
Abstract
Non-small cell lung cancer (NSCLC) is still the leading cause of cancer-related death, and the treatment of advanced NSCLC relies on systemic treatments. During the last decade, pemetrexed, an antifolate agent, gradually became a key component of the treatment for patients with advanced nonsquamous NSCLC. It has indeed been shown to be efficient for first-line, maintenance and second- or third-line treatment in this subgroup of NSCLC. Moreover, it is usually well tolerated, with few grade 3 and 4 toxicities. Several studies have tried to identify predictive biomarkers of pemetrexed efficacy. Due to pemetrexed’s mechanism of action, thymidilate synthase expression predictive value was investigated but could not be demonstrated. Currently, more than 400 trials of pemetrexed for the treatment of nonsquamous NSCLC are ongoing.
Introduction
Lung cancer is still the leading cause of cancer-related deaths worldwide [Torre et al. 2015]. Efforts have been made during the last decades to improve advanced non-small cell lung cancer (NSCLC) outcomes. The most significant improvement for patients with lung cancer is the development of targeted therapies, prescribed on a personalized approach based on molecular profiling of the tumor and the identification of predictive biomarkers. More recently, immune checkpoint inhibitors (nivolumab) and new antiangiogenic agents (nintedanib, ramucirumab) emerged as new treatment options for pretreated lung cancer patients. However, standard chemotherapy remains a key component of advanced NSCLC treatment. Figure 1 summarizes guidelines for the treatment of Epidermal growth factor receptor (EGFR) and Anaplastic lymphoma kinase (ALK)-negative stage IV nonsquamous NSCLC. American Society of Clinical Oncology (ASCO) guidelines currently suggest that patients with stage IV nonsquamous NSCLC negative or unknown EGFR sensitizing mutation or ALK rearrangement and performance status (PS) 0 to 1 should receive a platinum-based combination of two cytotoxic drugs [Masters et al. 2015]. Pemetrexed, an antifolate agent, is one of the recommended drugs combined with cisplatin or carboplatin for first-line treatment of these patients.

Treatment algorithm of EGFR and ALK wild-type nonsquamous stage IV non-small cell lung cancer.
Pemetrexed was approved by the Food and Drug Association for several steps of nonsquamous NSCLC treatment (first line, maintenance therapy, and second and third lines). Based on results of the phase III studies described below, pemetrexed progressively became one of the most frequently used cytotoxic chemotherapy agents for treating stage IV nonsquamous NSCLC.
This review provides an overview of pemetrexed pharmacodynamics and pharmacokinetics, of the main studies leading to pemetrexed indications in nonsquamous NSCLC treatment, and of potential predictive biomarkers of pemetrexed efficacy.
Pharmacodynamics and pharmacokinetics
Pemetrexed belongs to the ‘folate antimetabolites’ class of chemotherapy agents. Pemetrexed inhibits cell replication and growth through the inhibition of three enzymes involved in purine and pyrimidine synthesis: thymidylate synthase (TS), dihydrofolate reductase (DHFR) and glycinamide ribonucleotide formyltransferase (GARFT) [McLeod et al. 2000]. Consequently, pemetrexed inhibits deoxyribonucleic acid (DNA) and ribonucleic acid (RNA) synthesis, needed for cell growth and survival.
Pemetrexed undergoes limited hepatic metabolism and is mainly eliminated in the urine. Its half-life clearance is 3.5 hours for patients with normal renal function (glomerular filtration rate (GFR) = 90 ml/min). Phase I and pharmacokinetic studies of pemetrexed administered every 3 weeks to patients with advanced solid tumors suggested that pemetrexed was well tolerated at doses of 500 mg/m2 with vitamin supplementation [Mita et al. 2006]. Pemetrexed is not recommended for patients with a GFR of less than 40 ml/min. Pemetrexed pharmacokinetics are independent from concurrent administration of cisplatin or vitamins [Mita et al. 2006].
First-line treatment
Several phase II and III studies assessed the efficacy and safety of pemetrexed for first-line treatment of advanced nonsquamous NSCLC (Table 1). Based on the results of these studies, pemetrexed was approved in combination with cisplatin or carboplatin. In addition, the combination of pemetrexed with other cytotoxic chemotherapies, targeted therapies or antiangiogenic agents has also been studied in the first-line setting. Table 1 reports the results of the main phase III studies investigating pemetrexed in nonsquamous NSCLC treatment.
