
Abstract
Introduction:
The purpose of this retrospective study was to investigate the possible short-term benefit of a single intra-articular corticosteroid injection in those patients treated with physiotherapy when compared to a group of patients undergoing physiotherapy only (PT only).
Methods:
A retrospective chart review was conducted to identify eligible patients treated over a 4-year period. All female patients between 40 years and 60 years with a confirmed clinical diagnosis of idiopathic adhesive capsulitis who completed a prescribed physiotherapy program were considered eligible. Sixty-three patients fulfilled the inclusion criteria, but 22 were excluded because of missing data in the medical record. The remaining 41 patients comprise the study cohort; an experienced musculoskeletal physiotherapist assessed these patients both at initial presentation and at 12 weeks. Twenty patients with a mean age of 55.1 years underwent PT only and 21 patients with a mean age of 52.4 years received a single intra-articular dose of 40 mg methylprednisolone followed by physiotherapy. Outcome measures included the visual analogue scale (VAS) and measurement of range of motion.
Results:
At final assessment (12 weeks), significant between-group differences were identified for the ‘PT only’ group for flexion (p = 0.01) and abduction (p = 0.008). When comparing the mean change from the initial assessment, a significant between-group difference was observed for abduction (p = 0.03).
Conclusions:
The results of this study suggest that the intra-articular injection of a single dose of cortisone has no significant short-term benefit in female patients with idiopathic adhesive capsulitis managed with physiotherapy.
Keywords
Introduction
Idiopathic adhesive capsulitis, or ‘frozen shoulder’, is a common cause of shoulder pain and progressive loss of both active and passive range of motion. 1 –3 The disorder predominantly affects women aged 40 to 60 years and is estimated to affect 2–4% of the adult population. 1 –3 The pathogenesis is still unclear, although specific risk factors have been associated with the condition and include diabetes mellitus, thyroid disease, autoimmune diseases, myocardial infarction, stroke and prolonged immobilization. 3,4
The condition has a typical clinical course and characteristically passes through three defined stages, progressing over a period of several years. 4 –9 Insidious in onset, stage 1 is commonly described as the acute or ‘freezing’ stage; it consists of gradually increasing pain and stiffness and lasts between 2 months and 9 months. 4 Stage 2 is considered the ‘frozen’ or ‘steady-state’ stage; the loss of range of motion is most pronounced and lasts between 4 months and 20 months. Stage 3 is regarded as the ‘thawing’ or ‘recovery stage’; it is characterized by resolution of pain and gradual recovery and lasts between 5 months and 26 months. 4,7 Neiaser and Neviaser have described four stages based on the arthroscopic appearance. Stage 1 consists of the pre-adhesive stage with an inflammatory synovitis and full range of motion but report pain. 8 In his classification scheme, stages 2–4 correspond to the classical stages 1–3 as described by Codman.
The natural history of this disorder is still poorly understood, and although some researchers 6,9 have demonstrated full recovery, others have shown that it can result in long-term disability. 5,10
Many nonoperative treatment options have been described ranging from nonsteroidal anti-inflammatory medication, either oral or intra-articular corticosteroids, physical therapy, hydrodilatation and manipulation under anaesthesia. 1,8,10,11 In a systematic review, van der Heijden et al. investigated physical therapy interventions in patients with soft tissue disorders of the shoulder and concluded that there was insufficient evidence to support physiotherapy treatment over drug therapy or steroid injections. 12
The use of intra-articular steroid injections remains controversial. A Cochrane review from 2003 concluded that it may be beneficial in the short term, but the effect may be small and not maintained. 13 More recently, a meta-analysis by Page et al. reported that a glucocorticoid injection may be more beneficial than a combination of manual therapy and exercise. 14
The purpose of this retrospective study was therefore to investigate the possible short-term benefit from a single adjuvant intra-articular corticosteroid injection in patients with pain and restricted movement treated with physiotherapy, when compared to a group of similar patients undergoing physiotherapy only (PT only). We hypothesized that a single intra-articular injection of corticosteroid would significantly reduce pain and lead to an overall improvement in range of motion.
