
Abstract
Background:
Religious leaders are influential and can impact the uptake of family planning (FP). In this study of the Healthy Timing and Spacing of Pregnancies (HTSP) project, led in Siaya County, Kenya, from September 2017 to June 2019, we present findings from the project’s evaluation, to determine changes in knowledge of the key HTSP messages; changes in the proportion of community members who correctly identify at least three methods of contraception; changes in knowledge of healthy child spacing; and changes in modern contraceptive prevalence rate.
Methods:
This is a two-staged (baseline and endline) cross-sectional study, designed to assess the knowledge, practice, and coverage of HTSP/FP services. Primary data was collected using a questionnaire adapted from the United States Agency for International Development. Focus group discussion participants included men, women, representatives of community groups, faith leaders, and community heath volunteers. Frequencies were calculated from the ODK platform. Bivariate analytics (paired t test) were performed.
Results:
At baseline, women respondents aged 20–29 years constituted 66.3% of the women participants, dropping to 60.9% at endline. Women aged 30–34 years constituted 11.9% and 22% of the entire women respondents, at baseline and endline, respectively. Men aged 20–29 constituted 45.2% of all men respondents at baseline, and 35.4% at endline. There were statistically significant increases in the knowledge of modern contraceptives among women (p = 0.0342), faith leaders (p = 0.0464), and the entire population (p = 0.0097), from baseline to endline.
Conclusion:
The HTSP model identifies success factors for FP interventions in Kenya and other low- and middle-income countries where faith leaders and community stakeholders are influential, and that women and faith leaders are much more easily impacted positively with these efforts, as measured by increased knowledge and awareness of modern contraceptive methods, compared with men.
Introduction
There is strong evidence on the positive effect of family planning (FP) on the health of mothers and children, as well as nations (1 –4). However, estimates show that 218 million women of reproductive age in low- and middle-income countries (LMICs) still have an unmet need for modern contraception (5). In light of the vast commitment of resources to FP, it is worth reconsidering available approaches to promote sustained, scalable, and impactful FP programming, especially in sub-Saharan Africa, the region with the world’s highest total fertility, and maternal and child mortality rates (6,7). One such approach, Healthy Timing and Spacing of Pregnancy (HTSP), significantly improves outcomes for mothers and their newborns (8,9).
Background/rationale
Kenya is a country of 52.8 million people (10), with 1.5 million annual births. Kenya’s maternal mortality ratio is 342 deaths per 100,000 livebirths, and its under-five mortality rate is 43 deaths per 1000 livebirths. About half (49%) of under-five deaths occur among newborns (0–28 days old). The national total fertility rate (TFR) is 3.4 births per woman (11); among adolescents aged 15–19 years, the birth rate is 96 per 1000 girls. Kenya’s modern contraceptive prevalence rate (mCPR) among all women is 53%. To our knowledge, there is no national data on the current level of FP-specific health education/promotion across health facilities in Kenya. Reports from Kenya have demonstrated the roles played by faith-based organizations (12), volunteer groups (13), community health workers (14), mass media (15), and clinicians (12). Religious leaders have long been identified as influential forces that can promote the health-seeking behavior of FP (16,17). By collaborating with community-based stakeholders, such health promotion could be deepened. Examples of faith leaders’ promotion of FP abound, particularly in sub-Saharan Africa (18,19), but success factors are usually varied and multi-faceted. This report describes the Healthy Timing and Spacing of Pregnancies Challenge Project in Siaya County, Kenya.
The HTSP Challenge Project builds on the Mobilizing for Maternal and Neonatal Health through Birth Spacing and Advocacy (MOMENT) project – implemented from 2013 to 2016 in Alego Usonga, a sub-county of Siaya. Adding five sub-counties (Bondo, Gem, Rarieda, Ugenya, and Ugunja), the goal of the project was to promote reproductive health through changing social norms, myths and misconceptions around HTSP and FP, and through the collaborative support of faith and government leaders to increase voluntary use of modern FP. Through health promotion, with a focus on demand creation and health systems strengthening, the HTSP/FP project aligned with the implementing organization’s long-standing commitment to support the efforts of Kenya in improving the health of women and of children under the age of five years. Modern contraceptives are not entirely free of charge in Kenya.