Results of phase III trials of pemetrexed for nonsquamous non-small cell lung cancer treatment.
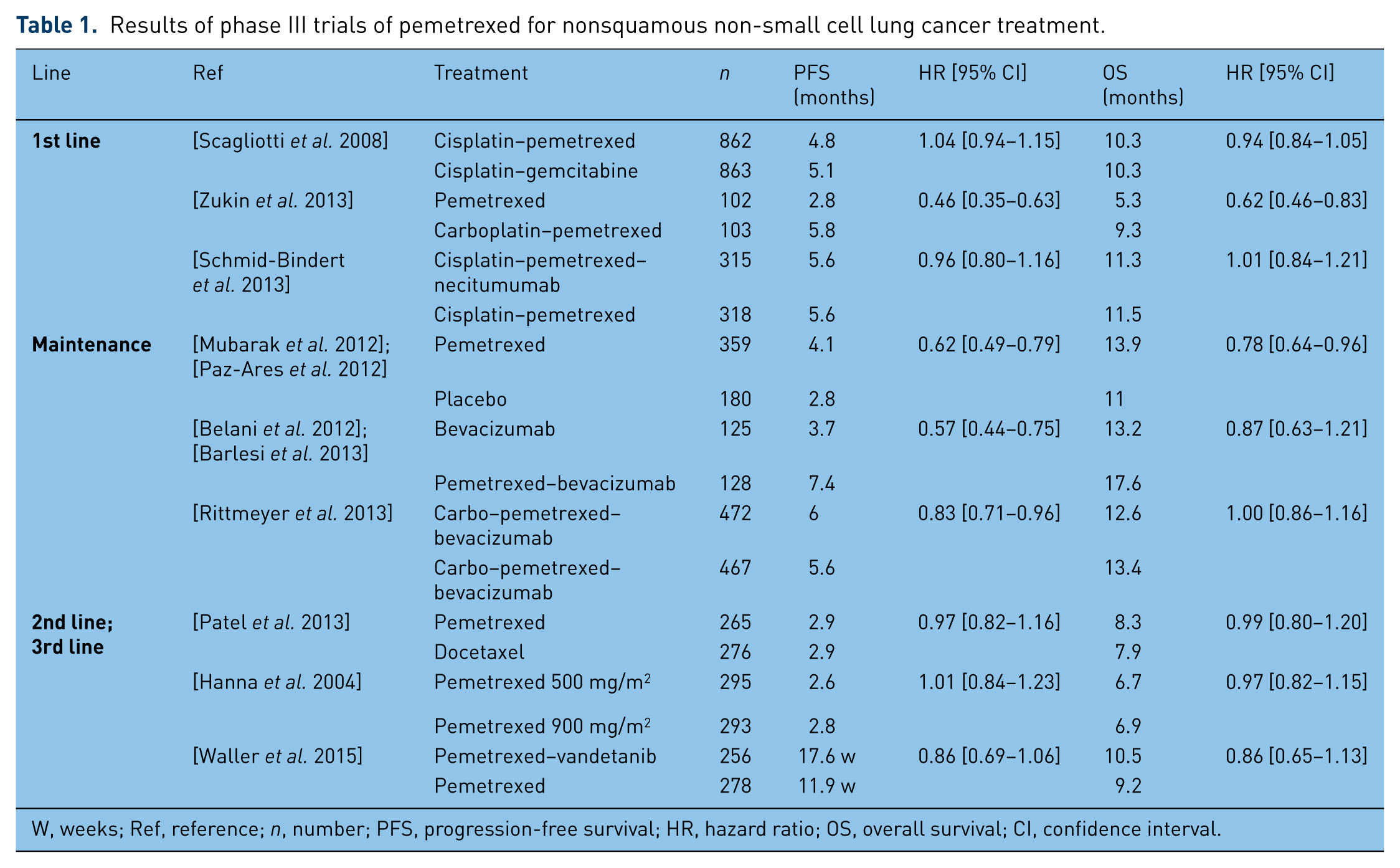
W, weeks; Ref, reference; n, number; PFS, progression-free survival; HR, hazard ratio; OS, overall survival; CI, confidence interval.
