
Abstract
Introduction:
Samoa faces a high burden of noncommunicable diseases (NCDs). Understanding health literacy can support more effective interventions. This pilot study aimed to culturally adapt the European Health Literacy Survey Questionnaire (HLS-EU-Q16) to the Samoan context (HLS-Samoa-Q24) and conduct a preliminary assessment of its psychometric properties and user feasibility.
Methods:
A non-probability purposive cluster sampling approach was used to recruit 73 adult respondents. The HLS-EU-Q16 was adapted by adding eight culturally relevant items, resulting in the 24-item HLS-Samoa-Q24. Items were scored on a 4-point Likert scale. Participants completed the instrument and provided feedback through six group interviews.
Results:
The health literacy level was defined as inadequate for 63 (84%), problematic for seven (12%) and adequate for three individuals (4%). The mean score was 3.90 (SD = 3.87; 95% CI 3.00–4.81), indicating inadequate health literacy. Internal consistency was high (Cronbach’s alpha = 0.92; Omega = 0.91). Due to the small, gender-imbalanced sample, confirmatory factor analysis was not feasible, and construct validity remains to be tested. User feasibility of HLS-Samoa-Q24 detailed comprehensibility, relevance of the added items, and an average completion time of 25 minutes.
Conclusion:
The HLS-Samoa-Q24 shows promise as a culturally adapted instrument for assessing health literacy in Samoa. However, the findings are preliminary and not generalizable. Further validation with a larger, representative sample is needed to confirm its psychometric robustness.
Introduction
Samoa, a small island developing state in the Pacific, is struggling with a high burden of noncommunicable diseases (NCDs). Recognizing that health literacy is an important asset to challenge the increasing burden of NCDs, this pilot study explores the adaptation of a validated health literacy measurement tool to the Samoan context (1). NCDs are the main causes of premature mortality and morbidity in Samoa, accounting for 82% of all deaths (2). National surveillance through the WHO STEPwise approach confirms high levels of NCD risk, including obesity rates of around 85% among adults (3,4). Beyond their health impact, NCDs impose considerable social and economic costs, contributing to a decline in national GDP since 2019 and placing pressure on families and the health system (5). The escalating costs associated with treating end-stage NCDs impose a major financial burden on the health system and broader society. Although Samoa has enacted several policy and community-based strategies – such as tobacco and food policy reforms and the PEN Fa’a Samoa programme – persistent challenges remain, particularly in relation to health literacy, case management, and access to medicines (6 –8).
Health literacy is recognized as a key determinant of NCD outcomes. Low health literacy is associated with poorer disease management, reduced use of preventive services, and higher hospitalization rates (9 –12). The European Health Literacy Survey Questionnaire (HLS-EU-Q) provides a validated framework to assess how people access, understand, appraise, and use health information across domains of healthcare, disease prevention, and health promotion (13 –16). The short version, HLS-EU-Q16, is widely used, easy to administer, and has been adapted across multiple cultural contexts (17 –19). Because health literacy is shaped by social and cultural factors, adapting the instrument to Samoa’s context – characterized by communal decision-making, extended family structures, and the frequent use of traditional healers – is essential for meaningful measurement. The addition of culture and/or disease-specific items in health literacy instruments is described in the literature of Gustafsdottir and colleagues (20). Evidence from Samoa highlights the influence of family dynamics, cultural beliefs, and traditional healing practices (‘fofo’) on health-seeking behaviour (21,22). Data on health literacy in Samoa are not available and the country has been struggling to address the NCD epidemic at a health systems, community, and individual level (8). However, no validated health literacy instrument currently exists for Samoa, and only one study has been conducted in American Samoa using a different tool (23). Relevant work among Māori and Pacific populations in New Zealand further supports the need for culturally grounded tools to assess health literacy in Polynesian communities (24,25). Traditional healing practices, such as the use of herbal remedies and spiritual rituals, may coexist alongside modern healthcare practices. Cultural beliefs about illness causation, treatment, and healing play a significant role in shaping health-seeking behaviours and decision-making (22). This pilot study therefore aimed to (i) culturally adapt the HLS-EU-Q16 for Samoa, resulting in the HLS-Samoa-Q24, and (ii) conduct a preliminary assessment of its internal consistency and user feasibility. By integrating culturally relevant elements and gathering user feedback, this feasibility study provides an initial step towards developing an appropriate instrument for measuring health literacy in Samoa.
