
Abstract
Despite vaccination and various prevention policies, the coronavirus (COVID-19) pandemic maintains its negative effects globally. Therefore, people must be adequately informed and put this knowledge into practice in order to take the necessary precautions. This can be achieved with adequate health literacy. In this context, this study was conducted to determine the relationship between health literacy, COVID-19 knowledge and adherence to preventive measures. The sample of this descriptive cross-sectional online survey consisted of 1086 people. Data were collected using a demographics questionnaire, the European Health Literacy Scale, the COVID-19 Knowledge Assessment Questionnaire and the COVID-19 Adherence Assessment Questionnaire. Participants’ health literacy index had a median score of 30.9, with 67.5% having inadequate or problematic health literacy. Gender, age, education, marital status, region of residence, employment status and economic status were associated with health literacy (p < 0.05). Participants’ median knowledge and adherence scores were 40 and 54, respectively. There were significant positive correlations between health literacy index, knowledge and adherence scores (p < 0.001). This study demonstrated that health literacy, COVID-19 knowledge and adherence were associated with each other. As a result, strategies aimed at improving health literacy may be beneficial in terms of having better knowledge and demonstrating high adherence to measures, thus, eradicating the COVID-19 pandemic, reducing COVID-19-related conditions and promoting public health.
Introduction
Pandemics are significant diseases in terms of public health because they affect not only infected individuals, but also the entire society (1). The COVID-19 pandemic is also one of those pandemics, resulting in many new cases and deaths, and has adversely affected public health (2). Since the first coronavirus (COVID-19) case was identified in Wuhan, China, COVID-19 has spread throughout the world and become a major pandemic (3). It resulted in 166,346,635 confirmed cases and 3,449,117 deaths worldwide as of 2021 (4). It also revealed significant inequalities in social life, economy and health (5,6).
There is no proven specific antiviral therapy that completely cures COVID-19 disease (3,7). On the other hand, as of 18 February 2021, at least seven different vaccines had been launched around the world (8). However, there are challenges in ensuring global access to COVID-19 vaccines (9). These challenges and the rapid global spread of COVID-19 have prompted people to learn more about the disease and the virus (10). Simultaneously, health authorities and policymakers have collaborated to reduce the risk of infection and virus spread around the world (7). Social awareness studies, publication of guides, curfew, online education and restrictions on religious, social, cultural and sporting activities have emerged with these collaborations (11). As a result of these efforts, health communication aimed at informing people about COVID-19 has become widespread, resulting in an infodemic and a lot of misinformation. Therefore, health literacy (HL) emerges as a critical concept in terms of obtaining accurate information and recognizing false information (10) as individuals’ ability to access, understand and apply this information, suggestions and solutions in daily life depend on their HL (7). HL is defined as ‘the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others’ (12). Combating the COVID-19 pandemic is possible with a high level of HL because the COVID-19 pandemic is manageable if society recognizes the significance of the measures to be implemented and then puts them into action (10).
Surveys carried out in numerous nations indicated that people’s levels of HL were inadequate. According to studies conducted in the United States and 17 European countries, 88% and 46% of people were found to have inadequate HL, respectively (13,14). Furthermore, 80% of Turks were found to have inadequate HL (15).
HL is an important aspect in increasing knowledge about diseases and behaviors for disease prevention. Several studies have found that HL is associated with knowledge and the practice of preventive behaviors against communicable diseases (16,17). According to Castro-Sánchez et al. (16), people with low or inadequate HL levels engage in less protective behavior against communicable diseases. Another study, conducted in Hong Kong, found a relationship between HL and older adults’ hand hygiene practices in the fight against infectious diseases (17). On the other hand, very few studies demonstrated that HL is an important determinant of COVID-19 knowledge and adherence to preventive measures (18–20).
Although it is well known that HL influences information and preventive behaviors against communicable and chronic diseases, it is unclear whether it will have a similar effect in this period when information regarding COVID-19 is scarce and there is much misinformation. Therefore, this study has been conducted to investigate the relationship between HL, COVID-19 knowledge level and adherence to preventive measures against COVID-19. This study will demonstrate whether there is an association between HL, COVID-19 knowledge and adherence to COVID-19 preventive measures in Turkey, which has not previously been explored.
