
Abstract
Background
Arthroscopic rotator cuff repair (ARCR) surgery is often recommended to reduce pain, restore function, and improve quality of life in patients with rotator cuff tears. Several factors can influence how effectively patients manage their pain, follow rehabilitation guidelines, and perceive their overall recovery, including patient perspectives, socioeconomic status, and beliefs on rehabilitation. Understanding these characteristics is crucial to optimizing patient outcomes and modifying rehabilitation approaches to meet specific patient requirements.
Objective
To obtain an in-depth understanding of patient perspectives, socioeconomic status, and beliefs on rehabilitation after ARCR.
Methods
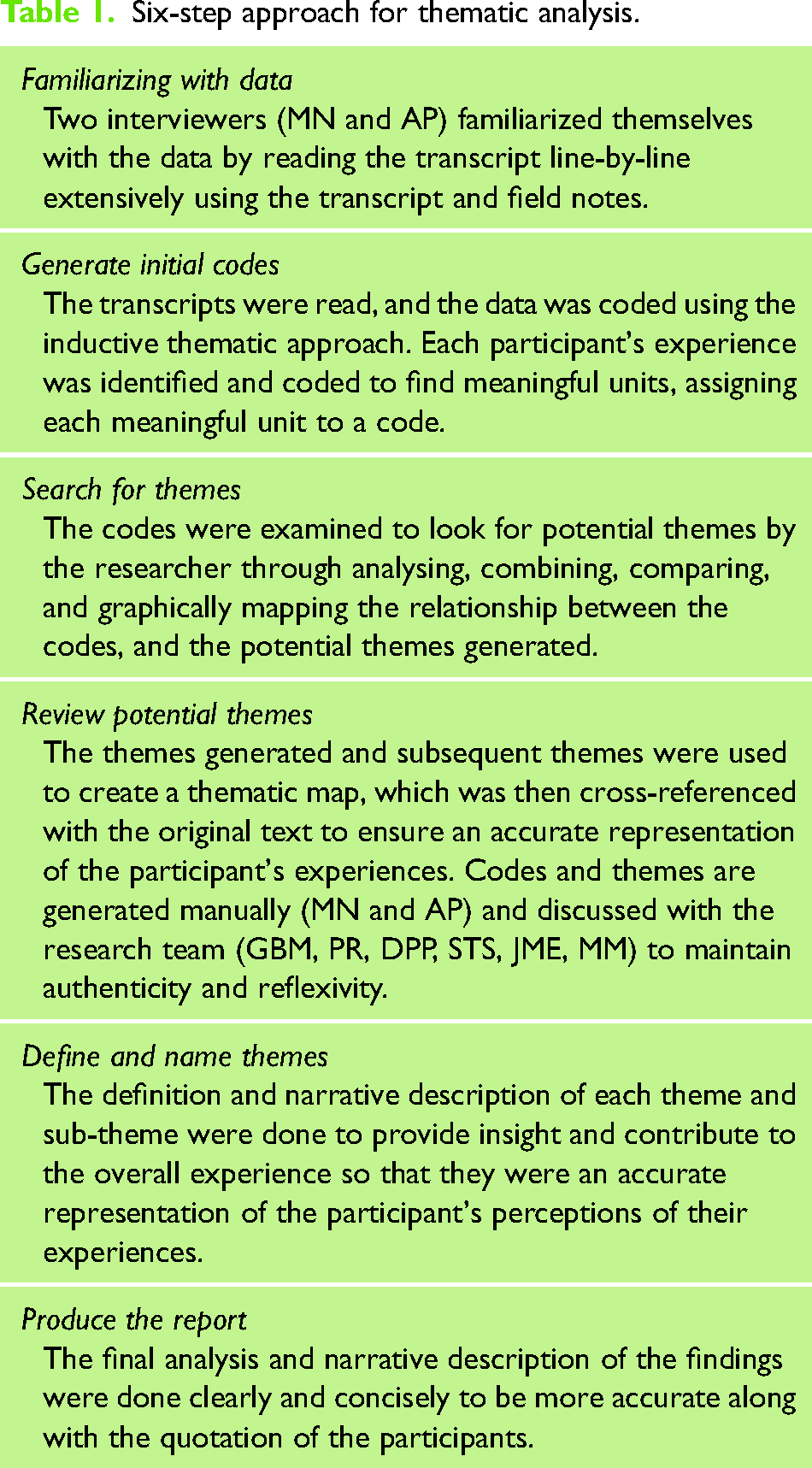
This qualitative study consisted of face-to-face semi-structured interviews with 13 participants who underwent ARCR. Interviews were recorded, transcribed, and analysed using a six-step approach as proposed by Braun and Clarke.