Methods
Patients
A retrospective chart review was conducted of all adult female patients who presented to the orthopaedic clinic with a clinical diagnosis of adhesive capsulitis. All female patients between 40 years and 60 years with a confirmed clinical diagnosis of idiopathic adhesive capsulitis who completed a prescribed physiotherapy program were included. The clinical diagnosis was made by an experienced orthopaedic surgeon using the following indicators: progressive painful decrease or complete loss of active and passive range of motion, positive external rotation test, dull or aching pain in the shoulder area, anterior and posterior shoulder tenderness, history of night or rest pain for at least three months but less than one year and inability to sleep on the affected side. 15 The following exclusion criteria were applied: inflammatory arthritis including rheumatoid arthritis; uncontrolled diabetes mellitus; failure to complete the physiotherapy course; bilateral shoulder pain; any history of previous trauma to the affected side; Parkinson’s disease; newly diagnosed hyperthyroidism, hypothyroidism and malignant disorders; and other causes of secondary adhesive capsulitis including rotator cuff injury, cerebrovascular accident and cardiovascular disease. Patients were advised regarding the risks and potential benefits of an intra-articular steroid injection and then given the option to add this additional element to their treatment prior to initiating formal physiotherapy.
A total of 650 medical records of patients with shoulder pain were reviewed, and 63 patients fulfilled the inclusion criteria. Of these 63 patients, 22 patients were excluded because of missing data in the chart. Twenty patients with a mean age of 55.1 ± 7.3 (range 41–71) were managed with physiotherapy without first receiving an injection and constitute the ‘PT only’ group. The remaining 21 patients with a mean age of 52.4 ± 8.5 (range 44–74) received a single steroid injection during their first presentation to the clinic and were then managed further with physiotherapy and constitute the ‘PT+INJ’ group.
Physiotherapy
Six experienced musculoskeletal physiotherapists participated in the care of all patients. Following initial clinical evaluation, each patient received weekly treatment for 9 months. For patients who underwent injection with cortisone, the first physiotherapy commenced 5–7 days post-injection; patients who underwent physiotherapy only were treated within 1 week of their initial presentation to the clinic. Therapeutic interventions included Kaltenborn passive joint mobilization, active or active assisted exercises and a strengthening exercise program. Passive articular stretching and active assisted/active exercises were used to improve range of motion specifically of the glenohumeral joint. In addition, patients were encouraged to perform strengthening exercises under the supervision of the physiotherapist using standard gymnasium equipment. Ice packs, hot packs and transcutaneous electrical nerve stimulation were used as indicated to reduce pain throughout treatment. Finally, all patients were encouraged to continue performing their usual activities of daily living. Patients were instructed regarding a standardized home exercise program and encouraged to perform these three times each day.
Steroid injection
Following initial assessment, patients were injected with a single dose of methylprednisolone. All injections were performed by a qualified, experienced orthopaedic surgeon who has used this technique on a regular basis. Patients were placed in the supine position with the arm at their side and the shoulder in internal rotation. An anterior approach was utilized in all cases, injecting a combination of 5 ml of 0.5% lignocaine and 1 ml of 40 mg methylprednisolone. The skin was cleaned and prepped with 70% alcohol, and a 21-gauge needle was inserted just medial to the head of the humerus and 1 cm lateral to the coracoid process. The needle was directed posteriorly, aiming slightly more superior and lateral to accomplish intra-articular delivery. Ultrasound guidance was not used. Bloom et al. demonstrated that there is insufficient evidence that ultrasound improves the accuracy of injection to the putative side of pathology. 16 Following injection, pain-free motion was established; the first session of physiotherapy was scheduled for 7 days after injection, as recommended by Arslan and Celiker. 17
Outcome measures
Patients were assessed at the initial presentation and at 12 weeks after the first physiotherapy treatment session.