Research questions
Is there an association between health literacy and COVID-19 knowledge?
Is there an association between health literacy and adherence to preventive measures?
Is there an association between COVID-19 knowledge and adherence to preventive measures?
Methods
Sample
The population of this descriptive cross-sectional online study consists of Turkish people aged 15 years and up. Inclusion criteria were; (a) being at least 15 years old, (b) being literate and (c) agreeing to participate in the research voluntarily. Without using any sampling process and after excluding four individuals under the age of 15, the sample was made up of 1086 people who met the inclusion criteria.
Measures
a. Demographics questionnaire
It consists of seven closed-ended questions about gender, age, education, marital status, region of residence, employment status and economic status.
b. European Health Literacy Scale (HLS-EU-Q47)
This scale was developed by the European Health Literacy Survey Consortium (21) and Abacıgil et al. adapted it into Turkish (22). There are 47 questions in total, with three subdomains: (a) health care, (b) disease prevention and (c) health promotion. For each question, participants must select ‘very difficult’ (one point), ‘difficult’ (two points), ‘easy’ (three points), ‘very easy’ (four points) or ‘don’t know’ for each question. The possible score can range between 47 and 188. In order to make the calculation easier, total scores were standardized between 0 and 50 using the formula; [mean − 1]*[50/3]. A score of ‘0–25’ points indicates inadequate HL, ‘> 25–33’ problematic HL, ‘> 33–42’ sufficient HL and ‘> 42–50’ excellent HL (22). Abacigil et al. calculated the Cronbach’s alpha value of the Turkish version as 0.95. Cronbach’s alpha coefficient of the HLS-EU-Q47 was found to be 0.963 in our study.
c. COVID-19 Knowledge Assessment Questionnaire
It is a self-administered form developed by the researchers based on various scientific publications regarding COVID-19 (23–28). It includes 50 information questions about the COVID-19 agent, symptoms, transmission routes, risk groups, treatment and prevention. Participants were asked to select one of the options of ‘True’, ‘False’ or ‘I Have No Information’ for each question about the COVID-19 agent, transmission routes and treatment; ‘Observed’, ‘Not Observed’ or ‘I Have No Information’ for each question about symptoms; ‘In Risk Group’, ‘Not in Risk Group’ or ‘I Have No Information’ for each question about risk groups and ‘Effective’, ‘Ineffective’ or ‘I Have No Information’ for the questions about prevention (Supplementary material Appendix 1 online). Correct responses were worth one point, while incorrect answers or marking ‘I Have No Information’ were worth zero points. The possible score can range between zero and 50. Higher scores on the scale indicate a higher level of knowledge. Cronbach’s alpha coefficient of the questionnaire was found to be 0.841 in our study.
d. COVID-19 Adherence Assessment Questionnaire
It is a self-administered form that was developed by researchers in order to assess the participants’ adherence to the COVID-19 preventive measures using the publications regarding COVID-19 (23–28). It consists of 30 preventative measures that should be implemented in order to prevent COVID-19 transmission. Participants were asked to select ‘Always’, ‘Sometimes’ or ‘Never’ for each item (Supplementary Appendix 2). ‘Always’ was worth two points, ‘Sometimes’ was worth one point and ‘Never’ was worth zero points. The possible score can range between zero and 60. Cronbach’s alpha coefficient of the questionnaire was found as 0.918 in our study.
Preliminary test of the measures
A preliminary test with 10 people was conducted to determine the comprehensibility of the data collection tools. The data collection phase of the research began after ensuring that there were no unclear questions in the questionnaires.
Data collection
Data of the study were collected between 07/June/2020 and 11/June/2020. At the start of the data collection, the daily number of cases and deaths in Turkey were 914 and 23, respectively (29). It was a normalization period in which the government relaxed restrictions on curfew, travel, workplace activities, lodging services and social life. Despite this, the researchers decided to collect the data online. Therefore, the survey link was distributed via WhatsApp, email and social media to those who agreed to participate in the study.