Objectives
To promote use of FP, the project aimed to expand the support of faith leaders from six sub-counties in Siaya County, Kenya (Figure 1) and was executed in partnership with the Siaya County Ministry of Health (MoH) and community stakeholders. This health promotion project is part of a larger effort to help communities embrace the benefits of child spacing and delayed childbearing, in order to achieve improved outcomes for mothers, children, and families.
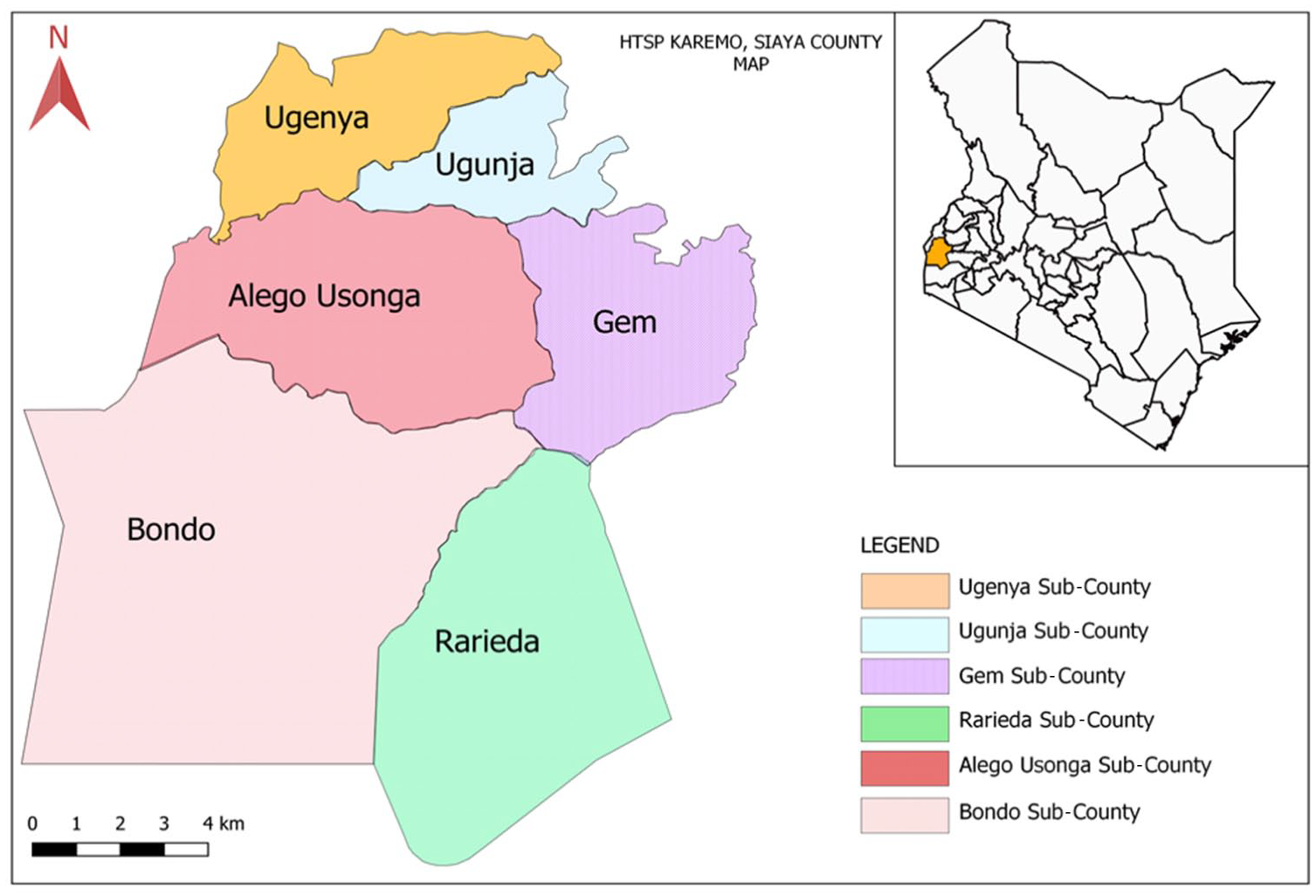
Map of Kenya’s Siaya County and its six sub-counties, with Siaya’s situation within Kenya in the inset.
