
Abstract
This study sought to examine gender differences in emotional reactions and compliance with Ministry of Health (MOH) guidelines during the COVID-19 pandemic in Israel, with the goal of gaining a deeper understanding of these gender-related variations throughout the lockdown periods. A longitudinal study comprising 2509 participants was conducted during two of Israel’s lockdowns: 1424 participants completed a questionnaire during the first lockdown (23 April–5 May 2020); of these, 1085 completed a follow-up questionnaire during the second lockdown (September 30–October 10, 2020). Participants exhibited higher levels of compliance with MOH guidelines (e.g., wearing face masks, maintaining social distancing) and knowledge about COVID-19 during the second lockdown, whereas they exhibited more negative emotional reactions during the first lockdown. Female participants scored higher than male participants on all measures. Multiple regression results showed that about 21% of the variance in compliance with MOH guidelines was explained by lockdown type (i.e., first or second), gender, and age, while knowledge and negative emotional reactions added another 19% to the explained variance. The results suggest that the impact of the pandemic on emotional reactions decreased over time, with people exhibiting greater compliance with MOH guidelines and more knowledge about COVID-19. Moreover, the behavioral and psychological impact of the pandemic was greater on women than on men. The results suggest that healthcare professionals should pay more attention to mental health issues during a pandemic. Moreover, policymakers should focus on women as a vulnerable group and suggest appropriate solutions to reduce their emotional distress. Furthermore, governments and employers should provide greater flexibility and support for single mothers during the pandemic. In addition, gender inequality during lockdowns may place women at greater risk of psychological distress.
Introduction
On 11 March 2020, the World Health Organization (WHO) (1) issued a declaration stating that COVID-19 (the disease caused by the SARS-CoV-2 virus) was a global pandemic. According to the latest WHO figures, the virus has infected over 770 million people worldwide, and more than 6,950,000 have succumbed to it (1). The results of a meta-analysis of global COVID-19 cases showed no differences between the numbers of men and women affected by the disease (2). Nevertheless, the long-term impact of gender in the context of COVID-19 is still unknown, particularly in terms of the effects of the lockdowns necessitated by the pandemic. Professionals have many reasons to be alarmed by the pandemic’s rapid and persistent detrimental impact on mental and physical health (3,4). In Israel, these lockdowns dictated that people must stay at home at all times, other than for purposes of work, health (e.g., doctor’s appointments), or purchasing necessities.
Lockdowns have been found to be an effective means of limiting the spread of disease during pandemics. Nevertheless, prolonged confinement at home can have deleterious effects on physical as well as mental health (5). Among these effects are symptoms of depression and anxiety, as well as acute stress disorders (6). Research conducted during the pandemic shows that women tend to report more mental health issues than men (7,8). Yet this gender difference also appears during normal times (9) and, therefore, cannot necessarily be attributed to lockdowns. In view of this, we sought to discover whether there were further gender differences in mental health during the lockdowns. A study that examined psychological and behavioral symptoms among the general non-infected population in Israel during the first two weeks of April, when restrictions were at their most severe, found that levels of anxiety and depression, poor sleep quality, and a tendency toward emotional eating predicted adjustment difficulties. Other variables that predicted adjustment difficulties included being female, intensive news consumption, and a decline in economic status due to the pandemic (10). The survey, conducted among 187 Israeli physicians, found that female physicians experienced higher levels of negative emotions than male physicians during COVID-19 (11).
Bangasser and Wicks (12) found that gender differences in stress response systems are manifested in increased endocrine, affective, and arousal responses to stress among women. Moreover, women’s predominant roles as family caregivers and frontline healthcare workers also serve as gender-related factors (13). Thelwall and Thelwall (14) examined tweets in English related to COVID-19. They found that women’s tweets about the virus referred mainly to family, social distancing, and healthcare, whereas men’s tweets focused on sports cancellations, the global spread of the virus, and political reactions. These findings are reinforced by the results of a cross-sectional study suggesting that women, individuals with previous psychiatric illnesses, and those with preexisting conditions are most likely to be affected psychologically by the pandemic (15,16).
A longitudinal survey from the UK before and during the lockdown period showed that women, and especially mothers who shouldered the major burden of housework and childcare, exhibited the most dramatic decline in well-being during the pandemic (17). The survey also pointed to strong gender differences in emotional reactions. Other studies, however, revealed no gender differences in health behavior or emotional distress during the pandemic (18,19). Indeed, some studies found higher values of extraversion or anxiety among men (20,21). Unlike previous studies, two cross-sectional surveys conducted in Israel about COVID-19 did not find that adherence to distancing regulations, or stress were predicted by age, gender, or subjective health status (22,23). Two other studies conducted during the second lockdown in Israel found a significant main effect of gender, with women reporting higher levels of posttraumatic growth than men (24,25).