Results
The mean age of the included participants was 53 ± 8.07 years, with 76% being male with most of the participants belonging to lower middle and upper lower socioeconomic status. Three major themes emerged from the interview: 1) Role of healthcare provider, 2) Socio-environmental factors, and 3) Cognitive-behavioural response.
Conclusion
Our findings imply that rehabilitation strategies should incorporate a more comprehensive patient-centred approach that considers a wider range of factors influencing compliance with therapy and overall rehabilitation.
Introduction
Rotator cuff tears are a prevalent cause of shoulder pain and disability, particularly among older adults, with incidences increasing with age. Rotator cuff tears affect about 25% of people in their sixties, and this number increases to about 50% in people who are 80 years of age and beyond. 1 Rotator cuff tears not only impair a person's ability to perform daily activities but also negatively impact personal, social, and economic well-being. 2 Conservative treatment usually consists of modifying activity, stretching, deltoid and periscapular muscle strengthening exercises, anti-inflammatory drugs, and corticosteroid injections.3,4 However, if symptoms persist despite conservative measures, arthroscopic rotator cuff repair (ARCR) may be indicated, with a notable rise in ARCR procedures over the past decade. 5
Post-operative rehabilitation following ARCR has been shown to aid recovery, enhancing functional outcomes.6–8 Available scientific literature guides the post-operative rehabilitation following the ARCR procedure.5,9 Restoring flexibility, muscle strength, and enabling a return to regular activities such as work, and leisure are the primary objectives of rehabilitation. 10 Patients experience a lot of uncertainties in post-operative rehabilitation, such as how to best balance the need to maximize return to work and other functional and recreational activities with the safeguarding of the repaired and healing tissue. 11 Nevertheless, patient involvement and motivation throughout the rehabilitation program are key factors in enabling the return to activities. 12 Non-compliance with post-operative rehabilitation has indeed been identified as a significant predictor of rotator cuff re-tear and suboptimal outcomes following ARCR. 7 Compliance with post-operative rehabilitation is essential for ARCR repair to be successful. Various types of regimens have been explored to improve patient compliance and the efficacy of rehabilitation following ARCR.13–15
Psychological impairments also contribute to patients’ perceptions of their disease. Patients with impaired psychological status often experience increased shoulder pain and reduced shoulder function, leading to a worse quality of life. Following a multidisciplinary approach that incorporates biological, psychological, and social interventions is important to achieve better results.12,16 Patients with altered sleep quality and sleep efficiency, impaired pain processing, and central sensitization may experience less effect from ARCR. 17 Social health determinants can create barriers leading to poorer clinical and patient-reported outcomes following ARCR. These include an increased risk of post-operative complications, failed repairs, higher rates of revision surgery, and reduced ability to return to work.18,19
Socioeconomic status and patient beliefs are known to affect pain perception and engagement in self-management, which, in turn, impacts recovery.20,21 Individuals from lower socioeconomic backgrounds are more likely to experience poorer health outcomes, including shorter life expectancies and a higher prevalence of chronic illnesses. 22 People with lower socioeconomic status have less access to post-operative care and face poorer outcomes following ARCR. 23 Besides, patient perspectives and beliefs may significantly shape patient attitudes and engagement toward rehabilitation, influencing their pain perception and overall satisfaction with recovery. 24
To develop individualized rehabilitation programs and optimize physiotherapy interventions specifically, it is essential to understand patients’ perspectives, socioeconomic status, and beliefs on their post-ARCR rehabilitation. Many individuals travel 200 to 300 kilometres for consultations at our tertiary care hospitals due to a lack of facilities for arthroscopy procedures and trained surgeons in local hospitals. After being discharged, patients return for suture removal in the second week. The typical follow-up timeline includes visits at 6 weeks, 3 months, 4 or 6 months, and 1 year post-operatively. Overall, adherence to these follow-up visits is relatively good, and exercise progression is planned based on the patient's presentation during each visit to the hospital. Gaining this insight can inform improvements in long-term outcomes and enhance the physiotherapist's ability to offer a more patient-centred approach. This qualitative study explores patient perspectives, socioeconomic status, and beliefs about rehabilitation following the ARCR procedure.
