
Abstract
Introduction:
Health literacy allows us to make appropriate decisions about our self-care and to use health services appropriately, therefore, it conditions people’s health.
Objectives:
The aim of this study was to describe the level of health literacy of leisure time monitors and the influence of self-perception of health in times of pandemic.
Study design:
We used a cross-sectional observational design with non-probabilistic purposive sampling among leisure time monitors in the Autonomous Community of Galicia (Spain).
Method:
For this purpose, the HLS-EU-Q47 questionnaire measuring health literacy and a questionnaire measuring perception of COVID-19 were used.
Results:
The results verify that the monitors consider that the pandemic affects their daily life, that it will be a situation that will last for a long time, and they are very worried. The low level of health literacy of the leisure time monitors is also confirmed.
Conclusions:
Therefore, it seems urgent to evaluate the existing training programme and to include health education contents in this programme, given the involvement of leisure time monitors in the training of children and adolescents.
Introduction
The limited training of individuals influences the advancement of educational attainment, but is also related to low health literacy (1,2).
Despite the assistance that may be provided in health services in interpreting health information, studies report that individuals experience difficulty and frustration when they cannot accurately understand the content of communication from their health care providers (3). Therefore, it seems necessary to increase and improve training in health literacy not only for health personnel but also for educational personnel, given their relationship with young people and adolescents, especially in pandemic situations. However, there are few studies on health literacy in educators.
Theoretical framework
Having health literacy is very important to make decisions about our self-care and to use health services appropriately. Health literacy conditions people’s health and the safety and quality of the health care they receive (4,5). Low health literacy is a common problem worldwide and a serious problem in health care as low levels of health literacy are related to worse health outcomes. Therefore, it seems clear that educators must have high literacy to be able to educate in health. There are different definitions and approaches to the concept of health literacy (6–9). Mancuso (10) reviews definitions of health literacy and notes that they encompass integrated skills and strategies that enable the maintenance of good health. Although some authors also point out that the concept of health literacy is merely a recycling of classic concepts used in health promotion such as ‘empowerment’ or ‘patient involvement’ (11,12). Liu et al. (5) note that the health literacy builder covers three broad elements: (a) knowledge of health and health systems; (b) the processing and use of information in various formats related to health and health care; and (c) the ability to maintain health through self-management and working collaboratively with health providers. In this study we followed that of Okan et al. (13) who state that health literacy is the ability to access, understand, evaluate and apply health information, making it crucial for navigating the coronavirus and COVID-19 information environments.
In this study, we understand that leisure time monitors are health promotion agents as they develop dissemination activities and design, implement and evaluate programmes to promote healthy lifestyle habits in different institutions and with different collectives. The functions performed by the leisure time educator in the Autonomous Community of Galicia are regulated by Decree 50/2000 (14). It states that these educators must be able to carry out socio-cultural and recreational activities, both in urban leisure time and in nature, and be trained in areas as diverse as: psychosociology, animation, environmental education and nature, health education and organization and management of resources.
In addition, a recent study concludes that there is coherence between the contents of the training offered by the leisure schools and the expectations of the monitors and the people involved in the different training processes (15). Therefore, their knowledge of health seems fundamental to develop these programmes, but also to favour vicarious learning. Moreover, it has been shown that learners themselves can become health agents both at school and in the community (16,17). However, there are no studies on the level of health literacy of leisure time instructors. If we take into account the scarce studies on the group of teachers, we can say that there is a lack of studies on the health literacy level of leisure time instructors; the health literacy level is quite low (18–20) despite the relationship between health literacy and students’ health behaviours (21) and with their quality of life (22). Therefore, it seems necessary to increase and improve health literacy training not only in health personnel but also in educational personnel.
Hypothesis 1: Leisure time monitors have low health literacy.
