
Abstract
Background:
The objective of this study was to review the pharmacology, efficacy, and safety of palbociclib, a first-in-class cyclin-dependent kinase 4/6 inhibitor, for the management of advanced breast cancer (ABC).
Methods:
Pharmacokinetics and drug interactions associated with palbociclib are described. Recent clinical trial data are reviewed, including patient-reported outcomes and subgroup analyses.
Results:
Palbociclib is indicated in combination with an aromatase inhibitor as initial endocrine therapy (ET) or with fulvestrant for patients with disease progression following ET for hormone receptor positive, human epidermal growth factor receptor 2 negative ABC or metastatic breast cancer. Palbociclib inhibits cyclin-dependent kinases 4/6, resulting in a blockade of phosphorylation of the retinoblastoma protein, which hinders the activation of transcription factors involved in S-phase entry, thereby arresting cell cycle progression at G1 phase. The efficacy and safety of palbociclib in combination with ET was established in three randomized trials (PALOMA-1, -2, and -3); all studies met their primary endpoint of significantly prolonging investigator-assessed progression-free survival versus ET alone. Findings were similar in subgroup analyses of the three PALOMA studies. Palbociclib plus ET also maintained health-related quality of life (QoL) compared with ET alone in PALOMA-2 and -3. A long-term safety profile for palbociclib, up to 3 years, has been established. Neutropenia, the most common any-grade and grade 3 or higher adverse event associated with palbociclib, is consistent with the drug’s mechanism of action and can be effectively managed with dose interruption, dose reduction, or delay in starting treatment cycles.
Conclusions:
Palbociclib in combination with ET improved progression-free survival and QoL in patients with ABC, including in several patient subgroups.
Keywords
Introduction
The lifetime incidence rate of female invasive breast cancer in the United States (US) is approximately 12% (one in eight women), and it is estimated that over 266,120 new cases of locally advanced or metastatic breast cancer, collectively referred to from hereon as advanced breast cancer (ABC), will be diagnosed in 2018. 1 Approximately 70% of breast cancer cases are of the luminal subtype or estrogen receptor positive (ER+)/human epidermal growth factor receptor 2 negative (HER2–) 2 and, for some time at least, are typically responsive to endocrine therapy. Sequential endocrine therapy, or endocrine-based therapy [e.g. palbociclib plus letrozole is now a National Comprehensive Cancer Network (NCCN) category 1 option for postmenopausal patients with advanced disease and no prior endocrine therapy within 1 year], is therefore considered the mainstay treatment for premenopausal and postmenopausal patients with de novo or recurrent hormone receptor positive (HR+)/HER2– ABC. 3 Current NCCN guidelines recommend sequential endocrine therapy until three successive endocrine therapy regimens offer no clinical benefit or until symptomatic visceral disease develops. 3 Similarly, the American Society of Clinical Oncology guidelines recommend sequential endocrine treatment, except in the event of immediately life-threatening HR+ ABC. 4 After first-line treatment, preferably with aromatase inhibitors (AIs) in postmenopausal women and tamoxifen or an AI in conjunction with ovarian suppression for premenopausal women without prior exposure to hormone therapy, endocrine agents can be given in any particular order for endocrine-responsive disease. 4
Despite major advances in our understanding of the heterogeneity, biology, and genomics of ABC over the past 2 decades, 2 the median survival rate after diagnosis of HR+ ABC has not exceeded 2–3 years and reflects the correspondingly modest improvement in disease management over the same period. 5 Although endocrine agents are generally well tolerated, resistance to endocrine therapy via various mechanisms is likely to occur over time in cases of ABC.2,6,7 Hence, the addition of a targeted biological therapy to delay the onset of endocrine resistance and disease progression has emerged as an innovative and promising treatment option. 7 This article provides a comprehensive review of the pharmacology, efficacy, and safety of palbociclib, a first-in-class inhibitor of cyclin-dependent kinases (CDK) 4 and 6 indicated for use in combination with endocrine therapy in first-line treatment and as therapy after disease progression on prior endocrine therapy for advanced cancer (an AI and fulvestrant, respectively) in patients with HR+ metastatic breast cancer or ABC.8,9 As of 12 February 2018, palbociclib in combination with endocrine therapy is an approved treatment for ABC in 82 countries; 79 of these countries are approved for the dual indication, including 48 for palbociclib plus AIs and 31 specifically for palbociclib plus letrozole.