Statistical analysis
Data were analyzed in ‘IBM SPSS Statistics 22.0’ using descriptive statistics (number, frequency, percentage, mean, median), Mann–Whitney U, Kruskal–Wallis, and Spearman’s correlation tests. Descriptive statistics were performed to present the demographics data. Non-parametric tests were utilized in the analysis as the data were not normally distributed. In this context, Mann–Whitney U and Kruskal–Wallis tests were utilized to see whether there was a significant difference in the HL index between the groups. The Spearman’s correlation test was used to examine the relationships between COVID-19 knowledge, adherence and HL index. Statistical significance level was set at p < 0.05.
Ethical considerations
This study was approved and given ethics committee approval by the Social and Human Sciences Ethics Committee of Ankara Yıldırım Beyazıt University (date: 6 June 2020, number: 84892257-604.01.02-E.16735), as well as official written permission from the Turkish Ministry of Health (application form: ERDAL CEYLAN-2020-11-01T23_16_38.xml). All data were gathered in accordance with the Declaration of Helsinki. An informational text was placed on the first page to inform the participants about the research and to obtain informed consent for the participation in the study. In order to utilize the Turkish version of the HLS-EU-Q47 within this research, written permission was obtained from the author who conducted the validity research.
Results
A total of 1086 individuals who met the inclusion criteria and were included in the study. Table 1 shows the demographic data of the participants. Accordingly, 66.4% of the participants are female, 62.6% are between the ages of 17 and 29 years, 61.6% have a bachelor’s degree, 64.5% have never been married and 63.5% reside in an urban area. According to the analysis of the economic variables, 50.3% of the participants work, and 56.3% reported their income level as ‘Income is equal to expenses’.
Demographic data (N=1086).
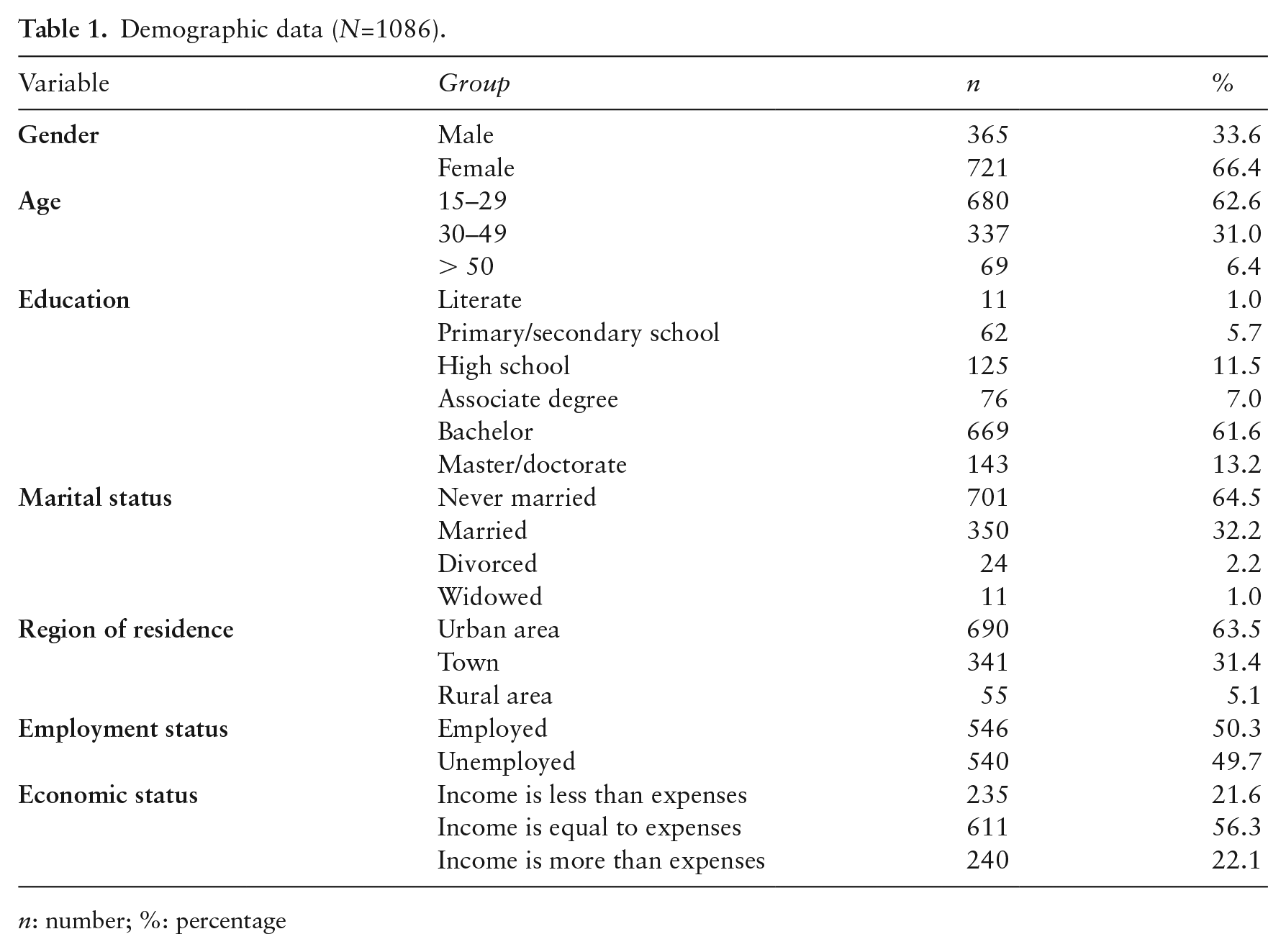
n: number; %: percentage
It was determined that 21.6% have inadequate HL and 45.9% have problematic HL while 20.3% and 12.2% have sufficient HL and excellent HL, respectively. The median score of the participants’ HL index was 30.9. This result indicates that participants in the study have a problematic HL level. Table 2 shows the distribution of HL scores among groups for each demographic variable, as well as the significance of results of the difference between groups. Accordingly, HL index was found to be associated with gender, age, education, marital status, region of residence and economic status.
Distribution of health literacy scores across demographic variables and the significance of group differences (N=1086).
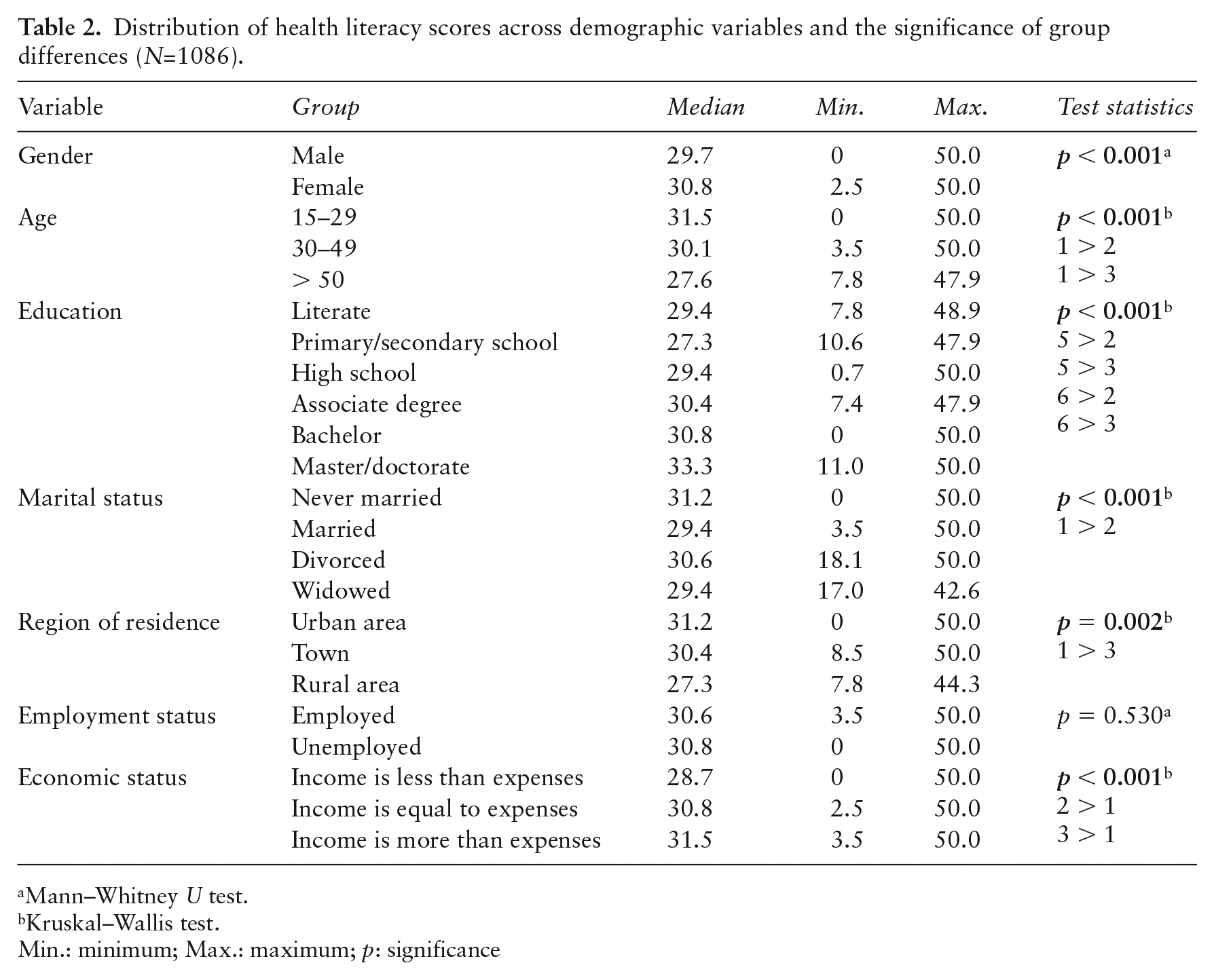