Methods
Health literacy measurement
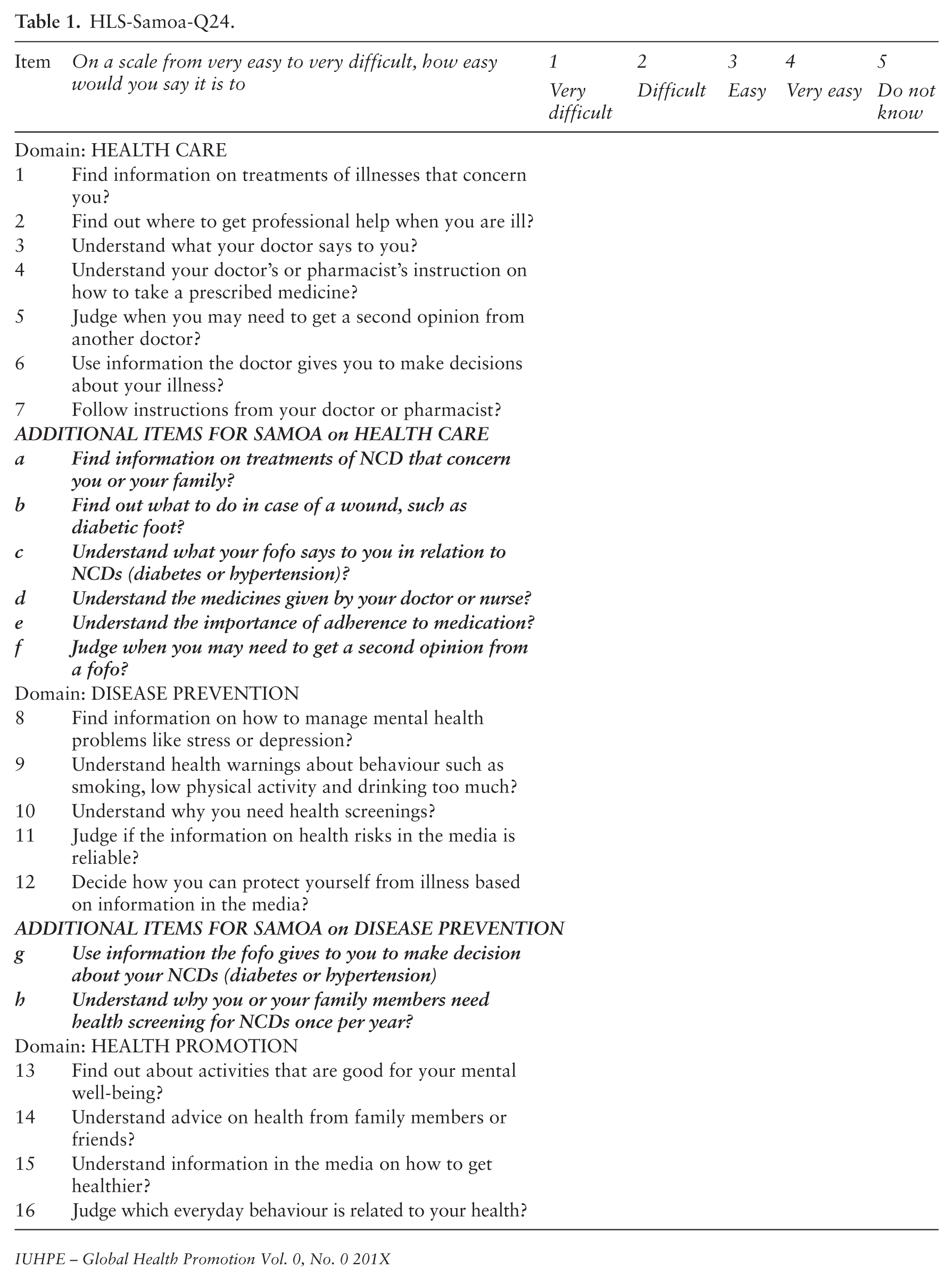
Health literacy was measured using the validated HLS-EU-Q16, which assesses three domains: health care, disease prevention, and health promotion. The HLS-EU-Q16 is scored using a five-point Likert scale, with categories ‘very difficult’, ‘difficult’, ‘easy’ and ‘very easy’ and ‘do not know’. ‘Do not know’ and ‘missing responses’ were treated as 0. Following established scoring recommendations (13), responses were dichotomized as follows: ‘Very difficult’/‘difficult’ = 0; ‘easy’/‘Very easy’ = 1. The total sum score of the HLS-EU-Q16, thus ranges from 0 (low health literacy) to 16 (high health literacy). The adapted HLS-Samoa-Q24 contains the original 16 items plus eight Samoan-specific items. The same dichotomization procedure was applied. Total scores ranged from 0 to 24, categorized using proportionally aligned thresholds: Inadequate (0–12), Problematic (13 –18), Sufficient (19 –24). This ensured comparability between the original and adapted instruments.
Adaptation of HLS-EU-Q16 to Samoan context
The adaptation followed three structured phases to ensure conceptual, linguistic, and cultural relevance. Authorization of the developers of the HLS-EU-Q16 to adapt the scale to Samoan culture was received through the principal researcher of HLS-EU-Q16. The model drew upon the existing conceptual framework proposed by Sørensen et al. (17). While the original HLS-EU-Q consists of 47 items, the shortened version the HLS-EU-Q16, which includes 16 items selected from the original questionnaire to capture key aspects of health literacy, was found easier for use and fit for purpose in Samoa.
Phase 1: Cultural and NCD-related content adaptation: A desk review of Samoan health system and cultural practices (21), combined with national NCD data (4), identified culturally specific factors that influence health literacy – such as communal decision-making, the role of extended families, and traditional healing practices. Eight additional items were drafted by the research team and Ministry of Health experts to capture these contextual dimensions. These items were reviewed and refined with the principal researcher of the original HLS-EU-Q16 to ensure conceptual consistency.
