
Abstract
Background
Limited passive shoulder external rotation (ER) range of motion (ROM) is one of the critical clinical criteria in the diagnosis of frozen shoulder. External rotation ROM is equally commonly assessed in sitting with the arm by the side or in supine at 90° shoulder abduction, but it is unclear if ER ROM varies with body posture or shoulder abduction angle. Using a repeated measures design the aim was to examine if there are differences in passive shoulder ER ROM when measured in different body postures and different shoulder abduction angles.
Methods
Eleven healthy adults aged between 18 and 60 years were recruited. Passive shoulder ER ROM was measured bilaterally in five different positions: sitting with the arm by the side, and supine with the arm by the side and at 30°, 60° and 90° shoulder abduction.
Results
There were significant increases in passive shoulder ER ROM with increasing shoulder abduction angle. No significance difference in ER ROM was found between body posture when measured with the arm by the side.
Discussion
Clinicians need to be cognisant of the shoulder abduction angle at which passive ER ROM tests are performed to ensure valid interpretation regarding diagnosis and treatment effectiveness.
Introduction
External rotation (ER) of the shoulder is needed to perform many functional activities of daily living, such as taking off and putting on clothes, washing one's hair as well as reaching and retrieving objects off high shelves. 1 When shoulder ER range is restricted, such activities of daily living become more difficult to perform affecting functional independence and overall quality of life. 2
Limited external ER range of motion (ROM) is associated with many shoulder pathologies but is particularly relevant to the condition known as frozen shoulder, which is characterised by marked restriction of passive shoulder range in multiple planes of movement, with ER being the most limited.3–6 Frozen shoulder is diagnosed from clinical assessment, with one of the main diagnostic criteria being a deficit in passive shoulder ER ROM of greater than 50%. 4 Therefore, accurate assessment of passive ER ROM is essential to make a diagnosis of frozen shoulder so that appropriate treatment for this debilitating condition can be implemented.
In the clinic, ER ROM at the shoulder is usually assessed with the elbow flexed at 90° in an upright sitting position with the arm by the side or in supine lying in varying degrees of shoulder abduction.7,8 Previous studies on young healthy individuals have reported significant differences in passive shoulder ER ROM when measured at similar abduction angles with the subject in a sitting or a supine posture. 7 Large differences in shoulder passive ER ROM measured at different abduction angles have also been reported in healthy young individuals, albeit without statistical analysis to confirm significant differences. 9
Given the absence of reliable imaging or pathology tests to diagnose frozen shoulder, 10 reliable clinical measurements of passive shoulder ROM, particularly passive ER ROM, are currently essential for diagnosis, to assess treatment progression and effectiveness and to enable consistent and optimal patient care between clinicians. As passive shoulder ER is equally commonly assessed in sitting with the arm by the side and in supine lying at varying degrees of abduction in the clinical setting, it is important to evaluate whether body posture and/or shoulder abduction angle influences passive ER ROM.
Therefore, the purpose of this study was to determine if there are differences in passive shoulder ER ROM at different shoulder abduction angles and in different body postures. We hypothesised that there would be a difference in passive shoulder ER ROM when measured in different body postures and in different ranges of shoulder abduction in healthy adults.
Methods
Design
Laboratory based repeated measures.
Participants
Participants were recruited via word of mouth and social media announcements on various platforms. Participants were eligible to participate if they met the following criteria: (1) no current shoulder pain, (2) aged between 18 and 60 years, (3) no previous shoulder pain in the past two years that required treatment and (4) no previous history of shoulder surgery. Following an explanation of the study to the participants, their written, informed consent was obtained. This research received approval from the institution's Human Research Ethics Committee (Approval No.: 2024/HE000257).
A power calculation using G*Power Version 3.1.9.2 11 was conducted based on data from Hollmann, 12 which reported difference in ER ROM between 90° of abduction compared to when the arm was at the side. Assuming a similar magnitude of change across abduction angles, a total of 19 shoulders was required to detect an average difference of 8° ± 15° in ER range for each increment of 30° of shoulder abduction, two-tailed test, at an alpha of 0.05, power of 0.8 and correlation between repeated measures assumed as 0.7. We aimed for 10 participants (20 shoulders) and to have an equal number of male and female participants.
