
Abstract
Purpose
To summarize complication rates, reoperation rates, length-of-stay (LOS), patient-reported outcome measures (PROMs), and range of motion following total shoulder arthroplasty (TSA) in patients with preexisting psychiatric disorders (PDs) compared to controls.
Methods
Three databases (MEDLINE, PubMed, and EMBASE) were searched from inception to 4 March 2024 to identify studies comparing outcomes between patients undergoing anatomic (aTSA) or reverse TSA (rTSA) with or without a preexisting psychiatric condition. The authors adhered to the preferred reporting items for systematic reviews and meta-analyses and revised assessment of multiple systematic review guidelines. Data on demographics, as well as postoperative complication rates, reoperation rates, LOS, PROMs, and range of motion were extracted from included studies. PROMs included the American Shoulder and Elbow Surgeons (ASESs) score, and visual analogue scale (VAS) pain score. Meta-analyses were conducted for outcomes reported by multiple studies, with odds ratios (ORs) and mean differences (MDs) as effect measures for continuous and dichotomous outcomes, respectively.
Results
Thirteen studies were included in this review, comprising a total of 820,831 TSA patients. The PD group (71.0% female) consisted of 150,432 patients (mean age: 67.6 ± 9.9) with a mean follow-up time of 34.1 ± 30.1 months. The control group (58.1% female) consisted of 670,399 patients (mean age: 69.4 ± 10.7) with a mean follow-up time of 39.1 ± 36.0 months. The PD group had significantly higher rates of complications and reoperation. The PD group also reported significantly lower postoperative ASES scores, higher postoperative VAS scores, and inferior postoperative abduction. There were no significant differences in postoperative LOS, forward flexion, internal rotation, or external rotation.
Conclusion
Patients with preexisting PDs may have a one-and-a-half times higher odds of postoperative complication or reoperation, as well as significantly worse postoperative pain and PROMs. Identification of at-risk individuals with preexisting psychiatric conditions and preoperative referral to a mental health specialist to optimize psychiatric conditions may benefit this patient cohort ahead of their shoulder arthroplasty procedure.
Level of evidence
IV.
Keywords
Introduction
Total shoulder arthroplasty (TSA) is a well-established treatment for patients experiencing persistent pain, reductions in range of motion, or strength deficits secondary to glenohumeral arthritis and related pathologies. 1 Specifically, TSA refers to two distinct modalities: anatomic TSA (aTSA), which aims to recreate the native biomechanics of the glenohumeral joint, and reverse TSA (rTSA), which involves inverting the concavity of the native glenoid and humerus to essentially reverse the native anatomy. 1 Despite unique indications, both operations have demonstrated similar functional outcomes and complications rates and have thus gained significant popularity in recent years.2,3 In fact, between 2011 and 2017, the incidence of TSAs increased at a rate even greater than total hip and knee arthroplasties. 4
While the surgical considerations for TSA are heavily emphasized, patients’ preexisting psychiatric histories are often overlooked. Previous studies have demonstrated that the presence of psychiatric disorders (PDs) is associated with poorer outcomes following orthopedic procedures, such as anterior cruciate ligament reconstruction.5,6 One proposed explanation for this association is an impaired adherence to postoperative rehabilitation protocols, thus delaying functional restoration and worsening pain perception. 7 This is especially problematic as the global prevalence of PDs, particularly mood and anxiety disorders, have significantly increased in recent years.8,9 A recent meta-analysis of 174 studies reported that 17.6% of the global population meets the criteria for at least one PD, while 29.2% of the population will experience a PD at some point in their lives. 10
It is imperative for surgeons to try and optimize patient outcomes following operative interventions. This necessarily implies that research must be directed at identifying which patient factors influence postoperative outcomes and assess the strength and direction of those associations. As such, this review and meta-analysis aims to evaluate the impact of preexisting PDs on postoperative outcomes following TSA.
Materials and methods
This systematic review was reported according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines and performed in accordance with the revised assessment of multiple systematic review recommendations.11,12
Search criteria
Three online databases (PubMed, MEDLINE, and EMBASE) were searched from database inception to 4th March 2024, to identify literature evaluating the impact of mood and anxiety disorders on clinical outcomes following RTSA and ATSA. Comprehensive search terms including “shoulder arthroplasty,” “reverse total shoulder arthroplasty,” “mood disorder,” “anxiety,” and “depression” were utilized (Supplemental Table S1). MeSH and EMTREE terms were utilized to increase search sensitivity and supplemented with free text terms.
Studies were selected for inclusion if they met the following criteria: (1) specific patient group or subgroup with a preoperative mood and/or anxiety disorder (2) patients undergoing RTSA or ATSA, (3) reporting on patient reported outcome measures (PROMs), rates of construct failure, complication rates, or related clinical outcomes (4) nonlaboratory human studies, (5) English studies. Exclusion criteria included (1) level of evidence V, (2) textbook chapters, (3) conference abstracts, (4) biomechanical studies, (5) cadaveric/animal studies, and (6) studies involving less than five patients.
Screening
Title and abstract screening were conducted by three authors (BS, VT, and RY), and conflicts that arose during this stage were resolved by consensus. A senior author (US) was consulted to review conflicts that could not be resolved. During full-text screening, studies were independently screened by the same three authors with disagreements being resolved in the same manner.
Assessment of agreement
The inter-reviewer agreement was evaluated using a kappa (κ) statistic throughout the screening stages. A priori classification was defined as follows: κ of 0.91–0.99 was near perfect agreement; κ of 0.71–0.90 was considerable agreement; k of 0.61–0.70 was high agreement; κ of 0.41–0.60 was moderate agreement; κ of 0.21–0.40 was fair agreement and a κ or ICC value of 0.20 or less was no agreement. 13
Quality assessment
The methodological index for nonrandomized studies (MINORS) criteria was used for quality assessment. Based on this criteria, noncomparative and comparative studies could achieve maximum scores of 16 and 24, respectively. 14 For noncomparative studies, an a priori classification based on a previous systematic review was used: 0–4 very low-quality evidence, 5–7 low quality, 8–12 fair quality, and scores ≥ 13 high quality. As for comparative studies, the following criteria was used: 0–6 very low quality, 7–10 low quality, 11–15 fair quality, 16–20 good quality, and ≥ 20 high quality. 14
Data extraction
Three authors (BS, VT, and RY) independently extracted and summarized data from included articles using Google Sheets software (Google LLC, Mountain View, CA, USA). Demographic data such as patient age at surgery, sex, mood/anxiety disorder status, follow-up time, loss to follow-up, were recorded. Details regarding the surgical procedure, such as whether aTSA or rTSA was performed, were also extracted. Outcomes included reoperation rate, complication rate, postoperative length-of-stay (LOS), American Shoulder and Elbow Surgeons (ASESs) score, visual analog scale (VAS) score, and range of motion (abduction, forward flexion, internal rotation, external rotation).