Methods
Study design and ethics
A qualitative exploratory study was conducted based on an interpretive phenomenological approach, 25 and the reporting is done following the consolidated criteria for reporting qualitative research guidelines. 26 The study received approval from the Institutional Ethics Committee (IEC2 no: 205/2023) and the trial was registered in the Clinical Trials Registryof India (CTRI/2023/08/056789).
Participants and recruitment
A qualitative study, applying a face-to-face semi-structured in-depth interview technique, was conducted on patients attending the outpatient physiotherapy department in a tertiary care hospital between October 2023 and January 2024. Purposive sampling was used to include participants in the study if they were aged between 35 and 65 years and underwent rehabilitation for at least 4 months following the ARCR and were able to speak English/Kannada language.
The age range for participants was set between 35 and 65 years, per the protocol ethics approval and trial registration. This range was chosen to avoid including a wide age group. The frequency of RC abnormalities increases with age, peaking between the third and sixth decades of life. 27 We established a higher age limit of 65 years to mitigate the potential impact of senescence disorders. Participants diagnosed with pre-existing or ongoing cognitive impairment or had undergone major concomitant procedures such as muscle-tendon transfer, patch augmentation, any associated fractures around the shoulder complex, and repair for re-tears of the rotator cuff tendons were excluded from the study.
The participant information sheet was provided, and written informed consent was obtained from all the participants after providing a detailed explanation of the study procedure. Separate written consent was obtained for audio-recording the interview. All participants following ARCR surgery had undergone standard rehabilitation protocol which included six weeks of immobilization, passive shoulder mobilization, and periscapular activation progressing to active and active-assisted range improvement and advanced strengthening exercises.
Data collection
The primary investigator (MN), fluent in English and Kannada languages, conducted the interview. MN received formal training and certification in face-to-face interviews while pursuing a master's degree in physiotherapy. This study was conducted as a part of her student thesis. Before the interview participants were screened for cognitive impairment using a Mini-cog scale, 28 demographic details, the current level of pain, and disability were assessed using the shoulder pain and disability index (SPADI), 29 along with the reports of shoulder ultrasound, and medical and surgical procedure.
The interview guide was developed based on the literature review and the expert opinions of the investigators.7,12,30 The interview guide framework was sent to four experts for review and feedback. The experts included three physiotherapists and one clinical psychologist, all trained in conducting and publishing qualitative research. Three experts had received formal training and published qualitative studies as a part of their PhD and student research projects (PR, DPP, STS)). The experts critically reviewed the items, scored the questions, and provided suggestions, which were incorporated into the final revised interview guide.
Four mock interviews were conducted to assess the reflectiveness and flow of the questions under the supervision of the research team. These mock interviews were not considered for the final analysis. Only minor changes to the interview guide were made to maintain the fluidity of the questions. Based on patients’ preferences, the interview was conducted in the Kannada language in a quiet room at the Department of Physiotherapy. All interviews were audio-recorded by the first author. Only the interviewer and the participant were present during the entire interview. Before starting the study, the interviewer established a rapport with the participant. Each interview lasted for approximately 30–45 min and probes were used to obtain additional information. Field notes were used during the interview and data collection continued until no new information emerged and thematic data saturation was achieved.
Diagnostic imaging findings and surgical history of the participants
Most of the participants had tears, identified on magnetic resonance imaging scans or diagnostic ultrasound ranging from isolated full-thickness tears of the supraspinatus tendon to near-complete tears of the supraspinatus, infraspinatus, and subscapularis tendon. Our participants had undergone both single- and double-row ARCR of the tendons.
Data analysis
Descriptive statistics were used to analyse the demographic characteristics of the participants. Verbatim transcription of audio-recordings from Kannada to English was done manually. Interviews were analysed by two investigators independently (MN, AP) using a six-step approach to thematic analysis as proposed by Braun and Clarke. 31 The analytical steps were performed as shown in Table 1 and validated throughout by the investigating team and thematic mapping was conducted based on emerging themes. Once no new information was derived from the interviews and the primary analytic structure was considered stable, it was decided that further interviews would not yield any new information that could add to the themes, and interviews were stopped. Following the transcription, the data was not returned to the participants. The researcher wiped out the audio tapes permanently after transcribing them verbatim. An individual participant ID was assigned to the transcribed interviews, which was unaffiliated with the participants’ identities.
Six-step approach for thematic analysis.