Pharmacology
Mechanism of action
Palbociclib is a highly selective inhibitor of CDK 4 and CDK 6 that has been approved by the US Food and Drug Administration (FDA) to treat HR+/HER2− ABC in combination with endocrine therapy. 8 These two serine/threonine family kinases are part of the cyclin D–CDK 4/6–INK4–retinoblastoma protein (pRb) signaling pathway downstream of numerous mitogenic cascades.10–12 When this signaling pathway is affected by various genetic or molecular perturbations, including but not limited to cyclin D overexpression, CCND1 amplification, the loss of function of pRb, or the tumor suppressor p16 (CDKN2A loss),13,14 CDK 4/6 activation is implicated in the cellular dysregulation that is characteristic of malignant breast cancer cells. The CDK 4/6 inhibitory activity of palbociclib leads to reduced pRb phosphorylation at serine residues 780 and 795 in Rb+ cells. 11 In vitro, inhibition of pRb phosphorylation starts 4 h after exposure, is maximal at 16 h, and can be reversed after palbociclib is removed. 11 Hypophosphorylation of pRb hinders activation of the transcription factors necessary for S-phase entry, thus arresting cell cycle progression at the G1 phase and preventing DNA synthesis required for cellular replication and the unrestricted proliferation of malignant cells 15 (Figure S1).
Differential cellular effects
Human breast cancer cells that are ER+ or HER2 amplified with luminal features have thus far proven to be most sensitive to the CDK 4/6 inhibitory effects of palbociclib.10,16 At clinically relevant concentrations, palbociclib has been shown to induce cellular senescence or the irreversible arrest of cell proliferation 17 in MCF-7 breast cancer cell lines that are ER+. 18 In a mechanistic study of palbociclib in combination with the antiestrogen treatment fulvestrant, which can also induce senescence, the senescence effect became additive, and cellular proliferation remained arrested with only a partial recovery occurring 5 days after the combined treatment was withdrawn.17,18 In contrast, the effect of the same treatment was quite different in human bone marrow mononuclear cells that became pharmacologically quiescent (i.e. transiently arrested) rather than senescent when treated with palbociclib alone or palbociclib plus fulvestrant. 18 Because of this differential effect of treatment on bone marrow cells compared with breast tumor cells, the potential exists to reverse hematologic toxicities associated with exposure to palbociclib. 18 Furthermore, this treatment effect differentiates the cytostatic effect of palbociclib combined with endocrine therapy from the usual cytotoxic effects of chemotherapeutic agents on bone marrow progenitor cells leading to apoptosis.13,18,19
Pharmacokinetics
Palbociclib is rapidly absorbed and detectable in the plasma of patients with Rb-positive solid tumors or non-Hodgkin lymphoma within 1 h of its oral administration20,21 and is metabolized in the liver. 8 In patients with solid tumors, including ABC, and in healthy patients, the time to peak concentration ranges from 6 to 12 h. 8 Mean absolute bioavailability of palbociclib after a 125 mg dose was 46%, and the pharmacokinetics are linear, with exposure that increases proportionally with dose. 8 Following repeated once-daily dosing of palbociclib, a steady state was achieved within 8 days, and the median accumulation ratio reached 2.4 (range 1.5–4.2). 8 In patients with ABC, the mean elimination half life was 29 ± 5 h, and the geometric mean apparent oral clearance was 63.1 liters/h (29% coefficient variation). 8
An exposure–response analysis was recently conducted using data from PALOMA-2 to assess the effect of changes in palbociclib exposure (due to dose modification) on progression-free survival (PFS) in patients with HR+/HER2− ABC. 22 Patients in the palbociclib (125 mg once daily/3 weeks on/1 week off schedule) plus letrozole (2.5 mg once daily continuously) cohort were divided into four quantiles (Q1, Q2, Q3, and Q4) based on their palbociclib exposure. 22 The median PFS was similar in each quantile (24.9, 27.7, 25.7, and 24.0 months for Q1, Q2, Q3, and Q4, respectively) and substantially higher than the letrozole-only cohort (14.5 months), indicating that PFS duration was not associated with palbociclib exposure. 22 The results suggest that patients who had different exposure to palbociclib benefited similarly and that the dose reduction algorithm implemented in PALOMA-2 effectively managed palbociclib toxicity without significantly affecting efficacy.