The effectiveness of official health guidelines depends on the public’s level of compliance, which often varies according to social group and location. Studies conducted in Israel examining compliance to Ministry of Health (MOH) guidelines at different times during the pandemic reveal a significant gender difference, with women reporting greater intentions to comply than men (8,26). Zhong et al. (27) further found that women were better informed about COVID-19 than men and tended to comply more with official guidelines such as wearing masks and social distancing.
Previous studies of COVID-19 compliance guidelines that took knowledge into account consistently found a positive association between knowledge level and adherence to COVID-19 protective measures (28). A study conducted in Germany revealed that 9 out of 10 adults felt they were well informed or very well informed about COVID-19. Moreover, women more frequently reported feeling confused by the variety of information about COVID-19 than men (29). Other studies show that the female gender exhibited a significant association with adequate knowledge (8,30).
The current study
The current study used longitudinal data to examine gender differences during two lockdowns in Israel. Our aim was to examine the impact of gender on people’s knowledge about the virus, their compliance with MOH guidelines, and the nature of their emotional reactions to COVID-19. By examining the evolution of gender differences in emotional reaction and compliance with MOH guidelines during the pandemic, we seek to understand whether the lockdowns have had any impact upon structural gender differences (8).
The study’s hypotheses are the following:
H1: Compliance with MOH guidelines, knowledge about COVID-19, and negative emotional reactions will be higher in the second phase than in the first.
H2: Compliance with MOH guidelines, knowledge about COVID-19, and negative emotional reactions will be higher among women than among men.
H3: The associations between knowledge about COVID-19, negative emotional reactions, and compliance with MOH guidelines will be higher for women than men.
Method
Participants and procedure
The study was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for observational studies (31). The Ethics Committee of Bar-Ilan University approved the study (Authorization No. 032003). Data from across Israel were collected during two periods via the Qualtrics online platform. A link to the electronic survey was distributed via Facebook™. Before completing the survey, participants were asked to read an informed consent form and indicate their agreement to participate. The sampling technique was a combination of non-probability consecutive sampling and snowball sampling. Participants were 2509 Israeli citizens: 1424 participants completed the study questionnaire during the first lockdown (23 April–5 May 2020); and 1085 of these same participants completed a follow-up questionnaire during the second lockdown (30 September–10 October 2020) (Figure 1).
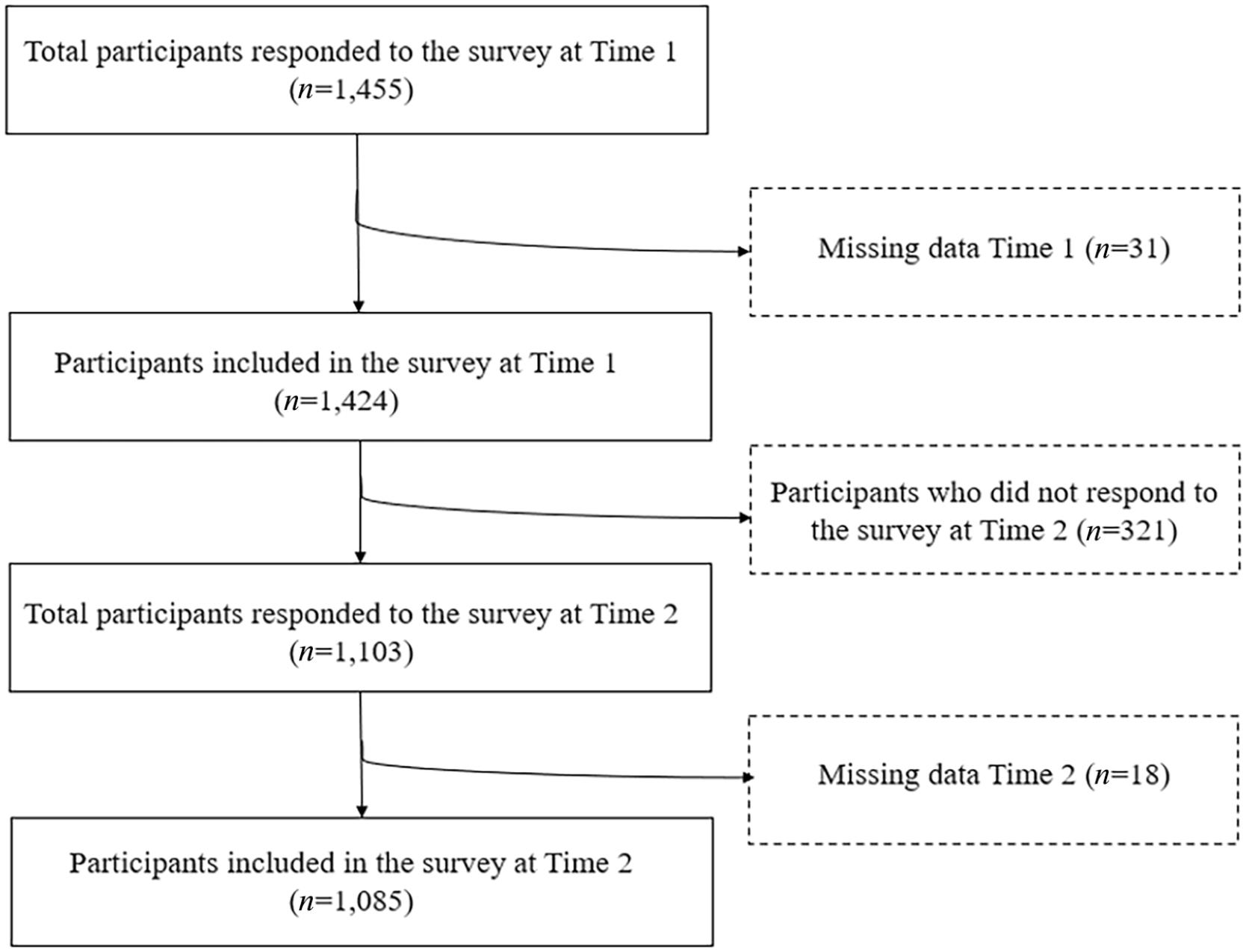
Flowchart illustrating participant selection.