The project’s expected outcomes were:
A 5 percentage points increase in community knowledge of each of the four key HTSP messages.
A 3 percentage points increase in proportion of community members who can correctly identify at least three methods of contraception, including long-acting reversible contraceptives.
A 10 percentage points increase among men and women (disaggregated) who know that a woman should wait until her child is at least two years old before attempting another pregnancy.
A 10 percentage points increase of the mCPR, from baseline.
Methods
Study design, population, and project setting
This study is of a two-staged (baseline and endline) cross-sectional design, to assess the knowledge, practice, and coverage (KPC) of HTSP/FP services in Siaya County, Kenya. According to the 2014 Kenya Demographic and Health Survey (KDHS), Siaya County is within a region whose unmet need for family planning is 23% and the TFR is 4.2, both higher than the national averages of 18% and 3.4, respectively. The population has been projected to reach 1,285,971 in the year 2030. Further, Siaya’s women of reproductive age (15–49 years old) are 24% of the county’s population, with adolescents and youths, ages 15–24 years, constituting 21%; and children under the age of five years old make up 18% (20,21).
The HTSP/FP project operated from September 2017 to June 2019 utilizing these two approaches – demand creation, and health systems strengthening.
Demand creation
The project employed three key approaches to foster demand creation:
Consistent messaging. The following messages were used, with the target audiences comprising faith leaders, community leaders, policymakers, health providers, men, women, adolescents, and youth. These messages were translated into Luo, the main language of Siaya: ■ ‘Too young’. Delay your first pregnancy until at least 18 years old. ■ ‘Too soon’. Wait at least six months after a miscarriage before attempting another pregnancy. ■ ‘Too close’. Wait at least two years after a birth before attempting another pregnancy. ■ ‘Too old’. Limit pregnancies to a mother’s healthiest years, ages 18–34.
Citizen Voice and Action (CVA). This is a social accountability approach that creates a forum for collaborative, non-confrontational dialogue. Through CVA, users are empowered to seek accountability for service delivery and take collective responsibility. CVA activities included structured meetings between community members and community health workers (CHWs) who used the HTSP messages. County officials and health care providers were also involved in advocacy for increased resources to improve maternal and child health (MCH) and HTSP/FP services.
Channels of Hope (CoH). This is an interactive process which mobilizes faith leaders to respond to issues affecting their communities — such as HIV/AIDS, MCH, and gender equity. Developed by the implementing organization, CoH does not proselytize, but, rather, equips faith leaders to better understand the issues and apply their sacred texts and beliefs as appropriate for health promotion. In this project, the training of 80 faith leaders in each sub-county was employed, utilizing the MCH-CoH module, updated with HTSP. The module includes learning activities to outline relevant science and facts, dispel misinformation and illustrate linkages between HTSP and the well-being of mothers and children. The goal was that faith leaders and the Congregational Hope Action Teams, formed during CoH, would be prepared to promote MCH/HTSP messaging.
Health systems strengthening
With the anticipated increased demand for HTSP/FP services, this project also focused on expanding the knowledge and skills of nurses to help ensure quality health services. The goal was to improve nurses’ ability to provide HTSP counseling, and information on a broader mix of modern contraceptives, including natural methods (e.g. CycleBeads®), as well as long-acting reversible contraceptives. To address the issue of stockouts, nurses were trained to forecast FP commodities. Additionally, CHWs across the six sub-counties were trained in HTSP messaging and how these messages relate to better MCH outcomes.
Data collection and procedure
Primary data was collected through questionnaires (baseline and endline) using a KPC questionnaire adapted from the United States Agency for International Development’s Maternal and Child Health Integrated Program (22). Focus group discussion (FGD) participants included men, women, community groups representatives, faith leaders, and community health volunteers. FGD participants were selected through snowball sampling based on initial referrals from sub-county officials in the six sub-counties of Siaya. Key informant interviews (KIIs) targeted the county director of health, faith leaders, CVA teams, and health facility in-charges. Overall, inclusion criteria for selection of research participants (KPC-adapted questionnaire, FGDs, and KIIs) include being a decision-maker, or being affected by the decision-making, of choices of promotional messaging related to healthy timing and spacing of pregnancies and family planning. Essentially, this included persons of parental capacity, and those sexually active, in a domestic setting. However, community stakeholders, including volunteers, groups’ representatives, and especially faith leaders, were also included as research participants. Women respondents were those with children under 24 months of age.