Statistical analysis
Meta-analyses were performed using Review Manager software (Review Manager (RevMan) (Computer program). Version 7.2.0. The Cochrane Collaboration, 2024.) for outcomes that were reported by two or more studies. A p-value of < .05 was set a priori as the threshold of statistical significance. Pairwise meta-analyses were performed using Mantel–Haenszel random effects models for dichotomous variables including reoperation rate and complication rate. Pairwise meta-analyses were performed using inverse variance random effects models for continuous variables including postoperative LOS, ASES score, VAS score, abduction, forward flexion, internal rotation, and external rotation. If studies did not report the standard deviation, the range was used to impute these values using a well-established technique by Walter et al. 15 Mean differences (MDs) and odds ratios (ORs) were calculated for continuous and dichotomous outcomes, respectively, along with their respective 95% confidence intervals (CIs), when the required parameters were available. The I² test was used to quantify heterogeneity, with values of <25% indicating low heterogeneity and values >75% indicating high heterogeneity. 16 Demographic data was presented descriptively using means and standard deviation or ranges for continuous variables and frequencies and percentages for dichotomous variables.
Results
Literature search
The initial search of the databases yielded 381 studies, with 135 being automatically filtered out as duplicates. Following title and abstract screening, 226 studies were deemed irrelevant, leaving 20 studies for full-text screening. Ultimately, 13 full-text articles satisfied the inclusion and exclusion criteria.17–29 The PRISMA flow chart is outlined in Figure 1. There was considerable agreement during the title and abstract stage (k = 0.896) and perfect agreement during the full-text stage (k = 1.00).
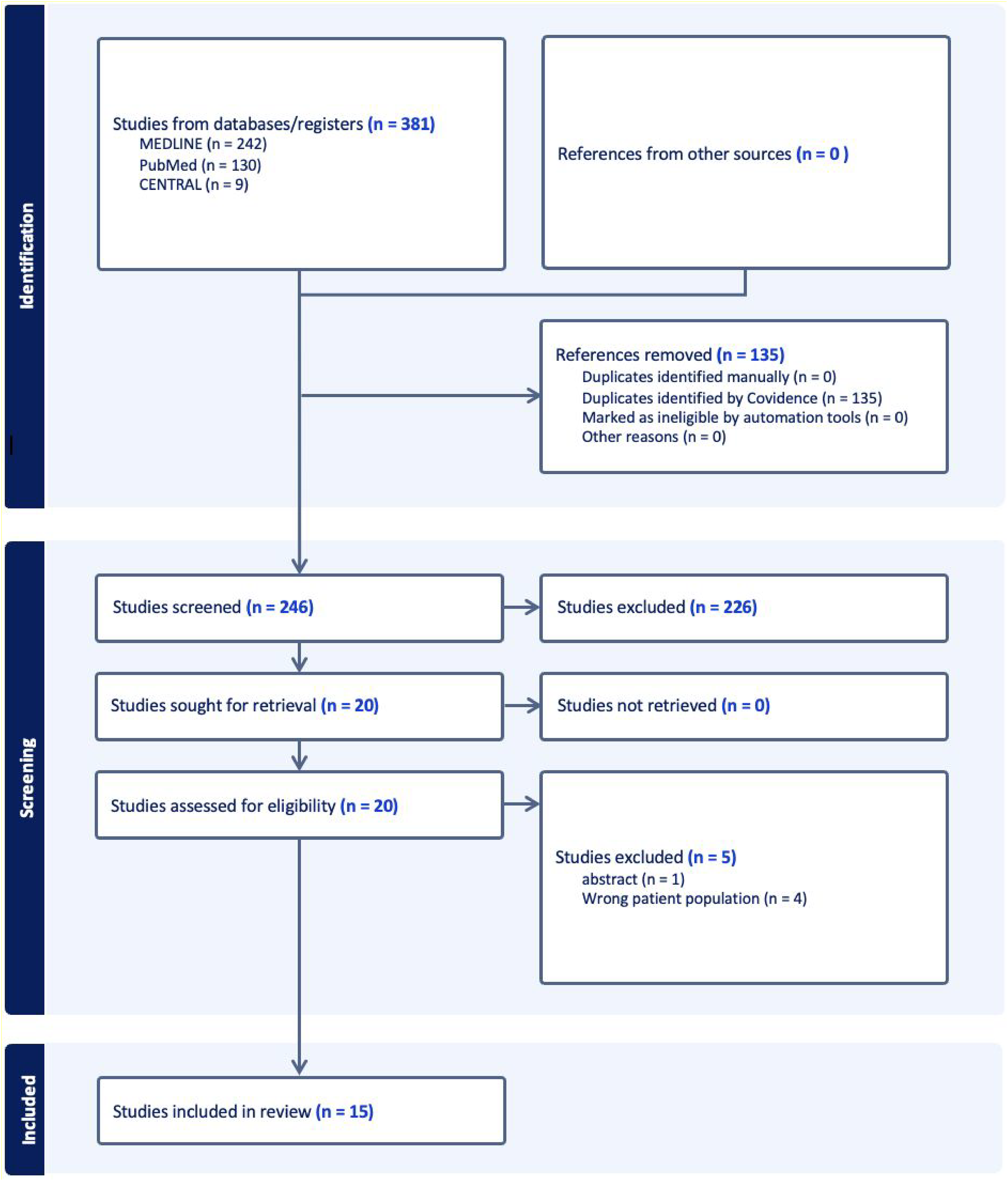
Preferred reporting items for systematic reviews and meta-analyses flow diagram representing a systematic review and meta-analysis of preoperative psychiatric disorders in patients undergoing total shoulder arthroplasty.
Study quality
Of the 13 studies included in this review, 12 were retrospective cohort studies (level of evidence III) and one was a case-control study (level of evidence III). The mean MINORS score for the 13 studies was 16.4/24 (Table 1).
Characteristics of eligible studies.