Participants were given the following instructions: participation in this study is anonymous; you do not have to answer any questions that make you uncomfortable and you can withdraw from participation at any time; the data will be used for research purposes only. All participants gave their informed consent by clicking on the following option: ‘I freely consent to participate in this survey’. Inclusion criteria were Hebrew speakers over the age of 18.
At the end of the questionnaire, participants were asked to provide their e-mail addresses to enable the researchers to contact them for a follow-up study. When the second lockdown was announced, the researchers decided to conduct a comparison of the two lockdowns. Not all participants from the first wave participated in the second wave. Among the reasons for failing to participate in the second wave were the following: e-mails that bounced back due to inactive or erroneous addresses; participants who declared they were too busy to answer the second questionnaire; and lack of time. For each wave, data collection ended after a period of 10 days. The participants’ e-mail addresses were deleted after the second wave.
Measures
The following variables were measured during both lockdowns:
Compliance with MOH guidelines was measured by participants’ responses to four positive statements reflecting precautionary guidelines issued by the Israeli MOH (3,4,8,32). Sample items included: ‘To what extent do you comply with the instructions to stay at home during the lockdown?’ and ‘To what extent do you comply with the social distancing guideline of 2 meters?’. Participants answered on a 5-point Likert scale, ranging from 1 (a very small extent) to 5 (a great extent). Scale validity was assessed by a panel of four expert physicians. This assessment, referred to as expert validity (a form of content validity), aimed to eliminate any completely irrelevant items from the instrument and to rephrase or reword items related to the measured construct, as necessary. We generated a composite index based on the average of all items, with a higher score indicating greater compliance with MOH guidelines. Cronbach’s α = 0.85.
Knowledge about COVID-19 was measured by six items covering COVID-19 symptoms: diagnosis, risk factors, means of spreading infection, ways to safeguard against COVID-19 infection, and knowledge in relation to when suspected cases should be referred for treatment (3,4,8,32). A sample item is the following: ‘Older adults and those with series chronic illnesses such as diabetes are at increased risk of developing more serious complications from COVID-19’. Participants answered on a 5-point Likert scale, ranging from 1 (a very small extent) to 5 (a great extent). We generated a composite index of the average of all items, with higher scores indicating higher levels of knowledge about COVID-19. Cronbach’s α = 0.82.
Emotional reactions to COVID-19 were assessed using three questions about stress, fear, and worry in the context of COVID-19. These questions were sourced from previous studies conducted among the general public (3,4,8,32): ‘To what extent do you worry about COVID-19?’, ‘To what extent are you afraid of COVID-19?’ and ‘To what extent are you stressed about COVID-19?’ Participants answered on a 5-point Likert scale ranging from 1 (a very small extent) to 5 (a great extent). We created a composite index of the average of all items, with higher scores indicating higher levels of negative emotional reactions toward COVID-19. Cronbach’s α = 0.94.
Socio-demographic variables included gender, age, years of education, marital status, number of children, employment status, and subjective health evaluation.
Statistical analyses
SPSS v27 was used to analyze the data. The analyses compared demographic and background characteristics, subjective health evaluation in the context of coping with the COVID-19 lockdowns, and gender. Chi-square tests and z-tests of dependent proportions were used to measure categorical variables, and dependent sample t-tests were used to measure continuous variables. A series of analyses of covariance were used to measure compliance with MOH guidelines, COVID-19 knowledge, and negative emotional reactions by lockdowns and gender, while controlling for age. We calculated a multiple hierarchical regression for compliance with MOH guidelines, COVID-19 knowledge, and negative emotional reactions, while controlling for lockdowns, gender, and age. The third step of the regression model involved standardizing the variables, defining all second- and third-order interactions with lockdowns and gender, and entering them in a stepwise manner. Significance level was set at p = 0.01.