Visual analogue scale
The visual analogue scale (VAS) is a commonly used measure for pain severity and relief, with a scale ranging from 0 (no pain) to 100 mm (worst pain). 18 The VAS is a horizontal line of 100 mm in length; the patient simply marks the line at the point that they feel represents their current perception of pain. It is easy to use, has been validated across cultures 19 –22 and is sensitive to treatment effects. The VAS score was determined by measuring the length in millimetres from the left end of the line to the point that the patient has marked. The treating physiotherapist performed this measurement using a calibrated ruler. The data derived can be analysed using parametric tests. 18 –20,23 Changes in the VAS score represent a relative change in the magnitude of pain sensation.
Range of motion
Active range of motion measurements included flexion, abduction, internal and external rotation. The goniometry method, as described by Hayes et al., was used for the measurement. 24 Patients were seated upright with the elbow on the side of the body and flexed to 90°, with neutral supination/pronation of the forearm. Flexion angles were measured by aligning the goniometer with the lateral condyle of the humerus and a vertical line in the coronal plane. Similar abduction angles were determined by aligning the goniometer with the lateral condyle of the humerus and a vertical line in the sagittal plane. Finally, external and internal rotation was measured by aligning the goniometer with the radial styloid and a horizontal line in the transverse plane.
Statistical analysis
A sample size calculation was performed. Selecting an alpha level of 0.05 and power value of 0.80, the study was able to detect a 20° between-group difference for range of motion, and a 20-mm between-group difference for VAS. The sample size analysis based on these parameters indicated that a minimum of 16 patients per group was needed to provide 80% statistical power. Means and standard deviations were calculated for the dependent variables. Within-group differences for the dependent variables (VAS, abduction, flexion, internal