Drug interactions
The oxidative metabolism of palbociclib is primarily mediated by cytochrome P-450 (CYP) 3A. 8 Thus, a number of medications 8 and foods, including grapefruit products, 23 which are CYP3A inhibitors, may interact with palbociclib.8,24 When multiple 200 mg doses of itraconazole, a strong CYP3A inhibitor, were coadministered with palbociclib, palbociclib exposure was markedly increased. 25 Although palbociclib was well tolerated, its peak concentration increased by 34%, and the area under the plasma concentration–time curve from time zero to infinity increased by 87% relative to a single 125 mg dose of palbociclib alone, which necessitates a palbociclib dose reduction to 75 mg if coadministration with strong CYP3A inhibitors is unavoidable.8,25 In contrast, moderate to strong CYP3A inducers can decrease the concentration of circulating palbociclib. 24 Concurrent administration of palbociclib with other drugs that are also CYP3A4 substrates (i.e. metabolized by CYP3A) may necessitate dose reductions of these substrates, especially those with a narrow therapeutic index, to avoid increased plasma concentrations of these agents. 24 The coadministration of acid-reducing agents, such as the proton pump inhibitor rabeprazole, can substantially decrease palbociclib exposure in a fasted state, but this effect is mitigated by food.8,26 Therefore, coadministration with acid-reducing agents is not thought to have any significant effect on palbociclib absorption when taken with food, as recommended. Although exposure to a single oral dose of palbociclib modestly increases in the fed state, its administration with food is recommended to avoid the variability in absorption that was observed in a small subset of patients dosed in a fasted state.8,27
Based on clinical trial data, no clinically relevant drug–drug interactions have been reported when palbociclib has been coadministered with letrozole,16,28 fulvestrant, or the luteinizing hormone releasing-hormone agonist goserelin.8,29
Clinical efficacy of palbociclib
Dosing
Palbociclib is taken orally with food, once daily (preferably at approximately the same time of day) for 3 weeks, followed by 1 week off treatment (i.e. a 3/1 schedule). Palbociclib is given in combination with either an AI or fulvestrant. 8 The recommended starting dose of palbociclib is 125 mg, and the available capsule strengths are 125 mg, 100 mg, and 75 mg to allow for dose reductions as necessary. 8 Palbociclib should be swallowed as a whole capsule and never be chewed, crushed, or ingested if capsules are broken, cracked, or otherwise not intact. 8
Efficacy
The efficacy of palbociclib in combination with endocrine therapy as a treatment for ABC has been established in several clinical trials.19,30–33 Three randomized studies (phase II, PALOMA-1; 19 phase III, PALOMA-2 and -330–32) enrolled women with HR+/HER2− ABC. The PALOMA-1 and -2 trials included postmenopausal women who were naive to systemic treatment for advanced disease, whereas the PALOMA-3 trial included pre- or perimenopausal and postmenopausal women whose disease had progressed on prior endocrine therapy in the adjuvant or metastatic setting.19,30–32 All three PALOMA studies met their primary endpoint of significantly prolonged investigator-assessed PFS compared with endocrine monotherapy according to the Response Evaluation Criteria in Solid Tumors (RECIST version 1.0 or 1.1). Key study design attributes and a trial efficacy summary are depicted in Table 1.19,30,31 At the time of the final analysis, patients in the palbociclib plus letrozole arms of the PALOMA-1 and -2 studies had achieved a significantly greater median PFS compared with that of patients receiving letrozole alone [PALOMA-1, 20.2 versus 10.2 months, respectively; hazard ratio (HR) 0.49; 95% confidence interval (CI) 0.32−0.75; PALOMA-2, 24.8 versus 14.5 months; HR 0.58; 95% CI 0.46−0.72].19,31 In the PALOMA-3 study, median PFS in the palbociclib plus fulvestrant group was significantly longer than that in the placebo plus fulvestrant group (9.5 versus 4.6 months, respectively; HR 0.46; 95% CI 0.36−0.59) (Table 1). After an updated analysis with longer follow up (through 23 October 2015) in the PALOMA-3 study, median PFS was 11.2 versus 4.6 months in the palbociclib plus fulvestrant versus placebo plus fulvestrant groups, respectively (HR 0.50; 95% CI 0.40−0.62; one-sided p < 0.0001). 34 Similarly, in an updated analysis of the PALOMA-2 study, palbociclib plus letrozole was shown to consistently improve median PFS compared with placebo plus letrozole in the overall population (27.6 versus 14.5 months, respectively), as well as across patient subgroups, after approximately 37 months of follow up (data cutoff: 31 May 2017). 35
Key aspects and findings of the PALOMA studies.

Patients with measurable disease.
Updated analysis available with a data cutoff date of 31 May 2017. 35
±Goserelin, dependent on menopausal status in both treatment arms.
Clinical benefit response = complete response plus partial response plus stable disease ⩾24 weeks.
Measurable disease was defined according to RECIST version 1.0 (PALOMA-1) and version 1.1 (PALOMA-2 and -3).
ABC, advanced breast cancer; CBR, clinical benefit rate; CI, confidence interval; ER+, estrogen receptor positive; HER2−, human epidermal growth factor receptor 2 negative; HR, hazard ratio; mBC, metastatic breast cancer; N/A, not available; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; RECIST, Response Evaluation Criteria in Solid Tumors.