During the pandemic the demand for health information has become more evident at a time of information overload and expectations to control health (13,23). The pandemic due to coronavirus disease 2019 (COVID-19) causes fear, as its immediate population consequences have created unprecedented challenges for education and health systems (24). Children and adolescents turn to the people with whom they spend the most time and have the most trust, making leisure educators a critical source of information. Indeed, Riiser et al. (25) indicate that it is television and family that are the primary sources of pandemic-related health information. But, as Paakkari and Okan (26) point out, health literacy is deficient among a population with a globally underestimated public health problem. Indeed, in Europe, almost half of adults have low levels of health literacy and lack the relevant skills to care for their health and the health of others. Therefore, health literacy is a central issue in curbing the spread of the virus and in disease prevention, as well as the preparedness of health systems in the treatment of the disease in situations that require a rapid reaction (27,28).
Hypothesis 2: Health literacy capabilities have an impact on the opinion of the pandemic situation.
The purpose of the study, therefore, was to determine the level of health literacy among leisure educators given their involvement in the training of children and adolescents and by dimensions and capabilities of the HLS-EU-Q47 scale (29); as well as the influence of health literacy on coping during the pandemic situation.
Method
We used a cross-sectional observational design with non-probabilistic purposive sampling among leisure time monitors in the Autonomous Community of Galicia (Spain).
Participants
The respondents were 156 women (85.7%) and 26 men (14.2%), with a mean age of 28.65 years (minimum = 19; maximum = 50). In relation to their area of residence, most of them live in a semi-rural environment (populations between 10,000 and 50,000 inhabitants) (45.1%), followed by those who live in a rural environment (populations under 10,000 inhabitants) (33%) and only 22% live in an urban environment (populations over 50,000 inhabitants).
Instruments
To measure the opinion on the pandemic situation, the Brief Illness Perception Questionnaire (BIP-Q5) for COVID-19 of Pérez-Fuentes et al. (30) was used, which is distributed in five questions with Likert scale type answers, on aspects related to the pandemic situation. The BIP-Q5 consists of five items on perceived threat of illness, where participants rate their agreement with the statements on a Likert-type scale from 0 to 10. In this case, each item has been analysed in particular. The questions asked were the following: Question 1 (Q1). How much does coronavirus infection affect your life? Q2. How long do you think coronavirus infection will last? Q3. To what extent are you experiencing symptoms due to coronavirus infection? Q4. To what extent are you concerned about coronavirus infection? Q5. How much does coronavirus infection affect you emotionally (i.e. does it make you feel angry, scared, upset or depressed)?
Other versions of the questionnaire have robust validations with Spanish samples (31,32).
The HLS-EU-Q47 (33) was used as an instrument to measure health literacy. It is a self-perception scale consisting of 47 questions that examen four health literacy capabilities (Access, Understand, Evaluate, Apply), referred to the processing of health information. Each of them has three different dimensions (Health care and attention, Disease prevention, Health promotion), which produces a matrix with 12 sub-dimensions of health literacy. Each item asks about the degree of difficulty each participant encounters in performing a particular task on a Likert scale with four categories (1 = very difficult, 2 = difficult, 3 = easy, 4 = very easy). A higher value will imply a better health literacy.
The reliability of the scale and all its capabilities and dimensions range from 0.786 to Apply to 0.947 for the health literacy scale. Access = 0.874; Understand = 0.810; Evaluate = 0.885; and Apply = 0.786. The dimensions obtained the following confidence: Health care = 0.842; Disease prevention = 0.878 and Health promotion = 0.905.
Procedure
To ensure the representativeness of the sample, the main associations of leisure time monitors in Galicia (N = 12) were identified, the number of professionals associated was determined and the survey was sent to them via email using a Google Forms form. The associations are located in the main cities of the autonomous community: Santiago de Compostela, Ourense, A Coruña, Lugo and Pontevedra.
The monitors completed the instrument sent by mail to their mailing addresses during the month of October 2020. Their participation was voluntary and anonymous, and their informed consent was requested respecting all ethical procedures for data collection, following the deontological standards recognized by the Declaration of Helsinki (revision of Fortaleza, Brazil, 2013) and in accordance with the recommendations of Good Clinical Practice of the EEC (document 111/3976/88 of July 1990) and the current Spanish legal regulations governing research.