Interviews were conducted using the Open Data Kit (ODK) mobile platform, and administered to the interviewees by supported field enumerators, through application-based mobile technology, between September 2017 and June 2019. Secondary data was obtained through desk reviews of relevant projects and other related documents, such as the project’s baseline and progress reports, Siaya County Integrated Development Plan 2018–2022, and the 2014 KDHS. Before fieldwork, the aforementioned data collection tools were developed, and field enumerators and FGD facilitators were trained.
Pre-testing of tools was conducted prior to the data collection, using a combined pool of 70 research participants reached through snowball sampling. The ODK mobile platform was pre-tested among 56 women, men, and youth, while the KII interview guide was pre-tested among 14 faith leaders and health facility in-charges. In total, 3300 questionnaires were successfully completed with a final sample of 900 women, 900 men, 900 faith leaders, and 600 adolescents and youth. Twelve FGDs and 30 KIIs were also conducted. Due to the cross-sectional design of this study, there was no specific intent to calculate sample size or power for an effect estimate, as is seen with the computation of risk ratios and odds ratios, for example.
Statistical analyses
The frequencies calculated (baseline and endline) were obtained from the ODK platform, and these were expressed as percentages. Bivariate analytics (paired t test) determined whether differences in the knowledge of modern contraceptives, from baseline to endline, were statistically significant. There was no baseline data for the adolescents and youth sub-population group, so the paired t test was not performed for this group. Another paired t test was performed on the total population’s baseline and endline frequencies. These percentage frequencies, for each modern contraceptive, were imputed as decimal figures in a spreadsheet, and loaded into the SAS® version 9.4 statistical computing platform (SAS Institute, Cary, North Carolina, USA) for paired t test analysis, in order to generate t values and p values.
Ethical considerations
This was a project implementation. We did a baseline and endline to measure impact on the project’s indicators. Informed consent was obtained from all research participants, and they were assured they were free to terminate their involvement at any time. There was no institutional review board approval for this project.
Results
Background characteristics
The baseline features of adolescents and youth were not captured ab initio. Nonetheless, on the advice of the Siaya County MoH, this group was included in the endline evaluation. Supplemental material Table 1 online shows the demographic characteristics of the sampled respondents. At baseline, women respondents between the ages of 20 and 29 years constituted 66.3% of the entire women participants, but this dropped to 60.9% at endline. For those women between the ages of 30 and 34 years, they constituted 11.9% and 22% of the entire women respondents, at baseline and endline, respectively. In contrast, men respondents of ages 20–29 were 45.2% of all men respondents at baseline, and 35.4% of all men at endline. Faith leaders, however, tended to be older (⩾45 years). Primary school education was the most prevalent level of education completed. Christianity is the main religion, accounting for about 86.7% (Protestant, 60.9%; Catholic, 25.8%) at endline. Respondents who were married or cohabiting at the time of study constituted 80.7%, while about 10% were either widowed, separated, or divorced.
Knowledge of HTSP and contraceptive methods
About 59% of respondents reported they had received HTSP/FP information. The majority (80.3%) received this information at a government/public health facility, followed by media (18%), community gatherings (16.5%), and health outreach events (11.8%). Community knowledge of each of the four HTSP messages indicated some improvement from baseline, as shown in Supplemental material Table 2, with knowledge of ‘Too soon’ exceeding the anticipated five percentage points increase. Supplemental material Table 3(a) describes respondents’ knowledge of modern contraceptives. Overall, there was an improvement in knowledge for all methods except the IUD. The proportion who knew at least three FP methods showed major increases from the baseline, exceeding the three percentage points target. At baseline, 66.4% of women knew at least three FP methods; this increased by 12.3 percentage points at endline. Among men, this measure increased by 12.0 percentage points, from a baseline of 51.1%. Among faith leaders, the increase was by 13.7 percentage points, from a baseline of 53.3%.