The efficacy of palbociclib plus endocrine therapy is consistent across various subgroups of patients in the PALOMA-1, -2, and -3 studies.30,35–41 Compared with letrozole alone, palbociclib plus letrozole improved the median PFS and clinical benefit response rate, regardless of age group, histological subtype (ductal carcinoma or lobular), prior neoadjuvant/adjuvant systemic treatment, and site of metastatic disease (bone only, visceral, or distant metastases at other sites); the degree of benefit observed in the subgroups evaluated was consistent with that demonstrated in the overall study population. 36 In PALOMA-3, compared with fulvestrant alone, palbociclib plus fulvestrant improved median PFS regardless of menopausal status, the number of disease sites, the site of metastatic disease, and previous chemotherapy. 30 Additionally, based on an analysis of patients from PALOMA-2 and PALOMA-3, palbociclib plus endocrine therapy improved the median PFS compared with endocrine therapy alone in patients with and without visceral metastases. 42 The PALOMA-3 trial assessed the effect of two gene mutations on outcomes. Irrespective of ESR1 mutation status 37 or PIK3CA mutation status, 30 palbociclib plus fulvestrant demonstrated a longer median PFS compared with fulvestrant alone. More recently explored results for efficacy in subgroups in the PALOMA-2 and -3 studies were presented at the 2017 American Society of Clinical Oncology Annual Meeting and the 2017 Annual San Antonio Breast Cancer Symposium and are summarized in Table 2.35,39–41 Subpopulation treatment effect pattern plot (STEPP) analysis presented at the 2018 American Society of Clinical Oncology Annual Meeting showed that the treatment effect of the addition of palbociclib to endocrine therapy was not impacted by the length of the initial treatment-free interval (TFI; PALOMA-2) or disease-free interval (DFI; PALOMA-3). 43 The median TFI in PALOMA-2 was 37.1 months for palbociclib plus letrozole and 30.9 months for letrozole plus placebo, with approximately 56% of patients having a TFI of over 2 years. 43 The median DFI in PALOMA-3 was 49.2 months for palbociclib plus fulvestrant versus 52.0 months for fulvestrant plus placebo, with over 80% of patients having had a DFI more than 2 years. 43 In addition, patient subgroup analyses of PALOMA-2 showed patients with either a low disease burden or a demonstrated sensitivity to endocrine monotherapy derived substantial PFS benefit from the combination of palbociclib plus letrozole (i.e. >3 years median PFS). 35 Collectively, these findings demonstrate the clinical benefit of adding palbociclib to endocrine therapy for various subgroups of patients with ABC.
Subgroup analyses.

Average concentration of palbociclib over the entire treatment (Cavg) was derived from ADI divided by estimated apparent oral clearance (CL/F) for each patient; Cavg (ng/ml) = [ADI / (CL/F)]/24 h.
Per tumor site.
Protocol-defined DFI refers to DFI since completion of prior (neo)adjuvant therapy and onset of metastatic disease or disease recurrence.
ADI, average daily dose intensity; ASCO, American Society of Clinical Oncology; Cavg, time-independent average daily palbociclib concentration; CI, confidence interval; DFI, disease-free interval; ET, endocrine therapy; HR, hazard ratio; NE, not estimable; NR, not reached; PFS, progression-free survival; SABCS, San Antonio Breast Cancer Symposium.