Participants were screened for eligibility by assessing active shoulder movement and resisted isometric shoulder strength. Participants were excluded if they presented with abnormal ROM or abnormal scapulohumeral rhythm (assessed by a physiotherapist with extensive clinical experience), or if pain was produced on any shoulder movements and/or isometric rotation testing.
Prior to testing, details of participants’ age, sex, hand dominance and sporting history (i.e., what sport they played, at what level, if their sport required overhead throwing movements) were collected. Participants had passive shoulder ER rotation ranges measured in one single, individual session.
Equipment specifications
The shoulder ER force was applied through a force transducer (Millennium Mechatronics, MT501 50 kg, 0.02% error, Universal Load Cell, Australia) positioned 0.35 m from the axis of rotation, aligned with the longitudinal axis of the humerus. Passive shoulder ER angle was measured using an optical encoder (New Hong Corp Rotary Encoder Model OVW6-1024-2HC, 0.35° resolution, China), also positioned at the longitudinal axis of the humerus. Both devices were mounted on an adjustable brace (Figure 1) that supported the forearm at 90° elbow flexion, allowed shoulder abduction angle adjustment and secured to the torso. Data from both sensors were sampled simultaneously at 10 Hz using a 24-Bit analogue to digital converter (Avia Semiconductor Model HX711, China) and transmitted via Bluetooth (ESP32-WROOM-32, Espressif Systems, China) to a PC for offline analysis.

The force transducer and optical encoder set up on a brace fixed to a participant sitting upright and having their shoulder external rotation passively measured with the arm by the side.
To ensure that participants were fully relaxed and a true measure of passive ROM was obtained, electromyography (EMG) Ag/AgCl dual surface electrodes (Noraxon #271S, USA – 10 mm diameter and 20 mm inter-electrode distance) were placed over the clavicular head of pectoralis major and anterior deltoid bilaterally, and activity levels were monitored via a wireless EMG system (Noraxon, Telemyo Clinical DTS, USA). The EMG signals were monitored (MR3.12 software, Noraxon, USA) but not recorded. These muscles were monitored because both are superficial internal rotators of the shoulder 13 and can limit passive shoulder ER movement when active. Prior to electrode placement, the skin was abraded with abrasive cream (NuPrep, Weaver and Company), cleaned with isopropyl alcohol and the dual surface electrodes were placed in line with the muscle fibres. Participants were prompted to stay as relaxed as possible during testing. If EMG recordings demonstrated increased activity in either the pectoralis major or anterior deltoid muscles, while the shoulder was moved passively into ER, those trials were discarded and the movement was repeated.
Data collection
Passive shoulder ER ROM was measured bilaterally with the elbow flexed to 90°, in both sitting and supine positions with the arm at the side, and in supine at 30°, 60° and 90° of shoulder abduction. Prior to each testing session, block randomisation via random function in Microsoft Excel was used to select testing side (right or left) and body posture (supine or sitting). The four shoulder abduction angles were randomised during the supine block.
Prior to the first measurement on each side, three repetitions of passive shoulder ER were performed to prepare the tissue for testing. The participant was asked to relax, and their arm was moved into ER (ensuring the axis of rotation of the humerus was aligned with the axis of the optical encoder) until the researcher determined that the joint was at end of range. End of range was established based on two criteria: first, the researcher manually determined the limit of arm movement, and second, the force-angle curve showed that any additional applied force no longer produced significant changes in angle. The force required to reach end of range was recorded and maintained for all further evaluations on that side. Two trials per posture and shoulder abduction angle were recorded, as was the amount of force required to take the testing shoulder to end-range. Measurements were repeated if it was deemed that insufficient force had been applied to reach end of range or the participant was not relaxed as evidenced by surface EMG recordings.
Data analysis
Maximum ER ROM and the corresponding applied force were extracted for each trial using Microsoft Excel. Maximum ER angle and corresponding applied force were compared between body postures with the arm by the side using a 4-factor (sex [male; female], side [dominant; non-dominant], body posture [sitting; supine] and trial [trial 1; trial 2]) repeated measures analysis of variance (ANOVA), and compared across shoulder abduction angles while supine using a 4-factor (sex [male; female], side [dominant; non-dominant], shoulder abduction angle [arm by the side; 30°; 60°; 90°] and trial [trial 1; trial 2]) repeated measures ANOVA (Statistica, version 10, Tulsa OK, USA). Tukey post-hoc tests were used to identify significant differences between conditions when significant ANOVA results were found. Significance level was set as p < 0.05.