Phase 2: Translation and back-translation: Two bilingual Samoan public health experts independently conducted the forward translation (English -> Samoan) and back translation (Samoan -> English). Both translators and the research leads then jointly reviewed each item to resolve discrepancies. Special attention was given to the translation of ‘noncommunicable diseases’, where two Samoan terms – fa‘ama‘i le pipisi and ma‘i tumau – were evaluated for cultural accuracy. Consensus favoured fa‘ama‘i le pipisi for its closer conceptual match.
Phase 3: Cognitive interviews and expert review: Cognitive interviews were conducted with four registered nurses, two Ministry of Health staff, two national health service administrators, seven women’s committee representatives, and seven village chiefs. Interviews assessed item clarity, cultural appropriateness, and comprehensiveness. Based on feedback, items were refined, and a pre-test was conducted with Ministry of Health staff. The pre-test indicated that respondents preferred oral facilitation, leading to the decision to use a Samoan facilitator (‘orator’) to introduce and explain the questionnaire in a culturally appropriate manner during data collection.
Table 1 presents all items, with the eight added Samoan-specific items shown in bold italics.
HLS-Samoa-Q24.
Respondents
A non-probability purposive cluster sampling strategy was used.
Clusters were selected across four regions (Apia Urban Area, Northwest Upolu, Rest of Upolu, and Savai‘i) (26). Seven villages agreed to participate. Village committees invited adult residents aged ⩾18 years. A total of 73 respondents were recruited. Followed by the research guidance from the Ministry of Health Samoa (27), the researchers asked for formal consent from the village committees for the recruitment of respondents and these committees subsequently invited the inhabitants of the selected villages above 18 years of age.