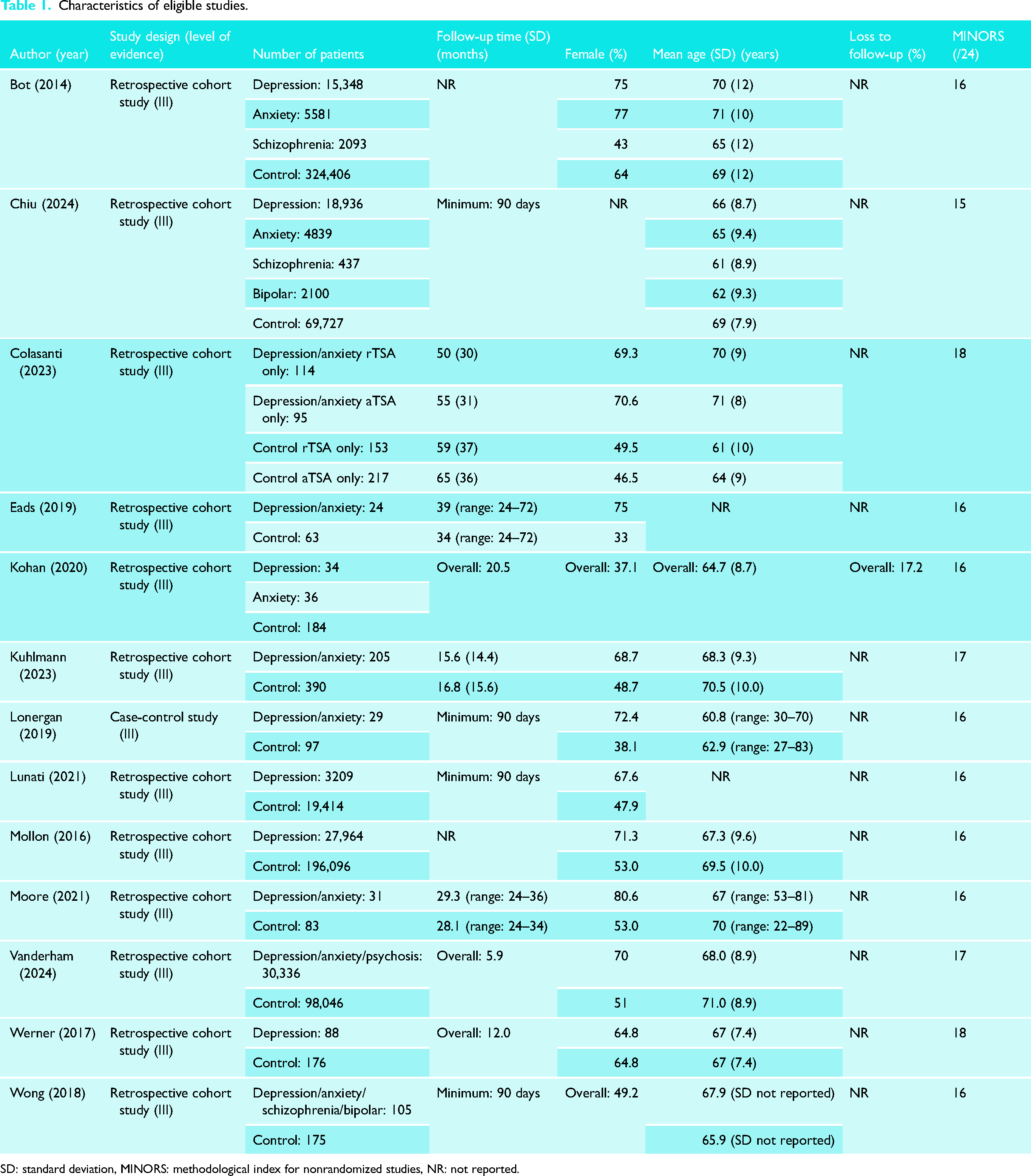
SD: standard deviation, MINORS: methodological index for nonrandomized studies, NR: not reported.
Study characteristics
Thirteen studies were included patients (18.3%) in this review, comprising a total of 820,831 patients.17–29 The PD group was composed of 150,432 with a mean age of 67.6 ± 9.9 years. Of the patients whose psychiatric diagnoses were specified, 65,579 had depression (81.3%), 10,456 had anxiety (13.0%), 2530 had schizophrenia (3.1%), and 2100 had bipolar disorder (2.1%). Female patients comprised 71.0% of patients in this group. The mean follow-up time in this group was 34.1 ± 30.1 months with four studies reporting a minimum follow-up time of 90 days. The control group was composed of 670,399 patients (81.7%) with a mean age of 69.4 ± 10.7 years. Female patients comprised 58.1% of patients in this group. The mean follow-up time in this group was 39.1 ± 36.0 months with four studies reporting a minimum follow-up time of 90 days. One study comprising 70 PD patients and 184 control patients reported an overall lost-to-follow up rate of 17.2%. 21 Study characteristics are summarized in Table 1.
Complications rate
Ten studies comprising 111,341 and 708,692 patients in the PD and control groups, respectively, reported on complications rates.17–20,22–27 A complication was defined as any adverse medical or prosthesis-related event occurring in the postoperative period, meaning that intraoperative complications were not considered. Mean follow-up times in the PD and control groups were 34.0 and 37.7 months, respectively. The PD group demonstrated a significantly higher complications rate than the control group with an OR of 1.47 (95% CI [1.36 to 1.58], p < .00001, I² = 86%) (Figure 2).
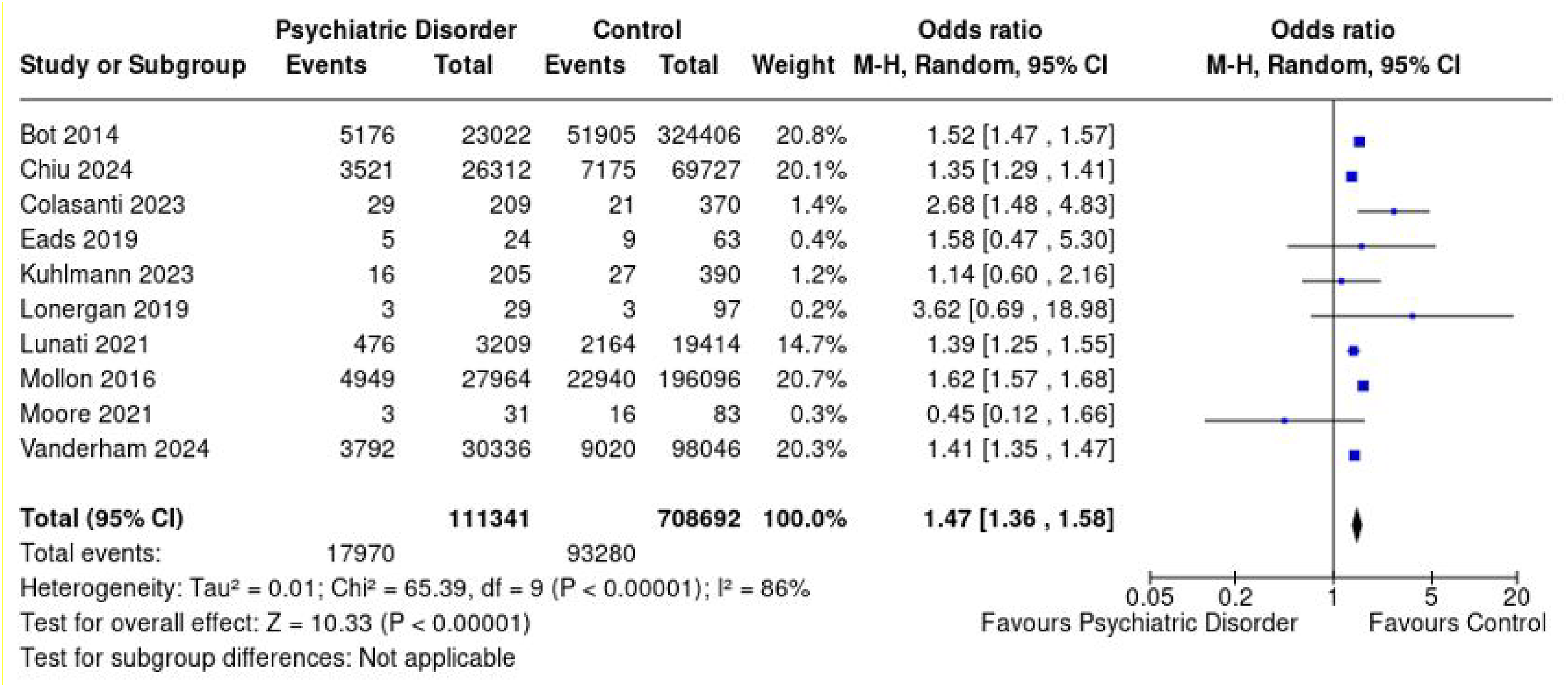
Forest plot demonstrating overall pooled odds ratio for complications rate of patients with psychiatric disorders and controls with associated 95% confidence intervals.