Data analysis
First, the mean, standard deviation, minimums and maximums of the abilities, dimensions and sub-dimensions that make up the health literacy scale are calculated. In order to compare the results with the Spanish average, data were collected for each of the abilities and dimensions from the study by Ruiz-Cabello (34). For the questions related to COVID-19 we proceeded to calculate the frequency and percentage. To verify the parametric assumption of normality, the Kolmogorov–Smirnov test was used (p > 0.05), although non-parametric measures were used for ordinal data. In turn, procedures were carried out to detect missing values and outliers. Spearman’s bivariate correlations were calculated to establish the relationships between the different abilities, dimensions of the health literacy scale, Lickert-type questions related to the pandemic situation and self-perceived health.
Statistical analyses were performed with the SPSS v. 23 statistical software (IBM Corp., 2012). The significance level for all analyses was p < 0.05.
Results
Most of the monitors have a high self-perceived health, and only 0.5% have a very high self-perceived health (low = 1.6; normal = 5.7; high = 62.1;
If we analyse the opinion of the monitors with respect to the pandemic, we find that with respect to Q1, which aimed to find out how much the coronavirus infection affects daily life, the majority of the monitors think that it affects them quite a lot (n = 113), while 46 think that it affects them a lot and only 27 think that it affects them a little.
Q2 related to the length of time the coronavirus infection will last. Most of the monitors thought it would last quite long (n = 126) and only 24 thought it would last a short time.
However, through Q3, which focused on how much they feel symptoms due to coronavirus infection, the vast majority of the monitors have had no symptoms.
But they are concerned about coronavirus infection (Q4) as almost 85.7% are quite or very concerned. And, through Q5 we know that the pandemic resulting from coronavirus infection affects the monitors emotionally (Table 1).
Distribution of questions on COVID-19 (N=182).
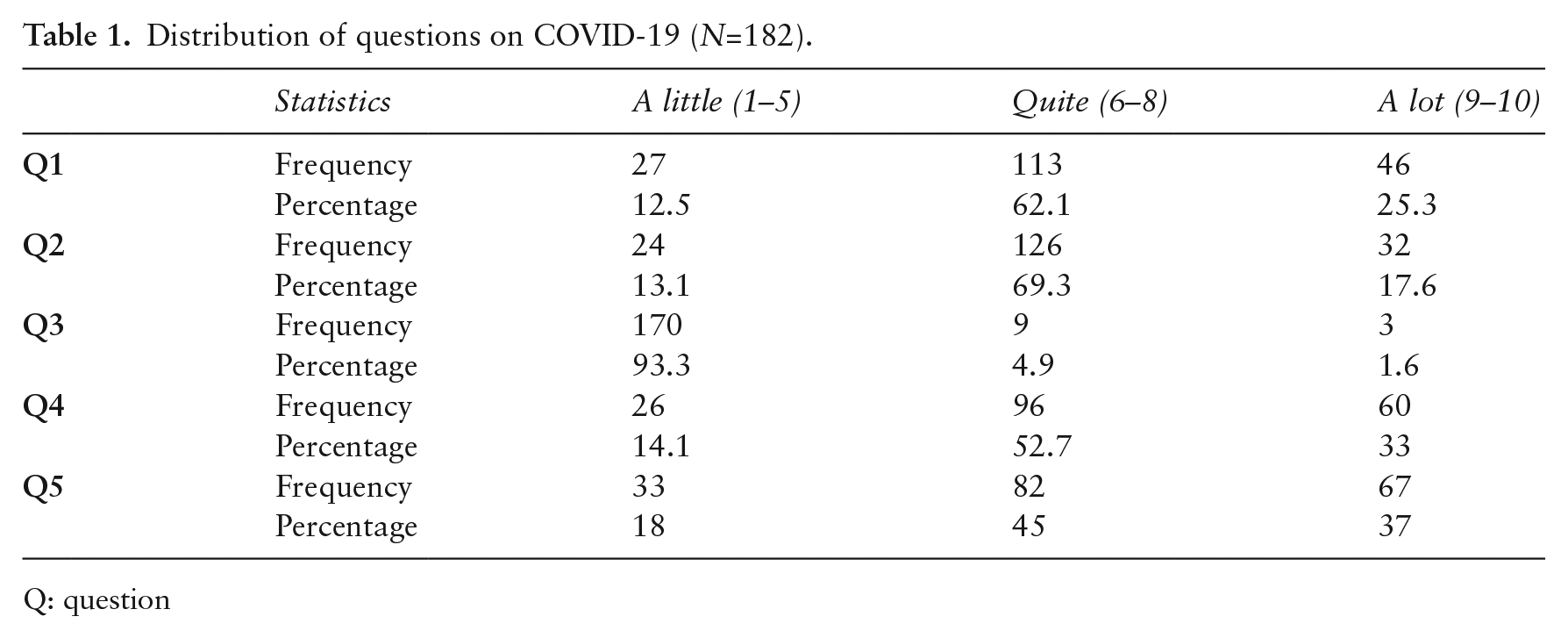
Q: question
With respect to the level of health literacy, we observe that the averages are relatively low, except in the case of understanding, which is the highest (
And in the case of the different dimensions, we can state that the highest mean is in the dimension attention and care of the disease (
We have included in Table 2 the average of the Spanish population in order to evaluate the level of health literacy of the monitors with respect to the general population. We can observe that the average in all dimensions and capacities is lower.