Supplemental material Table 3(b) shows the mean of the differences in knowledge of modern contraceptives, from baseline to endline, when each modern contraceptive option in Supplemental material Table 3(a) is entered into a spreadsheet as a separate observation. The results of the paired t test, which tested the null hypothesis of no difference between baseline and endline frequencies, are displayed in Supplemental material Table 3(b). The highest mean difference is seen among the total combined population (0.1066, SD 0.1109), and the least mean difference is seen among men (0.0743, SD 0.1108). We see statistically significant increases in the knowledge of modern contraceptives among women (p = 0.0342), faith leaders (p = 0.0464), and the entire population (p = 0.0097), from baseline to endline.
Support of men and faith leaders for HTSP/FP services
Figure 2 depicts the type of support women reported they received from their men. Moral support (e.g. being accompanied to the FP clinic) was most frequently cited at 59%, while one-third mentioned financial support to access the services. More than half of the interviewed women, across the six sub-counties (Figure 3), felt that men were generally positive about HTSP/FP services. This was highest in Gem sub-county, where more than 80.0% of women reported positive men’s perception, followed by Ugenya (79.2%) and Alego-Usonga (78.5%) sub-counties. Overall, 61.9% of the community members at endline, compared with 55.0% at baseline, felt that their faith leaders’ perception of HTSP/FP services had improved.
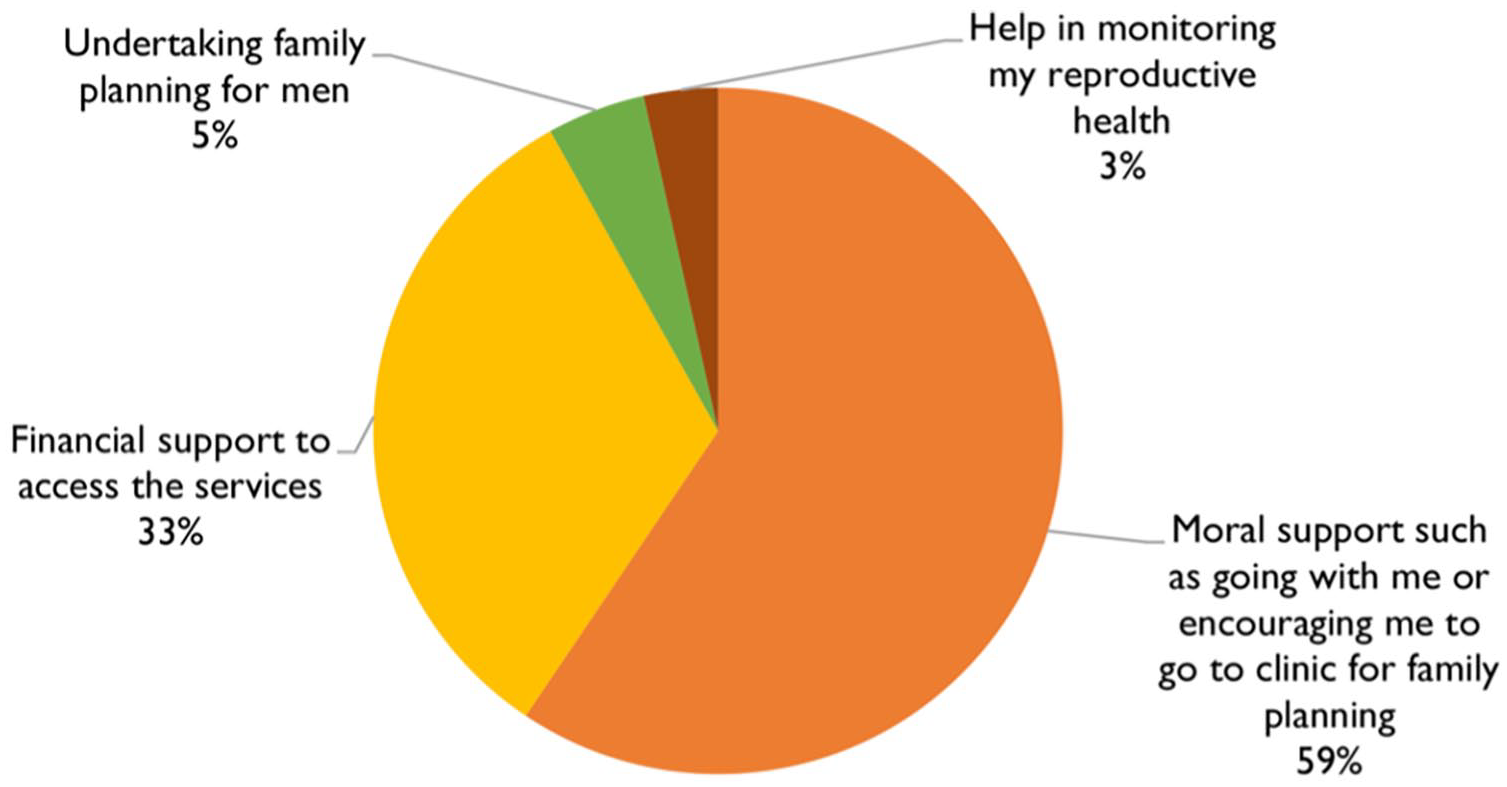
Types of male support received by women.