Reoperation rate
Six studies comprising 60,295 and 188,010 patients in the PD and control groups, respectively, reported on reoperation rates.18–20,22,24,27 Mean follow-up times in the PD and control groups were 34.4 and 38.7 months, respectively. The PD group demonstrated a significantly higher reoperation rate than the control group with an OR of 1.66 (95% CI [1.56 to 1.78], p < .00001, I² = 0%) (Figure 3).
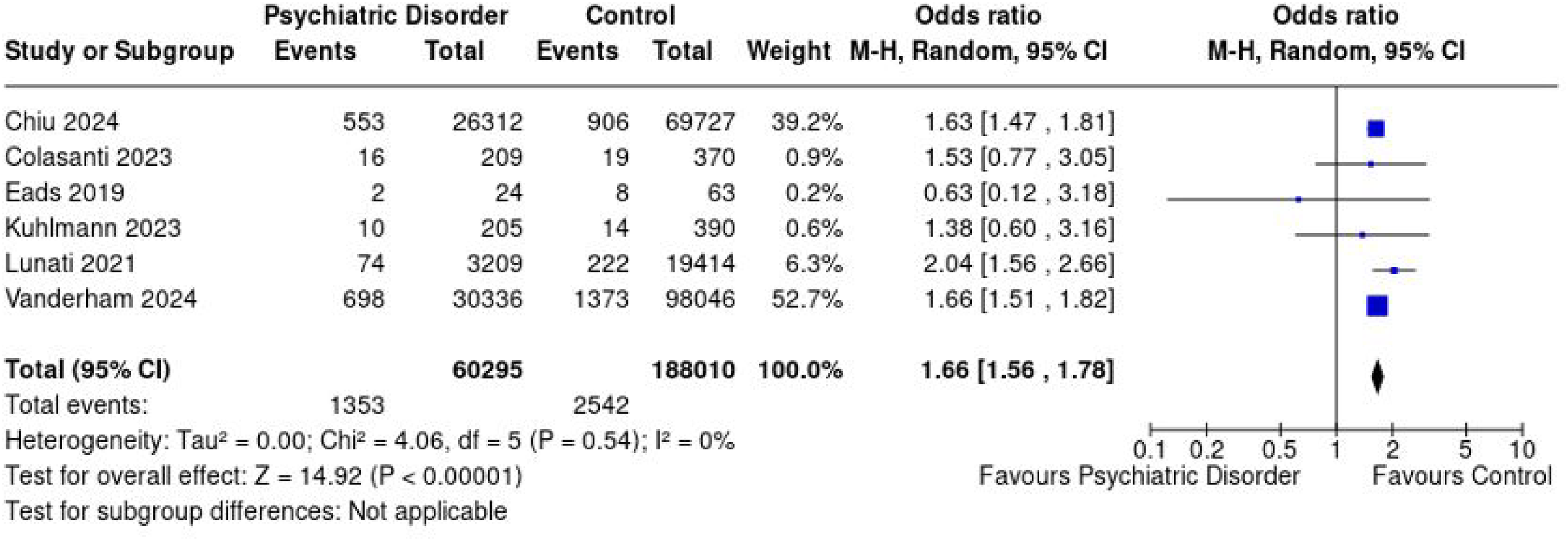
Forest plot demonstrating overall pooled odds ratio for reoperation rate of patients with psychiatric disorders and controls with associated 95% confidence intervals.
Length-of-stay
Four studies comprising 77,503 and 590,619 patients in the PD and control groups, respectively, reported on postoperative LOS.17,18,22,25 Mean follow-up times in the PD and control groups were 15.6 and 16.8 months, respectively. There was no significant difference between the two groups for LOS with an MD of 0.14 (95% CI [−0.06 to 0.33], p = .16, I² = 99%) favoring the PD group (Figure 4).
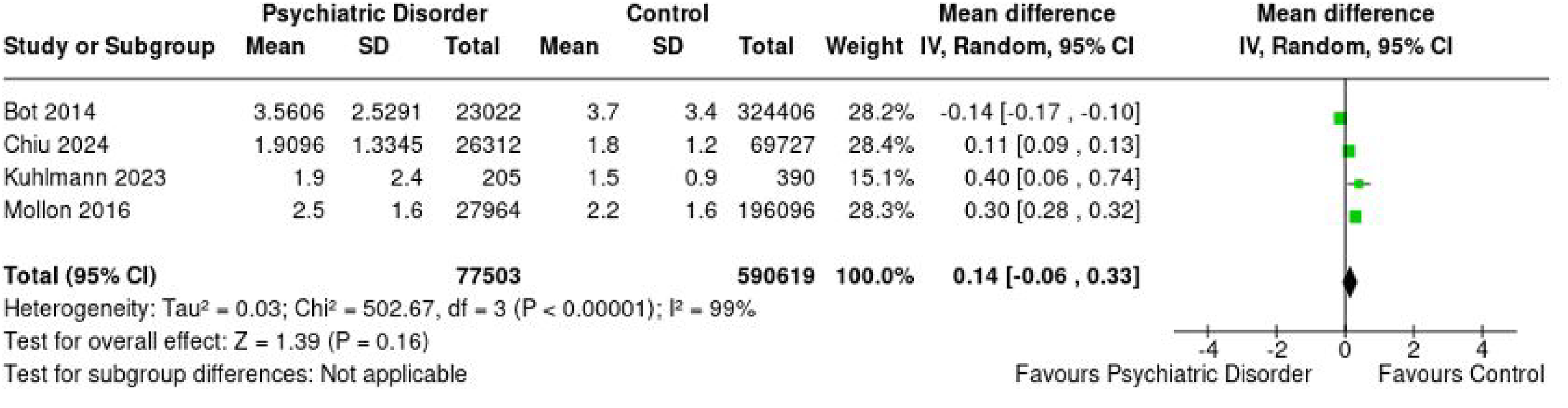
Forest plot demonstrating overall pooled mean difference in length-of-stay between patients with psychiatric disorders and controls with associated 95% confidence intervals.
Patient-reported outcome measures
ASES score
Four studies comprising 398 and 813 patients in the PD and control groups, respectively, reported on postoperative ASES scores.19,21,26,28 Mean follow-up times in the PD and control groups were 49.3 and 56.2 months, respectively. The PD group demonstrated significantly lower postoperative ASES scores than the control group with an MD of −6.73 (95% CI [−10.98 to −2.47], p = .002, I² = 80%) (Figure 5).