rotation and external rotation) were compared using a series of one-way analysis of variance. The overall mean change from the initial assessment for both the VAS and range of motion variables was compared between the PT only and PT+INJ groups (‘between-group differences’) using a series of paired t-tests. Between-group differences for VAS were analysed using the independent two-tailed t-test. Alpha level correction using Bonferroni corrections was performed to correct family wise error for multiple comparisons. Between-group analysis for the remaining range of motion parameters (flexion, abduction, internal rotation and external rotation) was performed using the Wilcoxon rank sum test. All analyses were conducted using Stata SE (version 12; StataCorp LP, College Station, Texas, USA).
Results
There were no significant between-group differences for the initial assessment for age (p = 0.33), VAS (p = 0.15), flexion (p = 0.93), abduction (p = 0.99), internal rotation (p = 0.45) and external rotation (p = 0.74) (Table 1). Significant between-group differences at the final assessment (12 weeks) were observed for flexion (p = 0.01) and abduction (p = 0.008) (Table 1). When comparing the mean change from the initial assessment, a significant between group difference was observed for abduction (p = 0.03) (Table 2).
Initial and final assessment at 12 weeks of VAS (in mm) and range of motion (in degrees): mean and standard deviation.
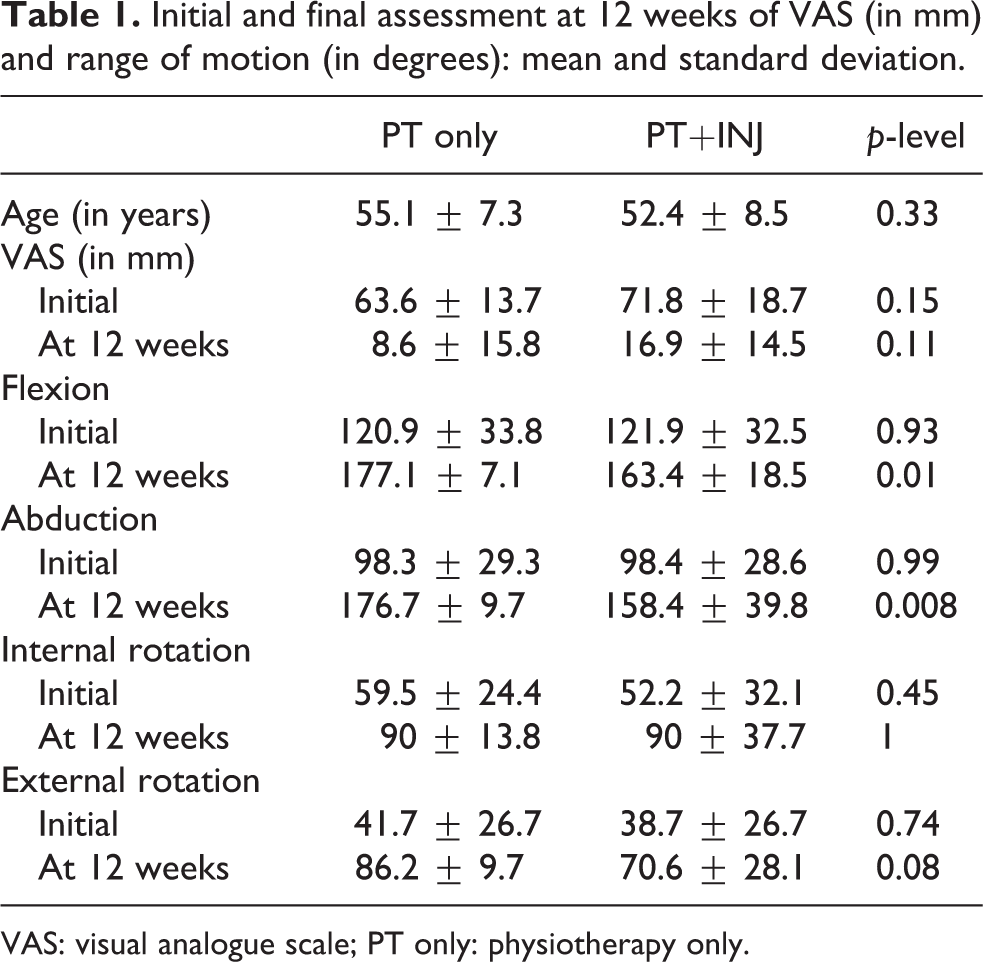
VAS: visual analogue scale; PT only: physiotherapy only.
VAS (in mm) and range of motion (in degrees) including p-levels: mean change and standard deviation from initial assessment.
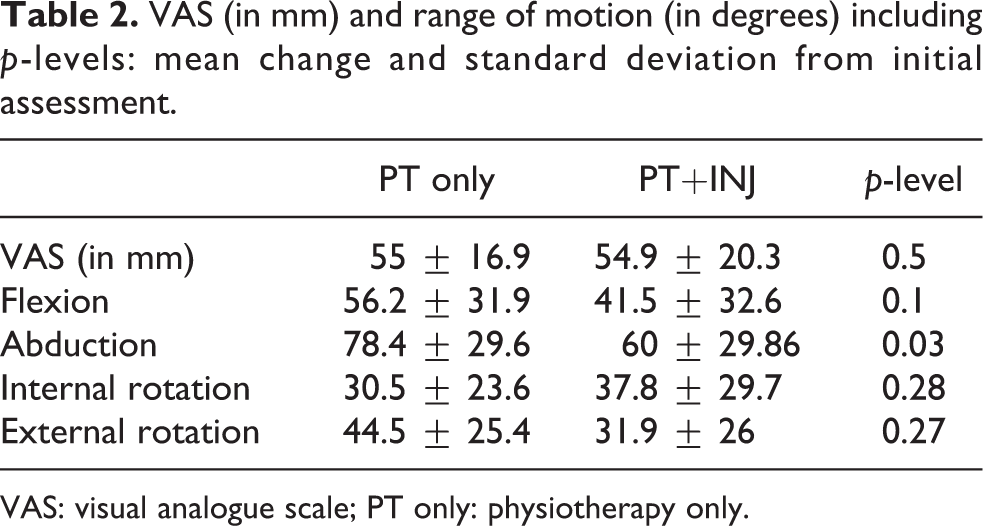
VAS: visual analogue scale; PT only: physiotherapy only.
Visual analogue score
Patients in the PT only group demonstrated significant improvement (p < 0.0001) in VAS from 63.6 ± 13.7 mm to 8.6 ± 15.8 mm. Similar patients in the PT+INJ group demonstrated significant improvement (p < 0.0001) in VAS from 71.8 ± 18.7 mm to 16.9 ± 14.5 mm. The results for both the PT only and PT+INJ groups are summarized in Tables 1 and 2.