Distribution of HLS-EU-Q4 scale abilities and dimensions (N = 182).
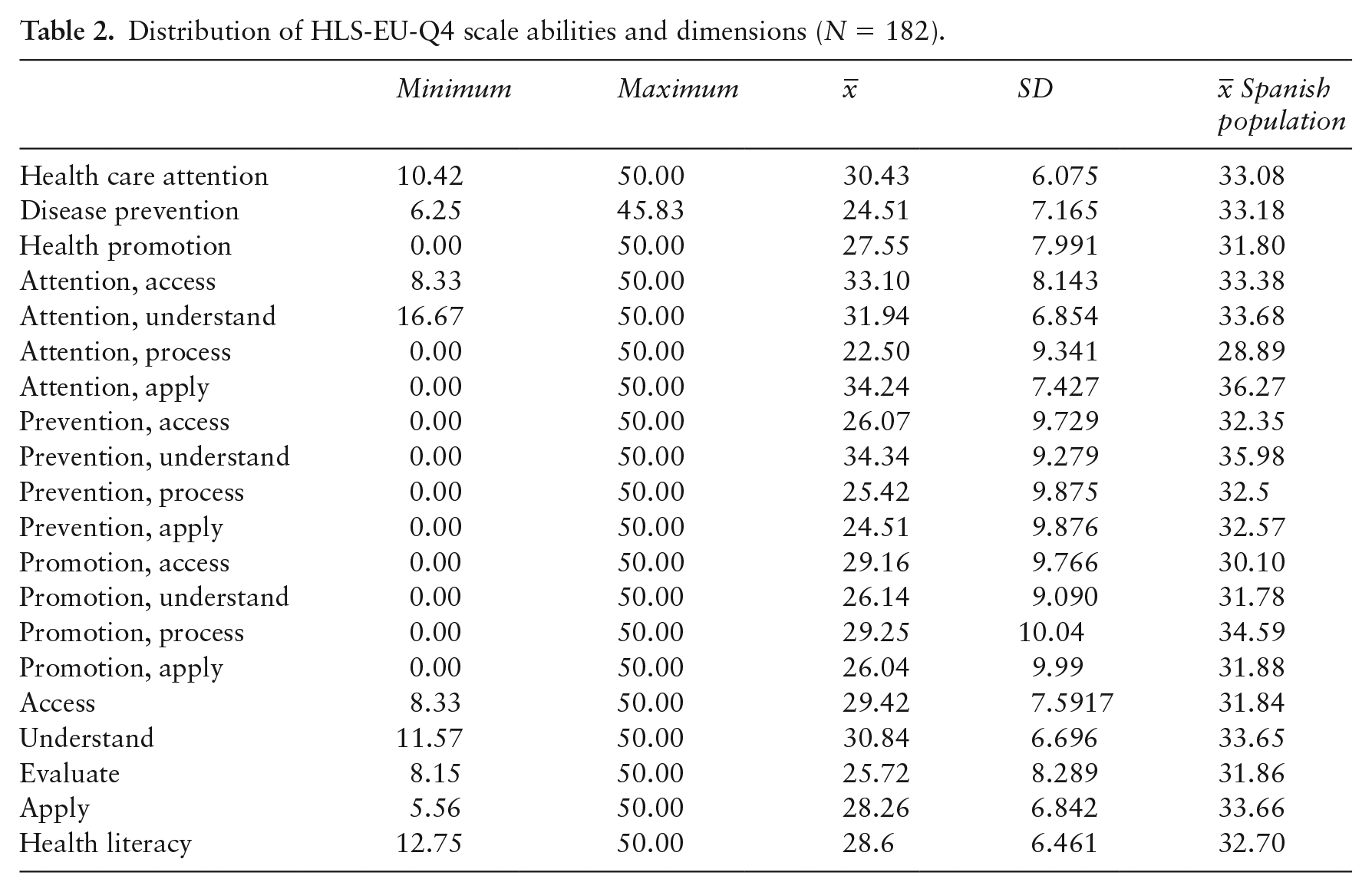
If we compare the data from the sample of monitors with the Spanish average, we can affirm that the average in all dimensions and skills is lower.