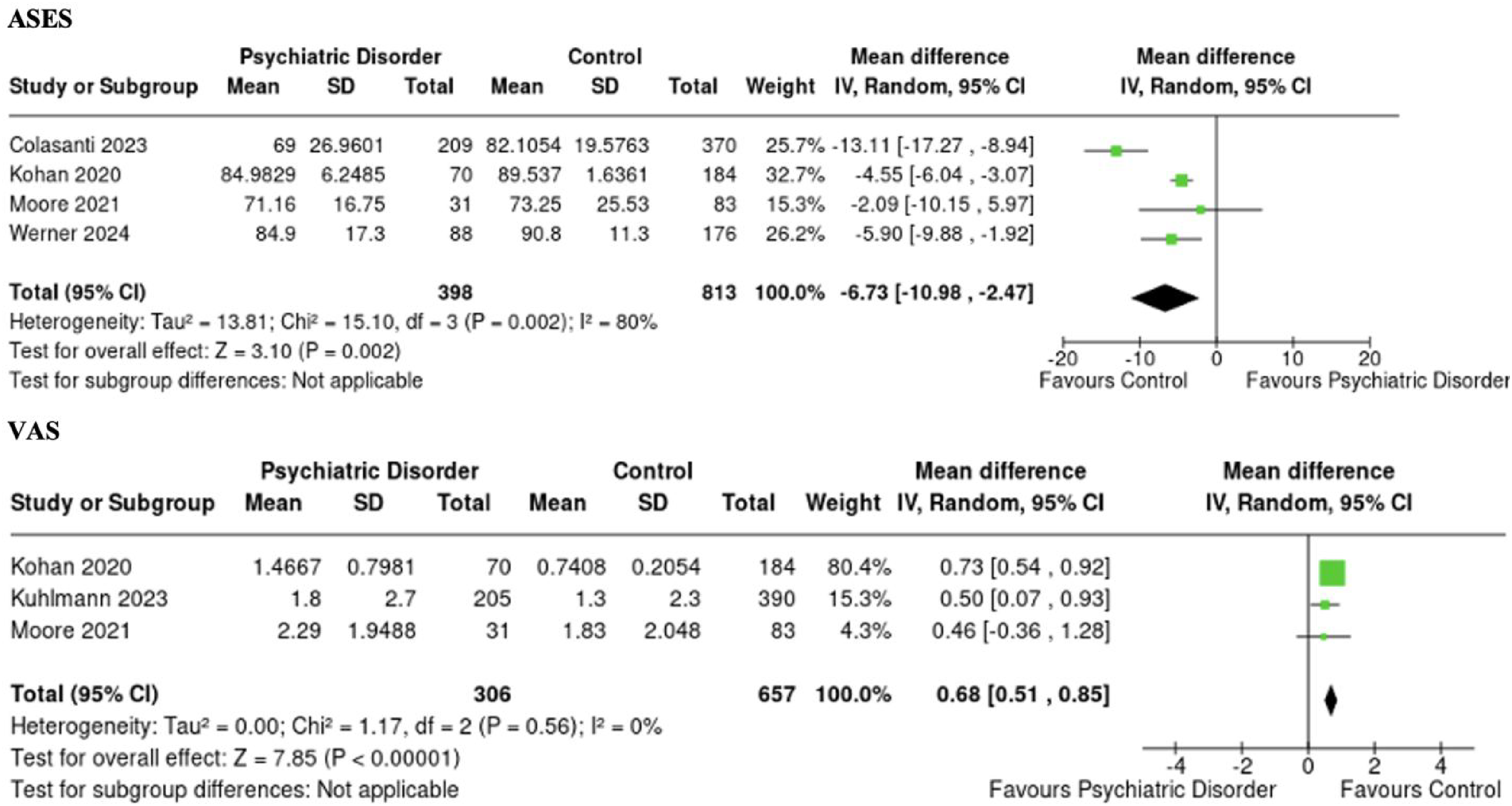
Forest plot demonstrating overall pooled mean difference in postoperative patient-reported outcome measures between patients with psychiatric disorders and controls with associated 95% confidence intervals.
Three studies comprising 310 and 637 patients in the PD and control groups, respectively, reported on pre- to postoperative changes in ASES scores.19,21,26 Mean follow-up times in the PD and control groups were 49.3 and 56.2 months, respectively. All included studies reported statistically significant improvements between preoperative and postoperative ASES scores for both PD and control patients. There was no significant difference between the two groups for mean ASES score change (pre- to postoperative) with an MD of −2.70 (95% CI [−10.66 to 5.27], p = .51, I² = 83%) (Figure 6).
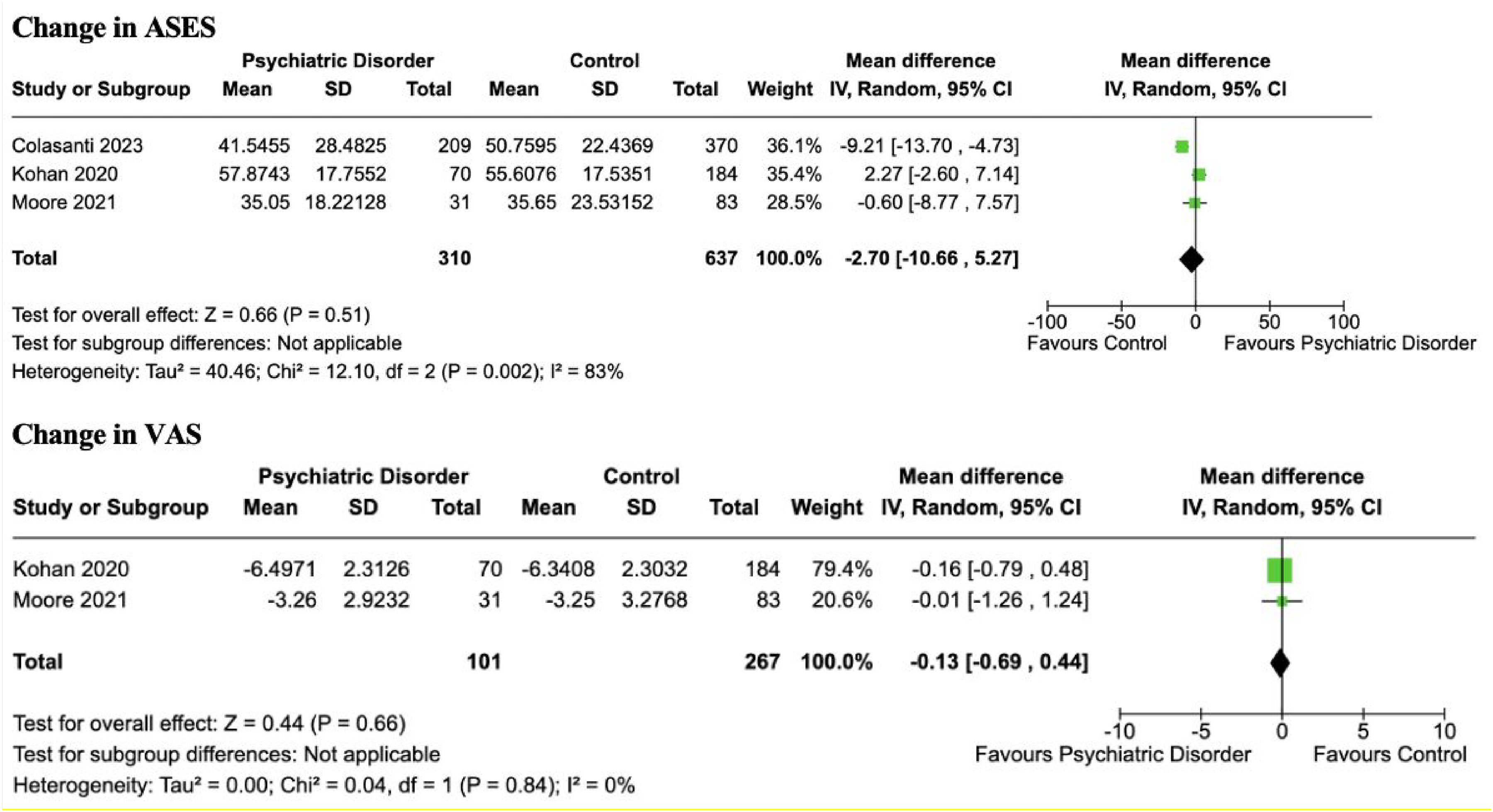
Forest plot demonstrating overall pooled mean difference for mean change in patient-reported outcome measures (preoperative to postoperative) between patients with psychiatric disorders and controls with associated 95% confidence intervals.