Results
In this study, 2509 Israeli citizens were surveyed during the COVID-19 outbreak: 1424 participants answered a questionnaire during the first lockdown; and 1085 of these same participants answered a follow-up questionnaire during the second lockdown. During both survey periods, most respondents were women (79.8%–77.5%) between the ages of 18 and 97 (Lockdown 1: M = 40.7, SD = 14.78; Lockdown 2: M = 45.13, SD = 15.16). Most participants were married (62.3%–66.7%) and had up to three children. About 83% of the respondents were employed during the first lockdown, compared to about 69% during the second lockdown. This difference is significant. Most respondents reported good subjective health (79% of the participants in the first lockdown and about 66% of the participants in the second lockdown), with no gender difference. A higher percentage of both men and women reported good health during the first lockdown than during the second (χ2 (2) = 28.44 and χ2 (2) = 51.29, p < 0.001, respectively; Table 1).
Participants’ background characteristics (N = 2509).
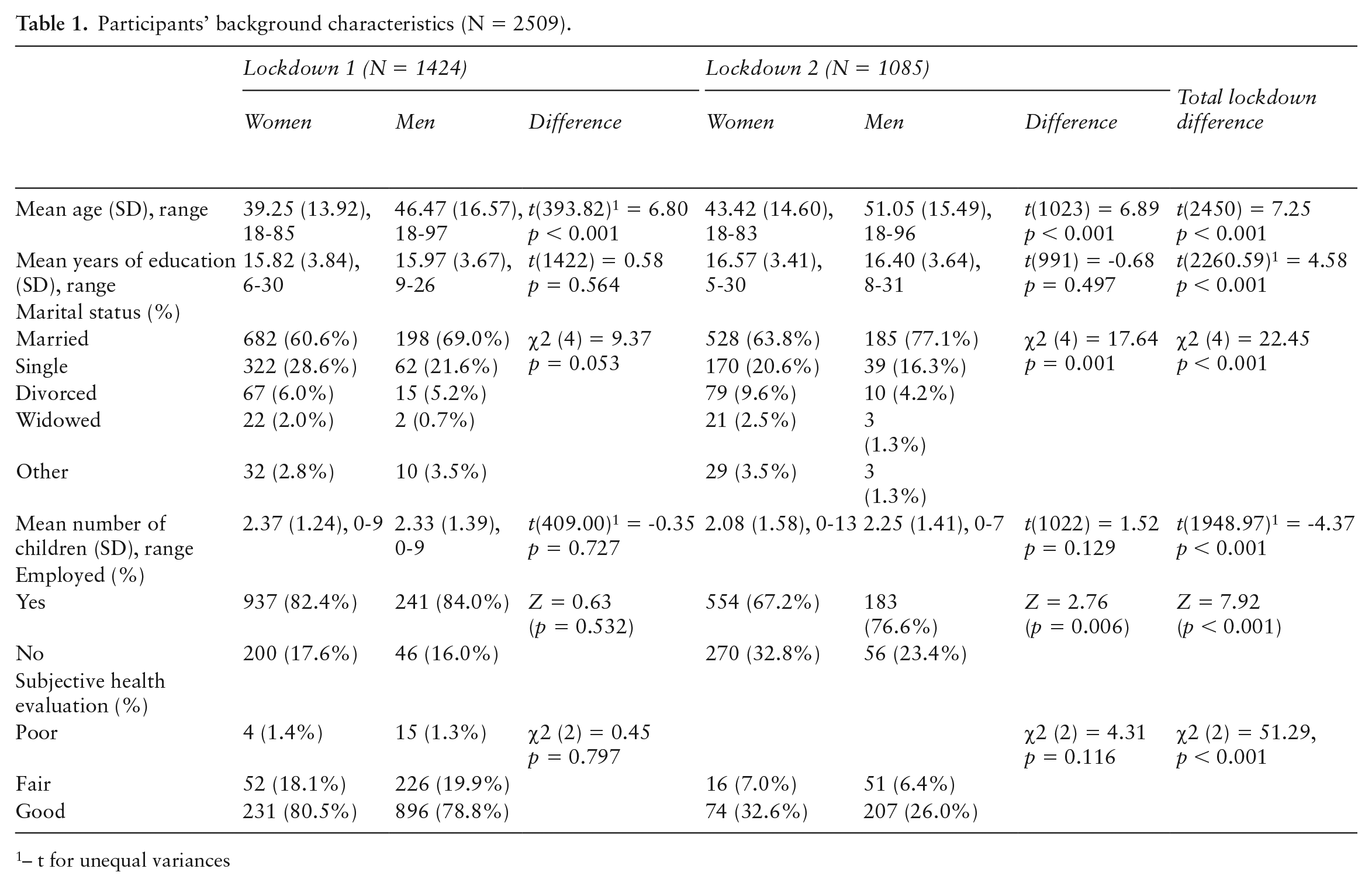
– t for unequal variances
Compliance with MOH guidelines, knowledge about COVID-19, and negative emotional reactions were significantly and positively higher in the second phase than in the first, supporting Hypothesis 1 (Table 2). Moreover, compliance with MOH guidelines, knowledge about COVID-19, and negative emotional reactions were higher among women than among men, supporting Hypothesis 2.