Mann–Whitney U test.
Kruskal–Wallis test.
Min.: minimum; Max.: maximum; p: significance
Knowledge and adherence scores were also analyzed. Accordingly, the median scores of knowledge and adherence were found to be 40 and 54, respectively. In addition, significant positive correlations were found between the HL index and knowledge score (r = 0.188, p < 0.001), as well as between HL index and adherence score (r = 0.182, p < 0.001). It was also determined that HL index was correlated with COVID-19 agent knowledge (r = 0.199, p < 0.001), symptoms knowledge (r = 0.123, p < 0.001), transmission routes knowledge (r = 0.099, p = 0.001), treatment knowledge (r = 0.126, p < 0.001) and prevention (r = 0.119, p < 0.001) knowledge scores, which are subdomains of the knowledge questionnaire (Table 3). The correlations between adherence and knowledge subdomains scores were also investigated. Accordingly, there were significant positive correlations between adherence and COVID-19 agent knowledge (r = 0.134, p < 0.001), as well as symptoms knowledge (r = 0.244, p < 0.001), while there was a weak negative relationship with transmission routes knowledge (r = −0.060, p = 0.046). Data on the correlation of HL, HL subdomains, general knowledge and knowledge subdomains scores are presented in Table 4.
Correlation analysis between knowledge, subdomains of knowledge, HL index and adherence scores (N=1086).