Procedure and methodology of group interview analysis
Prior to participation, all respondents were provided with detailed information about the study’s purpose, procedures, and their rights as participants. Informed consent was obtained in writing from each participant. After completing the HLS-Samoa-Q24, respondents participated in group interviews designed to assess comprehension, cultural relevance, and feasibility of the adapted instrument. Six group interviews were conducted between August and November 2015, each consisting of 11–14 participants (total n = 73). Group interviews were held in private community spaces to ensure confidentiality and cultural comfort. The Ministry of Health provided ethical approval through the Health and Research Committee (27). The consent form was read aloud in Samoan by the facilitator and consent was documented in the presence of the facilitator and main researcher of this paper. To ensure confidentiality, all data were anonymized at the point of collection. Participants were assigned unique codes. Group interviews were conducted in private community settings to ensure participants’ privacy. All data were stored securely and accessed only by the research team. The interviews were conducted in Samoan by a trained facilitator. The principal researcher observed the completion of the HLS-Samoa-Q24 and the group interviews in all groups. Respondents first completed the HLS-Samoa-Q24. Post completion, the facilitator guided the discussion to gather respondents’ opinions and observations about instrument. Opinions were gathered on comprehension of the items and reflections on the Samoan-specific items, as well as general remarks on coding instructions and ease of participation. A micro-interlocutor analysis approach (28) was used to document how respondents interpreted items. This included observing verbal explanations, response choices, collective interactions, and non-verbal cues (e.g. hesitation, requests for clarification, body language). Observation notes were compiled immediately following each session to minimize recall bias.
Data analysis
To assess reliability of HLS-Samoa-Q24 measures of Omega (ω) and Cronbach’s Alpha (α) were computed as indicators of scale reliability and internal consistency (29). To analyse Omega (ω), the open-source package R was used and SPSS for Cronbach’s Alpha (α). Population-based characteristics like age, gender, household size, and education and income level were obtained. Instrument feasibility of HLS-Samoa-Q24 was reviewed by analysis and detailed observation notes taken during the interview looking at verbal and non-verbal actions (30). The additional eight items were developed based on expert consultation and require further testing as will be explained below.
Results
Respondent characteristics
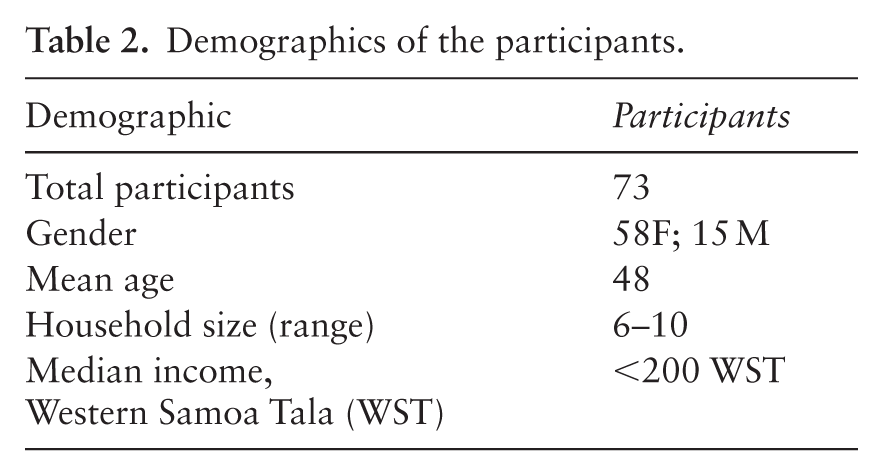
Demographic characteristics detail that most respondents have 6–10 members per household, which is comparable to a ‘normal’ household size in Samoa (26), as shown in Table 2. The mean age was 48 years (18–68 years), and females were overrepresented (58 females/15 males). With regards to education, 20% (15/73) had no education or reported to have gone only through primary education. A majority, 78% (57/73), completed secondary school education. The primary school completion rate is 97% and the net enrolment for secondary education in Samoa is 73%, as per the latest data reported in survey findings from the Demographic Health Survey 2019–2020 (26). The Demographic Health Survey details that the upper secondary completion rate (grade 13) is 56% for total population (26). From our study sample, 78% (57/73) completed secondary school education.