Of the PALOMA studies, only the PALOMA-1 data have thus far matured for assessment of overall survival (OS). There was no statistically significant survival benefit as a result of adding palbociclib to letrozole versus letrozole monotherapy in PALOMA-1; although, previous analyses have indicated that a longer median survival post progression can dilute an OS comparison and necessitate a larger sample size to sufficiently power the detection of a significant difference in the advanced disease setting (Table 1).44,45
Safety of palbociclib
In a comprehensive long-term safety analysis, safety data from the three PALOMA studies were combined (N = 872 safety population) to characterize the safety profile of palbociclib plus endocrine therapy. 46 Safety evaluations extended beyond the final analysis cutoff dates for the primary endpoints of PFS for PALOMA-1 (2 January 2015) and -3 (31 July 2015) and covered a 3-year period. 46 Among all three PALOMA studies, neutropenia [cluster of preferred terms (PTs), all causalities] was the most commonly reported toxicity (all grade, 75.7% patients) and peaked during the first 6 months of treatment (Figure 1); moreover, mean grade 3–4 neutropenia remained stable over time, indicative of a lack of cumulative toxicity following prolonged palbociclib treatment. 46 Unlike the DNA damage and apoptosis caused by myeloablative and cytotoxic chemotherapeutic agents, which is associated with slower recovery, palbociclib-induced neutropenia arises from the temporary growth arrest (quiescence) of dividing myeloid progenitor cells/neutrophil precursors. Palbociclib growth arrest is rapidly reversible upon removal of the drug. 18 Myelosuppression of this nature can be effectively managed by close monitoring of complete blood counts, particularly early during treatment, 47 and via an established dose modification schema that includes dose interruptions, dose reductions, or a delay in starting treatment cycles (Figure 2), 8 without any negative impact on efficacy. 47 Other safety data have shown no correlation between grade 3–4 neutropenia and serious infections or infections in either the PALOMA-1 or -3 studies, respectively.36,47 Similarly, findings from a single center retrospective study of 344 patients with ER+ metastatic breast cancer who received palbociclib as standard of care showed that dose reductions and delays did not negatively affect PFS. 48
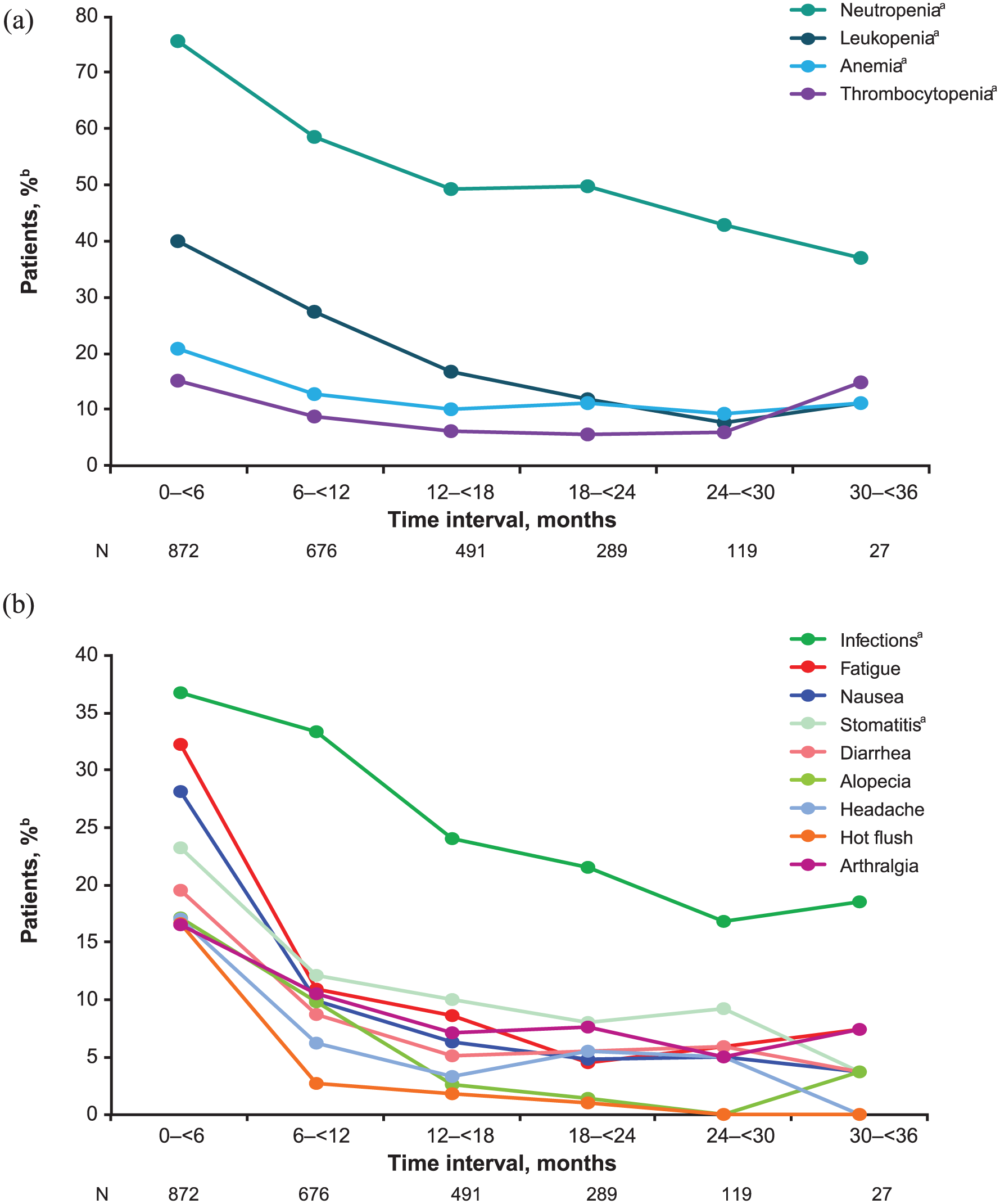
Incidence of (a) hematologic and (b) nonhematologic adverse events pooled from the three PALOMA studies by 6-month treatment intervals. Includes treatment-emergent adverse events of any grade and all causalities occurring in at least 15% of patients treated with palbociclib plus endocrine therapy.

Recommended palbociclib dose modifications for (a) neutropenia and (b) thrombocytopenia. 8 For patients who experience a maximum of grade 1 or 2 neutropenia in the first six cycles, monitor complete blood counts every 3 months in subsequent cycles at the beginning of the cycle and as clinically indicated. Grading according to CTCAE 4.0.