Visual analog scale
Three studies comprising 306 and 657 patients in the PD and control groups, respectively, reported on postoperative VAS scores.21,22,26 Follow-up times in the PD and control groups were 17.4 and 18.8 months, respectively. The PD group demonstrated significantly higher postoperative VAS scores than the control group with an MD of 0.68 (95% CI [0.51 to 0.85], p < .00001, I² = 0%) (Figure 5).
Two studies comprising 101 and 267 patients in the PD and control groups, respectively, reported on pre- to postoperative changes in VAS scores.21,26 Mean follow-up times in the PD and control groups were 29.3 and 28.1 months, respectively. All included studies reported statistically significant improvements between preoperative and postoperative VAS scores for both PD and control patients. There was no significant difference between the two groups for mean VAS score change (pre- to postoperative) with an MD of −0.13 (95% CI [−0.69 to 0.44], p = .66, I² = 0%) (Figure 6).
Range of motion
Abduction
Two studies comprising 414 and 760 patients in the PD and control groups, respectively, reported on abduction.19,26 Follow-up times in the PD and control groups were 34.1 and 39.1 months, respectively. The PD group demonstrated significantly inferior postoperative abduction compared to the control group with an MD of −4.03 (95% CI [−7.17 to −0.90], p = .01, I² = 0%) (Figure 7). Additionally, one study reported significant improvements between preoperative and postoperative abduction in the PD and control groups (Table 2).
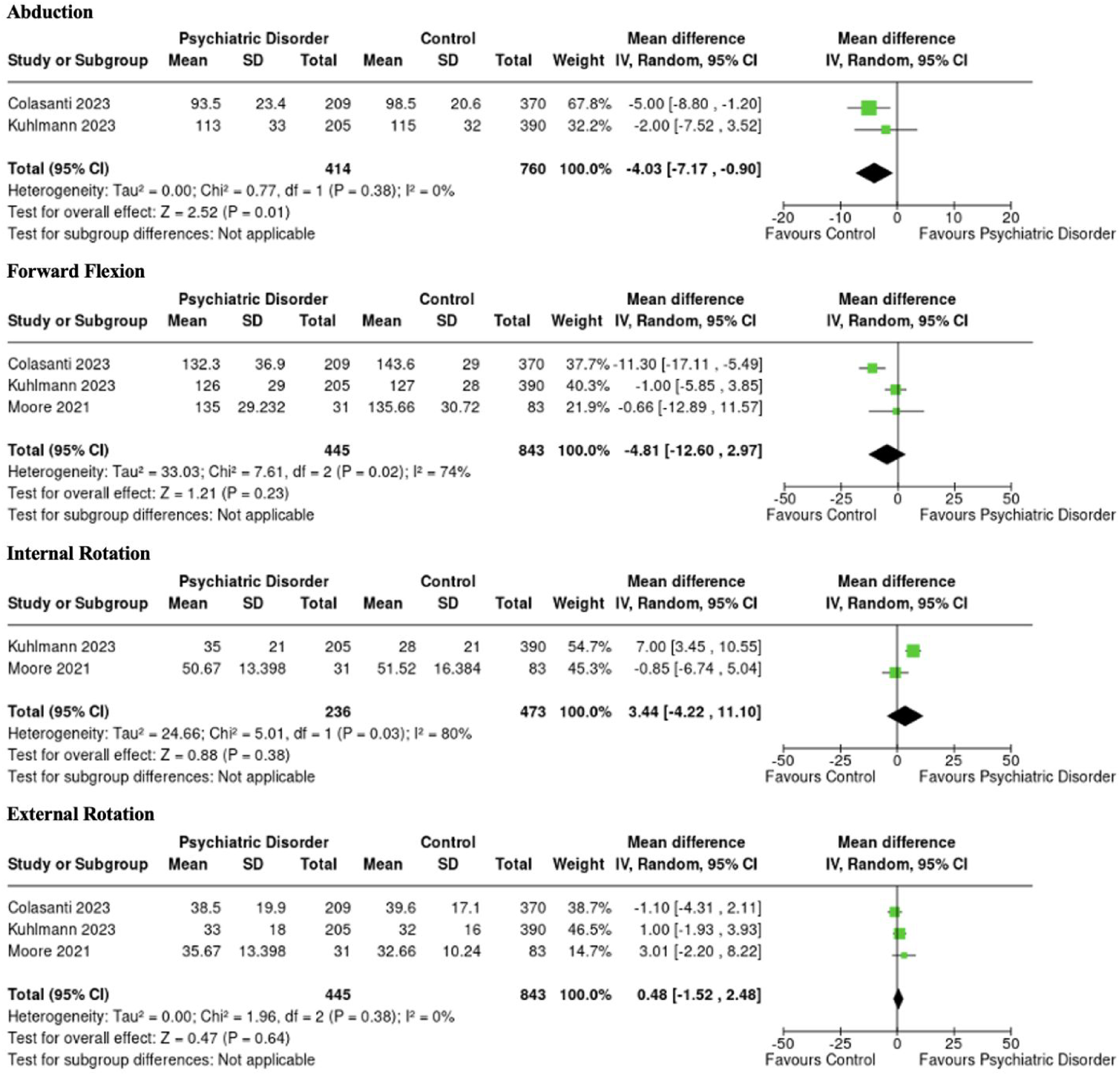
Forest plots demonstrating overall pooled mean difference in postoperative range of motion (degrees) between patients with psychiatric disorders and controls with associated 95% confidence intervals.
Reoperation rate, complication rate, and length-of-stay.