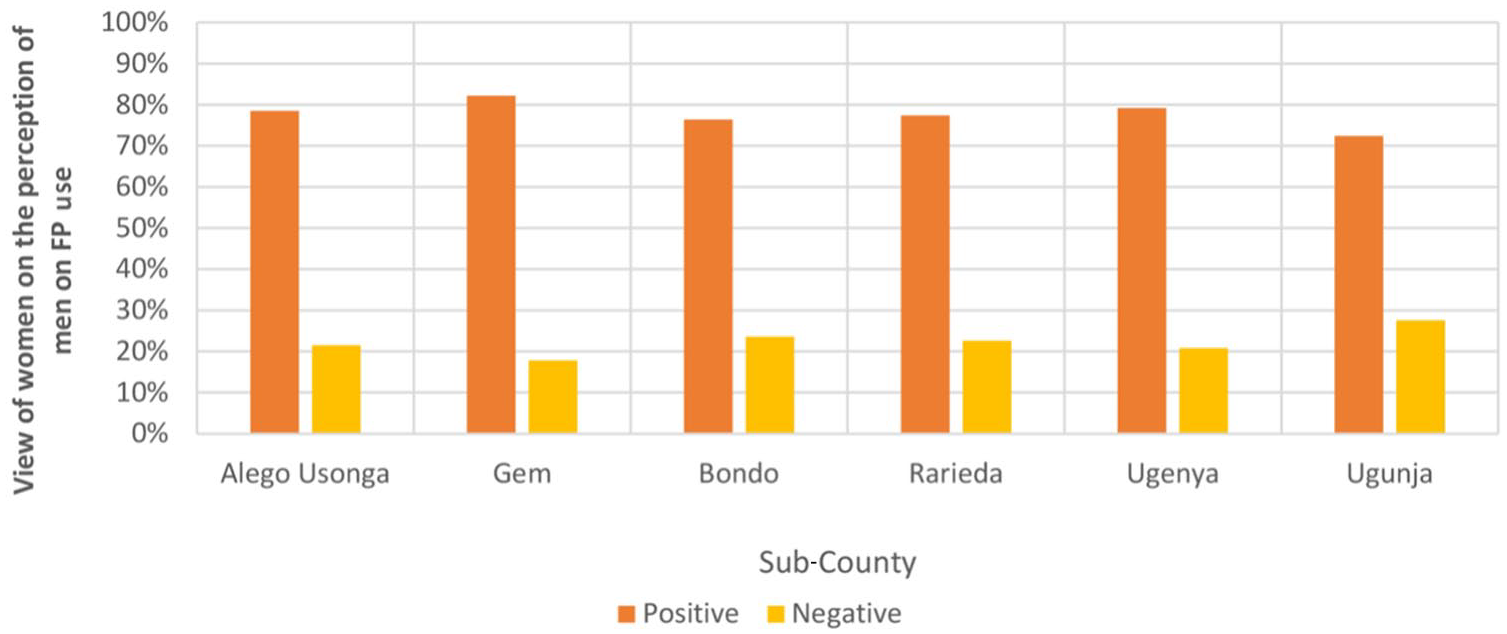
Views of women on the perception of men on FP use, by sub-county.
Contraceptive prevalence
The prevalence rate for modern contraceptives at endline was 66.7%, an increase of nearly five percentage points from baseline. This is higher than Kenya’s national mCPR of 53%.