Demographics of the participants.
Internal consistency of HLS-Samoa-Q24 and HLS-EU-Q16
The Cronbach alpha coefficients were 0.92 for HLS-Samoa-Q24 and 0.89 for HLS-EU-Q16. The reliability score of the HLS-Samoa-Q24 expressed in Omega is 0.91 [0.88, 0.94], which indicates a good internal reliability (29).
To explore the consistency between the original and adapted scale, the Spearman–Brown coefficient was calculated, given the addition of eight new items in the HLS-Samoa-Q24. The coefficient for the HLS-Samoa-Q24 was 0.81, compared with 0.73 for the HLS-EU-Q16. These results suggest a comparable level of reliability between the two scales. The estimated reliability coefficients for both instruments are presented in Table 3.
Estimated reliability coefficients for HLS-EU-Q16 and HLS-EU-Q24.
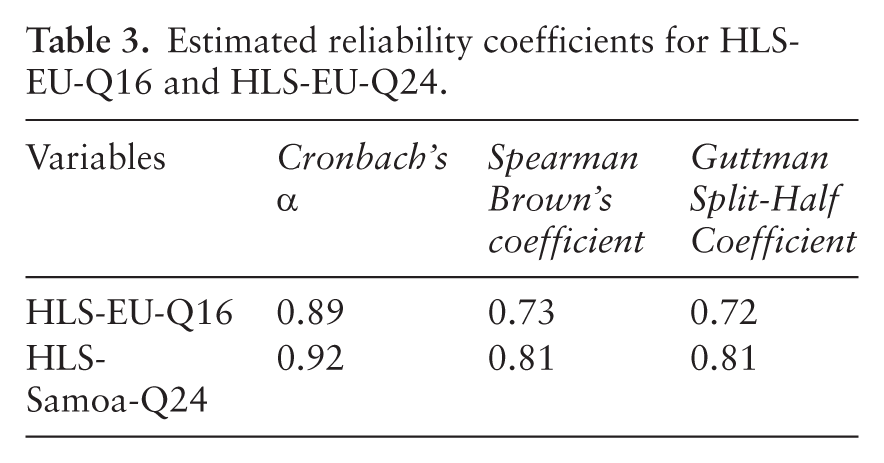
As shown, the reliability of the questionnaire increases as its length increases, as indicated by higher Spearman–Brown coefficients.
The Guttman split-half coefficient for the HLS-EU-Q16 was calculated to be 0.72. This coefficient reflects the extent to which the items in the questionnaire are parallel measures of the underlying construct. A higher coefficient indicates greater internal consistency reliability. Further analysis was conducted to examine the split-half reliability of the HLS-Samoa-Q24. The split-half correlation was found to be 0.81.
These results suggest that the HLS-Samoa-Q24 demonstrates strong internal consistency reliability in its current form. The high Guttman split-half coefficient indicates that the items in the questionnaire are parallel measures of the underlying construct, supporting the reliability of the instrument.
The item total correlation coefficient for the HLS-EU-Q16 and the HLS-Samoa-Q24 was calculated at the sub-dimension level displayed in Table 4.
Cronbach’s α for the HLS-EU-Q16 and the HLS-Samoa-Q24.