The most common all-grade nonhematologic adverse events associated with palbociclib in the PALOMA pooled safety analysis were infections (36.7% for the cluster of PTs), fatigue (32.2%), nausea (28.1%), and stomatitis (23.2% for the cluster of PTs). The incidence of nonhematologic adverse events associated with palbociclib generally were greatest during the first 6 months of treatment and largely decreased over time (Figure 1).
A thorough study of the effects on QT interval prolongation of any new drugs with systemic bioavailability is recommended by the FDA 49 and is particularly important in patients with cancer who often have several risk factors for cardiac disease and QT prolongation. 50 In a QT substudy of 125 patients in the PALOMA-2 trial, none of the patients in the palbociclib plus letrozole group had a 480 ms or higher maximum postbaseline study-specific correction factor (QTcS) or Frederica’s correction (QTcF) or a 60 ms or higher maximum increase from time-matched baseline QTcS or QTcF.51,52 Moreover, the upper bounds of the one-sided 95% CIs for QTcS, QTcF, and Bazett’s correction at all time points and at maximum steady-state concentration following repeated dosing with palbociclib 125 mg were less than 10 ms.51,52 Thus, palbociclib administered in combination with letrozole at the recommended therapeutic doses had no clinically relevant effect on the QT interval in patients with ABC enrolled in the substudy.
Overall, the long-term safety profile of palbociclib demonstrated by the PALOMA pooled safety analysis was consistent with previously reported safety findings for palbociclib plus endocrine therapy. 46
Patient-reported outcomes
The goal of treatment for patients with ABC is palliative and primarily aimed at maintaining quality of life (QoL) while delaying disease progression and prolonging survival. 6 However, improvements in efficacy as a result of adding additional treatments to a standard noncurative therapeutic regimen should not be accompanied by an increased toxicity burden that causes significant deterioration in the functioning or symptoms for patients. 6 The impact of palbociclib plus letrozole (as first-line therapy for ABC) or palbociclib plus fulvestrant as second-line therapy for patients with disease progression on prior endocrine therapy for advanced disease versus the same respective endocrine monotherapy on patient-reported QoL parameters was assessed in HR+/HER2− patients with ABC in the PALOMA-2 and -3 studies.6,53
In PALOMA-2, patient-reported outcomes (PROs) were assessed in patients previously untreated with systemic therapy for ABC randomized to receive letrozole with or without palbociclib (on day 1 of cycles 2 and 3 and every subsequent alternate cycle from cycle 5 until end of treatment) using the Functional Assessment of Cancer Therapy−Breast (FACT-B) questionnaires, including FACT-General (FACT-G) and the Breast Cancer Subscale. 53 There was no significant difference between palbociclib plus letrozole and letrozole monotherapy in overall change from baseline in FACT-B or FACT-G total scores, despite the longer duration of treatment in the combination arm, and no significant difference in FACT-B health-related QoL (HRQoL) based on FACT-B total scores. These findings suggest palbociclib plus letrozole maintained HRQoL in patients with advanced disease in first-line therapy while prolonging PFS. PROs were also assessed using the Euro-QOL 5 Dimension (EQ-5D) questionnaire, a two-part, self-administered, standardized measure of health status that includes the EQ-5D Index (comprising five dimensions: mobility, self care, usual activities, pain/discomfort, and anxiety/depression) and a visual analog scale (VAS). 54 Results showed that general health status and EQ-5D index scores were maintained from baseline in patients treated with palbociclib plus letrozole with no statistically significant differences between treatment arms. 54
In patients who developed resistance to prior endocrine therapy for advanced disease (PALOMA-3), PROs during treatment were assessed on day 1 of cycles 1–4 and alternate subsequent cycles (starting with cycle 6) using the European Organisation for Research and Treatment of Cancer QoL questionnaire (EORTC QLQ-C30 version 3.0) and its breast cancer module, QLQ-BR23. In the palbociclib plus fulvestrant arm versus the fulvestrant arm, estimated overall global QoL scores were significantly improved (66.1 versus 63.0, respectively; p = 0.03), patient-reported pain significantly improved from baseline (–3.3 versus 2.0; p = 0.001), and time to deterioration in global QoL and pain were significantly delayed (HR 0.64; 95% CI 0.45–0.91; p < 0.007; and HR 0.64; 95% CI 0.49–0.85; p < 0.001, respectively). 6 EORTC QLQ-BR23 functioning domains and the symptom domains for breast, arms, and systemic therapy side effects were similar between treatments. 6
Palbociclib in special populations
Elderly patients
No differences in the safety or efficacy of palbociclib have been shown between younger and older patients.8,36 Therefore, no dose adjustments are required based solely on age in patients taking palbociclib. 8 A subgroup analysis of patients from PALOMA-1 demonstrated improvement in median PFS with palbociclib plus letrozole versus letrozole alone in patients aged less than 65 years (HR 0.32; 95% CI 0.18–0.54; p < 0.00001) and in patients aged 65 years and over (HR 0.505; 95% CI 0.269–0.948; p = 0.0155). 36 A pooled analysis of data from elderly patients in the PALOMA-1, -2, and -3 studies showed that palbociclib combined with endocrine therapy versus endocrine therapy alone improved PFS in patients aged 65–74 years (HR 0.66; 95% CI 0.45–0.97; p = 0.0162) and those aged 75 years and over (HR 0.31; 95% CI 0.16–0.61; p = 0.0002). 55 Moreover, findings from the pooled analysis demonstrated no new safety concerns in elderly patients taking palbociclib. 55
Patients with hepatic or renal impairment
Palbociclib exposure is not altered in patients with mild hepatic impairment [total bilirubin ⩽ upper limit of normal (ULN) and aspartate aminotransferase (AST) > ULN, or total bilirubin >1.0–1.5 × ULN and any AST] or in patients with mild [60 ml/min ⩽ creatinine clearance (CrCl) <90 ml/min] or moderate renal impairment (30 ml/min ⩽ CrCl <60 ml/min) and therefore does not typically require dose adjustments. 8 Recently, palbociclib has also been studied in patients with moderate or severe hepatic impairment or severe renal impairment.