The correlations between the level of health literacy and the factors on their scale are very high, ranging from disease prevention (r = 0.932) to health care (r = 0.822). There is no correlation between the health literacy dimensions and their opinion on whether the coronavirus affects their daily life (Q1), nor in relation to the symptoms due to the infection (Q3), nor to the concern about the coronavirus infection (Q4), except for health promotion, in which, although the relationship is low (r = −0.175), it is significant. This means that the lower the capacity in health promotion, the higher the concern.
When the duration of the infection (Q2) is longer, there is a lower level of health literacy, especially in the ability to understand (r = −0.33), care (r = −0.182) and in health promotion (r = −0.175).
With respect to the extent to which coronavirus infection (Q5) affects them emotionally, there is a significant and negative relationship with all the abilities and dimensions of health literacy. Therefore, the more leisure time monitors feel angry, scared or depressed the lower their health literacy level is.
These data are consistent with the results of the correlation between self-perception of health and opinions about the pandemic. Thus, there is a negative and significant relationship between all the questions asked and self-perception of health. The lower the self-perception, the greater the concern about the pandemic, and the higher the self-perception, the higher the health literacy (r = 0.197; significance = 0.008) (Table 3).
Spearman correlation between opinion on pandemic, perception of health status and health literacy abilities and dimensions.
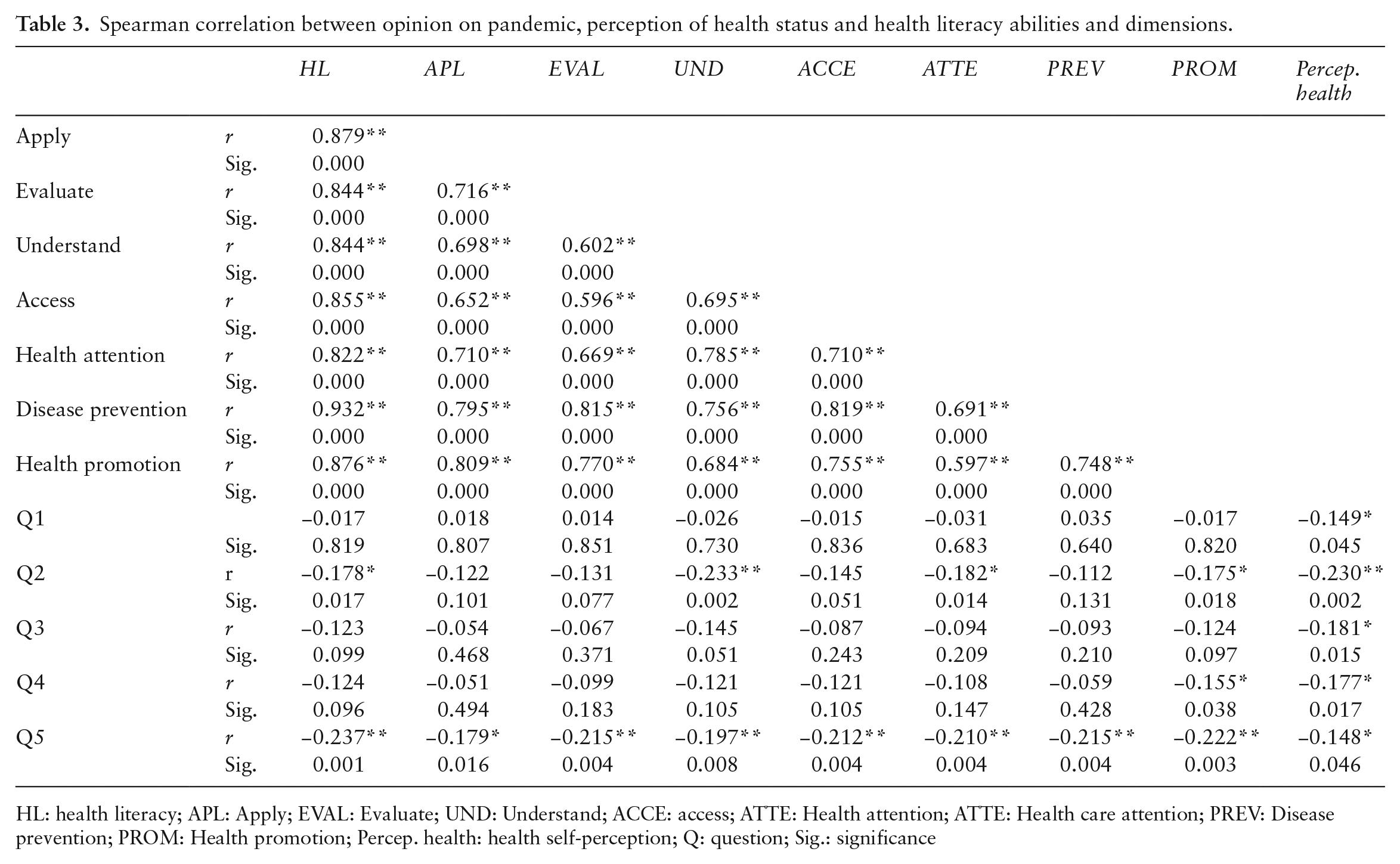
HL: health literacy; APL: Apply; EVAL: Evaluate; UND: Understand; ACCE: access; ATTE: Health attention; ATTE: Health care attention; PREV: Disease prevention; PROM: Health promotion; Percep. health: health self-perception; Q: question; Sig.: significance
Discussion and conclusions