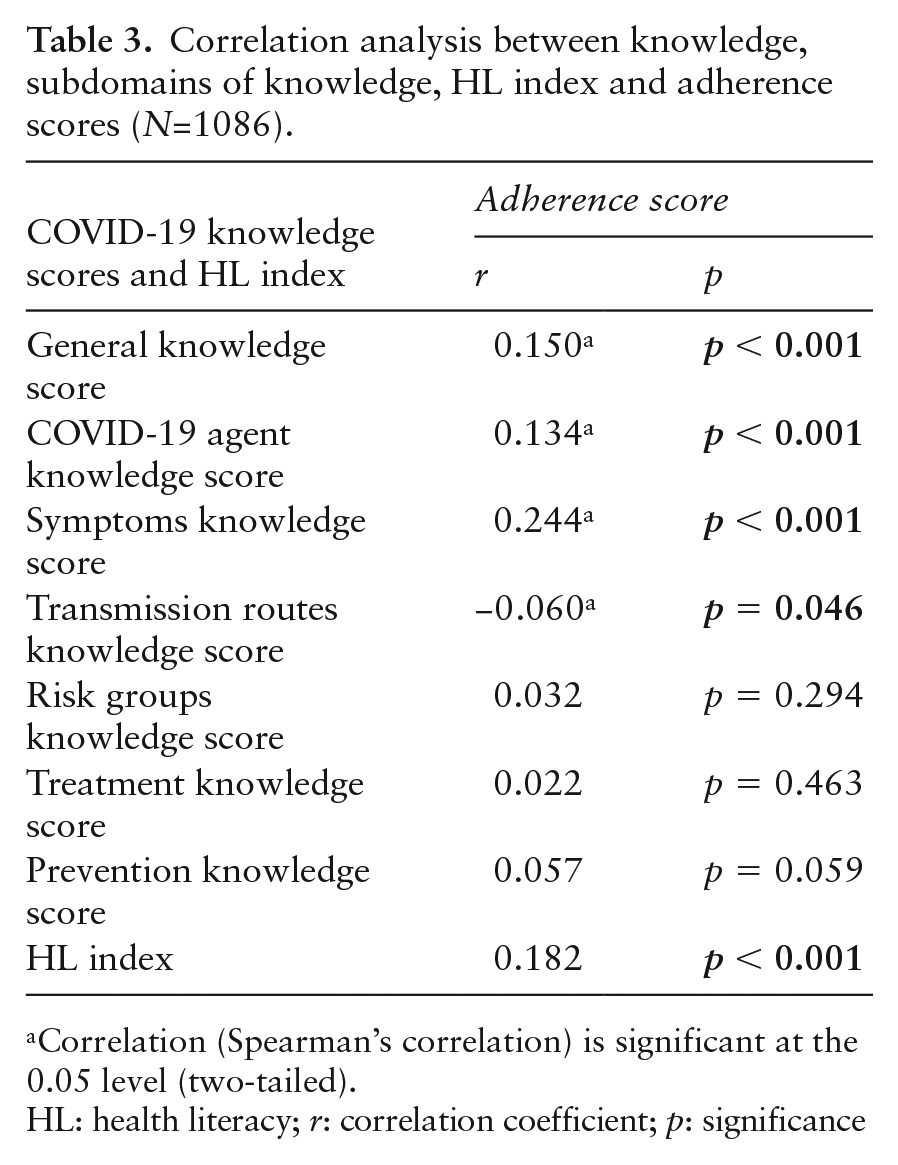
Correlation (Spearman’s correlation) is significant at the 0.05 level (two-tailed).
HL: health literacy; r: correlation coefficient; p: significance
Correlation analysis between health literacy, health literacy subdomains, general knowledge and knowledge subdomains scores (N=1086).
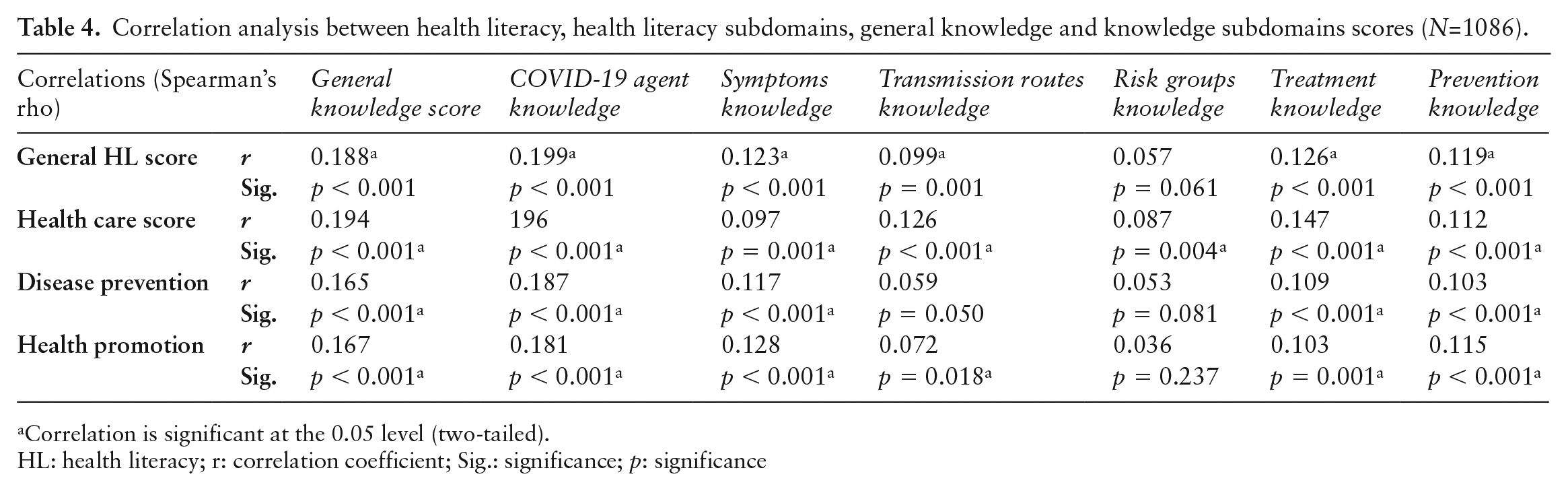
Correlation is significant at the 0.05 level (two-tailed).
HL: health literacy; r: correlation coefficient; Sig.: significance; p: significance
Discussion
This study was conducted to evaluate whether there was a relationship between HL, COVID-19 knowledge and adherence to preventive measures. To the best of our knowledge, this is the first study conducted with this aim in Turkey. It reveals significant findings in terms of emphasizing the importance of HL in improving COVID-19 knowledge, protecting individuals from COVID-19 and controlling the COVID-19 pandemic.
Since HL affects the health level of individuals and societies, it has been highlighted in various societies in recent years and is thus frequently studied. These studies revealed that HL levels were generally problematic or inadequate (13,15,30). Similar to these findings, we found that two out of every three people in our study had a problematic or inadequate HL level. We also determined that some sociodemographic characteristics were associated with HL. First, males scored higher on the HL scale than females. This finding is consistent with previous studies (31,32). The greater incidence of males in the 15–49 age group relative to females, where participants’ HL levels were higher than the other age groups’, is likely to have contributed to this result. Similar to this finding, various studies have also revealed that HL scores were better in younger age groups (33), inadequate HL was 1.83 times higher in individuals over 65 years old than in younger age groups (30) and age had a negative correlation with HL level (34). This result could be attributed to young people’s increased