A phase I study evaluating the pharmacokinetics of palbociclib in subjects with moderate to severely impaired hepatic function demonstrated that plasma palbociclib unbound exposure was decreased by 17% in subjects with mild hepatic impairment, while increasing by 34% and 77% in subjects with moderate or severe hepatic impairment, respectively, compared with subjects with normal hepatic function. Similarly, peak palbociclib unbound exposure increased by approximately 7%, 38%, and 72% in subjects with mild, moderate, and severe hepatic impairment, respectively. 56 These findings demonstrate that no dose adjustment is required for patients with mild or moderate hepatic impairment whereas the recommended dose of palbociclib for patients with severe hepatic impairment should be 75 mg once daily on a 3/1 schedule (i.e. 3 weeks on, followed by 1 week off palbociclib treatment). 56
A phase I study evaluating the pharmacokinetics of palbociclib in subjects with severe renal impairment demonstrated that plasma palbociclib total exposure increased modestly (range 31–42%), and maximum plasma concentration also increased but to a lesser extent (range 12–17%) after administration of a single oral 125 mg dose of palbociclib in subjects with mild, moderate, or severe renal impairment compared with subjects who had normal renal function. 57 No obvious trend was observed for unbound drug in plasma in subjects with worsening renal function. Additionally, in patients with normal renal function, and those with mild to severe renal impairment, single oral 125 mg doses of palbociclib were well tolerated. 57
Real-world patients
A retrospective cohort study was conducted to assess real-world treatment patterns and outcomes, both pre and post approval, of palbociclib in women with newly diagnosed HR+/HER2– metastatic breast cancer. 58 Additionally, the impact of NCCN guidelines for premenopausal women on treatment patterns and outcomes following palbociclib approval versus prior to the availability of CDK 4/6 inhibitors was assessed. The study used electronic health records data from the Flatiron Health Analytic metastatic breast cancer database (metastatic diagnosis from January 2011 to March 2017). 58 Overall, 10% (n = 415) of women were premenopausal (defined as age ⩽50 years) and 90% (n = 3576) were postmenopausal (age >50 years) at the index date. 58 Treatment patterns for initial endocrine therapy showed that after approval of palbociclib, approximately 30% of women aged up to 50 years were administered a palbociclib-containing regimen, with or without ovarian suppression, and this proportion was comparable to that observed in women aged over 50 years (27%). 58 Consistent with NCCN guidelines, the frequency of palbociclib use was similar for younger and older patients with palbociclib most commonly combined with letrozole in both age groups. In addition, the proportion of younger women who had initiated endocrine-based treatment with an AI alone prior to palbociclib approval was reduced by half post approval (46% versus 23%); however, the increased use of AI–palbociclib combinations (which increased to 25% after approval) offsets this reduction. 58 Results from this analysis show that in accordance with American Society of Clinical Oncology and NCCN guidelines, palbociclib has been incorporated into standard care in the US for women with HR+/HER2– metastatic breast cancer, irrespective of age. 58
Another retrospective observational study also used data from the Flatiron Health Analytic metastatic breast cancer database to analyze real-world population characteristics and utilization patterns in patients who had initiated treatment with palbociclib on or after the date of palbociclib approval (3 February 2015) to 31 March 2017. 59 Of the 1871 patients in the analysis who initiated treatment with palbociclib, 98.4% were women (pre- and postmenopausal) and 1.6% were men. Overall, 39.1% of patients received palbociclib as first-line therapy, 31.9% as second-line, and 40.9% as third-line or later therapy. 59 Among women who had initiated palbociclib with an AI, 45.7% initiated it as first-line therapy, 23.8% as second-line therapy, and 30.6% as third-line or later therapy. Among women who had initiated palbociclib in combination with fulvestrant, 22.3% initiated it as first-line therapy, 32.5% as second-line therapy, and 45.2% as third-line or later therapy. Moreover, among all patients who received first-line palbociclib, 65.7% used palbociclib in combination with an AI. In accordance with the product label, the majority of patients initiated palbociclib at the recommended 125 mg dose. 59
Ongoing and future palbociclib studies
As of February 2018, there were 70 ongoing breast cancer interventional studies that involve palbociclib. Select ongoing clinical trials to further assess the role of palbociclib in breast cancer are shown in Table 3. Currently, ongoing studies are evaluating the safety and efficacy of palbociclib in combination with endocrine therapy in patients with early breast cancer (adjuvant and neoadjuvant) and HER2+ metastatic breast cancer in combination with endocrine therapy, pertuzumab, and trastuzumab. Palbociclib is also being studied in patients with other tumor types, including gastrointestinal, and lung cancers.