Some studies point to the need to quantify the level of health literacy in the population given its benefits for maintaining adequate health (35). In addition, during this pandemic, we have been presented with a great challenge to integrate the vast amount of information into decision making about our personal behaviour. This requires basic health literacy (23). Indeed, since the emergence of the 2019 coronavirus disease pandemic, the disease has become one of the biggest challenges for public health systems globally (28). In this context, health literacy is more important than ever in the face of these global health threats, which have impacted all levels of the social-ecological model, including individual health behaviours, family relationships, organizational behaviour, state policy-making, mortality statistics and the international economy in the space of a few months and even weeks (27,36).
Therefore, it becomes necessary to have, in addition to a good health system, a key individual health literacy to solve complex real-life problems. Even during the pandemic it is difficult, but possible, to spend time to improve health literacy because governments and citizens require immediate action (26).
Given the communicative interaction that takes place in the educational processes during the free time of children and adolescents, we consider that these educators must have a high level of health literacy, especially in times of pandemic where the information must be very precise and consistent with the latest scientific advances.
With respect to hypothesis 1, the level of health literacy of leisure time monitors is low and below the Spanish average, thus confirming the poor training of these professionals (37,38). However, we must be cautious with this conclusion given that the study by Ruiz-Cabello (34) was conducted before the pandemic and covers the entire population, whereas this current study analyses a very specific population.
However, Paakkari and Okan (26) note that the rapid development of coronavirus 2019 disease has required individuals to acquire and apply medical information and adapt their behaviour at a very fast pace.
The highest abilities of the study monitors are Understand (ability to comprehend medical information, risk factors and health-related information and understand its meaning), Access (ability to access information on medical or clinical issues, risk factors and catch up) and Apply (ability to make informed decisions about medical problems, risk factors and thoughtful opinion on health issues) and the lowest is Evaluate (ability to interpret and evaluate medical information on risk factors and information related to health issues).
