
Abstract
Aromatase inhibitors (AIs) are routinely used in the adjuvant treatment of women with hormone receptor-positive early breast cancer. Patients who receive AIs have an increased risk of bone loss and arthralgia compared with those treated with tamoxifen. In addition to the effects of AIs, the population of women with early breast cancer has a high prevalence of 25-hydroxyvitamin D (25(OH)D) insufficiency. In our experience 88% of patients had concentrations lower than 30 ng/ml. Vitamin D supplementation should be adapted to the baseline concentration. Another relevant finding in our research program was the close relationship between 25(OH)D levels and intensity of AI-related arthralgia (AIrA). A target concentration of 40 ng/ml 25(OH)D may prevent development of AIrA. We also demonstrate that AIrA is genetically determined: single nucleotide polymorphisms located in genes encoding key factors for the metabolism of estrogens and vitamin D (CYP17A1, VDR, and CYP27B1) are associated with self-reported arthralgia during AI therapy. We recommend establishing an individualized protocol of bone-health surveillance based on baseline and evolutionary clinical variables.
Introduction
The use of adjuvant endocrine therapy for treatment of early-stage, hormone receptor-positive breast cancer has resulted in noteworthy improvements in disease-free and overall survival [Davies et al. 2011]. The initial large randomized clinical trials of adjuvant endocrine therapy did not report high treatment discontinuation rates [Early Breast Cancer Trialists Collaborative Group, 2005; Eiermann et al. 2001]. However, clinical practice observational studies have revealed much higher rates of treatment discontinuation. Variables associated with poor adherence to chronic oral medications include patient age, comorbidities, cost, and basically toxicity [Font et al. 2012].
Several studies have identified musculoskeletal toxicity as the most frequent cause for treatment discontinuation [Henry et al. 2012; Hadji et al. 2014].
Several antineoplastic drugs could have a negative impact on bone health. Androgen- deprivation therapy is a classic example in prostate-cancer cases, and aromatase inhibitors (AIs) are probably the most paradigmatic group of drugs with potential skeletal adverse events in breast cancer.
AIs have been routinely used in the adjuvant treatment of postmenopausal women with hormone receptor-positive early breast cancer since 2005 as a consequence of the significant benefit in disease-free survival when compared with tamoxifen [Howell et al. 2005; Thürlimann et al. 2005; Coates et al. 2007; Coombes et al. 2004].
Patients who receive AIs have an increased risk of bone loss and arthralgia compared with those treated with tamoxifen. The mechanism for the accelerated bone loss is thought to be, at least in part, profound suppression of estrogen synthesis; the end result is increased osteoclast activation and net bone resorption. In addition to the effects of AIs, the population of women with early breast cancer has a high prevalence of vitamin D insufficiency. Vitamin D plays an essential role in calcium homeostasis and bone metabolism. The importance of optimal plasma concentration of 25-hydroxyvitamin D (25(OH)D) for several health outcomes is addressed in a recent meta-analysis by Bischoff-Ferrari and colleagues, which suggests 30 ng/ml (75 nmol/l) as the serum concentration required to prevent increases in parathormone bone loss, and osteoporotic fractures [Bischoff-Ferrari et al. 2006]. Furthermore, maintenance of optimal levels of 25(OH)D is strongly recommended in the general population to prevent not only bone loss but also problems involving muscles, teeth, bone fractures, and risk of falls, as well as risk of breast and colorectal cancers [Vieth et al. 2007].
We are currently conducting a prospective, nonselected cohort study to investigate bone health, that is, bone mineral density (BMD), fractures occurrence, and vitamin D concentrations, in postmenopausal women treated for early breast cancer with adjuvant AI therapy. The main aim is to provide data from actual practice to establish the potential role of various assessments and interventions to correctly evaluate and reduce the impact of AI therapy on osteoarticular toxicity.
In this article, we will summarize some of our previously published results and also update the most relevant baseline data of our cohort.
Patients and methods
From January 2006 to December 2014, postmenopausal women with early breast cancer, candidates for AI treatment, and attending the outpatient breast cancer unit, were consecutively invited to participate in the trial and, after signing informed consent, were included in the study. Some of the participants had received tamoxifen for 2–5 years (switch group), and others had AIs as initial therapy (upfront group).
Patients with a history of any bone disease, rheumatoid arthritis, metabolic or endocrine diseases, prior diagnosis of Paget’s bone disease or osteomalacia, concurrent or previous treatment with bisphosphonates, oral corticosteroids, or any other bone-active drugs were excluded.
At the time of the present analysis we included 687 patients (840 patients were recruited and 153 were excluded).
Measurements
Plasma concentrations of 25(OH)D were determined at baseline before AI treatment was started and at 3 months after AIs were initiated, and will be determined annually, using competitive immunoluminometric direct assay with direct-coated magnetic microparticles (DiaSorin Iberia SA, Madrid, Spain).