Platinum-based chemotherapy
Four phase II studies investigated the combination of pemetrexed with cisplatin or carboplatin for nonsquamous NSCLC first-line treatment [Zinner et al. 2005]. These assays showed good clinical efficacy with an overall survival (OS) ranging between 8.9 and 13.5 months. A pooled retrospective analysis of two of these phase II trials showed that the pemetrexed plus platinum combination tended to be more effective in nonsquamous histology subtypes in comparison with squamous cell carcinoma, in terms of objective response rates (ORRs) that were 30% versus 17%, respectively; progression-free survival (PFS) that was 5.6 versus 4.7 months, respectively; hazard ratio (HR), 0.72; 95% confidence interval (CI), 0.43–1.19, and OS (10.5 versus 9.8 months, respectively; HR, 0.95; 95% CI, 0.52–1.74) [Zinner et al. 2010]. Moreover, Schuette and colleagues demonstrated that pemetrexed plus cisplatin and pemetrexed plus carboplatin had a good efficacy profile, with an OS of 11.7 and 8.9 months, respectively, and a PFS of 6.0 and 4.7 months, respectively [Schuette et al. 2013].
Several phase II studies also investigated pemetrexed in combination with nonplatinum cytotoxic chemotherapy such as gemcitabine [Spigel et al. 2010], vinorelbine [Clarke et al. 2005] or paclitaxel [Stathopoulos et al. 2007]. The results of these studies are encouraging, with median OS ranging from 7.9 to 14.0 months. However, Spigel and colleagues suggested that platinum-based regimens were associated with a better time to progression (TTP) that was 10.2 versus 4.7 months without platinum and OS (14.8 versus 7.5 months) [Spigel et al. 2012].
Finally, a phase III study showed that the combination of cisplatin and pemetrexed was not inferior to cisplatin–gemcitabine, with a similar median survival of 10.3 months (HR = 0.94; 95% CI, 0.84–1.05) [Scagliotti et al. 2008]. OS was significantly better with cisplatin–pemetrexed in the subgroup of adenocarcinoma in comparison with cisplatin–gemcitabine (12.6 versus 10.9 months, respectively, p = 0.03), whereas in the subgroup of squamous cell carcinoma, OS was better with cisplatin–gemcitabine than with cisplatin–pemetrexed (10.4 versus 6.7 months, respectively, p = 0.05). These results were then confirmed by two meta-analyses of randomized clinical trials [Treat et al. 2012]. The combination of cisplatin and pemetrexed was thus approved for first-line treatment of performance status, PS1, nonsquamous NSCLC patients.
Pemetrexed has also been studied for first-line treatment of special subpopulations. For elderly patients, pemetrexed alone showed a good antitumor activity (response rate = 25%) [Kim et al. 2013], and the combination of pemetrexed with carboplatin induced an ORR of 28.6% (95% CI, 16.58–43.26) [Gervais et al. 2013]. For patients with poor performance status, pemetrexed alone was compared with the combination of pemetrexed with carboplatin and OS was improved with the combination regimen (5.3 versus 9.3 months respectively, HR = 0.62; 95% CI, 0.46–0.83; p = 0.001) [Zukin et al. 2013]. Furthermore, the combination of pemetrexed with cisplatin was shown to be effective for the treatment of patients with asymptomatic brain metastasis (ORR = 34.9%) [Ortuzar et al. 2012].
Combinations with targeted therapies
Several targeted therapies were investigated in combination with pemetrexed and platinum for first-line treatment of nonsquamous NSCLC. Bevacizumab is the only antiangiogenic treatment approved for first-line treatment of selected nonsquamous NSCLC patients in association with platinum and pemetrexed [Spigel et al. 2012; Patel et al. 2009], and showed a comparable efficacy and safety profile for elderly patients [Dy et al. 2014]. Other antiangiogenic therapies such as ramucirumab (ORR = 49.3%) [Doebele et al. 2015], pazopanib (ORR = 23%) [Scagliotti et al. 2013], aflibercept (ORR = 26%) [Chen et al. 2014] and axitinib (ORR = 45.5%) [Belani et al. 2014] showed some clinical activity in combination with cisplatin and pemetrexed for first-line treatment of nonsquamous NSCLC. However, pazopanib and aflibercept showed unacceptable levels of toxicities.