The dimension with the highest score is Health care (ability to access, understand, evaluate and make decisions about medical information), followed by Health promotion (ability to access, understand, evaluate and make decisions about health-related information and understand its meaning) and, finally, Disease prevention (ability to access, understand, evaluate and make decisions about risk factors).
Based on these data, we can conclude that the monitors are not able to interpret and evaluate health information and, therefore, have difficulties in making decisions about risk factors that affect their health. We must keep in mind that health promotion involves environmental, economic, biological and lifestyle factors and aims to increase control over health.
With respect to hypothesis 2, the leisure time monitors believe that the pandemic will modify their daily lives, they think that it will last for a long time, they are worried about the situation that affects them emotionally, although they have not experienced symptoms.
There is no correlation between health literacy capacities and the monitors’ opinion on whether the coronavirus affects their daily life, neither in relation to symptoms due to infection, nor to concern about coronavirus infection, except in health promotion. Therefore, situations arising from the pandemic have affected their health decision-making. In fact, the lower their capacity in health promotion, the greater their concern about the pandemic situation and the lower their level of health literacy, especially in the capacity to understand, care for and promote health, the longer they believe the pandemic will last.
These results are supported by the study of Okan et al. (13), who concluded that confusion about coronavirus information was significantly higher among those who were less health literate.
In fact, leisure time monitors feel frightened and even depressed the lower their health literacy level. In this line, Nguyen et al. (24) establishes a protective effect on depression during the health literacy epidemic and Nguyen et al. (39) point out that health literacy prevents pandemic fear, even in medical students.
Moreover, the lower their self-perception the greater their concern about the pandemic. And the higher their self-perceived health the higher their level of health literacy.
Limitations of the study and prospective
An observational study was carried out, so it is necessary to be cautious in generalizing the results because the type of sampling does not allow us to calculate the incidence of these opinions. Furthermore, the non-randomization of the sample prevents us from establishing causality; only the association between the different variables analysed is established. It would be very important to extend this type of study to similar population samples to know the incidence of the level of health literacy among educators.
However, based on the conclusions we have reached, we suggest the implementation of training programmes on health education among monitors and social educators working in the non-formal setting with different populations and among teachers working in the formal setting. The current training programme for leisure time monitors could be evaluated and health education contents could be included in this programme given the involvement of leisure time monitors in the training of children and adolescents.
These programs should introduce essential skills and resources necessary for people to find, understand, evaluate, communicate and use information and health services appropriately. Health literacy was already considered a crucial tool for the prevention of non-communicable diseases, but in these pandemic times, the efficacy of long-term, sustainable over time and beginning early in the life course investments in education and communication has also been demonstrated (26). Sentell et al. (27) note that greater understanding, appreciation and application of health literacy can support policy action at multiple levels to address major public health challenges.
With respect to educational strategies, Damian and Gallo (40) propose four levels of practice: in health care organizations, in community associations and collectives, increasing cross-sector collaborations, and collaborating with individual health care providers.
These actions could be complemented by targeted public information campaigns and health literacy promotion in social networks to improve the quality of information during the pandemic by identifying misinformation and facilitating decision making based on valid and reliable information (13). On the other hand, it is also necessary for the public administrations to demand and promote the training of monitors in health literacy since, at present, in spite of the numerous educational proposals in non-formal education, practically all of them exclude this training and hardly give it any importance. Even the legislation itself in the Autonomous Community of Galicia specifies only 30 compulsory hours of training in the Area of Health Education in courses of 350 hours.
Improving the health literacy of the population and health systems is fundamental to achieve health equity (27).
Footnotes
Acknowledgements
The authors thank Mr Pedro Jorge for their help in the translation and correction of the English version. To our colleagues in RED-IS (Red Educativa Docente-Innovar en Sociedad) for their critical comments to this study and support.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
No ethical approval was needed. Since in accordance with current legislation on social research, the approval of an ethics committee has not been requested since this is a research study in which data are collected through an anonymous survey and participants are asked to give their informed consent for data processing.