BMD was measured at the lumbar spine (LS) L2–L4, femoral neck (FN), and total hip (TH) using the dual-energy X-ray densitometer QDR4500 SL® (Hologic, Waltham, MA, USA), following the usual protocol in our bone metabolism unit. In our department, the technique has an in vivo coefficient of variation of 1.0% for LS, 1.65% for FN, and 1.60% for TH measurements. BMD was assessed at baseline and will be repeated at 12 months and then annually, according to the study protocol [Nogues et al. 2010; Servitja et al. 2012].
Spine and nonvertebral fractures including previous nonfragility fractures, height decrease, and back pain were recorded. Thoracic and LS X-rays were performed to assess spine fractures at baseline in all participants. Spine fractures were defined according to Genant and colleagues [Genant et al. 1993].
Calcium daily intake was estimated using a weekly food intake frequency questionnaire, validated for the Spanish population [Orozco et al. 2004]. Previous treatment with calcium supplements was also recorded.
The following variables were recorded: current age, age at menarche and at menopause, weight, height, lactation, parity, and smoking status.
Interventions
All of the women included in the study received calcium and vitamin D oral supplements (1000 mg and 800 IU, daily); women with baseline vitamin D deficiency (plasma levels < 30 ng/ml) were prescribed an additional oral 16,000 IU of vitamin D (cholecalciferol, Hidroferol®, Faes Farma, Leioa, Spain) every 2 weeks. Moreover, patients were stratified by LS-BMD, FN-BMD, and TH-BMD and assigned to the corresponding therapeutic regimen. Patients with osteoporosis (t-score < –2.5) or osteopenia (t-score < –2.0) at any site plus one major risk factor or previous osteoporosis fragility fractures received bisphosphonates and 1000 mg of calcium plus 800 IU vitamin D. Patients with normal BMD or t-score > –2.0 at any site and no major risk factor received calcium and vitamin D only (Figure 1).

Treatment with vitamin D supplements (0.266 mg/16,000 IU) if baseline 25-hydroxyvitamin D is less than 30 ng/ml. BP, bisphosphonate; FxOP, osteoporotic fracture; OP, osteoporosis; RF, fracture risk.
BMD measurement should not be the only criterion for determining fracture risk. The World Health Organization fracture risk assessment tool algorithm is valid for postmenopausal women and calculates the 10-year fracture risk with or without BMD measurement and includes several fracture-related risk factors [World Health Organization Collaborating Centre for Metabolic Bone Diseases, University of Sheffield. http://www.shef.ac.uk/FRAX].
Results
Baseline characteristics of the patient population are shown in Table 1. Basal concentrations (mean ± standard deviation) of 25(OH)D in the whole studied population were 17.85 ng/ml ± 10.27 (range 4.0–76.3). Only 10% had normal 25(OH)D concentrations, as defined by > 30 ng/ml. Vitamin D insufficiency (concentrations < 30 ng/ml) was observed in 90% of the women (Figure 2) [Nogues et al. 2010; Servitja et al. 2012]. At baseline, 26% of the women had a normal BMD, 53.7% had osteopenia, and 19.4% had osteoporosis (Figure 3).
Baseline patient characteristics.

BP, bisphosphonate treatment; IQ, interquartile range; SD, standard deviation.
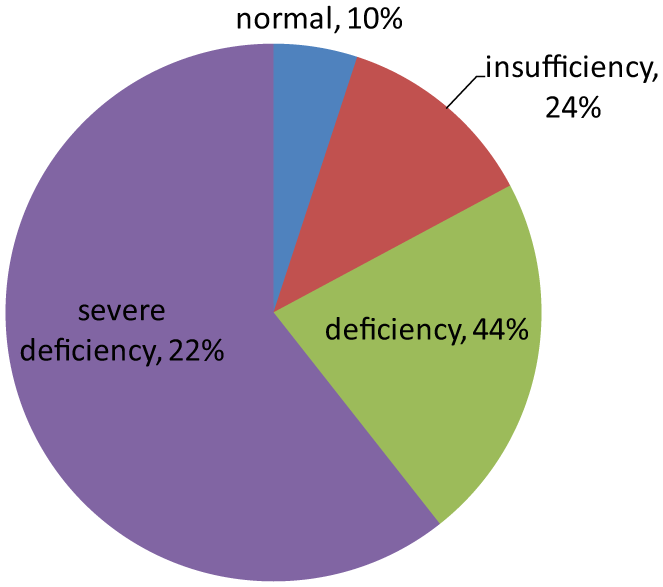
Vitamin D level at baseline.

Baseline BMD according to WHO (’94) criteria.
The implementation of individualized vitamin D supplementation achieved normal levels in half of our patients in less than 3 months, and those patients who achieved concentrations greater than 30 ng/ml experienced significantly less bone loss than those women who did not reach 25(OH)D normal concentrations (Figure 4).We conclude that improved vitamin D status using supplementation is associated with attenuation of AI-associated bone loss [Prieto-Alhambra et al. 2012].

Relationship between vitamin D levels at 3 months and BMD loss at 1 year.