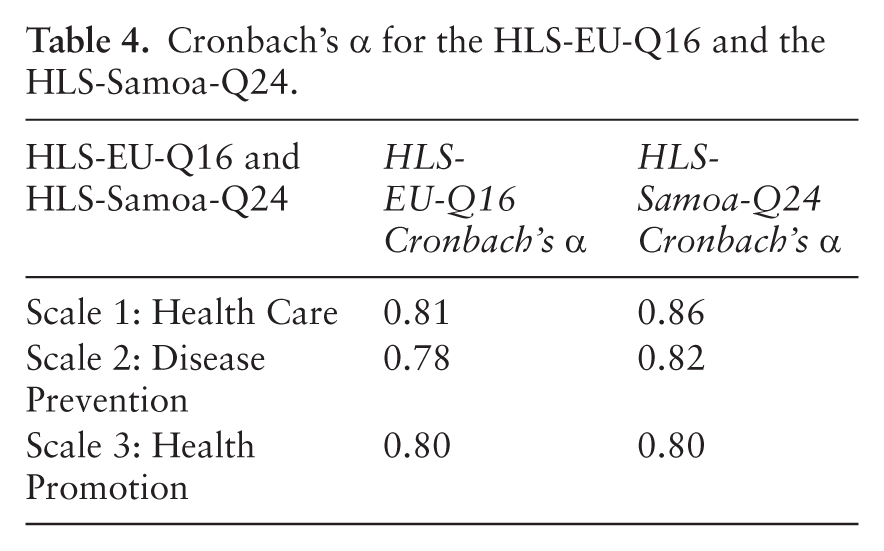
Table 4 presents the Cronbach’s alpha coefficients for the three scales – Health Care, Disease Prevention, and Health Promotion – of both the HLS-EU-Q16 and HLS-Samoa-Q24 instruments. These values demonstrate strong internal consistency across all scales, with alpha coefficients ranging from 0.78 to 0.86.
Health literacy scores
The health literacy level measured by HLS-EU-Q16 was defined as inadequate for 63 (84%), problematic for seven (12%), and adequate for three participants (4%) (Figure 1). The mean health literacy score value obtained in the sample using HLS-EU-Q16 was 3.90 (SD = 3.87; 95% CI 3.00–4.81), corresponding to an inadequate health literacy level. The health literacy level measured by HLS-Samoa-Q24 was defined as inadequate for 51 (70%), problematic for 18 (25%), and adequate for four (5%). The mean health literacy score value obtained in the sample using HLS-Samoa-Q24 was 9.48 (SD = 5.62), corresponding to an inadequate health literacy level as well.
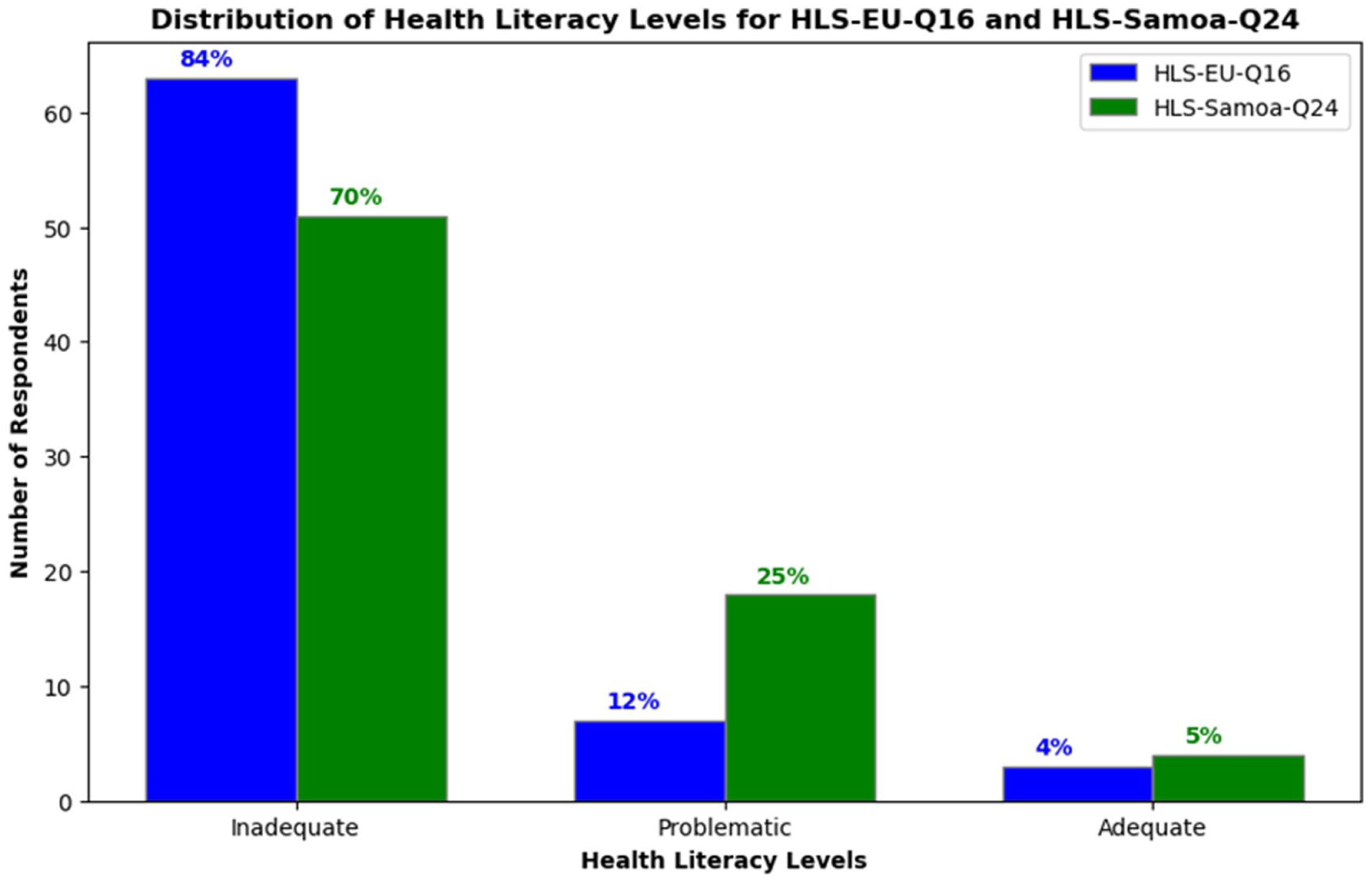
Distribution of health literacy levels among respondents using HLS-EU-Q16 and HLS-Samoa-Q24 instruments. Percentages indicate the proportion of respondents in each category (Inadequate, Problematic, Adequate).
User feasibility of HLS-Samoa-Q24
Comprehension, feasibility, and total time for completion of the HLS-Samoa-Q24 was assessed. The micro-interlocutor analysis detailed interaction data from the respondents. Observation and remarks of respondents showed issues with respect to completion of the HLS-Samoa-Q24. Comments were made about the difficulty of scoring (Likert scale). The HLS-Samoa-Q24 was completed by crossing the relevant cell per item while the respondents were sitting on a chair. It was observed that, in the Samoan context, people are used to sitting cross-legged. Several respondents moved to sit on the ground, cross-legged, making completion challenging (no hard surface to support the paper). Moreover, it was noted that some respondents requested assistance from the facilitator to read out the items. The facilitator provided additional explanatory information when requested and this increased confidence in completing the HLS-Samoa-Q24. Average time to complete the questionnaire was 25 minutes.