Correlates, Means, SDs, and ranges of study variables (N=2509).
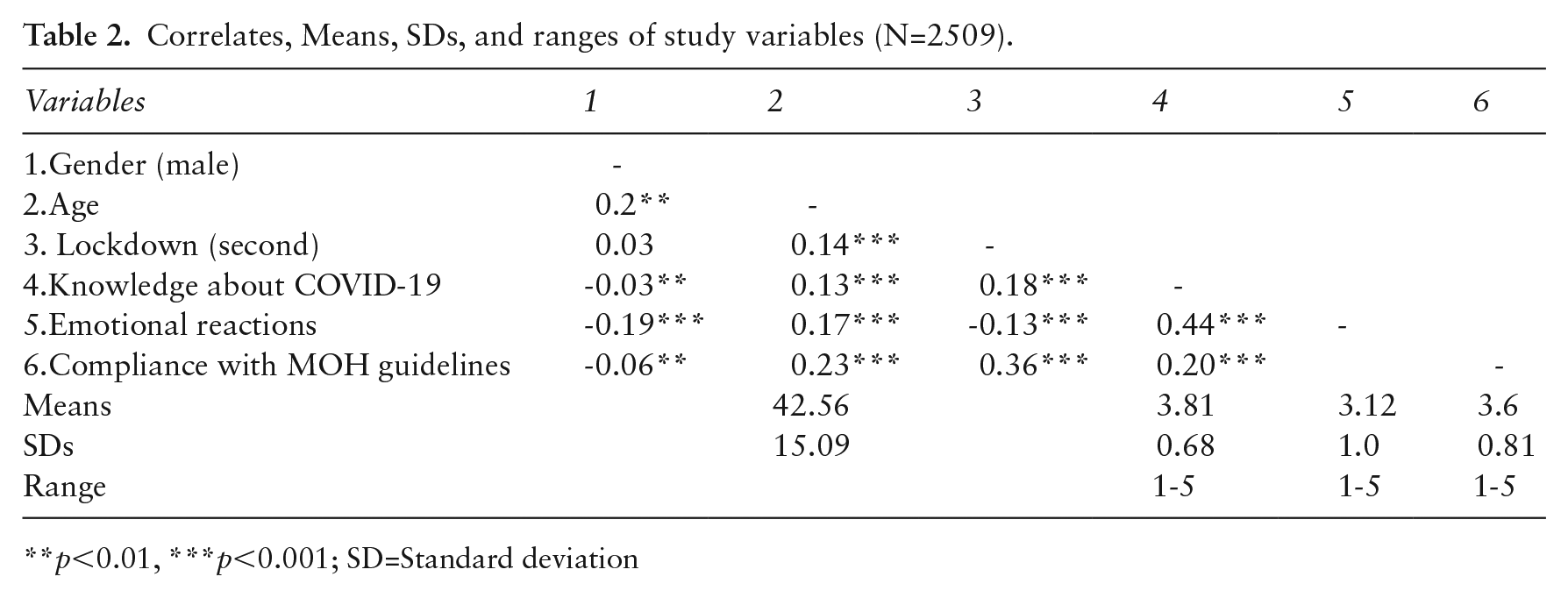
p<0.01, ***p<0.001; SD=Standard deviation
We ran a multiple hierarchical regression for compliance with MOH guidelines, with COVID-19 knowledge and negative emotional reactions serving as factors, while controlling for lockdown (0, first; 1, second), gender (0, women; 1, men), and age (Table 3). About 21% of the variance in compliance with MOH guidelines was explained by lockdown, gender, and age, while COVID-19 knowledge and negative emotional reactions added another 19% to the explained variance. Compliance with MOH guidelines was higher in the second lockdown, higher for women than for men, and higher among older participants. Beyond these background variables, compliance with MOH guidelines was higher when knowledge about COVID-19 was higher and negative emotional reactions were greater.
Multiple hierarchical regression for compliance with MOH guidelines (N = 2509).