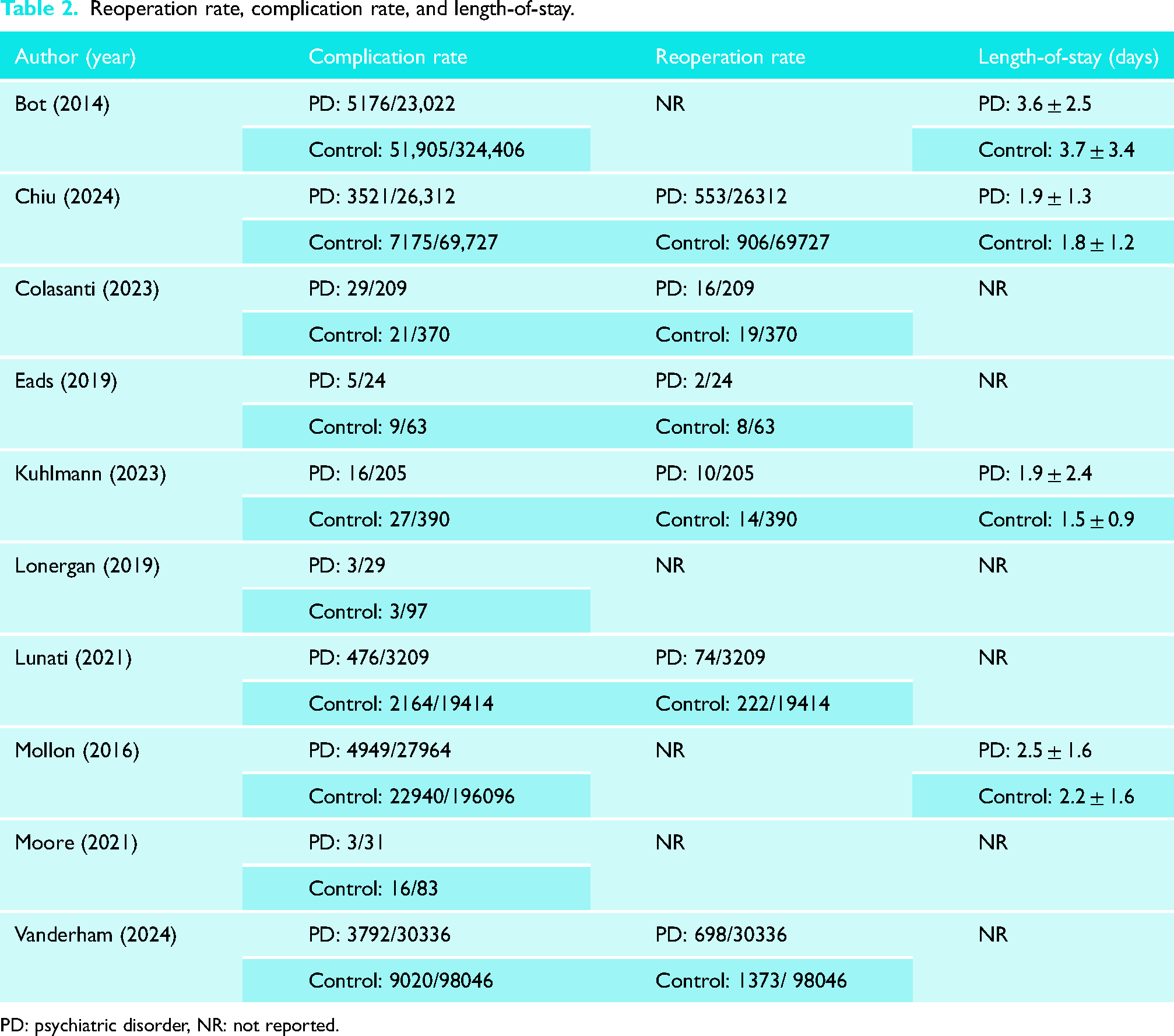
PD: psychiatric disorder, NR: not reported.
Forward flexion
Three studies comprising 445 and 843 patients in the PD and control groups, respectively, reported on forward flexion.19,22,26 Follow-up times in the PD and control groups were 33.8 and 38.0 months, respectively. There was no significant difference in postoperative forward flexion between the two groups with an MD of −4.81 (95% CI [−12.60 to 2.97], p = .23, I² = 74%) favoring the control group (Figure 7). Additionally, both studies reported significant improvements between preoperative and postoperative abduction in the PD and control groups.
One study comprising 31 and 83 patients in the PD and control groups, respectively, reported on pre- to postoperative changes in degrees of forward flexion. 26 Mean follow-up times in the PD and control groups were 29.3 and 28.1 months, respectively. There was no significant difference between the two groups (p = .388).
Internal rotation
Two studies comprising 236 and 473 patients in the PD and control groups, respectively, reported on internal rotation.22,26 Follow-up times in the PD and control groups were 17.4 and 19.2 months, respectively. There was no significant difference in postoperative internal rotation between the two groups with an MD of 3.44 (95% CI [−4.22 to 11.10], p = .38, I² = 80%) favoring the PD group (Figure 7). Additionally, one study reported significant improvements between preoperative and postoperative internal rotation in the PD and control groups, while another study found no differences.
One study comprising 31 and 83 patients in the PD and control groups, respectively, reported on pre- to postoperative changes in degrees of internal rotation. 26 Mean follow-up times in the PD and control groups were 29.3 and 28.1 months, respectively. There was no significant difference between the two groups (p = .315).
External rotation
Three studies comprising 445 and 843 patients in the PD and control groups, respectively, reported on external rotation.19,22,26 Follow-up times in the PD and control groups were 33.8 and 38.0 months, respectively. There was no significant difference between the two groups with an MD of 0.48 (95% CI [−1.52 to 2.49], p = .64, I² = 0%) favoring the PD group (Figure 7). Additionally, no studies reported significant improvements between preoperative and postoperative external rotation in the PD or control groups.
One study comprising 31 and 83 patients in the PD and control groups, respectively, reported on pre- to postoperative changes in degrees of external rotation. 26 Mean follow-up times in the PD and control groups were 29.3 and 28.1 months, respectively. There was no significant difference between the two groups (p = .664).
Discussion
The primary finding of this review was that preexisting PDs resulted in a higher incidence of complications and reoperation following TSA compared to controls. Additionally, patients with preexisting PDs demonstrated statistically inferior postoperative ASES and VAS scores, although no statistical difference was observed for changes in ASES and VAS scores (preoperative to postoperative). PD patients were also found to have significantly reduced postoperative abduction. There were no significant differences in postoperative LOS, forward flexion, internal rotation, or external rotation between the two groups.
It is well-established that complications and revision surgeries following TSA worsen patient function, satisfaction, and even mortality.30,31 Hence, optimizing patient factors to mitigate these outcomes is critical as a means to alleviate patient burden. 32 This review found that patients in the PD group had a significantly higher incidence of postoperative complications and reoperations. These findings align with existing literature, which have similarly reported increased risks for postoperative complications in PD patients undergoing other orthopedic procedures, such as arthroscopic rotator cuff repair. 33 Patients with PD may experience heightened levels of perioperative anxiety and stress, which can lead to increased cortisol production, immune dysregulation, and impaired wound healing, thus increasing susceptibility to postoperative complications such as prosthetic joint infections.34,35 Furthermore, elevated cortisol levels have been linked to impaired cognitive function and decision-making, especially in older adults. 36 Given the aging population and increasing rate of TSA operations in the elderly, this risk of cognitive impairment becomes especially problematic. 37 Depression and anxiety are also associated with systemic inflammation, marked by elevated levels of proinflammatory cytokines such as interleukin-6, tumor necrosis factor-alpha, and C-reactive protein. 38 Excessive inflammation has been shown to negatively impact bone healing processes, leading to complications such as prosthetic joint infections, delayed union or nonunion of bones, and prolonged recovery times.39,40 The presence of PD can also exacerbate comorbid conditions, which are known to adversely affect orthopedic surgical outcomes. 41 For instance, patients with diabetes are at an increased risk of infection and delayed wound healing, which are further compounded by the inflammatory state and worsened glycemic control associated with depression. 42 Lastly, a history of PDs is a known risk factor for opioid misuse and addiction, particularly in the postoperative period.43,44 The adverse effects of prescription opioids are well-established, and include physical dependence, immunosuppression, opioid-induced endocrinopathies such as sexual dysfunction and fatigue, and even paradoxical increases in nociceptive sensitization (opioid-induced hyperalgesia).45,46 As such, multimodal analgesia that minimizes opioid use should be emphasized, particularly for PD patients who are especially susceptible to its deleterious effects.