Discussion
This pilot study culturally adapted the HLS-EU-Q16 to the Samoan context, resulting in the HLS-Samoa-Q24, and examined its preliminary feasibility and internal consistency. Both the original and adapted instruments demonstrated high reliability, as indicated by strong Cronbach’s alpha and omega coefficients. While these findings suggest coherent item performance, they do not establish construct validity (Table 3).
However, because of the small sample size, confirmatory factor analysis (CFA) could not be conducted, and construct validity remains unconfirmed because of the small sample size, which did not permit confirmatory factor analysis (CFA) to be performed. The strong correlation between the HLS-EU-Q16 and HLS-Samoa-Q24 was expected, given the overlap of 16 items, and does not independently validate the adapted instrument. Although principal component analysis (PCA) was performed, the results were not reported because of the limited sample size. Nonetheless, preliminary indicators such as the Kaiser–Meyer–Olkin (KMO) measure of 0.816 and a significant Bartlett’s Test of Sphericity (p < 0.001) suggest a strong relationship among items. These findings support the potential for future structural validation, pending a larger study. Future studies with larger, more diverse samples are needed to confirm the factor structure and validate the tool. A key novel contribution of this pilot study lies in the development and integration of eight Samoan-specific items into the HLS-Samoa-Q24. These items were designed to reflect cultural and contextual realities, including the role of traditional healers (‘fofo’), communal decision-making, and the influence of extended family in health-related matters. This culturally grounded approach enhances the instrument’s relevance and potential utility in guiding public health interventions in Samoa. The adaptation process also revealed linguistic nuances, such as the translation of ‘noncommunicable diseases’ into Samoan, which required careful consensus to ensure conceptual clarity.