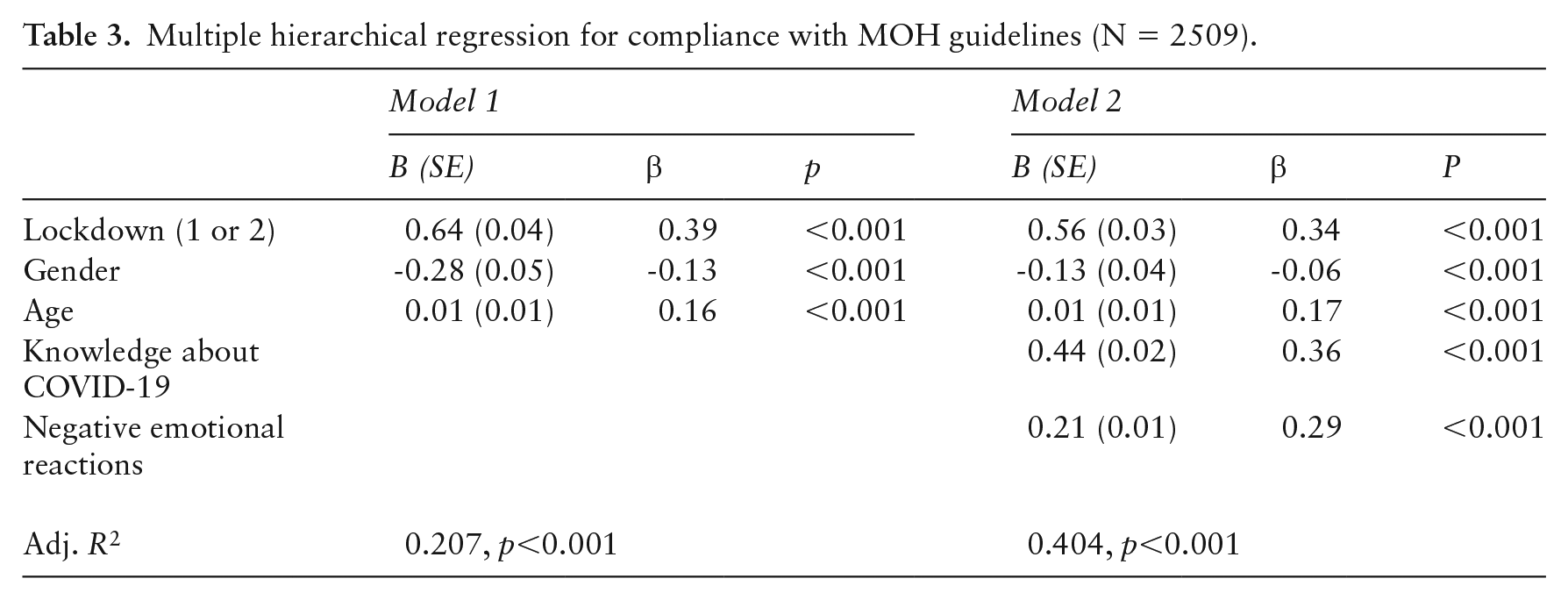
Table 4 presents the distribution of the study variables (compliance with MOH guidelines, COVID-19 knowledge, and negative emotional reactions) by lockdown and gender. For each variable, we calculated a two-way analysis of covariance that included lockdown and gender as independent variables and controlled for age.
Compliance with MOH guidelines, knowledge about COVID-19, and negative emotional reactions, by lockdown and gender (N = 2509).