Results
Characteristics of the participants
A total of 32 participants were screened, and 13 participants agreed to participate in the study. Eleven participants were excluded as they did not meet the eligibility criteria (three patients with cognitive impairments; five patients with major concomitant procedures; and three patients who underwent revision ARCR), further eight were not willing to participate due to time constraints. The demographic data of the participants is represented in Table 2. Thirteen participants completed the interview with a mean (SD) age of 53 (8.07) years; consisting of 10 males (76%) and 3 females (23%). The pain and disability scores measured using SPADI presented in Median [IQR] were 7 [1, 23] and 15 [6, 37] respectively; with a median total score of 20 [9, 56], which reveals that our study participants had a mild level of pain and disability. The socioeconomic status, pre-injury occupation of the participants, and month of interview post-ARCR are displayed in Table 2.
Participant characteristics.
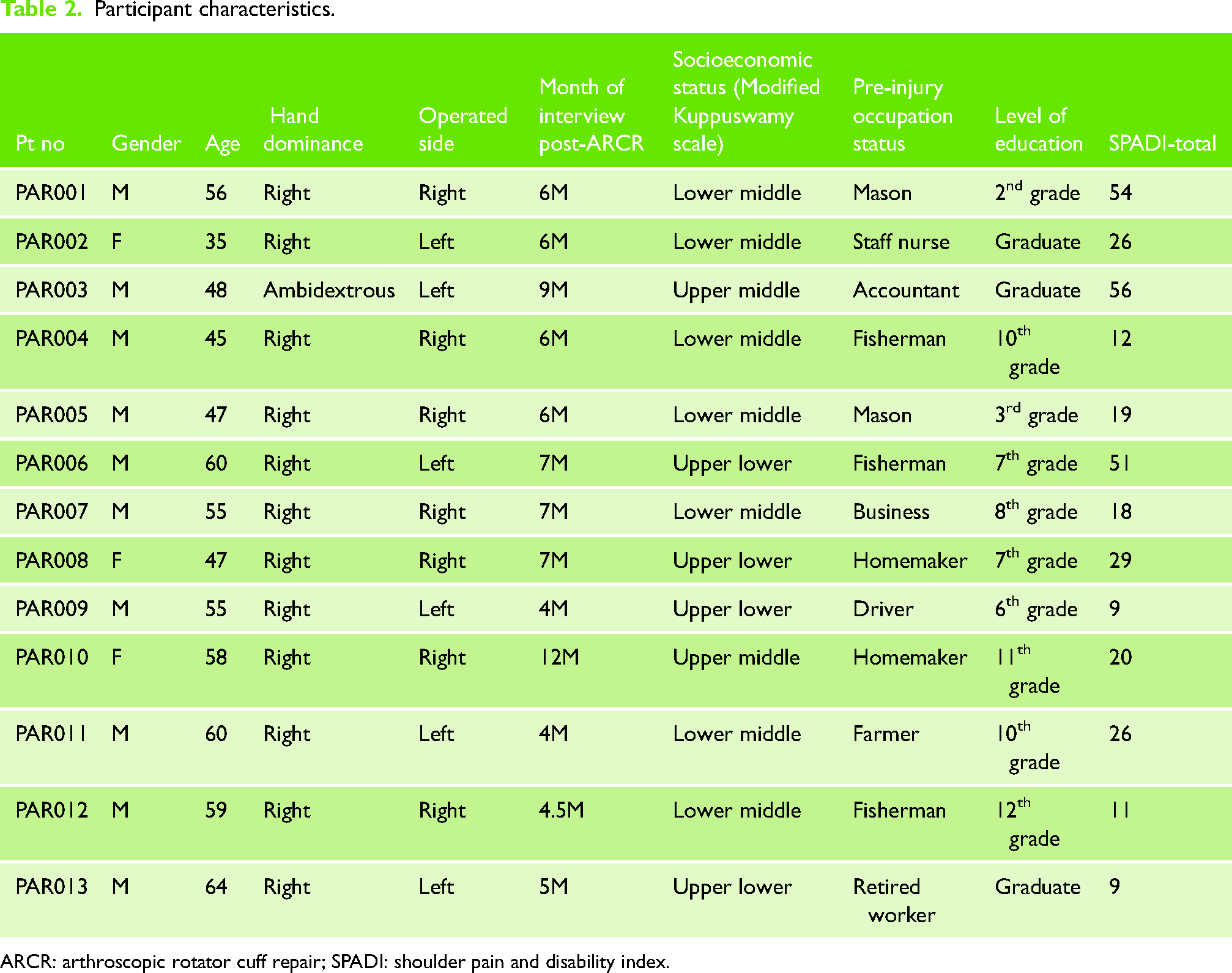
ARCR: arthroscopic rotator cuff repair; SPADI: shoulder pain and disability index.