ability to access information via resources such as the internet, mobile phones and computers. This facilitates their access to and utilization of health-related information and enhances their level of HL. These findings suggest that efforts to improve HL in Turkish society should be stepped up with a greater emphasis on women, adults and the elderly.
We determined that people with bachelor or master/doctoral degree had better HL than those with primary/secondary or high school degree. This finding was supported by studies from Vietnam, Turkey, Kazakhstan and Iran (31,33–36). Individuals’ ability to access, understand and apply information about health problems is expected to increase as their level of education increases. It suggests that more understandable messages should be delivered through more common channels in order to raise the HL level of individuals with low education levels.
We have also found that unmarried people had better HL level than married people. The majority of the unmarried people in the study were young, while the majority of the married people were older. This could have influenced this finding. People living in urban areas had also better HL levels than people living in rural areas. This finding has been supported by Shaukat and Naveed (37) and Zahnd et al. (38). It reflects the disparity between rural and urban areas in terms of technological infrastructure, communication channels, access to information and distribution of educated individuals, as well as demonstrating that people living in rural areas are more likely to have low HL, inequality and thus more COVID-19 transmission.
Another significant finding was that people with a higher income than their expenses had the highest HL level. Decreased socioeconomic status has also been linked to lower HL in previous studies (35–39). These findings might be explained by the fact that persons with high earnings are often well-educated, have appropriate technology and have access to a varied range of information sources.