Range of motion
Patients in the PT only group demonstrated significant improvement (p < 0.00001) in flexion from 120.9° ± 33.8° to 177.1° ± 7.1°, in abduction (p < 0.00001) from 98.3° ± 29.3° to 176.7° ± 9.7°, in internal rotation (p < 0.00001) from 59.5° ± 24.4° to 90° ± 13.8° and in external rotation (p < 0.00001) from 41.7° ± 26.7° to 86.2° ± 9.7°.
Similar patients in the PT+INJ group demonstrated significant improvement (p = 0.0002) in flexion from 121.9° ± 32.5° to 163.4° ± 18.5°, in abduction (p < 0.0001) from 98.4° ± 28.6° to 158.4° ± 39.8°, in internal rotation (p = 0.005) from 52.2° ± 32.1° to 90° ± 37.7° and in external rotation (p = 0.0006) from 38.7° ± 26.7° to 70.6° ± 28.1°. Significant between-group differences at 12 weeks were observed for flexion (p = 0.01) and abduction (p = 0.008). A significant (p = 0.03) between-group difference for the mean change from the initial assessment for range of motion was only observed for abduction (p = 0.03) (Table 2). The results for both the PT only and PT+INJ groups are summarized in Tables 1 and 2.
Discussion
The most important finding of this study is that there was no apparent short-term benefit derived from a single intra-articular steroid injection in middle-aged female patients with idiopathic adhesive capsulitis. In fact, with respect to abduction, patients in the PT only group demonstrated a significantly greater mean improvement from the baseline range, 78.7° more range in the PT only group compared to only 60° in the PT+INJ group.
Our results confirm the findings first noted by Lee et al. in 1974. 25 They compared patients treated with intra-articular cortisone injections, cortisone injections to the biceps region and physiotherapy only and could not demonstrate a significant difference between the three groups at 6 weeks. These early results were subsequently confirmed by others. 26,27 In a randomized controlled trial, Bulgen et al. compared patients treated using standard physiotherapy modalities in two separate groups, either with or without an initial intra-articular methylprednisolone injection. 26 Significant between-group differences regarding increased range of motion and decreased pain were found for the first 6 weeks; they could not demonstrate a significant advantage of steroid injections beyond this period. The authors concluded steroid injections may diminish pain and increase range of motion in the early stages of treatment. Similarly, Dacre et al. randomly allocated patients to receive PT only, steroid injection only or a combination of the two treatment modalities. 27 Although all patients had less pain and demonstrated improvement in range of motion, differences between these groups were not observed.
However, our results also contradict the results of several other previously published studies. 28 –31 van der Windt et al. reported an overall improvement in symptoms at 7 weeks in 77% of patients who had received an intra-articular steroid injection, compared to 46% of patients who were treated with PT only. 31 In a prospective randomized study, Carette et al. compared a group of patients receiving 40 mg of triamcinolone followed by supervised physiotherapy to three other groups: corticosteroid injection alone, saline injection followed by supervised physiotherapy and saline injection alone. 28 They reported superior outcomes at 6 weeks for range of motion and shoulder pain and disability index (SPADI) score in the group receiving a single intra-articular steroid injection coupled with physiotherapy. However, 9 out of 21 patients in the PT+INJ were lost during the follow-up (42%), which has potentially introduced outcome bias. Furthermore, five patients later received an additional steroid injection, another confounding factor. Ryans et al. compared the combined treatment effect of 20 mg triamcinolone and physiotherapy with three other groups: steroid injection only, saline injection with physiotherapy and saline injection only. 30 They demonstrated a beneficial effect on overall shoulder disability in those subjects who received an intra-articular steroid injection; they demonstrated increased external rotation in those subjects who received physiotherapy. However, no further clinical benefits beyond 6 weeks were identified.