Three main themes were constructed based on participants’ perceptions as displayed in Figure 1. The themes included i) the Role of health care provider, ii) Socio-environmental factors, and iii) Cognitive-behavioural responses. Few quotations are mentioned in the description. Each participant is assigned a number to ensure anonymity.
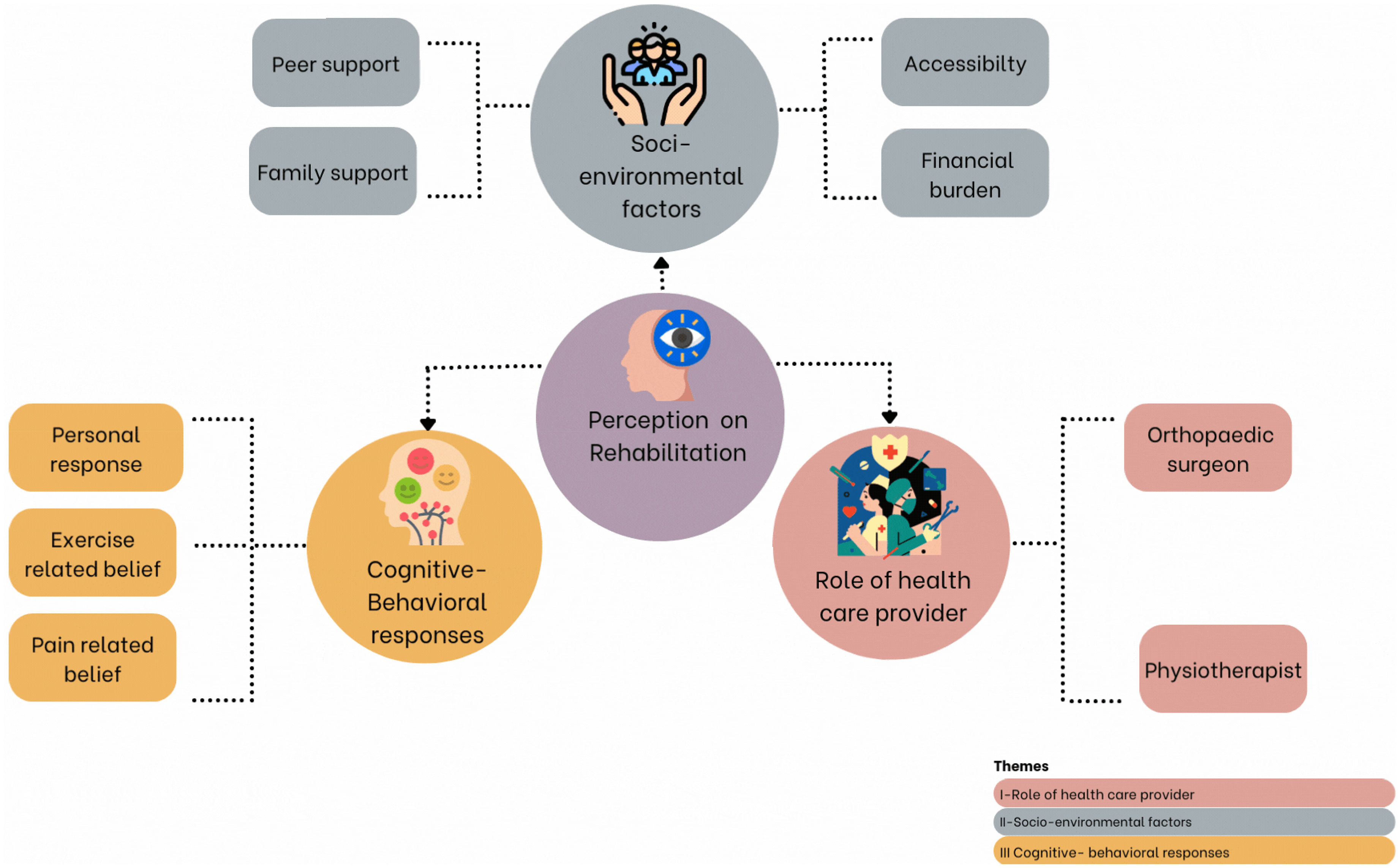
Thematic mapping on patient perspectives, socioeconomic status, and beliefs on rehabilitation after arthroscopic rotator cuff repair.
Themes
The main themes identified from the data were i) Role of the healthcare provider, ii) Socio-environmental factors, and iii) Cognitive-behavioural responses.