Arthromyalgia has probably a multifactorial etiology and includes different symptoms such as fatigue, pain, anxiety, and depression. As a consequence of this wide cluster of potential causes, this issue has been addressed by different therapeutic options (e.g. duloxetine, testosterone, omega 3 fatty acid, exercise, acupuncture, and vitamin D). Several ongoing trials are testing the efficacy of these treatments in clinical practice.
A relevant finding in our research program was the description of a close relationship between 25(OH)D levels and the intensity of AI-related arthralgia (AIrA). In the whole cohort, those with a higher 25(OH)D had a reduced increase in joint pain visual analog scale (VAS) and this was significant in the 30 ng/ml and 40 ng/ml thresholds. In those without joint pain at baseline, incident joint pain was significantly less likely in patients with a 3-month 25(OH)D treatment of 40 ng/ml or higher (adjusted p = 0.003). Among the 80 cases without pain at baseline, 25 (53.2%) with 3-month 25(OH)D concentrations of less than 40 ng/ml developed incident pain, compared with only 7/33 (21.2%) of those with concentrations equal or greater than 40 ng/ml (p = 0.008). Stratification by season when the 3 month sample was drawn did not change these results. Therefore a target concentration of 40 ng/ml 25(OH)D may prevent the development of AIrA, but higher loading doses are required to attain this level in women with deficiency at baseline [Prieto-Alhambra et al. 2011]. Other studies also described the relationship between low levels of 25(OH)D and high probability of AIrA [Rastelli et al. 2011; Khan et al. 2012].
We also demonstrated that genetic variants in the CYP17A1, VDR, and CYP27B1 genes lead to an association with the risk of AIrA. An additive effect of the unfavorable alleles for rs4646536 (CYP27B1) and rs6163 (CYP17A1) on pain intensity was observed: participants with four unfavorable alleles (13.54% and 13.59% at 3 and 12 months, respectively) had an average increase of two points on the VAS scale compared with those with only one unfavorable allele (8.61% and 8.97% at 3 and 12 months, respectively) (p < 0.001). An additive effect was also observed with worsening pain for participants with four unfavorable alleles: odds ratio (OR) 3.88 (1.42–11.12) (p < 0.01) at 3 months and OR 5.27 (1.81–16.44) (p < 0.001) at 12 months. The determination of these single nucleotide polymorphisms (SNPs), located in genes encoding key factors for the metabolism of estrogens and vitamin D, could be useful in clinical practice to identify women at high risk of AIrA and therapy discontinuation, who could then be targeted for higher dose vitamin D supplementation and/or monitoring strategies to improve quality of life and compliance [Garcia-Giralt et al. 2013].
In our experience, baseline vitamin D concentrations were not significantly related to bone loss. By contrast, vitamin D after 3 months of supplementation was inversely correlated to LS bone loss at 1 year follow up, independently of baseline 25(OH)D concentrations and of initial BMD. In addition, patients who reached a threshold of 25(OH)D 40 ng/ml or higher at 3 months had a significant reduction of 1.7% (almost half standard deviation according to our data) in bone-loss rates compared with those who stayed at vitamin D serum levels lower than 30 ng/ml. Vitamin D increments at 3 months were also inversely correlated to bone-loss rates at LS: each 10 ng/ml increase in vitamin D translated into a 0.6% bone-loss reduction (Figure 4) [Prieto-Alhambra et al. 2012].
Vitamin D status has been related to BMD, and most of the trials and available meta-analyses have shown that vitamin D supplementation is protective against fractures [Bischoff-Ferrari et al. 2009], and falls [Sanders et al. 2010]. In our cohort, with 47 months of follow up, the incident fracture rate was 6%. This low rate of fractures could be explained by the intensive intervention on bone health, but we need more follow up to establish the direct association.
Summary and recommendations
If we consider the high rate of osteoporosis and osteopenia at baseline, it is necessary to establish a comprehensive risk assessment of bone fragility and adapt accordingly the antiresortive strategy to the risk category.
Our data suggest a high prevalence of commonly unrecognized vitamin D deficiency in postmenopausal women with early breast cancer treated with AIs, a known osteopenic group of drugs. Our results support the need for a routine assessment of 25(OH)D levels and, when necessary, supplementation in these patients.
Vitamin D supplementation should be adapted to baseline concentration (high dose of cholecalciferol when 25(OH)D deficiency). Correcting 25(OH)D levels leads to a reduction of arthralgia intensity. Identify women at high-risk of AIrA (SNPs in CYP17A1, VDR and CYP27B1). Select these patients for close monitoring and offer strategies to avoid AI discontinuation.
Our results suggest that vitamin D higher concentrations after 3 months of supplementation are protective for AI-induced bone loss. A target threshold of 40 ng/ml or higher could be recommended for these patients in order to protect them from bone loss.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Spanish Government under projects RD12/0036/0051, PI12/00680; and by the Catalan Government under grant 2014 SRG 740.