Phase II studies also investigated enzastaurin, a protein kinase Cβ inhibitor, in combination with cisplatin and pemetrexed. Enzastaurin did not improve survival (OS = 7.2 versus 12.7 months with cisplatin plus pemetrexed, p = 0.05) [Casey et al. 2010].
Finally, pemetrexed has been studied in combination with anti-EGFR targeted therapies. Cetuximab showed an ORR of 38.5%, a PFS of 5.8 months and a 1-year survival rate of 45% in a single-arm phase II study [Schmid-Bindert et al. 2013]. However, the phase III INSPIRE study did not show any additional survival improvement due to the addition of necitumumab to chemotherapy with cisplatin–pemetrexed in comparison with chemotherapy alone (OS = 11.3 and 11.5 months respectively; HR = 1·01; 95% CI, 0.84–1.21; p = 0·96) [Paz-Ares et al. 2015].
Maintenance therapy
Pemetrexed was studied as continuation maintenance after pemetrexed and platinum-based first-line chemotherapy. A randomized phase II study of pemetrexed versus placebo after first-line chemotherapy with cisplatin–pemetrexed indeed showed promising results in terms of PFS [Mubarak et al. 2012]. A phase III study was then conducted and showed an improvement with pemetrexed in comparison with placebo regarding PFS (4.1 versus 2.8 months respectively; HR = 0.62; 95% CI, 0.49–0.79; p < 0.0001) [Paz-Ares et al. 2012] and OS (13.9 versus 11.0 months respectively; HR = 0.78; 95% CI, 0.64–0.96; p = 0.0195) [Paz-Ares et al. 2013]. The quality of life during maintenance therapy was similar in both arms except for an increased loss of appetite and a delayed worsening of pain and hemoptysis in the pemetrexed arm [Belani et al. 2012].
Furthermore, for patients receiving first-line treatment with cisplatin, pemetrexed and bevacizumab, maintenance therapy with pemetrexed and bevacizumab was compared with bevacizumab alone. The combination increased PFS (7.4 versus 3.7 respectively; HR = 0.57; 95% CI, 0.44–0.75; p < 0.001) [Barlesi et al. 2013]. However, there was a trend but no significant difference for OS between the combination of pemetrexed plus bevacizumab and bevacizumab alone (17.6 versus 13.2 months respectively; HR = 0.87; 95% CI, 0.63–1.21; p = 0.29) [Barlesi et al. 2014]. Notably, the addition of pemetrexed did not deteriorate quality of life [Rittmeyer et al. 2013].
Finally, following first-line chemotherapy with carboplatin, pemetrexed and bevacizumab, a study compared maintenance by pemetrexed plus bevacizumab versus paclitaxel plus bevacizumab. The efficacy was similar in both arms in terms of PFS (6.0 versus 5.6 months respectively, p = 0.12) and OS (12.6 versus 13.4 months respectively, p = 0.949) [Patel et al. 2013].
Second- and third-line treatment
Pemetrexed monotherapy
Pemetrexed monotherapy was approved as second- or third-line treatment of nonsquamous NSCLC on the basis of a phase III study of pemetrexed alone in comparison with docetaxel alone [Hanna et al. 2004]. There was no significant difference in terms of median PFS (2.9 and 2.9 months, respectively; HR = 0.97; 95% CI, 0.82–1.16) or median survival time (8.3 and 7.9 months, respectively; HR = 0.99; 95% CI, 0.80–1.20; p = 0.226) [Hanna et al. 2004]. A few years later, Cullen and colleagues compared two different doses of pemetrexed (500 and 900 mg/m2). As the higher dose did not improve efficacy, 500 mg/m2 remains the recommended dose of pemetrexed [Cullen et al. 2008]. It has also been proven that second-line pemetrexed efficacy was not influenced by maintenance therapy with gemcitabine continuation or switch maintenance with erlotinib [Bylicki et al. 2013]. Pemetrexed was also compared with gefitinib in an Asian population of EGFR wild-type nonsquamous NSCLC with a significant improvement in PFS for pemetrexed (4.8 versus 1.6 months, p < 0.001) [Zhou et al. 2014]. However, in comparison with erlotinib there was no significant difference in terms of TTP (p = 0.195), ORR (p = 0.469) or OS (p = 0.986) [Karampeazis et al. 2013].