1) Role of orthopaedic surgeon
Eight participants were not aware of the importance of rehabilitation in their post-operative recovery. They placed their trust in the orthopaedic surgeon and stated that the guidance provided by the surgeon significantly impacted the results. The surgeon positively influenced them either by educating and creating awareness about the condition, by explaining the importance of exercise, and by providing examples of de-identified patients who worsened because of a lack of adherence to exercise. They also reported a perception that the surgeon provided psychological support, assuring the patient that healing is a gradual process, and encouraged them to stay optimistic for improvements over time.
The doctor had already informed me that I must perform all exercises exactly as the physiotherapist has taught me to see improvements (PAR001)
The doctor informed me about patients who had not been exercising and were not showing any improvement (PAR003)
2) Role of physiotherapist
Confidence in the physiotherapist was considered to impact the performance of exercises. The participants stated that the physiotherapist actively involved them in the rehabilitation process by providing encouragement and positive reinforcement, educating them on the importance of exercises, and regularly monitoring their progress.
Every time I visited my physiotherapist, she encouraged me by showing my improvements, look how much you have improved! (PAR010)
She used to send me exercise videos and ask about progress. Overall, I'm satisfied with how things were handled (PAR002)
1) Financial burden
Finances played a significant role in deciding whether to access physiotherapy services, as this condition requires a long recovery period. Many people encountered challenges in financing both the surgery and rehabilitation, as their insurance covered the surgery but not the rehabilitation services, necessitating out-of-pocket payments.
I have insurance, but now I have been told it does not cover rehabilitation services (PAR001)
I had to borrow money for my surgery and again had to pay separately for physiotherapy… It's difficult to manage these expenses every time I come for a follow-up visit (PAR006)
Only two of the 13 participants were covered under the government schemes, so they did not face any difficulty paying for both surgery and physiotherapy.
I did not have any trouble since I am a government employee; the expenses were covered by my insurance (PAR003)
I had insurance, luckily, I applied for it last year, so it got covered, and hence I had to pay less (PAR010)
Support from family helped the patient confront the financial crisis. Many participants faced significant financial difficulties but received financial assistance from their family members, who helped them manage the financial burden during surgery.
I don’t have insurance, so my relatives helped by lending me money for the overall hospital expenses (PAR009)
I had to get help from my friends and family to arrange the money (PAR007)
2) Family support
Ten participants highlighted the importance of receiving support from their family members during the exercises. This shows how the encouragement and assistance from their families motivated them. Their positive attitude toward the exercises inspired the participants to stick to their regular exercise routines.
My wife used to help me in doing all the exercises, and I had good support from the family (PAR006)
My son helped me in doing all exercises, I used to do before he left for college and again after he returned (PAR007)
However, three participants highlighted a lack of adherence to the home exercise program because their family members were unavailable during exercise.
Usually, he does all his work, and by the time he's finished, it's too late for him to help me out. I had to adjust to his schedule to get my exercises done, so I couldn't complete all of them (PAR010)
I used to avoid exercises that required assistance. I would wait for someone to be available, but everyone seemed to be busy (PAR013)
Our female participants, who are accustomed to wearing traditional Indian sarees, expressed difficulty in draping and pinning a saree due to shoulder pain and stiffness. Similarly, some men faced challenges in wearing dhotis, which led them to resort to alternative clothing that they were not used to wearing.
3) Peer support
Some individuals who returned to work mentioned being supported by their colleagues, which motivated them to exercise. They also found encouragement from friends with similar experiences who shared the benefits of rehabilitation and the positive results they saw after their procedures.
My colleagues advised me to take breaks and exercise (PAR002)
4) Accessibility
Participants preferred exercising at home due to financial constraints and remote locations, limiting their access to physiotherapy rehabilitation centres.
It is too far to travel to the clinic to avail of rehabilitation services (PAR006)
I must pay a large amount, rather I do exercises by myself at home (PAR009)
Telerehabilitation could not be implemented for all participants because many participants did not have smartphones to share videos or monitor exercises using video calls. Our hospital's standard rehabilitation protocol does not include telerehabilitation. Patients with smartphones often requested exercise videos. The therapist helped by creating videos to serve as reference guides for their home programs.
1) Pain-related belief
The highly individual experience of pain significantly impacts exercising and functional abilities, serving as both a motivator and a barrier to engaging in rehabilitation. Those who maintained a consistent exercise routine reported improvements in daily activities, reduced pain, and decreased stiffness early in the rehabilitation process, which helped them adhere to their exercise regimen more effectively.
