid carcinoma, whether differentiated, medullary or anaplastic.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.