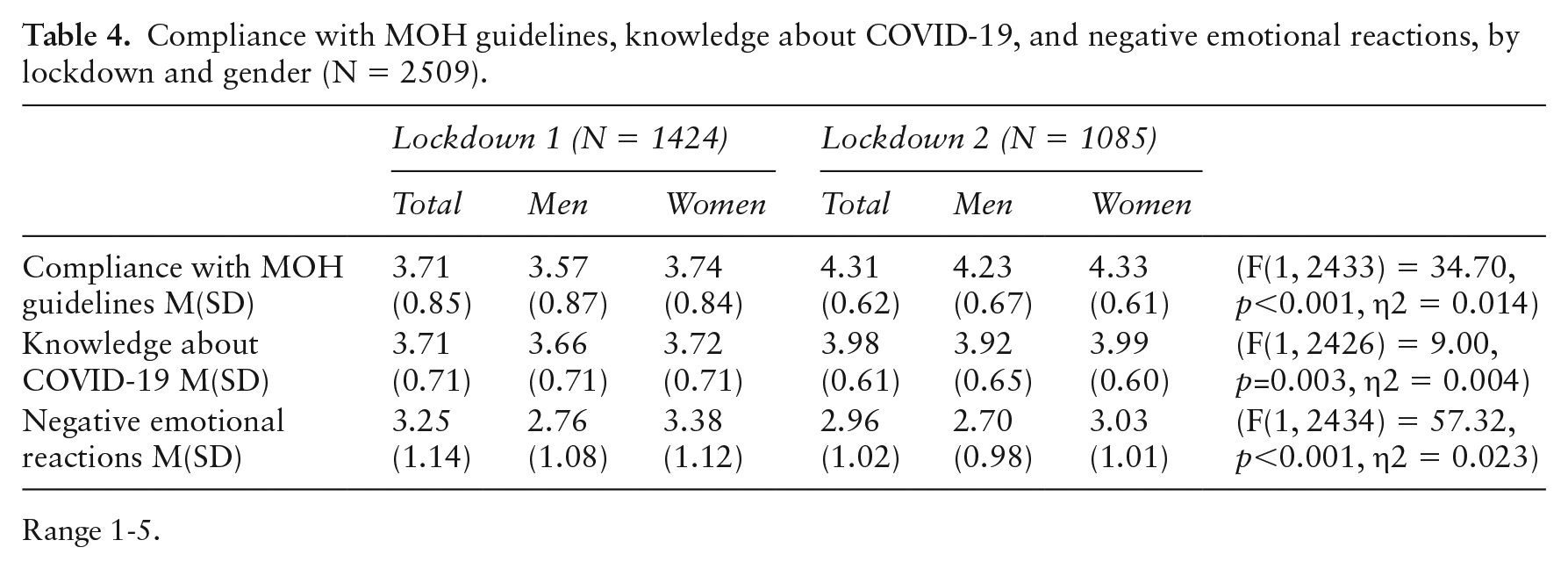
Range 1-5.
Compliance with MOH guidelines was significantly higher during the second lockdown than during the first (F(1, 2433) = 235.96, p < 0.001, η2 = 0.088). Overall, this factor was higher among women than among men (F(1, 2433) = 34.70, p <0.001, η2 = 0.014), while the interaction between lockdown and gender did not reach significance (F(1, 2433) = 0.77, p = 0.379, η2 = 0.001). The results for COVID-19 knowledge were significantly higher during the second lockdown than during the first (F(1, 2426) = 51.70, p < 0.001, η2 = 0.021). Overall, women knew more about COVID-19 than men (F(1, 2426) = 9.00, p = 0.003, η2 = 0.004), while the lockdown by gender interaction did not reach significance (F(1, 2426) = 0.08, p = 0.780, η2 = 0.001). The findings for negative emotional reactions were significantly higher during the first lockdown than during the second (F(1, 2434) = 9.44, p = 0.002, η2 = 0.004). Overall, negative reactions were higher among women than among men (F(1, 2434) = 57.32, p < 0.001, η2 = 0.023), and the lockdown by gender interaction was significant (F(1, 2434) = 7.38, p = 0.007, η2 = 0.003). That is, women scored higher than men on negative emotional reactions during both lockdowns, yet the extent of the difference was greater during the first lockdown (F(3, 2434) = 60.88, p < 0.001, η2 = 0.024) than during the second (F(3, 2434) = 10.96, p = 0.001, η2 = 0.004). To summarize, participants exhibited more compliance with MOH guidelines and had more COVID-19 knowledge during the second lockdown than during the first, whereas they exhibited more negative emotional reactions during the first lockdown than during the second. On all measures, women scored higher than men, corroborating Hypothesis 3.
Discussion
This study sought to examine gender differences in emotional reactions and compliance with MOH guidelines during two of Israel’s lockdowns.
The current study found that compliance with MOH guidelines, knowledge about COVID-19, and negative emotional reactions are higher among women than among men. These findings are generally consistent with those of previous research indicating that knowledge about COVID-19, psychological measures, and adhering to COVID-19 health guidelines are higher among women than among men (26,33). In a longitudinal online survey of 51,600 UK adults during lockdowns, compliance with guidelines was associated with negative emotional reactions, especially among women (34). Moreover, women had a greater burden of care during the lockdowns, both outside and within the home (13,17).
Additionally, our results found a significant interaction between gender and compliance with MOH guidelines, knowledge about COVID-19, and negative emotional reactions, with women’s results higher than those of men at both time points. During the first lockdown, people had to adapt to new circumstances in which shops, schools, and entertainment venues rapidly closed down, perhaps explaining the higher negative emotional reactions (4,7). Previous studies also showed that women were more affected by the psychological impact of the pandemic than men (7,8,10,12,14,15), consistent with our results. Note, however, that depression and anxiety are generally more prevalent in women than in men (35). A survey conducted in Israel a year after the COVID-19 outbreak found that men have higher risk-taking tendencies than women (e.g., consumption of beer, hard liquor, and illegal drugs) (25).