Well, I used to feel that my hand had become stiffer after wearing a sling for 6 weeks. Since I started exercising, I can move my hand more freely and can do most of my work (PAR011)
If I had not exercised, my hand would have become weaker, stiffer, and more painful (PAR003)
Some participants mentioned experiencing common post-exercise soreness and pain but continued to exercise despite discomfort.
Even after enduring pain, I kept up with my regular exercise routine (PAR010)
Experiencing pain after exercising is common like the discomfort felt when starting at the gym for the first time (PAR005)
However, five participants found that pain was a barrier to exercise. They used pain as a cue to modify or skip their regular exercise program.
It was painful, so I just stopped exercising (PAR006)
Whenever I experience pain, I cut down on my exercises (PAR004)
2) Exercise-related belief
Nine participants emphasized the importance of rehabilitation, noting changes in their daily activities, especially in the early stages. They believed exercise significantly improved their progress and overall quality of life.
Without regular exercise, I wouldn't be able to perform most of my daily tasks (PAR007)
Exercise significantly improved my daily life. Previously, simple tasks like combing hair or lifting a jug of water were a struggle. However, after incorporating exercises into my routine, these activities gradually became easier (PAR005)
Participants stressed that the exercise is a structured and distinctive process detached from daily activities, marking an important stride toward improvement.
Exercise is a structured activity. Regular tasks differ from specific exercise activities (PAR003)
Exercise must be approached systematically; results don't come easily otherwise (PART010)
In contrast, only four out of 13 participants believed that they could improve their strength and mobility by performing basic tasks such as cleaning the house and taking regular walks.
I don't believe exercise is necessary. I think I can gain strength from doing household chores and staying active (PAR012)
Occasionally, I visit farms and take a walk in the field. I don't set aside time specifically for exercise; I believe these activities are sufficient (PAR001)
3) Personal response
Four out of 13 despite the reassurance and education provided by the physiotherapist expressed fear of reinjury while performing daily activities and exercising. Consequently, they were apprehensive about pushing their limits during exercise and only did what they felt comfortable with.
I am scared. What if something happens, and I end up having another surgery? (PAR004)
The doctor told me my bone quality is weak, so I take a little extra precaution while exercising (PAR002)
Eight of our participants were dependent on their families for physical support, needing assistance with daily activities and exercises. They also experienced emotional distress, including feelings of depression, dependency, and demotivation.
I used to wish someone could help me with exercises. I was reliant on my family (PAR002)
I feel like many people have suffered because of me, especially my wife, as she had to take care of everything (PAR005)
However, 10 participants saw their dependency as a motivation to strive for greater independence and alleviate the burden on their families.
My job required me to drive outside of the city, so I had to become independent (PAR009)
I want to return to work because I am the sole breadwinner for my family and cannot rely on others (PAR006)
Discussion
This study aimed to explore patients’ perspectives, socioeconomic status, and beliefs on rehabilitation following ARCR. Several critical factors were identified that should be considered when designing post-operative rehabilitation programs, as they can significantly influence patients’ adherence to the prescribed exercises.
Role of healthcare provider
Noteworthy is the participants’ lack of comprehensive understanding of the benefits of exercise for their condition. However, when surgeons and physiotherapists provided education on the importance of rehabilitation, patients’ confidence in the prescribed exercise program improved. This observation aligns with previous research on low back pain, which showed that information from healthcare providers strongly influenced patients’ beliefs and adherence to exercise therapy. 32 A previous study conducted in India found that several factors contribute to comfort and trust in the healthcare system. These factors include having a good rapport with the doctor, the doctor demonstrating personal involvement with the patient, and the doctor being both behaviourally and culturally competent. 33 Having a single specialist perform all procedures and interact with patients during follow-up sessions fostered positive responses and trust in the operating surgeon.
Socio-environmental factors
A significant social barrier to rehabilitation observed in our study was financial constraints. Many participants reported that their health insurance did not cover the cost of physiotherapy services, impeding access to necessary services. Financial barriers to rehabilitation have been widely recognized in the literature, with studies suggesting that a lack of insurance coverage is a major determinant of inequitable healthcare access.34,35 Coordinated efforts among healthcare providers, insurers, and policymakers are essential to address financial disparities in rehabilitation services to optimize rehabilitation outcomes.