Combination of pemetrexed with chemotherapy
Pemetrexed was also investigated in combination with other drugs in pretreated patients with NSCLC. In this setting, the addition of carboplatin to pemetrexed was compared with pemetrexed alone in several phase II trials. Although this combination improved TTP (4.2 versus 2.8 months, respectively; p = 0.005), it did not improve survival (HR for OS = 0.90, 95% CI, 0.74–1.10) [Ardizzoni et al. 2012]. More recently, pemetrexed was studied in combination with other cytotoxic chemotherapies such as eribulin, but those kinds of combinations did not provide any therapeutic advantage: PFS was 21.4 weeks in the eribulin–cisplatin arm versus 23.4 weeks in the pemetrexed alone arm (HR = 1; 95% CI, 0.6–1.7) [Waller et al. 2015].
Combination of pemetrexed with targeted therapies
Pemetrexed was studied in combination with antiangiogenic therapies such as bevacizumab [Adjei et al. 2010], vandetanib [de Boer et al. 2011] or sunitinib [Heist et al. 2014]. None of these studies met their primary endpoint. A phase I trial also studied the combination pemetrexed and nintedanib, and showed one complete response and 50% stable disease among 26 patients treated [Ellis et al. 2010]. In the same way, several anti-EGFR-targeted therapies were studied in combination with pemetrexed in comparison with pemetrexed alone for second- or third-line treatment of nonsquamous NSCLC patients. The monoclonal antibodies cetuximab and matuzumab did not improve patients’ clinical outcomes, with a median survival of 42 weeks with cetuximab, 5.9 months with matuzumab every 3 weeks and 12.4 months with weekly matuzumab [Jalal et al. 2009; Schiller et al. 2010]. However, the addition of the tyrosine kinase inhibitor, erlotinib, to pemetrexed improved PFS in phase II trials in comparison with pemetrexed alone (3.2 versus 2.9 months, p = 0.005), but increased grade 3 and 4 toxicities [Dittrich et al. 2014]. In the subgroup of EGFR wild-type patients, the addition of erlotinib to pemetrexed did not improve its efficacy, with an ORR of 11.1% [Minami et al. 2013].
Several other drugs, such as gadolinium [Edelman et al. 2011], itraconazole [Rudin et al. 2013], enzastaurin [Chiappori et al. 2010] and bortezomib [Scagliotti et al. 2010] were studied in combination with pemetrexed for pretreated nonsquamous NSCLC patients. However, none of them improved efficacy in comparison with pemetrexed alone.
Safety and tolerability
Myelosuppression was the predominant dose-limiting toxicity of pemetrexed reported in phase I trials [McDonald et al. 1998]. As a correlation has been established between poor folate and increased toxicity to pemetrexed, folic acid and vitamin B12 supplementation is recommended during pemetrexed treatment [Niyikiza et al. 2002].
Furthermore, safety and tolerability were assessed in several phase III studies (Table 2). Scagliotti and colleagues showed that survival without any grade 3 or 4 drug-related adverse event was significantly higher with cisplatin–pemetrexed in comparison with cisplatin–gemcitabine (HR = 0.70; 95% CI, 0.63–0.78; p<0.001) [Scagliotti et al. 2009]. In the same way, Gronberg and colleagues found more grade 3 and 4 adverse events with carboplatin–gemcitabine than with carboplatin–pemetrexed [Grønberg et al. 2009]. However, health-related quality of life was not significantly different between the two arms (7.0 versus 7.3 months respectively, p = 0.63). In the second-line setting, Hanna and colleagues reported more neutropenia (40.2% versus 5.3%, p < 0.001), febrile neutropenia (12.7% versus 1.9%, p < 0.001) and hospital admission for other drug-related adverse events (10.5% versus 6.4%, p < 0.092) with docetaxel in comparison with pemetrexed [Hanna et al. 2004]. In addition, Pujol and colleagues demonstrated a significantly longer survival without grade 3 or 4 toxicity with pemetrexed in comparison with docetaxel (HR = 0.60; 95% CI, 0.50–0.72) [Pujol et al. 2007].
Grade 3 and 4 toxicities reported in phase III studies.

NA, not applicable.
Predictive biomarkers
As mentioned above, the benefit of pemetrexed has been demonstrated in nonsquamous NSCLC and not in squamous NSCLC [Syrigos et al. 2010].