As stated in concluding remarks by Nutbeam and colleague (31): ‘future health literacy intervention research should focus on reaching and engaging the population groups who are disproportionately affected by low health literacy’.
Feasibility findings underscore the practical considerations required for health literacy assessment in Samoa. Respondents often preferred sitting on the ground in a circle, a traditional arrangement that influenced how the questionnaire could be completed. The average completion time (25 minutes) was notably longer than that reported in European settings (approximately 3 minutes), reflecting both unfamiliarity with written survey tools and the seriousness with which participants approached the task. Some respondents required assistance with reading or interpreting items, reinforcing the value of oral facilitation and the potential usefulness of alternative response formats such as visual symbols.
Health literacy assessment instruments may in fact lack practical utility, and the length of the administration of the questionnaires is not user friendly in a low-income setting (32). Availability of the HLS-Samoa-Q24 could stimulate research into health literacy in populations of other Polynesian countries. In 2022, Tofaeono and colleagues (23) completed a study in American Samoa to develop and validate a health literacy instrument. A better understanding of level and background of health literacy could enhance appropriate public health measures to address priority conditions.
The study also indicates that many participants exhibited inadequate health literacy, although the small, non-representative sample precludes population-level inference. Similar patterns have been observed in other low-resource settings, including studies adapting the HLS-EU-Q16 for India (33).
Several limitations must be acknowledged. The sample size was small and predominantly female (80%), likely reflecting gendered roles in health-related community engagement as well as the practical realities of men’s involvement in agricultural labour. Additionally, women may feel a stronger sense of responsibility for health‑engagement discussions, reflecting their traditional roles in preventive health and sanitation, such as through women’s village committees (21). Although participants were drawn from all seven districts and shared demographic similarities with the broader population, the sample cannot be considered representative. Comparison of the sample with a representative national sample suggests similar characteristics like rural setting, education, income per household, household size, and age (26). Test–retest reliability was not assessed, and structural validity remains untested. As such, the HLS-Samoa-Q24 should be viewed as an early-stage adaptation requiring further refinement.
Despite these limitations, this study establishes an important foundation for future health literacy research in Samoa and potentially other Polynesian contexts. Insights from this feasibility phase suggest that subsequent iterations of the instrument may benefit from focusing more narrowly on specific priority conditions, such as hypertension and diabetes, which were frequently referenced by participants and align with the national NCD burden (34).
Conclusion
Considering the small and gender-imbalanced sample, this initial study found that the health literacy measurement instrument that was culturally adapted for Samoa (HLS-Samoa-Q24) seems fit to describe health literacy. HLS-Samoa-Q24 was furthermore shown to have high internal consistency. However, due to the limited and non-representative nature of the sample, the findings should be interpreted with caution and cannot be generalized to the wider Samoan population. Adjustments to the procedures are recommended to ensure appropriate support for its application in broader settings. Within the public health context in Samoa, health literacy measurement could provide more insight on how the target audience will perceive, appraise, and use public health information to increase the quality of public health interventions mitigating the impact of NCDs in Samoa. Further validation with a larger, more representative sample is essential to confirm the instrument’s psychometric properties and enhance its utility in national health planning.
Footnotes
Acknowledgements
In memoriam: We dedicate this work to the memory of Prof. Nanne de Vries, whose contributions to this study and to the field of health promotion were invaluable.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
(This manuscript was submitted on 11 July 2023. Following anonymous peer review, it was accepted for publication on 29 January 2026).