In the current study, women also reported higher levels of COVID-19 knowledge than men. Indeed, by the second lockdown, women knew a great deal about COVID-19. A possible explanation for this finding is that the high level of stress and anxiety caused by the pandemic stimulated the need for additional knowledge (8,27,28,30). The findings in the literature regarding the association between gender and knowledge are contradictory. In support of our finding, Zhong et al. (27) found that during the COVID-19 pandemic, women were more informed than men about the disease and were more diligent in following guidelines such as wearing masks and social distancing.
The women in our study also exhibited higher levels of compliance with MOH guidelines and had more knowledge about COVID-19 than men. In previous studies, gender has been consistently associated with rule adherence, such that during the COVID-19 pandemic, women were more likely to engage in protective behaviors (e.g., social distancing) than their male counterparts (8,26,27,36). During a prolonged lockdown in Melbourne (Australia) in late 2020 (112 days), women were found to have greater compliance intentions than men (36). This finding suggests that women are more inclined than men to adopt precautionary behaviors. These include washing hands, using hand sanitizer, wearing face masks, cleaning surfaces, and planning to seek medical attention if they suspect symptoms. This may reflect a broader perception that women are more susceptible to illness (8,26,27,36).
In line with previous results (13,17,21,34), the participants in our sample reported higher levels of compliance with MOH guidelines and had more knowledge about COVID-19 during the second lockdown and exhibited more negative emotional reactions during the first lockdown. One possible explanation for this finding is that during the first lockdown in Israel, participants described their sense of shock and chaos at the outbreak of the pandemic. This was followed by a gradual process of adjustment to the new situation, although they still had fears and concerns for their own welfare and that of their loved ones (3). People’s knowledge may have increased due to explanations provided by the government and the MOH, and media exposure. Nevertheless, stress levels in Israel remained high during the second lockdown, such that the situation was still perceived as unstable and unpredictable (37,38). Our study also showed that compliance with MOH guidelines and knowledge about COVID-19 were higher during the second lockdown. We assume that people who are conscious of the extent of a threat are likely to take reasonable steps to prevent harm (22,33). Further, high levels of pressure and threat may increase people’s motivation to comply with the guidelines to protect themselves from the pandemic (27,28,30).
Limitations
This study is limited by several factors. The majority of the study participants were women. Moreover, the sample was biased by the research design, which entailed online collection of self-report questionnaires, thus limiting the generalizability of our results. The research questionnaire assessed emotional reactions to COVID-19 by three questions about stress, fear, and worry. Yet emotional reactions in the context of mental health are much broader. Hence, future studies should also include items measuring depression, anxiety, and other emotional responses.
In addition, the online design made it more likely that participants would have access to digital resources, and have virtual social connections. Nevertheless, the lockdowns severely restricted physical mobility. Thanks to online recruitment, we were able to collect data from a diverse sample within a short time. In addition, including only respondents who completed the questionnaire in both collection periods may have produced a selection bias. The low response rate in the second wave may be explained by the fact that participants did not receive any compensation for participating in the study. Moreover, the length of the survey may have influenced the participation rate.
It should be noted that about a quarter of Israel’s population is composed of non-Jews, including Muslim Arabs, Christian Arabs, Druze, Bedouins, Circassians, and other communities. This study did not examine ethnic differences. Such differences should be examined in future studies.
Conclusion
Our findings revealed gender differences in negative emotional responses, compliance with MOH guidelines, and knowledge about COVID-19 during two lockdowns in Israel. The results showed higher levels of compliance with MOH guidelines and knowledge during the second lockdown, whereas people’s negative emotional reactions were higher during the first lockdown. Women scored higher than men on all measures. The fact that women seemed to experience more distress during the lockdowns shows that the lockdowns contributed to widening the existing structural gender gap. Previous studies have shown the need for health interventions targeting unique population groups. The results of this study suggest a need for developing gender-targeted interventions during future pandemics as well (39). For example, policymakers should consider providing childcare services during lockdowns as a means of reducing this gender gap in mental health. Women are usually the ones who take care of children while also working outside the home, potentially causing additional mental health problems. Moreover, health authorities should offer accessible e-mental health modules to help people cope with their mental health issues even when they must stay at home. We recommend conducting further research studies to examine these variables at additional points in time, as people continue coping with the crisis caused by the novel coronavirus.
Footnotes
Acknowledgements
We thank all those who participated for their efforts.
Author contributions
Both authors recruited the participants and collected the data. IL extracted and analyzed the data and wrote the paper. SSA revised the manuscript. Both authors read and approved the final manuscript.
Consent for publication
Not applicable.
Availability of data and materials
The data sets used in the study are available from the corresponding author upon request.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Oranim College of Education.
Ethics approval and consent to participate
The Ethics Committee of Bar-Ilan University approved the study (Authorization No. 032003). Our survey’s introductory page stated explicitly that proceeding to the questionnaire would signify consent to participate.