Facility staff training and FP commodities
The project engaged with 90 health facilities, 15 in each sub-county. Supplemental material Table 4 describes the distribution of the 205 clinical providers trained on all contraceptive methods. KIIs revealed that implants and female condoms were the most available contraceptives at their facilities within the study period. The visited facilities had male condom dispensers accessible to all clients, but several were out of stock in the study period. Respondents indicated that uptake of FP commodities increased as a result of HTSP/FP promotion.
Discussion
Our findings mirror similar projects in Kenya’s Siaya County, where faith leaders and community volunteers helped improve FP access (12). Our work adds to this body of evidence, and there are similar contexts with previous research that have shown the increased potential for reproductive health promotion from education about, as well as awareness of, FP benefits, following engagement with faith leaders (23). In line with the project’s aforementioned objectives, our findings suggest that educating faith and community leaders on HTSP/FP, who then are equipped to inform and educate their communities, advances the health promotion of voluntary FP services. A critical understanding and documentation of these efforts will expand the knowledge base. Throughout the literature, our case study is the first to report outcomes on a sub-county level within Kenya’s Siaya County. In general, Outcome 1 results can be attributed to the health promotion activities of faith leaders and CHWs, through the use of the HTSP/FP messaging, with FGD discussions revealing that messages in the local language (not English) were more effective for sub-counties. The high positive perceptions were attributed to men’s involvement in the health promotion efforts of HTSP/FP messaging. KIIs revealed that, in instances where they were not consulted, some men would push for discontinuation of FP methods.
There was improvement in the knowledge of HTSP messages among women. In comparison with baseline, the largest differences were seen in the ‘Too close’ and ‘Too young’ messages, with increases of 8.8 and 5.4 percentage points, respectively. Conversely, male respondents showed a 16.9 percentage points increase in the ‘Too soon’ messages; nearly no change in ‘Too young’ and a decrease in the ‘Too close.’ The 3.2 percentage points decline in the knowledge of ‘Too old’ messages among men may be attributed to the biological fact that, even at advanced ages, men can continue to father children. These findings highlight the urgent need for male involvement and engagement in HTSP/FP health promotion. HTSP messaging on ‘Too close’ and ‘Too soon,’ coupled with CVA activities and HTSP messaging coming from faith leaders on voluntary use of modern contraceptives, may have resonated more with women, contributing to these results. The recognition that faith leaders’ perception of HTSP/FP had improved was attributed to CoH training, and the health promotion faith leaders performed in spreading HTSP/FP messages. KIIs with faith leaders revealed that some of them did not necessarily organize any forums, separate from their regular religious services, to promote HTSP/FP in their communities. Additionally, some faith leaders were older (⩾60 years) and either not well conversant with HTSP/FP or were uncomfortable promoting it. Overall, these results demonstrate the potential of longer time frames of reproductive health promotion interventions using HTSP/FP messaging.
It is worthy of note that mean differences in the knowledge of modern contraceptives, from baseline to endline, were statistically significant, except among men. This may be useful in reproductive health promotion planning and implementation, as it lends credence to the evidence that HTSP/FP approaches aimed at expanding knowledge and awareness of modern contraceptives may be better deployed at women and faith leaders, especially where resources are limited.
The key challenges experienced in this project’s implementation included myths and misconceptions around the harmful effects of FP, religious doctrines that discourage FP, weak spousal support, staff shortages and unskilled staff, especially in government-owned health facilities, insufficient youth-friendly services and limited supply of FP commodities. Creating demand for modern contraception is only effective if supplies are available to meet that demand. Situating these findings within the context of Kenya’s comparatively better performance (24) relative to other countries in the region emphasizes the niche importance of this critical FP promotion. Sustained behavior change, especially for social norms, happens over time, and is linked to many factors. Long-term investments and multisector engagement are thus needed to realize success. Governments and other stakeholders should collaboratively consider results from health promotion efforts like these, as they expand approaches to improve uptake of FP services.