Bal et al. treated 80 patients with physiotherapy after randomly assigning them to either of two groups: one group received an intra-articular steroid injection and the other received a saline injection. 4 As was observed in our study, as well as by Bulgen et al., 26 they noted an initial significant decrease in pain and increased abduction at 2 weeks. However, at 12 weeks, no differences between the two groups were identified. Similar to Ryans et al., given the significant early reduction in pain, 30 Bal et al. therefore concluded that adjuvant intra-articular steroid injections could be beneficial in those patients with adhesive capsulitis who have significant complaints and limitations related to pain. 4 Of interest, we did not observe a direct effect on pain in our study cohort and both groups had a mean improvement in VAS from baseline by 55 points. A possible difference between these authors findings and our results could be that both Bal et al. 4 and Ryans et al. 30 included patients with more recent onset pathology. Both those studies have potentially included patients who presented with Neviaser stage 1 inflammatory symptoms. Steroids act as powerful anti-inflammatory agents by reducing interleukin-1, leukotrienes and prostaglandins. 32 Using steroids in the acute inflammatory stage would certainly have an effect on pain and may explain the effect observed. 4,30 We have specifically excluded those patients with a only short duration of symptoms in order to reduce the risk of including patients in the acute inflammatory stage. In a recent systematic review by Song et al., it was concluded that corticosteroid injections may offer initial improvements for the first 6 weeks but do not provide added benefits in improving pain and ROM compared to physical therapy alone. 33 Adhesive capsulitis is clearly a disease of inflammation in the early stages and fibrosis in the later stages which could explain why there was no benefit identified in our cohort.
We failed to demonstrate a significant difference in the range of motion, except for abduction. This study was powered to detect a difference of >20° for range of motion at 12 weeks, which was considered to be clinically meaningful. However, we were able to demonstrate a significant overall improvement in range of motion from the mean baseline in both groups. There was greater improvement in shoulder range of motion from the baseline in the PT only group, but this failed to reach significance. Compared to the PT+INJ group, who improved their total range of shoulder motion by 171°, we observed an overall improvement of 210° in the PT only group. An individual patient in the PT only may perceive this improvement as a clinical advantage; the inclusion of a validated subjective outcome score such as DASH, SPADI or SF 12 would have therefore been beneficial and is a further limitation of our study.
The current project aimed to include patients in Neviaser stages 2 and 3 only. It cannot be entirely excluded that some of the patients included were going through Neviaser stage 1. The inclusion criteria strictly stated that both pain and progressive loss of motion had to be present for inclusion. However, it is expected that this effect would have occurred equally in both groups, and it is unlikely to have influenced the outcomes. Vastamäki et al. clearly showed that the length of symptoms and restriction of motion are shorter than originally described, and the focus of the present study was to specifically investigate the effect of a single corticosteroid injection in the symptomatic stage in patients with both pain and stiffness. 34
The inclusion of a placebo group would have been beneficial to investigate the effect of natural recovery and resolution of pain, but given the retrospective nature of the project, this was not possible. Finally, six experienced musculoskeletal physiotherapists assessed range of motion. Repeated longitudinal measurement of shoulder motion may not be reliable and reproducible, introducing the potential for measurement error. Tveita et al. documented intraclass correlation coefficients (ICCs) and smallest detectable differences (SDDs) in 32 patients with adhesive capsulitis using two observers. 35 The ICC ranged from 0.77 to 0.91 (abduction, flexion, internal and external rotation) for the affected shoulder, while the SDD (for a 90% probability) ranged from 13° to 24°. Hayes et al. investigated the inter-rater and intra-rater reliability of the goniometry method. 24 They demonstrated fair to good reliability with inter-rater reliability ranging from 0.64 to 0.69 and intra-rater reliability from 0.53 to 0.65. It therefore cannot be entirely excluded that measurement bias was introduced; however, it is again expected that the effect would have occurred in both groups and it is unlikely that this would have influenced the outcomes.
Conclusion
The results of this study suggest that injection of a single dose of intra-articular cortisone does not have a genuine short-term benefit in middle-aged female patients with idiopathic adhesive capsulitis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.