To provide a visual representation of the average pattern of force angle profiles across trials and participants for each condition, the applied force and ER angle signals were time-normalised to 101 points, where 0% represents the initiation of movement, 50% represents the maximum ER ROM and 100% represents return to the starting position (Matlab Version 11, R2024a, The MathWorks, Natick, MA, USA). The normalised signals were then averaged across trials to provide a representative curve per condition for each participant and averaged across participants to provide an average curve across participants for each condition.
Results
Eleven healthy adults (38.5 ± 10 years of age), consisting of six males and five females were recruited for this study. Eight participants were right-hand dominant and three left-hand dominant. Of the 11 participants, 10 had a previous sporting history in overhead throwing sports and/or in swimming. Data for one participant was lost due to technical difficulties during passive ER measurement on the non-dominant side in sitting. In addition, data at different abduction angles during supine posture was not available for one participant who experienced signs of apprehension preventing testing. Therefore, 20 shoulders (dominant and non-dominant sides of 10 participants) were included in each analysis. Shoulder abduction angle with the arm by the side varied between 0° and 20° depending on the size of the participant and restriction from the measuring equipment.
Sitting versus supine with the arm by the side
There were no significant differences in passive shoulder ER ROM between males and females (F(1,8) = 1.018, p = 0.343), dominant and non-dominant sides (F(1,8) = 0.654, p = 0.429), sitting vs. supine (F(1,8) = 0.005, p = 0.945) nor trial 1 vs. trial 2 (F(1,8) = 3.155, p = 0.114). No significant interaction effects were found (p ≥ 0.682). Figure 2 presents the mean ± standard deviation (SD) ER ROM across participants, sides and trials for sitting and supine with the arm by the side postures, and the mean time normalised force angle curves across participants, sides and trials for sitting and supine with the arm by the side.