Select palbociclib breast cancer clinical studies.

Final data collection date for the primary outcome measure.
Normal indicates with an immunohistochemistry score 0−1 or a fluorescent in situ hybridization negative result (that is, an in-situ hybridization ratio <2.0 status) preferably based on tissue from postneoadjuvant residual invasive disease or a core biopsy of the breast, or if no other tissue is available, the residual tumor of the lymph node.
ABC, advanced breast cancer; BC, breast cancer; CCR, complete clinical response; CDK 4/6, cyclin-dependent kinases 4 and 6; EBC, early breast cancer; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; HR, hormone receptor; iDFS, invasive disease-free survival; mBC, metastatic breast cancer; PFS, progression-free survival.
Current literature on the real-world use of palbociclib in clinical practice is limited, but findings from ongoing real-world retrospective studies, such as those presented above analyzing data from the Flatiron Health Analytic database, will provide important information regarding the use of palbociclib in clinical practice. An ongoing retrospective, longitudinal, observational study showed that demographic and clinical characteristics of patients initiating treatment with palbociclib in the real world generally are similar to those in US studies. 60 Another retrospective, observational study is currently assessing the demographic and clinical characteristics and treatment patterns of patients initiating palbociclib in the real world. 61 At present, a prospective, noninterventional study of palbociclib in ABC treatment is underway to understand prescribing and treatment patterns in routine clinical practice; ABC treatment prior to, during, and after palbociclib; patient perceived tolerability; geriatric assessment in elderly patients; and biomarkers underlying resistance or response mechanisms to palbociclib treatment.
Conclusion
Palbociclib is a first-in-class CDK 4/6 inhibitor indicated for combination with endocrine therapy as first-line treatment and after progression on prior endocrine therapy in patients with HR+/HER2– metastatic breast cancer or ABC, and over 70,000 patients in the US and over 100,000 patients worldwide are estimated to have been treated with palbociclib to date. Clinical studies have demonstrated that palbociclib in combination with endocrine therapy is efficacious and tolerable, including in several subgroups of patients, and furthermore, it maintains HRQoL. Although a comprehensive review of the class of CDK 4/6 inhibitors is beyond the scope of this publication, it should be noted that other CDK 4/6 inhibitors have been approved more recently (FDA approval of ribociclib as of 13 March 2017 and abemaciclib as of 28 September 2017). In clinical trials of CDK 4/6 inhibitors, notable differences between the adverse event profiles of palbociclib and the other two agents have become apparent and should be taken into consideration when selecting an appropriate therapy.62–64 Future clinical studies are ongoing to assess palbociclib use in the real world and as a potential treatment for patients with HR+ early breast cancer.
Supplemental Material
McShane_et_al_Additional_File_1_Supplementary_Materials – Supplemental material for Updates on managing advanced breast cancer with palbociclib combination therapy
Supplemental material, McShane_et_al_Additional_File_1_Supplementary_Materials for Updates on managing advanced breast cancer with palbociclib combination therapy by Teresa M. McShane, Thomas A. Wolfe and Joanne C. Ryan in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Editorial support was provided by Susan Reinwald, PhD, Anny Wu, PharmD, and Alan Klopp, PhD, of Complete Healthcare Communications, LLC (West Chester, PA), a CHC Group company, and was funded by Pfizer Inc. All authors contributed to the concept and design of the manuscript, interpretation of data, critical revision for important intellectual content, and final approval of the submitted version.
Funding
This work was funded by Pfizer Inc.
Conflict of interest statement
All authors are employees of and own stock in Pfizer Inc.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.