Family support was found to be particularly important during the early stages of rehabilitation, especially when passive mobilization is part of the standard protocol. Participants with adequate family support reported greater ease in adhering to their exercise regimens. Conversely, those lacking caregiver support struggled to maintain their prescribed exercise routines. This finding resonates with existing literature, which has shown that family and peer support play a pivotal role in motivating patients to adhere to rehabilitation exercises. 36
Accessibility also posed challenges for participants, particularly those from rural areas with limited access to rehabilitation services. These participants expressed a preference for home-based exercises due to distance, lack of insurance coverage, and geographical barriers. Similar challenges have been noted in other studies where patients from rural areas faced logistical difficulties in accessing physiotherapy services. 37
Cognitive-behavioural response
Pain management was another critical factor influencing adherence. Participants who experienced pain during exercises often interpreted it as a signal to reduce exercise intensity. Those who underwent supraspinatus or multiple tendon repairs reported higher levels of pain and disability, which in turn affected their adherence to the rehabilitation program. A similar finding pattern was observed in a study in which participants with shoulder pain were prescribed self-management, highlighting pain as a primary cause for avoiding certain exercises. 38
Psychological factors, including depression, fear of re-injury, and demotivation, were identified as key determinants of rehabilitation. Several participants reported emotional distress, which hindered their ability to adhere to prescribed exercises. Psychological distress is widely recognized as a barrier to successful rehabilitation, and studies suggest that integrating psychological support into rehabilitation programs can enhance patient adherence.39,40 Interestingly, hand dominance also appeared to affect exercise adherence. Participants who had surgery on their non-dominant hand exhibited lower adherence to their rehabilitation exercises, likely due to fewer disruptions in their daily activities. This phenomenon has been observed in previous studies, where reduced functional impairment led to lower motivation for rehabilitation. 32 More research is required to determine the clinical implications of this, potentially, spurious, finding.
Limitations
While these findings offer valuable insights, they should be interpreted with caution due to several limitations. The potential for recall bias exists, as participants were asked to reflect on their rehabilitation experiences retrospectively. Secondly, we did not systematically evaluate adherence to the rehabilitation or outcome in a standardized manner and thus interrelations or impact of barriers and facilitators on these, as this was out of the scope of the present qualitative study. But overall, despite completing the prescribed rehabilitation program, many participants expressed dissatisfaction with their post-surgical recovery. Most were manual workers, such as fishermen, farmers, and masons, and were unable to return to their pre-injury level of work performance. This finding underscores the need for rehabilitation programs that are tailored to the specific functional demands of patients’ occupations, as suggested in earlier research. 41 Next to that, the homogeneity of our sample, consisting of primarily male manual workers, limits the generalizability of the results. Lastly, responder bias may have also influenced the findings, as the same therapist conducted both the treatment and interviews. Future research should explore patient perspectives, socioeconomic status, and beliefs across diverse healthcare settings and sociocultural contexts and link them to compliance and outcome to enhance our understanding of factors affecting rehabilitation adherence to physiotherapy after ARCR.
Conclusion
Our research shows that individuals’ perceptions of post-surgical rehabilitation following ARCR are significantly influenced by the role of the healthcare provider, socio-environmental factors, and cognitive-behavioural responses. The findings indicate that effective rehabilitation strategies should extend beyond addressing physical limitations to include a comprehensive, patient-centred approach. This approach must account for various factors impacting treatment outcomes, such as peer and family support, accessibility to rehabilitation, financial burden, patient beliefs, and personal responses. Incorporating these aspects throughout the rehabilitation process may enhance compliance, resulting in improved recovery outcomes and patient satisfaction.
Footnotes
Acknowledgements
The authors would like to thank all the participants for spending their valuable time and taking part in our study. We wish to thank Dr Vivek Pandey for his continued support and guidance. Declaration: We guarantee that we are submitting our original work, we have rights to the work, and that we are submitting the work for first publication in the Journal that it is not being considered for publication elsewhere and has not already been published elsewhere, and we have obtained and can supply all necessary permissions for the reproduction of any copyrighted work not owned by us.
Contributorship
AP, MN, and GBM were responsible for generating hypothesis; AP, MN, and GBM were involved in research design and development; MN was involved in data collection; AP, MN, GBM, DPP, STS, and PR were responsible for data analysis; GBM, MN, MM, JME, PR, AP, DPP, and STS were responsible for interpretation of findings; MN and AP were responsible for manuscript writing; GBM, STS, DPP, PR, JME, and MM manuscript review and approval.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
IEC2 no: 205/2023
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AP
Informed consent
All participants were provided with participant information sheet and written informed consent was obtained.
Trial registration
CTRI/2023/08/056789