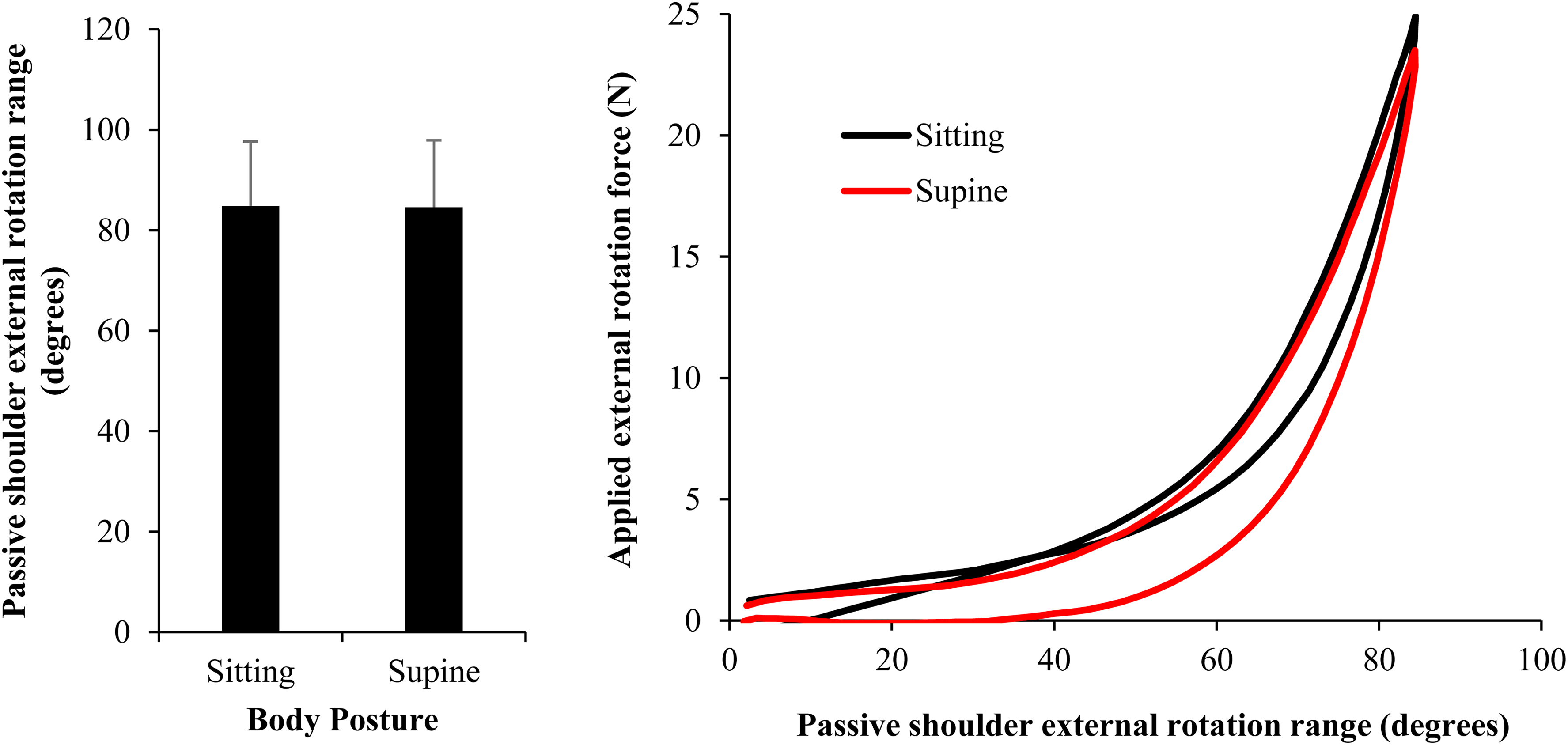
The mean ± standard deviation passive shoulder external rotation range and mean time-normalised force angle curves across participants and sides when comparing between body postures.
The maximum applied force was significantly higher in trial 2 (mean ± SD [95% confidence interval] 25.2 ± 3.7 [21.8, 26.1] N) than in trial 1 (24.0 ± 2.9 [22.5, 27.9] N) with a mean difference [95% confidence interval of the difference] of 1.2 [0.5, 1.9] N (
Different shoulder abduction angles in supine
There were no significant differences in passive shoulder ER ROM between males and females (F(1,8) = 0.045, p = 0.837) and dominant and non-dominant sides (F(1,8) = 1.152, p = 0.314). There were significant differences in passive shoulder ER ROM among shoulder abduction angles (F(1,8) = 117.440, p < 0.01), and between trial 1 (97.6 ± 12.7°) vs. trial 2 (98.7 ± 12.9°) with a mean difference [95% confidence interval of the difference] of 1.1 [0.5, 1.8]° (F(1,8) = 15.650, p < 0.01).
Figure 3 presents the mean ± SD ER ROM and mean time-normalised force angle curves across participants, sides and trials for supine with the arm by the side, 30°, 60° and 90° shoulder abduction. Tukey post-hoc tests revealed that there were significant differences in passive shoulder ER range between the arm by the side and 60° abduction (p < 0.01), the arm by the side and 90° abduction (p < 0.01), between 30° and 60° abduction (p < 0.01), 30° and 90° abduction (p < 0.01) and 60° and 90° abduction (p < 0.01). No differences in passive shoulder ER ROM were found between the arm by the side and 30° abduction (p = 0.078).