Strengths and limitations
In addition to the aforementioned results, the strengths of this study include its innovation, as the first to explore FP knowledge in Siaya County on a sub-county level, as well as its experimental/intervention approach. The limitations include the short project implementation time frame (<2 years), and the vast intervention area, worsening transportation problems for CHWs, and difficult one-on-one supervision of the enumerators during data collection. Covering such a large area within this limited time frame was challenging for achieving expected outcomes. Another limitation was that HTSP messages were translated into Luo, ahead of project activities. During implementation, however, we learned that the Luo dialect is slightly different from sub-county to sub-county, with a potential for systematic errors. Finally, the request by Siaya County MoH to include adolescents came after baseline results. Hence baseline measurements for adolescents and youth are unavailable. This limits the utility of the information for endline analysis but may be beneficial for the Siaya County government as they plan reproductive health strategies for this population group.
Recommendations
Utilizing approaches such as CoH and CVA social accountability early on in faith-based reproductive health promotion interventions will help increase comprehension of the unique contexts in which faith leaders are willing and able to embrace FP goals, and advance the success of such interventions. Therefore, faith leaders and community actors must be intricately involved in the design, implementation, and evaluation of sexual and reproductive health policies, projects, and programs, as well as their linkages to maternal and child health.
Future research directions
Governments, academic researchers, and global health stakeholders in LMICs should consider HTSP and FP efforts at more granular, sub-national levels, when researching to delineate deficient areas. Detailed analyses and subsequent interventions may help tease out and address challenges that may be missed in those focused on larger geographical areas. Other future research directions recommended include the potential moderation (statistical interaction) by faith leaders’ knowledge and communication of HTSP/FP on the effect of school-based comprehensive sexuality education for adolescents in sub-Saharan African countries.
Conclusion
A cautious overall interpretation of the results of this study includes the fact that the HTSP model described in this study identifies important processes and success factors for developing, implementing, and evaluating FP interventions in Kenya and other LMICs where faith leaders and community stakeholders are influential, and that women and faith leaders are much more easily impacted positively with these efforts, as measured by increased knowledge and awareness of modern contraceptive methods, compared with men. Continuous and interlinked approaches by trained faith leaders and health workers using the same HTSP messages throughout Siaya County could, over time, sustain social norm changes. Despite pockets of modest successes, FP programming in LMICs remains beset with inadequacies, as well as poor demand-seeking behavior. By engaging trained faith leaders and community actors in the manner described in this report, sub-Saharan Africa has an opportunity to move closer to its demographic dividend, through a scale-up of high-impact and broad-reach HTSP/FP programming.
Supplemental Material
sj-docx-1-ped-10.1177_17579759241252787 – Supplemental material for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya
Supplemental material, sj-docx-1-ped-10.1177_17579759241252787 for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya by Susan A. Otchere, Isabellah Moraa, Vincent Rotich, Stephen Omunyidde and Kimberly Q. Jillson in Global Health Promotion
Supplemental Material
sj-docx-2-ped-10.1177_17579759241252787 – Supplemental material for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya
Supplemental material, sj-docx-2-ped-10.1177_17579759241252787 for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya by Susan A. Otchere, Isabellah Moraa, Vincent Rotich, Stephen Omunyidde and Kimberly Q. Jillson in Global Health Promotion
Supplemental Material
sj-docx-3-ped-10.1177_17579759241252787 – Supplemental material for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya
Supplemental material, sj-docx-3-ped-10.1177_17579759241252787 for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya by Susan A. Otchere, Isabellah Moraa, Vincent Rotich, Stephen Omunyidde and Kimberly Q. Jillson in Global Health Promotion
Supplemental Material
sj-docx-4-ped-10.1177_17579759241252787 – Supplemental material for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya
Supplemental material, sj-docx-4-ped-10.1177_17579759241252787 for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya by Susan A. Otchere, Isabellah Moraa, Vincent Rotich, Stephen Omunyidde and Kimberly Q. Jillson in Global Health Promotion
Supplemental Material
sj-docx-5-ped-10.1177_17579759241252787 – Supplemental material for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya
Supplemental material, sj-docx-5-ped-10.1177_17579759241252787 for The Healthy Timing and Spacing of Pregnancies (HTSP) project: improving family planning in Siaya County, Kenya by Susan A. Otchere, Isabellah Moraa, Vincent Rotich, Stephen Omunyidde and Kimberly Q. Jillson in Global Health Promotion
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The John Templeton Foundation (grant identification number 60851).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.