This review found that postoperative PROMs, namely the ASES and VAS score, were significantly poorer in patients with preexisting PD. These findings potentially suggest that PD worsen the subjective experience of recovery. Several possible mechanisms may explain this potentially causative relationship. It is already well-documented that depression and anxiety are associated with a heightened perception of pain and lower pain thresholds, which could manifest as differences in postoperative VAS and ASES scores. 47 This is further complicated by recent literature which highlights how the severity of psychiatric illnesses similarly increases in response to worsening pain, thus generating a vicious cycle of symptom intensification. 48 Patients with depression and anxiety are also more likely to experience catastrophizing, a maladaptive cognitive-emotional response characterized by an exaggerated negative orientation towards pain stimuli. 49 This may similarly lead to poorer pain management and higher subjective pain and function scores. Lastly, recent studies have highlighted the relationship between pain intensity and kinesiophobia, or the fear of reinjury, which itself has been shown to positively correlate with PDs.48,50 In addition to its direct aggravation of pain perception, kinesiophobia also reduces engagement with rehabilitation, thereby delaying the restoration of strength and range of motion as well. 51 However, it is important to note that no significant differences were observed for pre- to postoperative changes in ASES and VAS scores between PD and control patients. Although fewer studies reported data, these findings argue against the conclusion that preexisting PDs worsen PROMs following TSA. Thus, future studies must elucidate whether PDs truly influence post-TSA PROMs, thereby clarifying the necessity of interventions.
One of the most important steps in managing TSA patients with PD should be the early identification and optimization of these conditions before surgery. Preoperative psychiatric screening should be integrated as a routine part of the surgical assessment. Tools such as the Patient Health Questionnaire-9 for depression and the Generalized Anxiety Disorder 7-item scale for anxiety can be employed to systematically evaluate patients’ psychological status, if not already diagnosed.52,53 Identifying at-risk patients enables the implementation of early interventions, such as referring patients to psychiatric professionals for counseling, cognitive-behavioral therapy (CBT), or pharmacologic treatment to stabilize their psychiatric conditions before surgery. Emerging evidence suggests that preoperative psychological interventions, including CBT, can effectively reduce anxiety and depression symptoms, thereby improving postoperative outcomes. In fact, a study by Monticone et al. found that CBT, combined with physical therapy, significantly improved postoperative pain and functional recovery in orthopedic patients with PD. 54 Such approaches should be more widely considered for this high-risk population, with the goal of enhancing psychological resilience, reducing PD-associated pain catastrophizing and kinesiophobia, and promoting better adherence to rehabilitation programs. Additionally, robust preoperative screening tools and guidelines will enable surgeons to better guide patient expectations and practice patient-centered care. This is crucial as it is well-known that patient-centered care is associated with improved postoperative outcomes and decreased healthcare costs. 55
Limitations of this study mainly arose from the limited amount of evidence, with only 13 studies being included, all of which constituted Level III evidence. As most studies were not prospective, the risk of selection bias is high. Another limitation was the significant heterogeneity (>75%) among the included studies for complications rate, LOS, ASES, forward flexion, and internal rotation. Although a random-effects model was used to address some of this variability, the external validity of the findings remains uncertain. Factors such as differences in surgical techniques (aTSA vs rTSA), types of PDs (e.g., depression vs anxiety), and demographic characteristics were not standardized across the included studies, likely worsening the observed heterogeneity. Unfortunately, no subgroup analyses were undertaken to explore these factors as the included studies did not stratify data accordingly. Furthermore, different surgeons may have unique thresholds for reoperation, which acts as a confounding variable. In particular, they may weigh the impact of psychiatric comorbidities to different degrees when considering the likelihood of successful reoperation. Lastly, the presence of multiple registry-based studies introduces the potential for patient overlap and the overrepresentation of certain populations and associations. Hence, this review advocates for the consideration of further well-designed, long-term prospective cohort studies comparing post-TSA outcomes between patients with and without preexisting PD diagnoses. These studies should focus on specific PDs and TSA techniques while also controlling for between-group differences in demographic factors.
Conclusion
Patients with preexisting PDs may have one-and-a-half times higher odds of postoperative complication or reoperation, as well as significantly worse postoperative pain and PROMs. Identification of at-risk individuals with preexisting psychiatric conditions and preoperative referral to a mental health specialist to optimize psychiatric conditions may benefit this patient cohort ahead of their shoulder arthroplasty procedure. Nonetheless, further high-quality prospective studies are warranted given the current lack of data on the topic.
Supplemental Material
sj-docx-1-sel-10.1177_17585732251314130 - Supplemental material for The impact of preexisting psychiatric disorders on patient outcomes following primary total shoulder arthroplasty: A systematic review and quantitative synthesis
Supplemental material, sj-docx-1-sel-10.1177_17585732251314130 for The impact of preexisting psychiatric disorders on patient outcomes following primary total shoulder arthroplasty: A systematic review and quantitative synthesis by Bryan Sun, Vetri Thangavelu, Rose Yakubov, Clare Sun, Moin Khan, Sumit Chaudhari and Ujash Sheth in Shoulder & Elbow
Supplemental Material
sj-docx-2-sel-10.1177_17585732251314130 - Supplemental material for The impact of preexisting psychiatric disorders on patient outcomes following primary total shoulder arthroplasty: A systematic review and quantitative synthesis
Supplemental material, sj-docx-2-sel-10.1177_17585732251314130 for The impact of preexisting psychiatric disorders on patient outcomes following primary total shoulder arthroplasty: A systematic review and quantitative synthesis by Bryan Sun, Vetri Thangavelu, Rose Yakubov, Clare Sun, Moin Khan, Sumit Chaudhari and Ujash Sheth in Shoulder & Elbow
Supplemental Material
sj-docx-3-sel-10.1177_17585732251314130 - Supplemental material for The impact of preexisting psychiatric disorders on patient outcomes following primary total shoulder arthroplasty: A systematic review and quantitative synthesis
Supplemental material, sj-docx-3-sel-10.1177_17585732251314130 for The impact of preexisting psychiatric disorders on patient outcomes following primary total shoulder arthroplasty: A systematic review and quantitative synthesis by Bryan Sun, Vetri Thangavelu, Rose Yakubov, Clare Sun, Moin Khan, Sumit Chaudhari and Ujash Sheth in Shoulder & Elbow
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Contributorship
BS contributed to study design, data acquisition, data analysis, data interpretation, manuscript drafting, and manuscript revision. VT, RY, and CS all contributed to data acquisition and manuscript drafting. US conceived of the study, contributed to study design, and critically revised the manuscript. MK and SC critically revised the manuscript. All authors read and gave approval of the final manuscript to be published, and agree to be held accountable for all aspects of the work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.