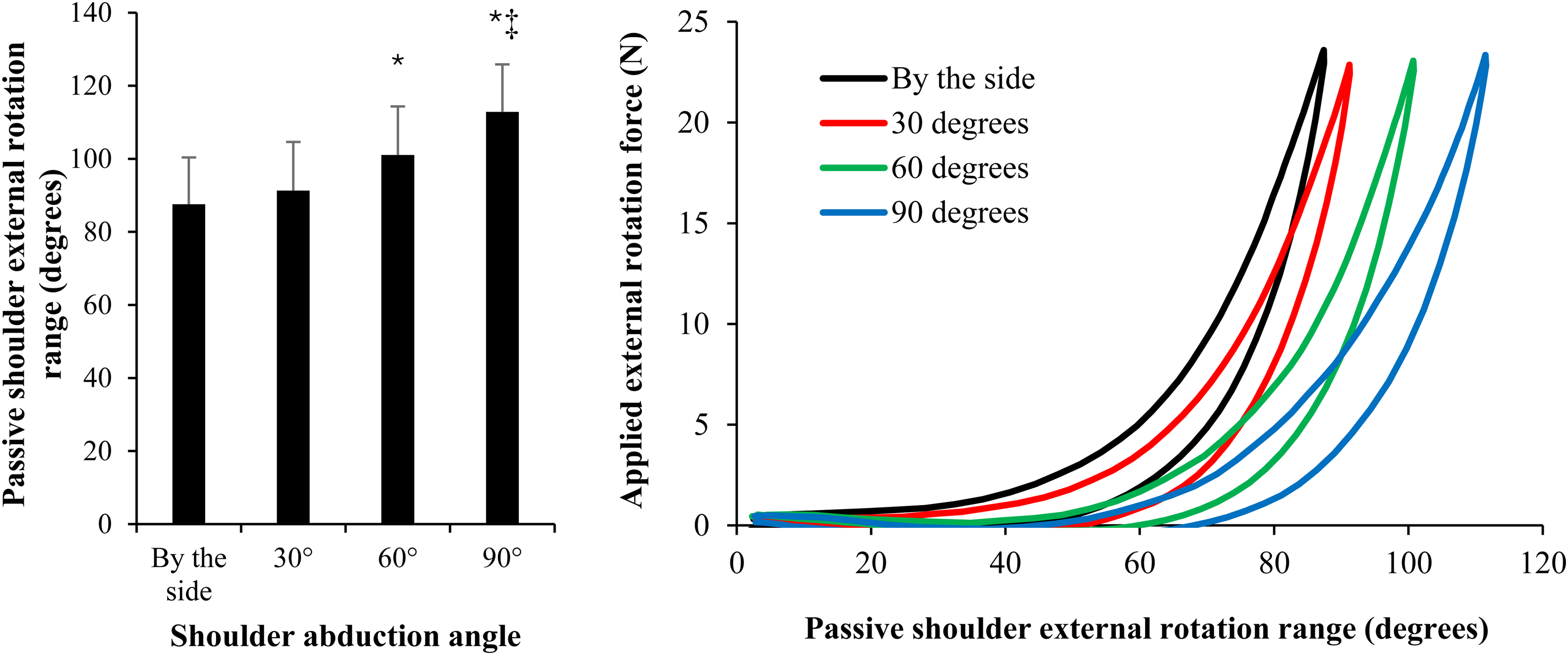
The mean ± standard deviation passive shoulder external rotation range and mean time-normalised force-angle curves when comparing measurements between different shoulder abduction angles across sides. * indicates significant (p < 0.05) difference to by the side and 30° shoulder abduction. ‡ indicates significant difference between 60° and 90° shoulder abduction.
A significant angle × sex interaction was found (F(3148) = 3.405, p = 0.034); however, Tukey post-hoc testing did not detect any differences between males and females at any of the abduction angles (p ≥ 0.998). No other significant interaction effects were found (p ≥ 0.096).
The maximum applied force was significantly higher in trial 2 (24.05 ± 3.7 N) than in trial 1 (23.21 ± 3.4 N) with a mean difference [95% confidence interval of the difference] of 0.8 [0.4, 1.3] N (F(1,8) = 21.000, p < 0.01). There were no significant differences found in applied force between males and females (F(1,8) = 0.862, p = 0.380), dominant and non-dominant sides (F(1,8) = 0.762, p = 0.408) nor between abduction angles (F(1,8) = 1.272, p = 0.306). No significant interaction effects were found (p ≥ 0.067).
Discussion
In contrast to previous research, the results of the current study indicated that posture does not significantly influence passive shoulder ER ROM when measured with the arm by the side. 7 In this previous study, passive ER ROM was measured without applied force or EMG feedback, which may explain this discrepancy in results. Based on the results of the current study, the two commonly used postures used to measure shoulder passive ER ROM in the clinic, sitting upright and lying supine with the arm by the side, can be validly compared.
Passive shoulder ER ROM, however, did significantly increase as shoulder abduction angle increased, supporting the preliminary conclusions from previous research. 9 This result implies that clinicians must be consistent in the shoulder abduction angle at which passive shoulder ER is measured to ensure valid interpretation of this clinical diagnostic test and valid assessment of treatment results.