In this study, HL was found to be associated with COVID-19 general knowledge, COVID-19 agent knowledge, symptoms knowledge, transmission routes knowledge, treatment knowledge and prevention knowledge scores. Similarly, adequate HL was found to be associated with higher levels of hypertension, chronic obstructive pulmonary disease, diabetes (40), HIV/AIDS (41) and COVID-19 knowledge level, as well as the knowledge of COVID-19 agent, symptoms, transmission routes, treatment and prevention (18). As can be seen, HL plays an important role in increasing disease knowledge in people suffering from communicable and non-communicable diseases. Given that two-thirds of the study sample had insufficient or problematic HL, which could make it difficult to have sufficient knowledge of COVID-19 and which is believed to have a significant impact on COVID-19 protection, this finding should be taken seriously and acknowledged.
The health care HL subdomain was found to be related with general knowledge and all subdomains of knowledge in the study. Except for risk groups knowledge, the health promotion HL subdomain was related with all knowledge subdomains. Finally, there was a link between the disease prevention HL subdomain and general knowledge, agent, symptoms, treatment and prevention knowledge. Improved knowledge of COVID-19, agent, risk factors, symptoms, transmission routes, prevention and treatment can be attributed to a rise in HL toward health care, disease prevention and health promotion.
We also found a significant relationship between HL and adherence to preventive measures. This finding supports previous findings that HL influences prevention behaviors for sexually transmitted diseases (42,43), infectious diseases (17) and COVID-19 (44). Protection from communicable diseases can be achieved by avoiding disease-related risk factors and adhering to preventive measures, both of which are the outcomes of having adequate HL, which not only makes it easier for individuals to understand and interpret information about diseases, but also enables them to gain the ability to use this information and demonstrate appropriate behaviors.
Another notable finding of this study was the significant relationship between adherence to preventive measures, COVID-19 knowledge and subdomain scores of knowledge (agent, symptoms and transmission routes). This finding also corroborates the findings of Li and Liu as well as of Alrubaiee et al. (44,45). Similarly, it was reported that greater COVID-19 knowledge positively influenced self-adherence to COVID-19 mitigation recommendations (46). Individuals with high level of disease knowledge are thought to be more aware of the negative effects of diseases, symptoms, complex/difficult treatment processes and preventive measures. Therefore, the increase in the level of knowledge about COVID-19, symptoms and transmission routes is thought to improve the awareness of the importance of adopting appropriate behaviors for protection against disease and, as a result, adherence to preventive behaviors.
Strength and limitations
The main strength of the study is that the study survey link reached most of the cities in Turkey with different socio-demographic structures. In addition, the high research population and the high reliability coefficients of the scales are other strengths of the study. The main limitations of the study, on the other hand, are that the questionnaire link was not homogeneously distributed across all age groups, the sample size calculation required for the study has not been performed, and the validity and reliability analyses of the questionnaires developed by the researchers were not performed prior to their use.
Conclusion
HL was found to be associated with both knowledge and adherence to preventive measures. Furthermore, it was determined that as the knowledge improved, so did adherence to the preventive measures. However, HL level in this population was not at the desired level. Therefore, it is recommended to create education, interventions and policies by taking into account the factors affecting HL. Improving HL is thought to be beneficial in increasing both COVID-19 knowledge and adherence to preventive measures during the COVID-19 pandemic. This would result in a more informed and adherent society. As a result, managing the COVID-19 pandemic would be facilitated.
Supplemental Material
sj-docx-1-ghp-10.1177_17579759231187615 – Supplemental material for The association between health literacy, COVID-19 knowledge and adherence to preventive measures in Turkey
Supplemental material, sj-docx-1-ghp-10.1177_17579759231187615 for The association between health literacy, COVID-19 knowledge and adherence to preventive measures in Turkey by Erdal Ceylan and Ayşegül Koç in Global Health Promotion
Supplemental Material
sj-docx-2-ghp-10.1177_17579759231187615 – Supplemental material for The association between health literacy, COVID-19 knowledge and adherence to preventive measures in Turkey
Supplemental material, sj-docx-2-ghp-10.1177_17579759231187615 for The association between health literacy, COVID-19 knowledge and adherence to preventive measures in Turkey by Erdal Ceylan and Ayşegül Koç in Global Health Promotion
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.