Several molecular biomarkers have been investigated for the prediction of response to pemetrexed but none has been approved. It has first been suggested that a low level of TS expression could be responsible for a better sensitivity to pemetrexed. Several retrospective and prospective studies showed that a low TS level was associated with a better PFS for patients treated with pemetrexed [Lee et al. 2013]. However, since all patients were treated with pemetrexed in these studies, it was not possible to assess if the role of the TS expression level was prognostic or predictive. Moreover, Gronberg and colleagues also found that a low TS expression level was associated with a longer OS (9.7 versus 6.2 months, p < 0.001), but this effect was the same for patients treated with carboplatin plus pemetrexed and carboplatin plus gemcitabine, suggesting a prognostic role of the TS level more than a predictive role [Grønberg et al. 2013]. More recently, Chamizo and colleagues found that a low TS expression level was associated with higher response rates to pemetrexed (29% versus 3% in patients with TS overexpression, p = 0.025) [Chamizo et al. 2015]. Sun and colleagues also showed that cisplatin plus pemetrexed was superior to cisplatin plus gemcitabine in TS-positive patients (ORR = 40% and 39%, respectively) but not in TS-negative patients (ORR = 47% and 21%, respectively, interaction p = 0.0084) [Sun et al. 2015], finally suggesting a predictive role of TS expression. As the results of these studies are inconsistent, there is a need for further predictive studies to confirm the predictive role of TS expression for response to pemetrexed therapy. Moreover, in a phase I study of pemetrexed and lapatinib for second-line treatment of advanced NSCLC, a high level of cell-free TS RNA was associated with poorer outcomes [Ramlau et al. 2015].
Furthermore, Fennell and colleagues conducted an exploratory study of gene-expression profiling and found nine genes related to TS expression and associated with PFS and OS of patients treated with pemetrexed in a phase II trial of pemetrexed maintenance [Fennell et al. 2014]. Other studies suggested that TS gene polymorphism could be associated with PFS of patients receiving pemetrexed [Krawczyk et al. 2014]. Finally, ALK fusions were investigated as a potential predictive biomarker of pemetrexed efficacy. EML4-ALK rearrangements were indeed shown to be associated with low TS-mRNA expression [Xu et al. 2015]. PFS was not statistically different in ALK-positive and ALK-negative patients [Shaw et al. 2013].
Perspectives
During the last decade, the place of pemetrexed for the treatment of nonsquamous NSCLC became established. More recently, the development of new therapeutic options such as targeted therapies or immunotherapy modified the use of pemetrexed. However, pemetrexed remains a key drug for the treatment of patients with advanced nonsquamous NSCLC because of its good efficacy and tolerability profile. Further development of the drug relies on combinations of pemetrexed with other drugs or on the extension of pemetrexed use to early-stage or locally advanced diseases. More than 400 clinical trials are currently investigating pemetrexed for the treatment of advanced lung cancer patients (www.clinicaltrials.gov). Among these trials, 132 are still recruiting patients. Most of them are studying the combination of pemetrexed with other chemotherapies, targeted therapies, or immunotherapies.
However, it was shown that incremental costs per life-year gained for first-line treatment were US$148,994 for cisplatin plus pemetrexed induction in comparison with cisplatin plus gemcitabine followed by erlotinib maintenance, and US$191,270 for cisplatin plus pemetrexed followed by pemetrexed maintenance in comparison with cisplatin plus pemetrexed induction only [Kumar et al. 2015]. Further comparative cost-effectiveness studies are required to efficiently use the pemetrexed. To date, these data by themselves should not limit the use of pemetrexed and must be integrated into the cost-effectiveness assessment of all new treatment options, such as targeted therapies and immunotherapies.
Conclusion
Pemetrexed has become one of the most frequently prescribed chemotherapeutic agents for advanced nonsquamous NSCLC treatment. It is now approved for first-line, maintenance and second or third-line treatment of nonsquamous NSCLC and is generally well tolerated, with few grade 3 and 4 toxicities. Several biomarkers, such as TS expression, have been investigated as predictive biomarkers of pemetrexed efficacy. However, all biomarkers to date have failed to demonstrate any predictive role. Finally, hundreds of clinical trials of pemetrexed for NSCLC treatment are still ongoing in order to extend the development of the drug.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.