No significant differences in passive ER ROM were found between males and females or between dominant and non-dominant arms. The force applied during measurements was consistent across conditions, although it was ∼1N higher in the second trial, leading to a slight increase (∼1°) in ROM across different shoulder abduction angles. However, this did not result in significant differences in passive shoulder ER ROM between trials across the conditions tested.
At the glenohumeral joint, passive shoulder ER is limited by the three capsular glenohumeral ligaments—superior, middle and inferior—and the coracohumeral ligament. 14 All these ligaments contribute to limiting shoulder ER through the full range of shoulder abduction, but the proportional contribution from each ligament changes depending on the angle of shoulder abduction. The superior glenohumeral and coracohumeral ligaments contribute the most to limiting ER below 60° abduction15,16; the middle glenohumeral ligament contributes the most between 45° and 90° of abduction 16 ; while the inferior glenohumeral ligament mainly contributes to limiting ER when the shoulder is abducted beyond 90°.17,18 This proportional contribution to limiting ER ROM from each of these glenohumeral ligaments at different angles of shoulder abduction could explain the finding of significant increases in passive ER ROM with increasing shoulder abduction in this study. The middle glenohumeral ligament whose greatest contributes to limiting ER ROM is in mid-range abduction is sometimes absent,16,19 or has a vestigial appearance.20,21 This anatomical variation could contribute to less restraint to passive shoulder ER ROM at the glenohumeral joint in mid-shoulder abduction range and thus to the significant increases in average ER ROM observed at 60° and 90° abduction in this study.
As the scapula is not firmly stabilised during the common clinical measurements of passive shoulder ER ROM examined in this study, the differences in shoulder ER ROM at different shoulder abduction angles may not be restricted to these glenohumeral joint anatomical features. The significant differences in passive shoulder ER ROM as shoulder abduction ROM increased found in this study may also be explained by an increasing contribution of scapula movement to shoulder passive ER ROM at these higher shoulder abduction angles.
No significant difference in passive shoulder ER ROM was found when comparing measurements taken with the arm by the side and in 30° abduction. These findings would be expected as the ligamentous contribution limiting passive shoulder ER ROM at the glenohumeral joint (i.e., predominantly the superior glenohumeral and coracohumeral ligaments) is similar at these shoulder abduction angles. In addition, the arm was slightly abducted when the arm was positioned by the side for many of our participants. Consequently, the difference in shoulder abduction angle with the arm by the side and 30° abduction was small in these participants, further contributing to this result.
The small sample size in the current study included a middle age population with balanced sex representation. However, it did include a predominance of individuals with a history of overhead sports participation, who may exhibit sport-specific adaptations in shoulder capsular characteristics and ER ROM. These factors may limit the robustness of the findings and future studies should confirm these results in larger studies in a more general population with a broader age range.
In the current study, the force applied by the examiner increased on average by approximately 1 N (∼4%) during the second trial at each position compared with the first, yet this was associated with only minimal increases in passive ER ROM (∼1°, ∼1%) in some positions. As the force was manually applied, this small increase may reflect examiner-related variation rather than learning effects, systematic measurement bias or participant-driven changes. Importantly, the lack of a meaningful increase in ROM despite the higher applied force suggests minimal tissue accommodation or viscoelastic creep between trials, supporting the reliability of end-range determination.
Conclusion
Passive shoulder ER ROM changes with changes in shoulder abduction angle, with greater ER ranges observed as shoulder abduction approaches 90°. In contrast, changes in body posture do not appear to influence passive ER ROM at the shoulder when measured with the arm by the side, although future research will need to determine if this is true at higher abduction angles. In order to ensure valid interpretation of passive shoulder ER clinical tests with regards to diagnosis and treatment effectiveness, clinicians need to consider the shoulder abduction angle at which these tests are performed.
Footnotes
Ethical approval
The University of Sydney Human Research Ethics Committee – Approval No.: 2024/HE000257.
Informed consent
Following an explanation of the study written, informed consent was obtained from all participants.
Contributorship
All authors made a substantial contribution to the concept or design of the work; or acquisition, analysis or interpretation of data, were involved in the drafting of the article or revised it critically for important intellectual content, approved the version to be published and take public responsibility for appropriate portions of the content.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Guarantor
MH.